
Comparison of Point Shear Wave Elastography and 2-Dimensional Shear Wave Elastography Values of Liver Metastases from Colorectal Cancer
 , , and
, , and 
Abstract
:1. Introduction
2. Aim
3. Materials and Methods
3.1. Patients
3.2. Methods
3.3. Statistical Analysis
4. Results
4.1. Background Information about the Patients with Liver Metastases from Colorectal Cancer
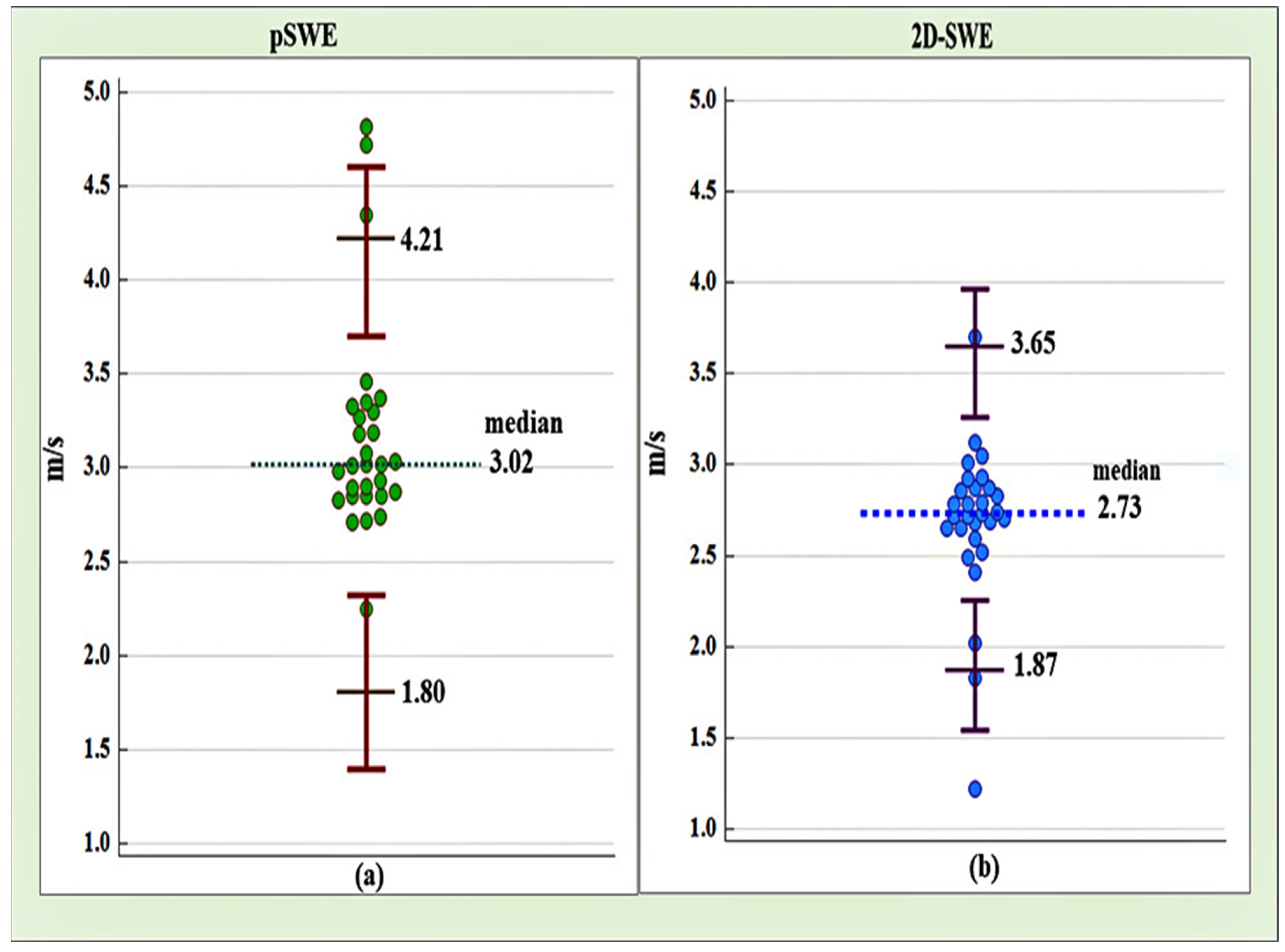
4.2. Reference Intervals Based on Point Shear Wave Elastography (pSWE) and Two-Dimensional Shear Wave Elastography (2D-SWE) for Liver Metastases from Colorectal Cancer
4.3. Level of Agreement between Point Shear Wave Elastography (pSWE) and Two-Dimensional Shear Wave Elastography (2D-SWE)
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kamaya, A.; Machtaler, S.; Sanjani, S.S.; Nikoozadeh, A.; Sommer, F.G.; Khuri-Yakub, B.T.; Willmann, J.; Desser, T.S. New technologies in clinical ultrasound. Semin. Roentgenol. 2013, 48, 214–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherlock, S. Diseases of the Liver and Biliary System: Needle Biopsy of the Liver, 8th ed.; Blackwell Scientific Publications: Boston, MA, USA; Melbourne, Australia, 1989; pp. 36–48. [Google Scholar]
- Arnold, M.; Sierra, S.M.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhat, S.K.; East, A.J. Colorectal cancer: Prevention and early diagnosis. Medicine 2015, 43, 295–298. [Google Scholar] [CrossRef]
- Wang, X.; O’Connell, K.; Jeon, J.; Song, M.; Hunter, D.; Hoffmeister, M.; Du, M. Combined effect of modifiable and non-modifiable risk factors for colorectal cancer risk in a pooled analysis of 11 population-based studies. BMJ Open Gastroenterol. 2019, 6, e000339. [Google Scholar] [CrossRef] [Green Version]
- Frampton, M.; Houlston, R.S. Modeling the prevention of colorectal cancer from the combined impact of host and behavioral risk factors. Genet Med. 2017, 19, 314–321. [Google Scholar] [CrossRef] [Green Version]
- Van Der Geest, L.G.M.; Lam-Boer, J.; Koopman, M.; Verhoef, C.; Elferink, M.A.G.; De Wilt, J.H.W. Nationwide trends in incidence, treatment and survival of colorectal cancer patients with synchronous metastases. Clin. Exp. Metastasis 2015, 32, 457–465. [Google Scholar] [CrossRef]
- Morris, E.J.; Forman, D.; Thomas, J.D.; Quirke, P.; Taylor, E.F.; Fairley, L.; Cottier, B.; Poston, G. Surgical management and outcomes of colorectal cancer liver metastases. Br. J. Surg. 2010, 97, 1110–1118. [Google Scholar] [CrossRef]
- Andres, A.; Mentha, G.; Adam, R.; Gerstel, E.; Skipenko, O.G.; Barroso, E.; Lopez-Ben, S.; Hubert, C.; Majno, P.E.; Toso, C. Surgical management of patients with colorectal cancer and simultaneous liver and lung metastases. Br. J. Surg. 2015, 102, 691–699. [Google Scholar] [CrossRef]
- De Baère, T.; Aupérin, A.; Deschamps, F.; Chevallier, P.; Gaubert, Y.; Boige, V.; Fonck, M.; Escudier, B.; Palussiére, J. Radiofrequency ablation is a valid treatment option for lung metastases: Experience in 566 patients with 1037 metastases. Ann. Oncol. 2015, 26, 987–991. [Google Scholar] [CrossRef]
- Klint, Å.; Engholm, G.; Storm, H.H.; Tryggvadóttir, L.; Gislum, M.; Hakulinen, T.; Bray, F. Trends in survival of patients diagnosed with cancer of the digestive organs in the Nordic countries 1964–2003 followed up to the end of 2006. Acta Oncol. 2010, 49, 578–607. [Google Scholar] [CrossRef] [PubMed]
- Stebbing, J.; Farouk, L.; Panos, G.; Anderson, M.; Jiao, L.R.; Mandalia, S.; Bower, M.; Gazzard, B.; Nelson, M. A meta-analysis of transient elastography for the detection of hepatic fibrosis. J. Clin. Gastroenterol. 2010, 44, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Gennisson, J.L.; Deffieux, T.; Fink, M.; Tanter, M. Ultrasound elastography: Principles and techniques. Diagn. Interv. Imaging 2013, 94, 487–495. [Google Scholar] [CrossRef] [PubMed]
- Bamber, J.; Cosgrove, D.; Dietrich, C.F.; Fromageau, J.; Bojunga, J.; Calliada, F.; Piscaglia, F. EFSUMB guidelines and recommendations on the clinical use of ultrasound elastography. Part 1: Basic principles and technology. Ultraschall Der Med. Eur. J. Ultrasound 2013, 34, 169–184. [Google Scholar] [CrossRef]
- Tang, A.; Cloutier, G.; Szeverenyi, N.M.; Sirlin, C.B. Ultrasound Elastography and MR Elastography for Assessing Liver Fibrosis: Part 1, Principles and Techniques. Am. J. Roentgenol. 2015, 205, 22–32. [Google Scholar] [CrossRef] [Green Version]
- Shiina, T.; Nightingale, K.R.; Palmeri, M.L.; Hall, T.J.; Bamber, J.C.; Barr, R.G.; Castera, L.; Choi, B.I.; Chou, Y.H.; Cosgrove, D.; et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 1: Basis principals and terminology. Ultrasound Med. Biol. 2015, 41, 1126–1147. [Google Scholar] [CrossRef] [Green Version]
- Ferraioli, G.; Filice, C.; Castera, L.; Choi, B.I.; Sporea, I.; Wilson, S.R.; Cosgrove, D.; Dietrich, C.F.; Amy, D.; Bamber, J.C.; et al. WFUMB guidelines and recommendations for clinical use of ultrasound elastography: Part 3: Liver. Ultrasound Med. Biol. 2015, 41, 1161–1179. [Google Scholar] [CrossRef] [Green Version]
- Park, H.S.; Kim, Y.J.; Yu, M.H.; Jung, S.I.; Jeon, H.J. Shear Wave Elastography of Focal Liver Lesion: Intraobserver Reproducibility and Elasticity Characterization. Ultrasound Q. 2015, 31, 262–271. [Google Scholar] [CrossRef]
- Guibal, A.; Boularan, C.; Bruce, M.; Vallin, M.; Pilleul, F.; Walter, T.; Scoazec, J.Y.; Boublay, N.; Dumortier, J.; Lefort, T. Evaluation of shearwave elastography for the characterisation of focal liver lesions on ultrasound. Eur. Radiol. 2013, 23, 1138–1149. [Google Scholar] [CrossRef]
- Brunel, T.; Guibal, A.; Boularan, C.; Ducerf, C.; Mabrut, J.Y.; Bancel, B.; Boussel, L.; Rode, A. Focal nodular hyperplasia and hepatocellular adenoma: The value of shear wave elastography for differential diagnosis. Eur. J. Radiol. 2015, 84, 2059–2064. [Google Scholar] [CrossRef]
- Fahey, B.J.; Nightingale, K.R.; Nelson, R.C.; Palmeri, M.L.; Trahey, G.E. Acoustic radiation force impulse imaging of the abdomen: Demonstration of feasibility and utility. Ultrasound Med. Biol. 2005, 31, 1185–1198. [Google Scholar] [CrossRef]
- Piccinino, F.; Sagnelli, E.; Pasquale, G.; Giusti, G. Complications following percutaneous liver biopsy. A multicentre retrospective study on 68,276 biopsies. J. Hepatol. 1986, 2, 165–173. [Google Scholar] [CrossRef]
- McGill, D.B.; Rakela, J.; Zinsmeister, A.R.; Ott, B.J. A 21-year experience with major hemorrhage after percutaneous liver biopsy. Gastroenterology 1990, 99, 1396–1400. [Google Scholar] [CrossRef]
- Beyer, T.; Townsend, D.W.; Brun, T.; Kinahan, P.; Charron, M.; Roddy, R.; Jerin, J.; Young, J.; Byars, L.; Nutt, R. A combined PET/CT scanner for clinical oncology. J. Nucl. Med. 2000, 41, 1369–1379. [Google Scholar] [PubMed]
- Bar-Shalom, R.; Yefremov, N.; Guralnik, L.; Gaitini, D.; Frenkel, A.; Kuten, A.; Altman, H.; Keidar, Z.; Israel, O. Clinical performance of PET/CT in evaluation of cancer: Additional value for diagnostic imaging and patient management. J. Nucl. Med. 2003, 44, 1200–1209. [Google Scholar]
- Cohade, C.; Osman, M.; Leal, J.; Wahl, R.L. Direct comparison of 18F-FDG PET and PET/CT in patients with colorectal carcinoma. J. Nucl. Med. 2003, 44, 1797–1803. [Google Scholar]
- Grant, A.; Neuberger, J. Guidelines on the use of liver biopsy in clinical practice. Gut 1999, 45 (Suppl. 1), 1V1–1V11. [Google Scholar] [CrossRef] [PubMed]
- Rockey, D.C.; Caldwell, S.H.; Goodman, Z.D.; Nelson, R.C.; Smith, A.D. Liver biopsy. Hepatology 2009, 49, 1017–1044. [Google Scholar] [CrossRef] [PubMed]
- Ronot, M.; Di Renzo, S.; Gregoli, B.; Duran, R.; Castera, L.; Van Beers, B.E.; Vilgrain, V. Characterization of fortuitously discovered focal liver lesions: Additional information provided by shearwave elastography. Eur. Radiol. 2015, 25, 346–358. [Google Scholar] [CrossRef]
- Akdoğan, E.; Yılmaz, F.G. The role of acoustic radiation force impulse elastography in the differentiation of benign and malignant focal liver masses. Turk. J. Gastroenterol. 2018, 29, 456–463. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total (n = 31) | Men (n = 20) | Women (n = 11) | p |
|---|---|---|---|---|
| Age | ||||
| ◦ mean ± SD | 65.37 ± 9.17 | 66.90 ± 9.52 | 62.90 ± 8.18 | 0.261 t |
| ◦ minimum-maximum | 37–80 | 37–80 | 49–78 | |
| Histology n (%) | ||||
| ◦ LD-AC | 3 (10.35%) | 3 (16.70%) | 0 (0.00%) | 0.07 f |
| ◦ MD-AC | 19 (65.50%) | 13 (72.20%) | 6 (54.50%) | 0.432 f |
| ◦ HD-AC | 7 (24.15%) | 2 (11.10%) | 5 (45.50%) | 0.268 f |
| BMI | ||||
| ◦ mean ± SD | 22.02 ± 1.41 | 22.25 ± 1.28 | 21.65 ± 1.58 | 0.278 t |
| ◦ minimum-maximum | 19.20 to 24.70 | 20.40 to 24.70 | 19.20 to 23.90 | |
| GGT median (IQR) | 56.00 (54.00) | 51.00 (42.50) | 76.00 (65.00) | 0.102 U |
| ALP mean ± SD | 298 ± 109.90 | 275.90 ± 75.10 | 335.20 ± 147.90 | 0.163 t |
| Total bilirubin median (IQR) | 17.20 (5.70) | 16.60 (5.10) | 18.30 (8.30) | 0.438 U |
| Direct bilirubin median (IQR) | 5.30 (3.60) | 5.30 (4.18) | 5.50 (3.80) | 0.759 U |
| ASAT median (IQR) | 44 (32.50) | 41.00 (22.00) | 45.00 (76.00) | 0.465 U |
| ALAT mean (±SD) | 47 (24.50) | 45.28 ± 18.19 | 58.09 ± 28.79 | 0.206 t |
| pSWE velocity (m/s) | ||||
| ◦ median | 3.02 (0.47) | 3.02 (0.42) | 2.98 (0.52) | 0.580 U |
| ◦ minimum-maximum | 2.25 to 4.82 | 2.25 to 4.82 | 2.71 to 4.72 | |
| 2D-SWE (m/s) | ||||
| ◦ median (IQR) | 2.73 (0.25) | 2.76 (0.24) | 2.68 (0.27) | 0.068 U |
| ◦ minimum-maximum | 1.22 to 3.70 | 1.22 to 3.12 | 1.83 to 3.70 | |
| pSWE depth (mm) | ||||
| ◦ median (IQR) | 47.72 (9.11) | 46.52 (9.24) | 50.70 (8.64) | 0.465 U |
| ◦ minimum-maximum | 30.37 to 54.33 | 31.49 to 51.97 | 30.37 to 54.33 | |
| 2-D-SWE depth (mm) | ||||
| ◦ median (IQR) | 46.80 (8.10) | 46.80 (6.05) | 50.20 (9.00) | 0.412 U |
| ◦ minimum-maximum | 29.40 to 54.40 | 32.00 to 53.40 | 29.40 to 54.40 | |
| Alcohol n (%) | 17 (56.60%) | 13 (72.20%) | 4 (36.40%) | 0.119 f |
| Smoking n (%) | 19 (65.50%) | 12 (66.70%) | 7 (63.60%) | 1.000 f |
| Variables | pSWE (m/s) | 2D-SWE (m/s) |
|---|---|---|
| Age | ||
| ◦ Pearson r | 0.114 | 0.392 |
| ◦ p | 0.557 | 0.035 |
| BMI | ||
| ◦ Pearson r | 0.162 | 0.091 |
| ◦ p | 0.402 | 0.637 |
| GGT | ||
| ◦ Spearman rho | 0.195 | −0.130 |
| ◦ p | 0.311 | 0.530 |
| ALP | ||
| ◦ Pearson r | −0.229 | 0.447 |
| ◦ p | 0.232 | 0.015 |
| Total bilirubin | ||
| ◦ Pearson r | −0.336 | 0.256 |
| ◦ p | 0.075 | 0.118 |
| Direct bilirubin | ||
| ◦ Pearson r | −0.254 | 0.070 |
| ◦ p | 0.192 | 0.722 |
| ASAT | ||
| ◦ Pearson r | −0.174 | 0.463 |
| ◦ p | 0.380 | 0.011 |
| ALAT | ||
| ◦ Pearson r | −0.267 | 0.459 |
| ◦ p | 0.162 | 0.012 |
| Tumor grade (histology) | ||
| ◦ Spearman r | −0.109 | −0.004 |
| ◦ p | 0.572 | 0.984 |
| Alcohol | ||
| ◦ Spearman r | 0.130 | −0.059 |
| ◦ p | 0.502 | 0.763 |
| Smoking | ||
| ◦ Spearman r | −0.100 | −0.117 |
| ◦ p | 0.607 | 0.704 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nacheva-Georgieva, E.L.; Doykov, D.I.; Hristov, B.K.; Doykova, K.A.; Doykov, M.I. Comparison of Point Shear Wave Elastography and 2-Dimensional Shear Wave Elastography Values of Liver Metastases from Colorectal Cancer. Gastroenterol. Insights 2023, 14, 271-281. https://doi.org/10.3390/gastroent14030019
Nacheva-Georgieva EL, Doykov DI, Hristov BK, Doykova KA, Doykov MI. Comparison of Point Shear Wave Elastography and 2-Dimensional Shear Wave Elastography Values of Liver Metastases from Colorectal Cancer. Gastroenterology Insights. 2023; 14(3):271-281. https://doi.org/10.3390/gastroent14030019
Chicago/Turabian StyleNacheva-Georgieva, Emiliya Lyubomirova, Daniel Ilianov Doykov, Bozhidar Krasimirov Hristov, Katya Angelova Doykova, and Mladen Ilianov Doykov. 2023. "Comparison of Point Shear Wave Elastography and 2-Dimensional Shear Wave Elastography Values of Liver Metastases from Colorectal Cancer" Gastroenterology Insights 14, no. 3: 271-281. https://doi.org/10.3390/gastroent14030019
APA StyleNacheva-Georgieva, E. L., Doykov, D. I., Hristov, B. K., Doykova, K. A., & Doykov, M. I. (2023). Comparison of Point Shear Wave Elastography and 2-Dimensional Shear Wave Elastography Values of Liver Metastases from Colorectal Cancer. Gastroenterology Insights, 14(3), 271-281. https://doi.org/10.3390/gastroent14030019