


EncephalApp Stroop Test as a Screening Tool for the Detection of Minimal Hepatic Encephalopathy in Patients with Cirrhosis—Single-Center Experience
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
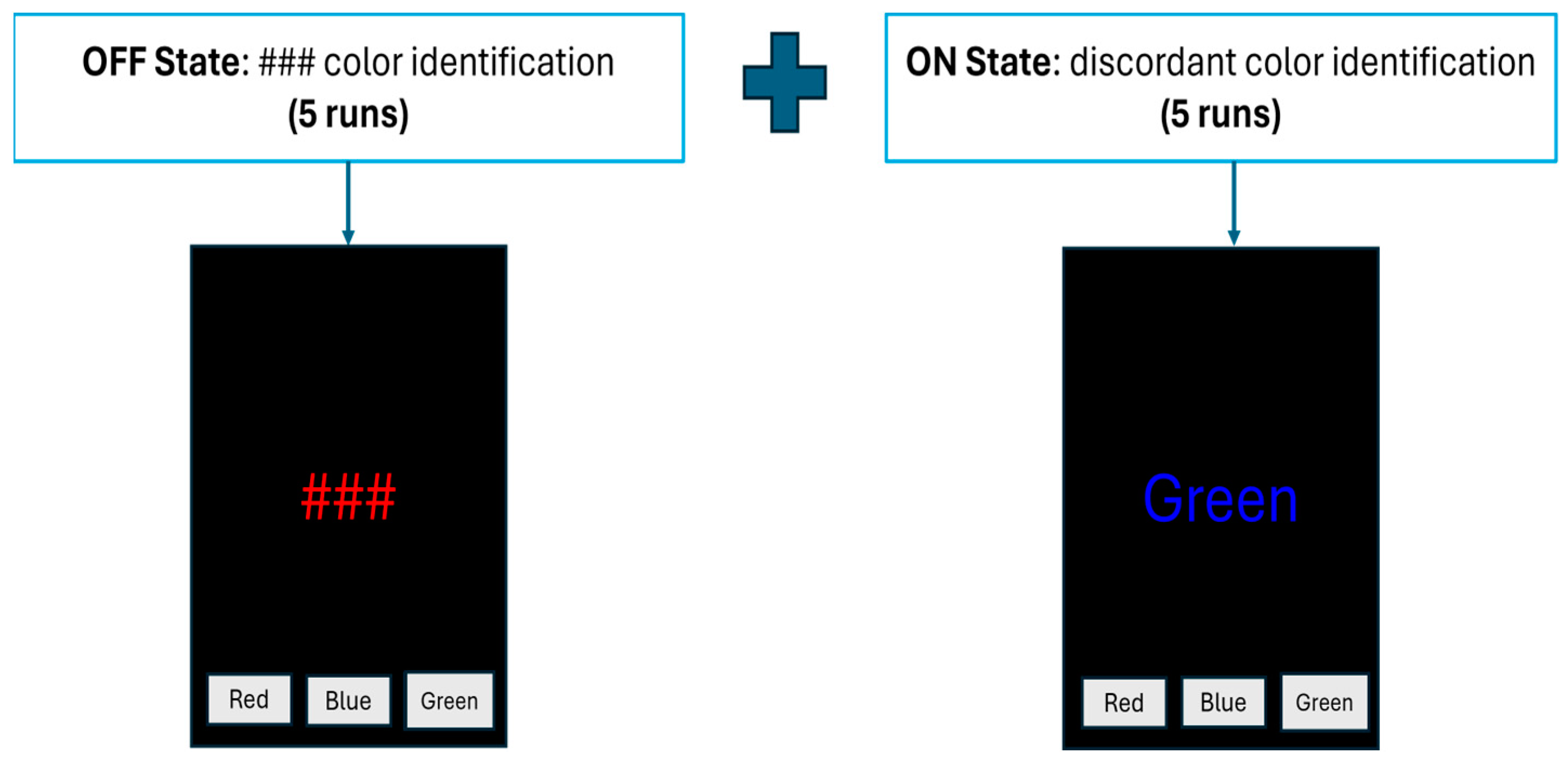
2.2. EncephalApp—Stroop Test
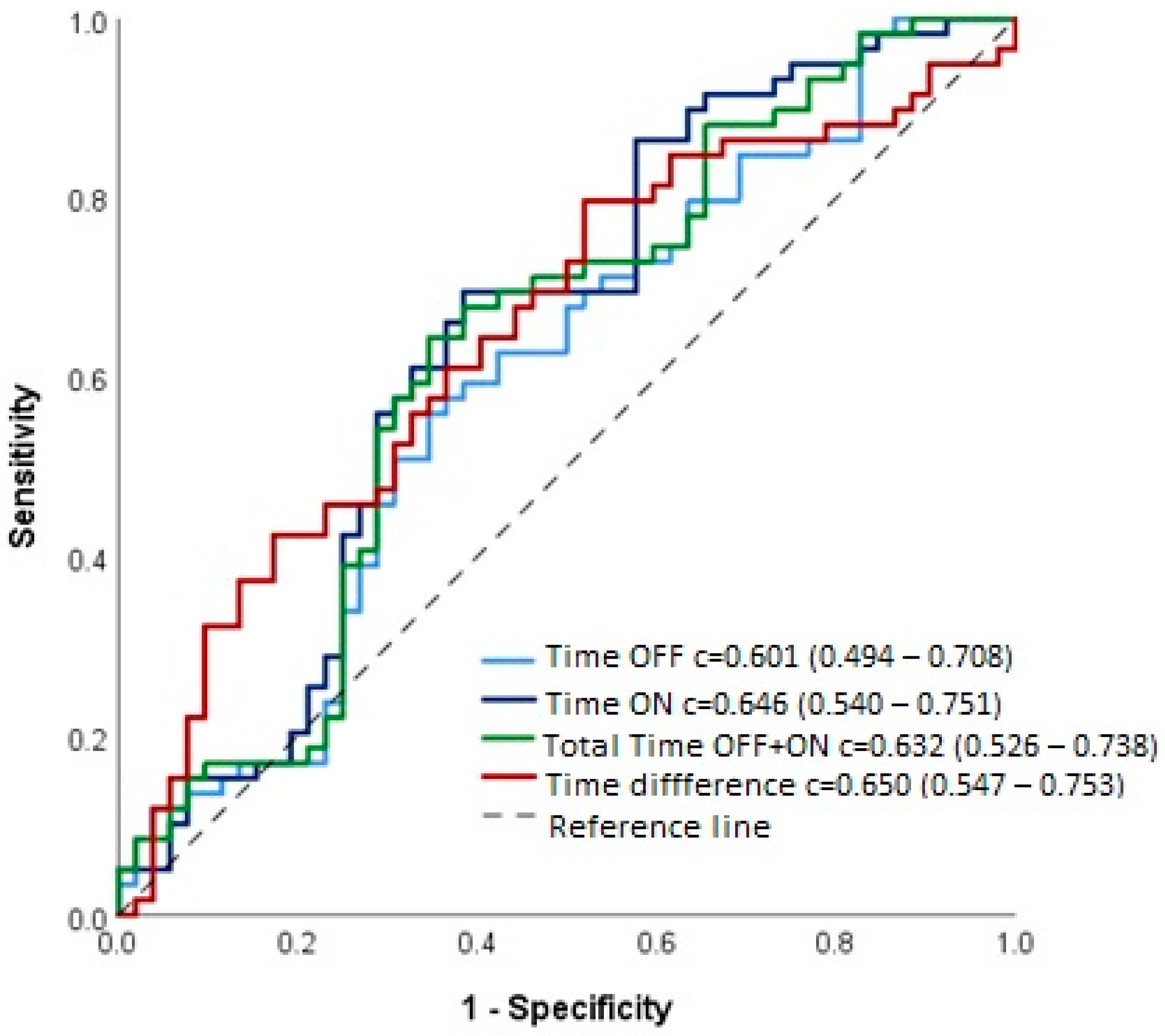
2.3. Statistical Analyses
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vilstrup, H.; Amodio, P.; Bajaj, J.; Cordoba, J.; Ferenci, P.; Mullen, K.D.; Weissenborn, K.; Wong, P.; Talwalkar, J.A.; Conjeevaram, H.S.; et al. Hepatic Encephalopathy in Chronic Liver Disease: 2014 Practice Guideline by the European Association for the Study of the Liver and the American Association for the Study of Liver Diseases. J. Hepatol. 2014, 61, 642–659. [Google Scholar] [CrossRef]
- Ferenci, P.; Lockwood, A.; Mullen, K.; Tarter, R.; Weissenborn, K.; Blei, A.T. Hepatic encephalopathy—Definition, nomenclature, diagnosis, and quantification: Final report of the Working Party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology 2002, 35, 716–721. [Google Scholar] [CrossRef]
- Montagnese, S.; Rautou, P.E.; Romero-Gómez, M.; Larsen, F.S.; Shawcross, D.L.; Thabut, D.; Vilstrup, H.; Weissenborn, K. EASL Clinical Practice Guidelines on the management of hepatic encephalopathy. J. Hepatol. 2022, 77, 807–824. [Google Scholar] [CrossRef]
- Rudler, M.; Weiss, N.; Bouzbib, C.; Thabut, D. Diagnosis and Management of Hepatic Encephalopathy. Clin. Liver Dis. 2021, 25, 393–417. [Google Scholar] [CrossRef]
- Montagnese, S.; Russo, F.P.; Amodio, P.; Burra, P.; Gasbarrini, A.; Loguercio, C.; Marchesini, G.; Merli, M.; Ponziani, F.R.; Riggio, O.; et al. Hepatic encephalopathy 2018: A clinical practice guideline by the Italian Association for the Study of the Liver (AISF). Dig. Liver Dis. 2019, 51, 190–205. [Google Scholar] [CrossRef] [PubMed]
- Faccioli, J.; Nardelli, S.; Gioia, S.; Riggio, O.; Ridola, L. Minimal Hepatic Encephalopathy Affects Daily Life of Cirrhotic Patients: A Viewpoint on Clinical Consequences and Therapeutic Opportunities. J. Clin. Med. 2022, 11, 7246. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Duarte-Rojo, A.; Xie, J.J.; Acharya, C.; Wade, J.B.; Robles, C.; Thacker, L.R.; Flud, C.; Fagan, A.; Garcia-Saenz-de-Sicilia, M.; et al. Minimal Hepatic Encephalopathy and Mild Cognitive Impairment Worsen Quality of Life in Elderly Patients With Cirrhosis. Clin. Gastroenterol. Hepatol. 2020, 18, 3008–3016.e2. [Google Scholar] [CrossRef] [PubMed]
- Tandon, P.; Pidborochynski, T.; Abraldes, J.G.; Carbonneau, M.; Newnham, K.; Bailey, R.; Ismond, K.P.; Bajaj, J.S.; Dobbs, B. The Assessment of Driving Fitness Using an On-Road Evaluation in Patients With Cirrhosis. Am. J. Gastroenterol. 2022, 117, 2017–2024. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Etemadian, A.; Hafeezullah, M.; Saeian, K. Testing for minimal hepatic encephalopathy in the United States: An AASLD survey. Hepatology 2007, 45, 833–834. [Google Scholar] [CrossRef] [PubMed]
- Montagnese, S.; Balistreri, E.; Schiff, S.; De Rui, M.; Angeli, P.; Zanus, G.; Cillo, U.; Bombonato, G.; Bolognesi, M.; Sacerdoti, D.; et al. Covert hepatic encephalopathy: Agreement and predictive validity of different indices. World J. Gastroenterol. 2014, 20, 15756–15762. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, J.S.; Thacker, L.R.; Heuman, D.M.; Fuchs, M.; Sterling, R.K.; Sanyal, A.J.; Puri, P.; Siddiqui, M.S.; Stravitz, R.T.; Bouneva, I.; et al. The stroop smartphone application is a short and valid method to screen for minimal hepatic encephalopathy. Hepatology 2013, 58, 1122–1132. [Google Scholar] [CrossRef]
- Allampati, S.; Duarte-Rojo, A.; Thacker, L.R.; Patidar, K.R.; White, M.B.; Klair, J.S.; John, B.; Heuman, D.M.; Wade, J.B.; Flud, C.; et al. Diagnosis of Minimal Hepatic Encephalopathy Using Stroop EncephalApp: A Multicenter US-Based, Norm-Based Study. Am. J. Gastroenterol. 2016, 111, 78–86. [Google Scholar] [CrossRef]
- Acharya, C.; Shaw, J.; Duong, N.; Fagan, A.; McGeorge, S.; Wade, J.B.; Thacker, L.R.; Bajaj, J.S. QuickStroop, a Shortened Version of EncephalApp, Detects Covert Hepatic Encephalopathy With Similar Accuracy Within One Minute. Clin. Gastroenterol. Hepatol. 2023, 21, 136–142. [Google Scholar] [CrossRef]
- Bajaj, J.S.; Heuman, D.M.; Sterling, R.K.; Sanyal, A.J.; Siddiqui, M.; Matherly, S.; Luketic, V.; Stravitz, R.T.; Fuchs, M.; Thacker, L.R.; et al. Validation of EncephalApp, Smartphone-Based Stroop Test, for the Diagnosis of Covert Hepatic Encephalopathy. Clin. Gastroenterol. Hepatol. 2015, 13, 1828–1835.e1. [Google Scholar] [CrossRef] [PubMed]
- Gairing, S.J.; Schleicher, E.M.; Galle, P.R.; Labenz, C.; Gairing, S.J.; Schleicher, E.M.; Galle, P.R.; Labenz, C. Prediction and prevention of the first episode of overt hepatic encephalopathy in patients with cirrhosis. Hepatol. Commun. 2023, 7, e0096. [Google Scholar] [CrossRef] [PubMed]
- Campagna, F.; Montagnese, S.; Ridola, L.; Senzolo, M.; Schiff, S.; De Rui, M.; Pasquale, C.; Nardelli, S.; Pentassuglio, I.; Merkel, C.; et al. The animal naming test: An easy tool for the assessment of hepatic encephalopathy. Hepatology 2017, 66, 198–208. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Taneja, S.; Chopra, M.; Duseja, A.; Dhiman, R.K. Animal Naming Test—A simple and accurate test for diagnosis of minimal hepatic encephalopathy and prediction of overt hepatic encephalopathy. Clin. Exp. Hepatol. 2020, 6, 116–124. [Google Scholar] [CrossRef]
- Labenz, C.; Beul, L.; Toenges, G.; Schattenberg, J.M.; Nagel, M.; Sprinzl, M.F.; Nguyen-Tat, M.; Zimmermann, T.; Huber, Y.; Marquardt, J.U.; et al. Validation of the simplified Animal Naming Test as primary screening tool for the diagnosis of covert hepatic encephalopathy. Eur. J. Intern. Med. 2019, 60, 96–100. [Google Scholar] [CrossRef]
- Huang, C.H.; Yu, T.Y.; Tseng, W.E.J.; Huang, Y.T.; Chang, S.H.; Hsieh, S.Y.; Chien, R.N.; Amodio, P. Animal naming test is a simple and valid tool for detecting covert hepatic encephalopathy and predicting outcomes in Chinese-speaking regions: A preliminary study. Ann. Med. 2023, 55, 2236013. [Google Scholar] [CrossRef]
- Guerra-Carrillo, B.; Katovich, K.; Bunge, S.A. Does higher education hone cognitive functioning and learning efficacy? Findings from a large and diverse sample. PLoS ONE 2017, 12, e0182276. [Google Scholar] [CrossRef]
- Ochoa-Sanchez, R.; Tamnanloo, F.; Rose, C.F. Hepatic Encephalopathy: From Metabolic to Neurodegenerative. Neurochem. Res. 2021, 46, 2612–2625. [Google Scholar] [CrossRef] [PubMed]
- Senzolo, M.; Pizzolato, G.; Ferronato, C.; Chierichetti, F.; Boccagni, P.; Dam, M.; Burra, P. Long-Term Evaluation of Cognitive Function and Cerebral Metabolism in Liver Transplanted Patients. Transplant. Proc. 2009, 41, 1295–1296. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, S.; Allampati, S.; Riggio, O.; Mullen, K.D.; Prakash, R.; Gioia, S.; Unser, A.; White, M.B.; Fagan, A.C.; Wade, J.B.; et al. Hepatic Encephalopathy Is Associated with Persistent Learning Impairments Despite Adequate Medical Treatment: A Multicenter, International Study. Dig. Dis. Sci. 2017, 62, 794–800. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Li, X.X.; Shi, P.M.; Zhang, Y.Y.; Song, Y.; Liu, Q.; Wei, L.; Bajaj, J.S.; Zhu, Y.H.; Li, Y.; et al. Utility of the EncephalApp Stroop Test for covert hepatic encephalopathy screening in Chinese cirrhotic patients. J. Gastroenterol. Hepatol. 2019, 34, 1843–1850. [Google Scholar] [CrossRef]
- Kaps, L.; Hildebrand, K.; Nagel, M.; Michel, M.; Kremer, W.M.; Hilscher, M.; Galle, P.R.; Schattenberg, J.M.; Wörns, M.-A.; Labenz, C. Validation of EncephalApp_Stroop as screening tool for the detection of minimal hepatic encephalopathy in German patients with liver cirrhosis. Clin. Res. Hepatol. Gastroenterol. 2022, 46, 101873. [Google Scholar]
- Hanai, T.; Shiraki, M.; Nishimura, K.; Miwa, T.; Maeda, T.; Ogiso, Y.; Imai, K.; Suetsugu, A.; Takai, K.; Shimizu, M. Usefulness of the Stroop Test in Diagnosing Minimal Hepatic Encephalopathy and Predicting Overt Hepatic Encephalopathy. Hepatol. Commun. 2021, 5, 1518–1526. [Google Scholar] [CrossRef] [PubMed]
- Kondo, Y.; Iwasa, M.; Kawaratani, H.; Miyaaki, H.; Hanai, T.; Kon, K.; Hirano, H.; Shimizu, M.; Yoshiji, H.; Okita, K.; et al. Proposal of Stroop test cut-off values as screening for neuropsychological impairments in cirrhosis: A Japanese multicenter study. Hepatol. Res. 2021, 51, 674–681. [Google Scholar] [CrossRef]
- Hamzaoui, L.; Mahmoudi, M.; Mohamed, G.; Elloumi, H.; Laabidi, A.; Boubaker, J.; Boudabbous, M.; Tahri, N.; Jemni, I.; Safer, L.; et al. EncephalApp Stroop Test for covert hepatic encephalopathy screening in Tunisian cirrhotic patients. F1000Research 2023, 11, 686. [Google Scholar] [CrossRef]
- Bai, W.; Chen, P.; Cai, H.; Zhang, Q.; Su, Z.; Cheung, T.; Jackson, T.; Sha, S.; Xiang, Y.-T. No TitlWorldwide prevalence of mild cognitive impairment among community dwellers aged 50 years and older: A meta-analysis and systematic review of epidemiology studiese. Age Ageing 2022, 51, afac173. [Google Scholar]
- Weissenborn, K. Minimal/Covert Hepatic Encephalopathy—Impact of Comorbid Conditions. J. Clin. Exp. Hepatol. 2019, 9, 109–111. [Google Scholar] [CrossRef]
- Cunha-Silva, M.; Neto, F.L.P.; de Araújo, P.S.; Pazinato, L.V.; Greca, R.D.; Secundo, T.M.L.; Imbrizi, M.R.; Monici, L.T.; Sevá-Pereira, T.; Mazo, D.F. EncephalApp Stroop Test validation for the screening of minimal hepatic encephalopathy in Brazil. Ann. Hepatol. 2022, 27, 4–9. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group | p-Value | ||
|---|---|---|---|
| Patients (n = 59) | Controls (n = 52) | ||
| Age (yrs) | 47.4 ± 18.1 | 48.1 ± 13.9 | 0.814 a |
| Sex (male) | 29 (49.2%) | 18 (34.6%) | 0.122 b |
| Education yrs | 12 (8–21) | 12 (8–16) | 0.219 c |
| Etiology | |||
| Alcohol | 22 (37.3%) | / | |
| Autoimmune | 20 (33.9%) | / | |
| Other | 17 (28.8%) | / | |
| Child-Pugh class | |||
| A | 13 (22.0%) | / | |
| B | 37 (62.7%) | / | |
| C | 9 (15.3%) | / | |
| Group | p-Value | ||
|---|---|---|---|
| Patients (n = 59) | Controls (n = 52) | ||
| Unsuccessful attempts | 0.86 ± 1.37 (0) | 0.42 ± 0.78 (0) | 0.049 a |
| Unsuccessful attempts | 27 (45.8%) | 15 (28.8%) | 0.067 b |
| 0 | 32 (54.2%) | 37 (71.2%) | 0.148 b |
| 1 | 15 (25.4%) | 10 (19.2%) | |
| 2+ | 12 (20.3%) | 5 (9.6%) | |
| Time OFF | 106.3 (84.5–126.3) | 91.4 (79.8–124.6) | 0.068 a |
| Time ON | 122.3 (97.8–150.2) | 105.3 (84.5–136.3) | 0.008 a |
| Total Time OFF + ON | 228.0 (180.7–274.9) | 195.6 (166.0–262.6) | 0.017 a |
| Time difference | 17.8 (8.8–29.7) | 9.8 (4.4–19.8) | 0.006 a |
| Etiology | p-Value | ||
|---|---|---|---|
| Alcohol (n = 22) | Non-Alcohol (n = 37) | ||
| Time OFF | 109.0 (93.7–137.1) | 98.3 (81.5–121.7) | 0.141 a |
| Time ON | 130.3 (115.8–166.1) | 117.3 (93.2–147.2) | 0.069 a |
| Total Time | 233.3 (215.9–300.4) | 212.9 (175.4–261.8) | 0.106 a |
| Child–Pugh Class | p-Value | |||
|---|---|---|---|---|
| A (n = 13) | B (n = 37) | C (n = 9) | ||
| Age (yrs) | 41.1 ± 17.6 | 50.7 ± 10.9 | 47.6 ± 17.0 | 0.212 a |
| Gender (male) | 7 (53.8%) | 18 (48.6%) | 4 (44.4%) | 1.000 b |
| Unsuccessful attempts | 1.08 ± 2.14 (1) | 0.92 ± 1.14 (0) | 0.33 ± 0.71 (0) | 0.320 c |
| Unsuccessful attempts | 7 (53.8%) | 18 (48.6%) | 2 (22.2%) | 0.338 b |
| 0 | 6 (46.2%) | 19 (51.4%) | 7 (77.8%) | 0.233 b |
| 1 | 6 (46.2%) | 8 (21.6%) | 1 (11.1%) | |
| 2+ | 1 (7.7%) | 10 (27.0%) | 1 (11.1%) | |
| Time OFF | 89.4 (74.2–134.0) | 106.3 (90.4–125.5) | 112.4 (92.3–118.9) | 0.401 c |
| Time ON | 118.1 (85.3–140.0) | 122.6 (98.2–147.2) | 138.9 (109.5–158.6) | 0.564 c |
| Total Time OFF + ON | 212.9 (161.6–274.9) | 227.0 (194.6–261.8) | 249.7 (204.6–271.1) | 0.457 c |
| Time difference | 21.2 (7.2–28.4) | 15.8 (8.8–24.5) | 28.1 (17.5–32.4) | 0.377 c |
| Age | ||||||
|---|---|---|---|---|---|---|
| <45 Years | ≥45 Years | |||||
| Patients (n = 24) | Controls (n = 23) | p-Value | Patients (n = 35) | Controls (n = 29) | p-Value | |
| Gender male | 13 (54.2%) | 11 (47.8%) | 0.664 b | 16 (45.7%) | 7 (24.1%) | 0.073 b |
| Education (yrs) | 12.7 ± 1.9 | 13.3 ± 1.9 | 0.242 a | 13.5 ± 2.8 | 11.8 ± 2.3 | 0.008 a |
| Education > 12 yrs | 5 (20.8%) | 9 (39.1%) | 0.170 a | 17 (48.6%) | 5 (17.2%) | 0.009 b |
| Unsuccessful attempts | 0 (0–1) | 0 (0–0) | 0.412 d | 1 (0–2) | 0 (0–1) | 0.059 d |
| Unsuccessful attempts | 7 (29.2%) | 4 (17.4%) | 0.341 b | 20 (57.1%) | 11 (37.9%) | 0.126 b |
| 0 | 17 (70.8%) | 19 (82.6%) | 0.542 c | 15 (42.9%) | 18 (62.1%) | 0.170 c |
| 1 | 5 (20.8%) | 2 (8.7%) | 10 (28.6%) | 8 (27.6%) | ||
| 2+ | 2 (8.3%) | 2 (8.7%) | 10 (28.6%) | 3 (10.3%) | ||
| Time OFF | 84.0 (75.3–103.1) | 78.8 (65.9–84.5) | 0.018 d | 118.8 (98.3–164.0) | 113.5 (92.5–156.9) | 0.522 d |
| Time ON | 98.0 (90.6–119.4) | 82.8 (75.1–91.0) | <0.001 d | 137.7 (121.0–188.1) | 127.0 (107.5–173.7) | 0.266 d |
| Total Time OFF + ON | 178.0 (165.7–227.5) | 161.2 (139.1–181.0) | 0.002 d | 258.5 (222.0–359.2) | 243.0 (199.4–338.1) | 0.335 d |
| Time difference | 13.9 (7.0–20.1) | 6.1 (1.0–12.7) | 0.014 d | 21.6 (11.0–32.4) | 17.1 (6.3–21.9) | 0.078 d |
| Education | ||||||
|---|---|---|---|---|---|---|
| ≤12 Years | >12 Years | |||||
| Cirrhosis (n = 37) | Healthy (n = 38) | p-Value | Cirrhosis (n = 22) | Healthy (n = 14) | p-Value | |
| Gender male | 17 (45.9%) | 14 (36.8%) | 0.423 b | 12 (54.5%) | 4 (28.6%) | 0.126 a |
| Unsuccessful attempts | 0.5 (0–1) | 0 (0–1) | 0.193 d | 0 (0–2) | 0 (0–0) | 0.116 c |
| Unsuccessful attempts | 18 (48.6%) | 12 (31.6%) | 0.131 b | 9 (40.9%) | 3 (21.4%) | 0.292 b |
| 0 | 19 (51.4%) | 26 (68.4%) | 0.225 c | 13 (59.1%) | 11 (78.6%) | 0.039 b |
| 1 | 13 (35.1%) | 7 (18.4%) | 2 (9.1%) | 3 (21.4%) | ||
| 2+ | 5 (13.5%) | 5 (13.2%) | 7 (31.8%) | 0 | ||
| Time OFF | 99.9 (81.5–134.0) | 95.6 (80.9–139.1) | 0.633 d | 111.1 (92.3–121.9) | 85.5 (78.8–90.5) | 0.004 c |
| Time ON | 121.0 (96.3–147.2) | 106.6 (84.0–149.8) | 0.215 d | 127.0 (108.6–150.2) | 91.2 (86.8–109.6) | 0.003 c |
| Total Time OFF + ON | 224.3 (175.5–274.9) | 199.5 (166.0–297.9) | 0.289 d | 236.9 (199.3–271.1) | 178.6 (166.0–197.0) | 0.003 c |
| Time difference | 16.3 (8.9–28.4) | 10.0 (5.4–20.4) | 0.055 d | 19.0 (8.8–31.3) | 9.0 (1.9–18.3) | 0.038 c |
| Patients (No Adjustment) | Adjusted for Age and Education | |
|---|---|---|
| Time OFF | 12.23 (0.139); Eta = 0.020 | 13.03 (0.039); Eta = 0.039 |
| Log Time OFF | 0.047 (0.092); Eta = 0.026 | 0.049 (0.013); Eta = 0.056 |
| Time ON | 18.27 (0.068); Eta = 0.030 | 18.71 (0.016); Eta = 0.053 |
| Log Time ON | 0.066 (0.025); Eta = 0.045 | 0.066 (0.001); Eta = 0.093 |
| Total Time | 30.49 (0.090); Eta = 0.026 | 31.74 (0.020); Eta = 0.049 |
| Log Total Time | 0.057 (0.043); Eta = 0.037 | 0.058 (0.003); Eta = 0.080 |
| Time difference | 6.045 (0.106); Eta = 0.024 | 5.673 (0.121); Eta = 0.022 |
| Time OFF x #Attempts | 61.13 (0.139); Eta = 0.020 | 65.18 (0.039); Eta = 0.039 |
| Log Time OFF x #Attempts | 0.047 (0.092); Eta = 0.026 | 0.049 (0.013); Eta = 0.056 |
| Time ON x #Attempts | 91.36 (0.068); Eta = 0.030 | 93.55 (0.016); Eta = 0.053 |
| Log Time ON x #Attempts | 0.066 (0.025); Eta = 0.045 | 0.066 (0.001); Eta = 0.093 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vojnovic, M.; Pantic, I.; Jankovic, G.; Stulic, M.; Lalosevic, M.S.; Pejic, N.; Milovanovic, T. EncephalApp Stroop Test as a Screening Tool for the Detection of Minimal Hepatic Encephalopathy in Patients with Cirrhosis—Single-Center Experience. Gastroenterol. Insights 2024, 15, 237-247. https://doi.org/10.3390/gastroent15010017
Vojnovic M, Pantic I, Jankovic G, Stulic M, Lalosevic MS, Pejic N, Milovanovic T. EncephalApp Stroop Test as a Screening Tool for the Detection of Minimal Hepatic Encephalopathy in Patients with Cirrhosis—Single-Center Experience. Gastroenterology Insights. 2024; 15(1):237-247. https://doi.org/10.3390/gastroent15010017
Chicago/Turabian StyleVojnovic, Marko, Ivana Pantic, Goran Jankovic, Milos Stulic, Milica Stojkovic Lalosevic, Nina Pejic, and Tamara Milovanovic. 2024. "EncephalApp Stroop Test as a Screening Tool for the Detection of Minimal Hepatic Encephalopathy in Patients with Cirrhosis—Single-Center Experience" Gastroenterology Insights 15, no. 1: 237-247. https://doi.org/10.3390/gastroent15010017
APA StyleVojnovic, M., Pantic, I., Jankovic, G., Stulic, M., Lalosevic, M. S., Pejic, N., & Milovanovic, T. (2024). EncephalApp Stroop Test as a Screening Tool for the Detection of Minimal Hepatic Encephalopathy in Patients with Cirrhosis—Single-Center Experience. Gastroenterology Insights, 15(1), 237-247. https://doi.org/10.3390/gastroent15010017