
Anti-SARS-CoV-2 Antibody Status at the Time of Hospital Admission and the Prognosis of Patients with COVID-19: A Prospective Observational Study

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Patients
2.3. Biochemical Analysis
2.4. Statistical Analysis
2.5. Ethics
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Taylor, L. Covid-19: True global death toll from pandemic is almost 15 million, says WHO. BMJ 2022, 377, 1144. [Google Scholar] [CrossRef] [PubMed]
- Burn, E.; Tebé, C.; Fernandez-Bertolin, S.; Aragon, M.; Recalde, M.; Roel, E.; Prats-Uribe, A.; Prieto-Alhambra, D.; Duarte-Salles, T. The natural history of symptomatic COVID-19 during the first wave in Catalonia. Nat. Commun. 2021, 12, 777. [Google Scholar] [CrossRef] [PubMed]
- de Bruin, S.; Bos, L.D.; van Roon, M.A.; Boer, A.M.T.-D.; Schuurman, A.R.; Koel-Simmelinck, M.J.; Bogaard, H.J.; Tuinman, P.R.; van Agtmael, M.A.; Hamann, J.; et al. Clinical features and prognostic factors in Covid-19: A prospective cohort study. EBioMedicine 2021, 67, 103378. [Google Scholar] [CrossRef] [PubMed]
- Marin, B.G.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef] [PubMed]
- De Vito, D.; Di Ciaula, A.; Palmieri, V.O.; Trerotoli, P.; Larocca, A.M.V.; Montagna, M.T.; Portincasa, P. Reduced COVID-19 mortality linked with early antibodies against SARS-CoV-2, irrespective of age. Eur. J. Intern. Med. 2022, 98, 77–82. [Google Scholar] [CrossRef]
- Zohar, T.; Loos, C.; Fischinger, S.; Atyeo, C.; Wang, C.; Slein, M.D.; Burke, J.; Yu, J.; Feldman, J.; Hauser, B.M.; et al. Compromised humoral functional evolution tracks with SARS-CoV-2 mortality. Cell 2020, 183, 1508–1519. [Google Scholar] [CrossRef]
- Dispinseri, S.; Secchi, M.; Pirillo, M.F.; Tolazzi, M.; Borghi, M.; Brigatti, C.; De Angelis, M.L.; Baratella, M.; Bazzigaluppi, E.; Venturi, G.; et al. Neutralizing antibody responses to SARS-CoV-2 in symptomatic COVID-19 is persistent and critical for survival. Nat. Commun. 2021, 12, 2670. [Google Scholar] [CrossRef]
- Liu, X.; Zheng, X.; Liu, B.; Wu, M.; Zhang, Z.; Zhang, G.; Su, X. Serum IgM against SARS-CoV-2 correlates with in-hospital mortality in severe/critical patients with COVID-19 in Wuhan, China. Aging 2020, 12, 12432–12440. [Google Scholar] [CrossRef]
- Garcia-Beltran, W.F.; Lam, E.C.; Astudillo, M.G.; Yang, D.; Miller, T.E.; Feldman, J.; Hauser, B.M.; Caradonna, T.M.; Clayton, K.L.; Nitido, A.D.; et al. COVID-19-neutralizing antibodies predict disease severity and survival. Cell 2021, 184, 476–488. [Google Scholar] [CrossRef]
- Cheng, Z.J.; Li, B.; Zhan, Z.; Zhao, Z.; Xue, M.; Zheng, P.; Lyu, J.; Hu, C.; He, J.; Chen, R.; et al. Clinical application of antibody immunity against SARS-CoV-2: Comprehensive review on immunoassay and immunotherapy. Clin. Rev. Allergy Immunol. 2022. [Google Scholar] [CrossRef]
- Chen, W.; Zhang, J.; Qin, X.; Wang, W.; Xu, M.; Wang, L.-F.; Xu, C.; Tang, S.; Liu, P.; Zhang, L.; et al. SARS-CoV-2 neutralizing antibody levels are correlated with severity of COVID-19 pneumonia. Biomed. Pharmacother. 2020, 130, 110629. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Wang, Y.; Sun, Q.; Knopf, J.; Herrmann, M.; Lin, L.; Jiang, J.; Shao, C.; Li, P.; He, X.; et al. Immune response in COVID-19: What is next? Cell Death Differ. 2022, 29, 1107–1122. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.L.; Suscovich, T.J.; Fortune, S.M.; Alter, G. Beyond binding: Antibody effector functions in infectious diseases. Nat. Rev. Immunol. 2018, 18, 46–61. [Google Scholar] [CrossRef] [PubMed]
- Kreuzberger, N.; Hirsch, C.; Chai, K.L.; Tomlinson, E.; Khosravi, Z.; Popp, M.; Neidhardt, M.; Piechotta, V.; Salomon, S.; Valk, S.J.; et al. SARS-CoV-2-neutralising monoclonal antibodies for treatment of COVID-19. Cochrane Database Syst. Rev. 2021, 9, CD013825. [Google Scholar] [CrossRef] [PubMed]
- Nation Institutes of Health Guidelines. Clinical Spectrum of SARS-CoV-2 Infection. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 17 October 2022).
- Health Care Surveillance Authority. Available online: https://www.udzs-sk.sk/en/welcome-at-the-hcsa-web-site/ (accessed on 17 October 2022).
- Atyeo, C.; Fischinger, S.; Zohar, T.; Slein, M.D.; Burke, J.; Loos, C.; McCulloch, D.J.; Newman, K.L.; Wolf, C.; Yu, J.; et al. Distinct early serological signatures track with SARS-CoV-2 survival. Immunity 2020, 53, 524–532. [Google Scholar] [CrossRef]
- Yan, X.; Chen, G.; Jin, Z.; Zhang, Z.; Zhang, B.; He, J.; Yin, S.; Huang, J.; Fan, M.; Li, Z.; et al. Anti-SARS-CoV-2 IgG levels in relation to disease severity of COVID-19. J. Med. Virol. 2022, 94, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.B.; Jarlhelt, I.; Pérez-Alós, L.; Landsy, L.H.; Loftager, M.; Rosbjerg, A.; Helgstrand, C.; Bjelke, J.R.; Egebjerg, T.; Jardine, J.G.; et al. SARS-CoV-2 antibody responses are correlated to disease severity in COVID-19 convalescent individuals. J. Immunol. 2021, 206, 109–117. [Google Scholar] [CrossRef]
- García-Abellán, J.; Padilla, S.; Fernández-González, M.; García, J.A.; Agulló, V.; Andreo, M.; Ruiz, S.; Galiana, A.; Gutiérrez, F.; Masiá, M. Antibody response to SARS-CoV-2 is associated with long-term clinical outcome in patients with COVID-19: A longitudinal study. J. Clin. Immunol. 2021, 41, 1490–1501. [Google Scholar] [CrossRef]
- Giamarellos-Bourboulis, E.J. Complex immune deregulation in severe COVID-19: More than a mechanism of pathogenesis. EBioMedicine 2021, 73, 103673. [Google Scholar] [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; et al. Dysregulation of immune response in patients with coronavirus 2019 (COVID-19) in Wuhan, China. Clin. Infect. Dis. 2020, 71, 762–768. [Google Scholar] [CrossRef]
- Pang, N.Y.-L.; Pang, A.S.-R.; Chow, V.T.; Wang, D.-Y. Understanding neutralising antibodies against SARS-CoV-2 and their implications in clinical practice. Mil. Med. Res. 2021, 8, 47. [Google Scholar] [CrossRef] [PubMed]
- Shirbhate, E.; Pandey, J.; Patel, V.K.; Kamal, M.; Jawaid, T.; Gorain, B.; Kesharwani, P.; Rajak, H. Understanding the role of ACE-2 receptor in pathogenesis of COVID-19 disease: A potential approach for therapeutic intervention. Pharmacol. Rep. 2021, 73, 1539–1550. [Google Scholar] [CrossRef] [PubMed]
- Ni, W.; Yang, X.; Yang, D.; Bao, J.; Li, R.; Xiao, Y.; Hou, C.; Wang, H.; Liu, J.; Yang, D.; et al. Role of angiotensin-converting enzyme 2 (ACE2) in COVID-19. Crit. Care 2020, 24, 422. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Dutta, S.; Xiong, S.; Chan, M.; Chan, K.K.; Fan, T.M.; Bailey, K.L.; Lindeblad, M.; Cooper, L.M.; Rong, L.; et al. Engineered ACE2 decoy mitigates lung injury and death induced by SARS-CoV-2 variants. Nat. Chem. Biol. 2022, 18, 342–351. [Google Scholar] [CrossRef] [PubMed]
- Qi, H.; Liu, B.; Wang, X.; Zhang, L. The humoral response and antibodies against SARS-CoV-2 infection. Nat. Immunol. 2022, 23, 1008–1020. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Badekar, P.; Kearsley, A.J.; Patrone, P.N. The production of immunoglobulins in COVID-19 usually starts within the first or second week of infection and peaks in 2 months. arXiv 2022, arXiv:2208.02127. [Google Scholar] [CrossRef]
- Latifi-Pupovci, H.; Namani, S.; Pajaziti, A.; Ahmetaj-Shala, B.; Ajazaj, L.; Kotori, A.; Haxhibeqiri, V.; Gegaj, V.; Bunjaku, G. Relationship of anti-SARS-CoV-2 IgG antibodies with Vitamin D and inflammatory markers in COVID-19 patients. Sci. Rep. 2022, 12, 5699. [Google Scholar] [CrossRef]
- Hoffman, T.; Kolstad, L.; Rönnberg, B.; Lundkvist, Å. Evaluation of production lots of a rapid point-of-care lateral flow serological test intended for identification of IgM and IgG against the N-terminal part of the spike protein (S1) of SARS-CoV-2. Viruses 2021, 13, 1043. [Google Scholar] [CrossRef]
- Dellière, S.; Salmona, M.; Minier, M.; Gabassi, A.; Alanio, A.; Le Goff, J.; Delaugerre, C.; Chaix, M.-L. Evaluation of the COVID-19 IgG/IgM Rapid Test from Orient Gene Biotech. J. Clin. Microbiol. 2020, 58, e01233-20. [Google Scholar] [CrossRef]
- Nakayama, E.E.; Kubota-Koketsu, R.; Sasaki, T.; Suzuki, K.; Uno, K.; Shimizu, J.; Okamoto, T.; Matsumoto, H.; Matsuura, H.; Hashimoto, S.; et al. Anti-nucleocapsid antibodies enhance the production of IL-6 induced by SARS-CoV-2 N protein. Sci. Rep. 2022, 12, 8108. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Garcia, J.L.; Sanchez-Nievas, G.; Arevalo-Serrano, J.; Garcia-Gomez, C.; Jimenez-Vizuete, J.M.; Martinez-Alfaro, E. Baricitinib improves respiratory function in patients treated with corticosteroids for SARS-CoV-2 pneumonia: An observational cohort study. Rheumatology 2021, 60, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Octavius, G.S.; Wijaya, J.H.; Tan, A.O.; Muljono, M.P.; Chandra, S.; Juliansen, A. Autopsy findings of pediatric COVID-19: A systematic review. Egypt. J. Forensic Sci. 2022, 12, 32. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Anti-SARS-CoV-2 Ig Positive n = 330 | Anti-SARS-CoV-2 Ig Negative n = 224 | p-Value | ||
|---|---|---|---|---|
| Age (years) | 60.49 ± 13.71 | 61.11 ± 14.03 | 0.607 | |
| BMI (kg/m2) | 30 (26–33) | 30 (27–35) | 0.218 | |
| CRP (mg/L) | 106 (48–161) | 82 (40–128) | 0.018 | |
| IL-6 (pg/mL) | 58 (27–101) | 56 (27–87) | 1.000 | |
| N/L ratio | 6 (4–10) | 5 (3–9) | 0.071 | |
| GFR (mL/min) | 64 (48–75) | 60 (44–71) | 0.768 | |
| D-dimer (mg/L) | 1.00 (1.00–3.00) | 1.00 (0.00–1.00) | 0.011 | |
| Duration of symptoms to admission (days) | 9 (6–11) | 7 (4–9) | 0.0001 | |
| Hospitalisation length (days) | 9 (6–14) | 11 (7–5) | 0.01 | |
| Length of follow-up (months) | 21 (20–25) | 21 (20–23) | 0.388 | |
| Number of comorbidities * | 1 (0, 2) | 1 (0, 2) | 0.566 | |
| Survival in deceased patients (Days) | 59 (14–412) | 160 (24–312) | 0.704 | |
| Categorical variables | Yes | anti-SARS-CoV-2 Ig positive, n/n-total (%) | anti-SARS-CoV-2 Ig negative, n (%) | p-value (chi-square) |
| No | ||||
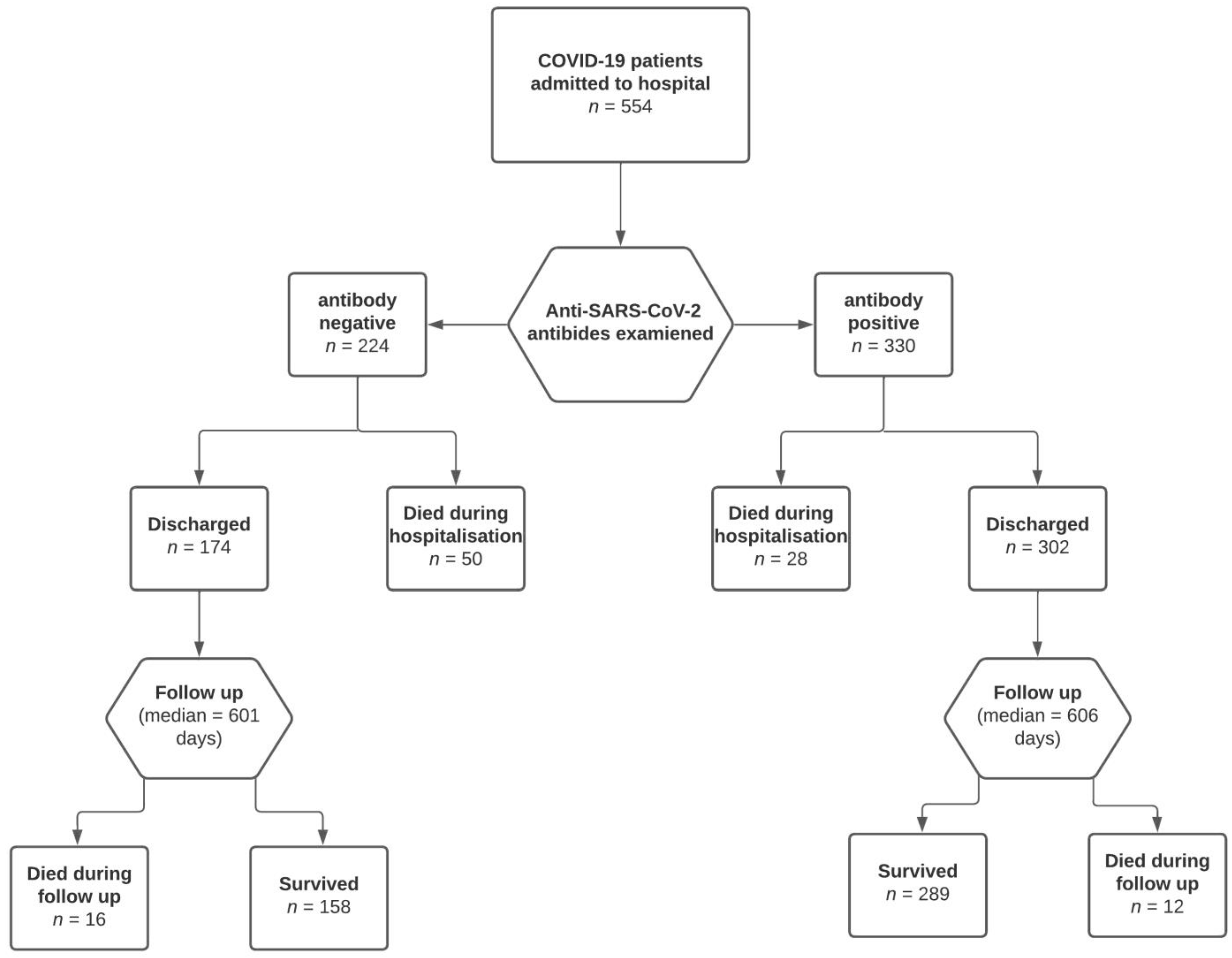
| Death during hospitalisation | Yes | 28/330 (8.5%) | 50/224 (22.3%) | 0.0001 |
| No | 302/330 (91.5%) | 174/224 (77.7%) | ||
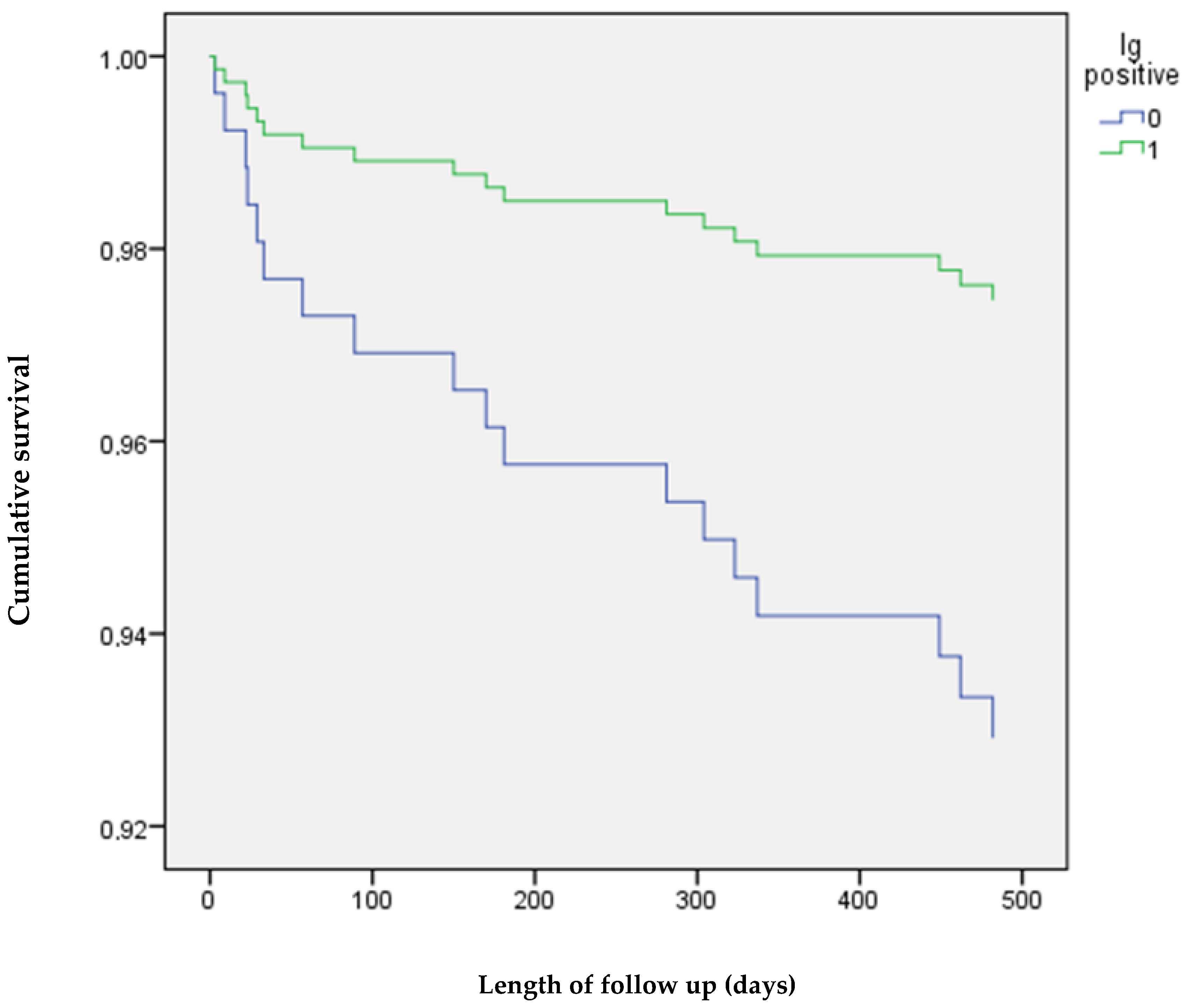
| Death after discharge | Yes | 12/330 (3.6%) | 16/224 (7.1%) | 0.030 |
| No | 318/330 (96.4) | 208/224 (92.9%) | ||
| Mechanical ventilation | Yes | 13/330 (3.9%) | 23/224 (10.3%) | 0.004 |
| No | 317/330 (96.1%) | 201/224 (89.7%) | ||
| Intensive care unit | Yes | 64/330 (19.4%) | 60/224 (26.8%) | 0.048 |
| No | 226/330 (68.5%) | 164/224 (73.2%) | ||
| Male gender | Yes | 197/330 (59.7%) | 133/224 (59.4%) | 0.930 |
| No | 133/330 (40.3%) | 91/224 (40.4%) | ||
| Diabetes mellitus | Yes | 62/330 (18.8%) | 39/224 (17.4%) | 0.737 |
| No | 268/330 (81.2%) | 185/224 (82.6%) | ||
| Arterial hypertension | Yes | 178/330 (53.9%) | 77/224 (54.9%) | 0.862 |
| No | 152/330 (46.1%) | 147/224 (65.6%) | ||
| MI history | Yes | 26/330 (7.9%) | 21/224 (9.4%) | 0.539 |
| No | 304/330 (92.1%) | 203/224 (90.6%) | ||
| Stroke history | Yes | 11/330 (3.3%) | 14/224 (6.3%) | 0.143 |
| No | 319/330 (97.7%) | 210/224 (93.7%) | ||
| Atrial fibrillation | Yes | 19/330 (5.8%) | 18/224 (8.1%) | 0.304 |
| No | 311/330 (94.2%) | 206/224 (91.9%) | ||
| Asthma | Yes | 26/330 (7.9%) | 22/224 (9.8%) | 0.445 |
| No | 304/330 (92.1%) | 202/224 (90.2%) | ||
| COPD | Yes | 8/330 (2.4%) | 11/224 (4.9%) | 0.153 |
| No | 322/330 (97.6%) | 213/224 (95.1%) | ||
| CKD G4/G5 | Yes | 22/330 (6.7%) | 13/224 (5.7%) | 0.701 |
| No | 308/330 (93.3%) | 209/224 (93.3%) | ||
| Baricitinib | Yes | 97/330 (29.4%) | 92/224 (41.1%) | 0.003 |
| No | 295/330 (89.4%) | 132/224 (58.9%) | ||
| COVID Severity † | ||
|---|---|---|
| Anti-SARS-CoV-2 Ig Positive, n/n-Total (%) | Anti-SARS-CoV-2 Ig Negative, n/n-Total (%) | |
| Moderate illness | 52/330 (15.8%) | 32/224 (14.3%) |
| Severe illness | 268/330 (81.2%) | 174/224 (77.7%) |
| Critical illness | 10/330 (3%) | 18/224 (8%) |
| 0.030 | ||
| p-Value | OR | 95% CI | |
|---|---|---|---|
| Anti-S SARS-CoV-2 negative | 0.0001 | 3.800 | 1.844–7.829 |
| Critical disease | 0.0001 | 7.460 | 2.475–22.222 |
| Number of comorbidities (n) | 0.002 | 1.664 | 1.197–2.312 |
| Age (years) | 0.001 | 1.063 | 1.026–1.101 |
| D-dimer (mg/L) | 0.043 | 1.099 | 1.003–1.204 |
| Binary regression model for separate anti-SARS-CoV-2 IgM | |||
| p-value | OR | 95% CI | |
| Anti-S SARS-CoV-2 IgM negative | 0.0001 | 4.542 | 2.126–9.706 |
| Critical disease | 0.001 | 6.757 | 2.257–20.000 |
| Number of comorbidities (n) | 0.003 | 1.649 | 1.179–2.305 |
| Age (years) | 0.002 | 1.056 | 1.020–1.094 |
| D-dimer (mg/L) | 0.051 | 1.096 | 1.000–1.202 |
| N/L ratio | 0.045 | 1.043 | 1.001–1.086 |
| Binary regression model for separate anti-SARS-CoV-2 IgG | |||
| p-value | OR | 95% CI | |
| Anti-S SARS-CoV-2 IgG negative | 0.005 | 2.983 | 1.393–6.388 |
| Critical disease | 0.0001 | 9.434 | 3.165–27.778 |
| Number of comorbidities (n) | 0.042 | 1.099 | 1.003–1.203 |
| Age (years) | 0.0001 | 1.067 | 1.031–1.105 |
| D-dimer (mg/L) | 0.003 | 1.657 | 1.188–2.310 |
| p-Value | OR | 95% CI | |
|---|---|---|---|
| Anti-S SARS-CoV-2 negative | 0.030 | 2.863 | 1.110–7.386 |
| Age (years) | 0.024 | 1.048 | 1.006–1.092 |
| Cox regression model for separate anti-SARS-CoV-2 IgM | |||
| p-value | OR | 95% CI | |
| Anti-S SARS-CoV-2 IgM negative | 0.038 | 2.728 | 1.057–7.039 |
| Age (years) | 0.028 | 1.046 | 1.005–1.089 |
| Cox regression model for separate anti-SARS-CoV-2 IgG | |||
| Anti-S SARS-CoV-2 IgM negative | 0.033 | 3.369 | 1.105–10.270 |
| Age (years) | 0.016 | 1.052 | 1.009–1.097 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jurenka, J.; Nagyová, A.; Dababseh, M.; Mihalov, P.; Stankovič, I.; Boža, V.; Kravec, M.; Palkovič, M.; Čaprnda, M.; Sabaka, P. Anti-SARS-CoV-2 Antibody Status at the Time of Hospital Admission and the Prognosis of Patients with COVID-19: A Prospective Observational Study. Infect. Dis. Rep. 2022, 14, 1004-1016. https://doi.org/10.3390/idr14060100
Jurenka J, Nagyová A, Dababseh M, Mihalov P, Stankovič I, Boža V, Kravec M, Palkovič M, Čaprnda M, Sabaka P. Anti-SARS-CoV-2 Antibody Status at the Time of Hospital Admission and the Prognosis of Patients with COVID-19: A Prospective Observational Study. Infectious Disease Reports. 2022; 14(6):1004-1016. https://doi.org/10.3390/idr14060100
Chicago/Turabian StyleJurenka, Ján, Anna Nagyová, Mohammad Dababseh, Peter Mihalov, Igor Stankovič, Vladimír Boža, Marián Kravec, Michal Palkovič, Martin Čaprnda, and Peter Sabaka. 2022. "Anti-SARS-CoV-2 Antibody Status at the Time of Hospital Admission and the Prognosis of Patients with COVID-19: A Prospective Observational Study" Infectious Disease Reports 14, no. 6: 1004-1016. https://doi.org/10.3390/idr14060100
APA StyleJurenka, J., Nagyová, A., Dababseh, M., Mihalov, P., Stankovič, I., Boža, V., Kravec, M., Palkovič, M., Čaprnda, M., & Sabaka, P. (2022). Anti-SARS-CoV-2 Antibody Status at the Time of Hospital Admission and the Prognosis of Patients with COVID-19: A Prospective Observational Study. Infectious Disease Reports, 14(6), 1004-1016. https://doi.org/10.3390/idr14060100