Autism, Therapy and COVID-19

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures and Tasks
2.2.1. ADOS 2—Toddler Module
2.2.2. ADI-R (Autism Diagnostic Interview-Revised)
2.2.3. Vineland II (Vineland Adaptive Behavior Scales II, VABS-II)
2.2.4. Questionnaire
3. Procedures
4. Methods
5. Results
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; Edizione italiana: Manuale diagnostico e statistico dei disturbi mentali, Raffaello Cortina; American Psychiatric Association Publishing: Arlington, VA, USA, 2013. [Google Scholar]
- Woods, J.J.; Wetherby, A.M. Early identification of and intervention for infants and toddlers who are at risk for autism spectrum disorder. Lang. Speech Hear. Serv. Sch. 2003, 34, 180–193. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Prevalence of autism spectrum disorder among children aged 8 years-Autism and developmental disabilities monitoring network, 11 sites, United States, 2010. MMWR Surveill. Summ. 2014, 63, 1–21. [Google Scholar]
- Christensen, D.L.; Baio, J.; Van Naarden Braun, K.; Bilder, D.; Charles, J.; Constantino, J.N.; Daniels, J.; Durkin, M.S.; Fitzgerald, R.T.; Kurzius-Spencer, M.; et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years—Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2012. MMWR Surveill. Summ. 2018, 65, 1–23. [Google Scholar] [CrossRef]
- Lovaas, O.I. Behavioral treatment and normal educational and intellectual functioning in young autistic children. J. Consult Clin. Psychol. 1987, 55, 3–9. [Google Scholar] [CrossRef]
- Matson, J.L.; Benavidez, D.A.; Compton, L.S.; Paclawskyj, T.; Baglio, C. Behavioral treatment of autistic persons: A review of research from 1980 to the present. Res. Dev. Disabil. 1996, 17, 433–465. [Google Scholar] [CrossRef]
- McGee, G.G.; Krantz, P.J.; Mason, D.; McClannahan, L.E. A modified incidental teaching procedure for autistic youth. J. Appl. Behav. Anal. 1983, 16, 329–338. [Google Scholar] [CrossRef] [Green Version]
- Koegel, R.L.; Koegel, L.K. Pivotal Response Treatments for Autism: Communication, Social & Academic Development; Paul H Brookes Publishing: Baltimore, MD, USA, 2006. [Google Scholar]
- Koegel, R.L.; O’Dell, M.C.; Koegel, L.K. A natural language teaching paradigm for nonverbal autistic children. J. Autism Dev. Disord. 1987, 17, 187–200. [Google Scholar] [CrossRef]
- Laski, K.E.; Charlop, M.H.; Schreibman, L. Training parents to use the natural language paradigm to increase their autistic children’s speech. J. Appl. Behav. Anal. 1988, 21, 391–400. [Google Scholar] [CrossRef] [Green Version]
- Schreibman, L.; Koegel, R.L. Training for parents of children with autism: Pivotal responses, generalization, and individualization of interventions. In Psychosocial Treatment for Child and Adolescent Disorders: Empirically Based Strategies for Clinical Practice, 2nd ed.; Hibbs, E.D., Jensen, P.S., Eds.; American Psychological Association: Washington, DC, USA, 2005; pp. 605–631. [Google Scholar]
- Dawson, G.; Rogers, S.; Munson, J.; Smith, M.; Winter, J.; Greenson, J.; Donaldson, A.; Varley, J. Randomized, controlled trial of an intervention for toddlers with autism: The Early Start Denver Model. Pediatrics 2010, 125, 17–23. [Google Scholar] [CrossRef] [Green Version]
- Dawson, G.; Bernier, R.; Ring, R.H. Social attention: A possible early indicator of efficacy in autism clinical trials. J. Neurodev. Disord. 2012, 4, 11. [Google Scholar] [CrossRef] [Green Version]
- Rogers, S.J.; Dawson, G. Early Start Denver Model for Young Children with Autism: Promoting Language, Learning and Engagement; The Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Rogers, S.J.; Dawson, G.; Vismara, L. An Early Start for Your Child with Autism: Using Everyday Activities to Help Kids Connect, Communicate, and Learn; The Guilford Press: New York, NY, USA, 2012. [Google Scholar]
- U.S. Department of Health and Human Services. Mental Health: A Report of the Surgeon General; US Department of Health and Human Services; Substance Abuse and Mental Health Services Administration; Center for Mental Health Services; National Institutes of Health; National Institute of Mental Health: Rockville, MD, USA, 2006.
- New York State Department of Health. Clinical Practice Guideline: The Guideline Technical Report. Autism/Pervasive Development Disorders, Assessment and Intervention for Young Children (Age 0–3 Years). Publication No. 4217; 1999. Available online: http://www.health.ny.gov/publications/4219.pdf (accessed on 10 July 2020).
- National Academy of Sciences. Educating Children with Autism; Commission on Behavioral and Social Sciences and Education: Washington, DC, USA, 2001. [Google Scholar]
- Luyster, R.; Gotham, K.; Guthrie, W.; Coffing, M.; Petrak, R.; Pierce, K.; Bishop, S.; Esler, A.; Hus, V.; Oti, R.; et al. The Autism Diagnostic Observation Schedule—Toddler Module: A new module of a standardized diagnostic measure for autism spectrum disorders. J. Autism Dev. Disord. 2009, 39, 1305–1320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rutter, M.; Le Couteur, A.; Lord, C. Autism Diagnostic Interview-Revised; Western Psychological Services: Los Angeles, CA, USA, 2003; Volume 29, p. 30. [Google Scholar]
- Sparrow, S.S.; Cicchetti, V.D.; Balla, A.D. Vineland Adaptive Behavior Scales, 2nd ed.; American Guidance Service: Circle Pines, MN, USA, 2005. [Google Scholar]
- IBM (2019) to Acquire SPSS Inc. to Provide Clients Predictive Analytics Capabilities. in ibm.com, 28 luglio 2009. Available online: https://www-03.ibm.com/press/us/en/pressrelease/27936.wss (accessed on 5 August 2020).
- Granpeesheh, D.; Tarbox, J.; Dixon, D.R. Applied behavior analytic interventions for children with autism: A description and review of treatment research. Ann. Clin. Psychiatry 2009, 21, 162–173. [Google Scholar] [PubMed]
- McEachin, J.J.; Smith, T.; Lovaas, O.I. Long term outcome for children with autism who received early intensive behavioral treatment. Am. J. Ment. Retard. 1993, 97, 359. [Google Scholar] [PubMed]
- Rosenwasser, B.; Axelrod, S. The contribution of applied behavior analysis to the education of people with autism. Behav. Modif. 2001, 25, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Sallows, G.O.; Graupner, T.D. Intensive Behavioral Treatment for Children with Autism: Four Year Outcome and Predictors. Am. J. Ment. Retard. 2005, 110, 417–438. [Google Scholar] [CrossRef]
- Smith, T.; Groen, A.D.; Wynn, J.W. Randomized trial of intensive early intervention for children with pervasive developmental disorder. Am. J. Ment. Retard. 2000, 105, 269–285. [Google Scholar] [CrossRef]
- Eldevik, S.; Eikeseth, S.; Jahr, E.; Smith, T. Effects of low intensity behavioral treatment for children with autism and mental retardation. J. Autism Dev. Disord. 2006, 36, 211–224. [Google Scholar] [CrossRef]
- Reed, P.; Osborne, L.A.; Corness, M. Brief report: Relative effectiveness of different home-based behavioral approaches to early teaching intervention. J. Autism Dev. Disord. 2006, 37, 1815–1821. [Google Scholar] [CrossRef]
- Sheinkopf, S.J.; Siegel, B. Home-based behavioral treatment of young children with autism. J. Autism Dev. Disord. 1998, 28, 15–23. [Google Scholar] [CrossRef]
- Eikeseth, S.; Smith, T.; Jahr, E.; Eldevik, S. Intensive behavioral treatment at school for 4- to 7-year-old children with autism: A one-year comparison controlled study. Behav. Modif. 2002, 26, 49–68. [Google Scholar] [CrossRef]
- Howard, J.S.; Sparkman, C.R.; Cohen, H.G.; Green, G.; Stanislaw, H. A comparison of intensive behavior analytic and eclectic treatments for young children with autism. Res. Dev. Disabil. 2005, 26, 359–383. [Google Scholar] [CrossRef] [PubMed]
- Zachor, D.A.; Ben-Itzchak, E.; Rabinovich, A.-L.; Lahat, E. Change in autism core symptoms with intervention. Res. Autism Spectr. Disord. 2007, 1, 304–317. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
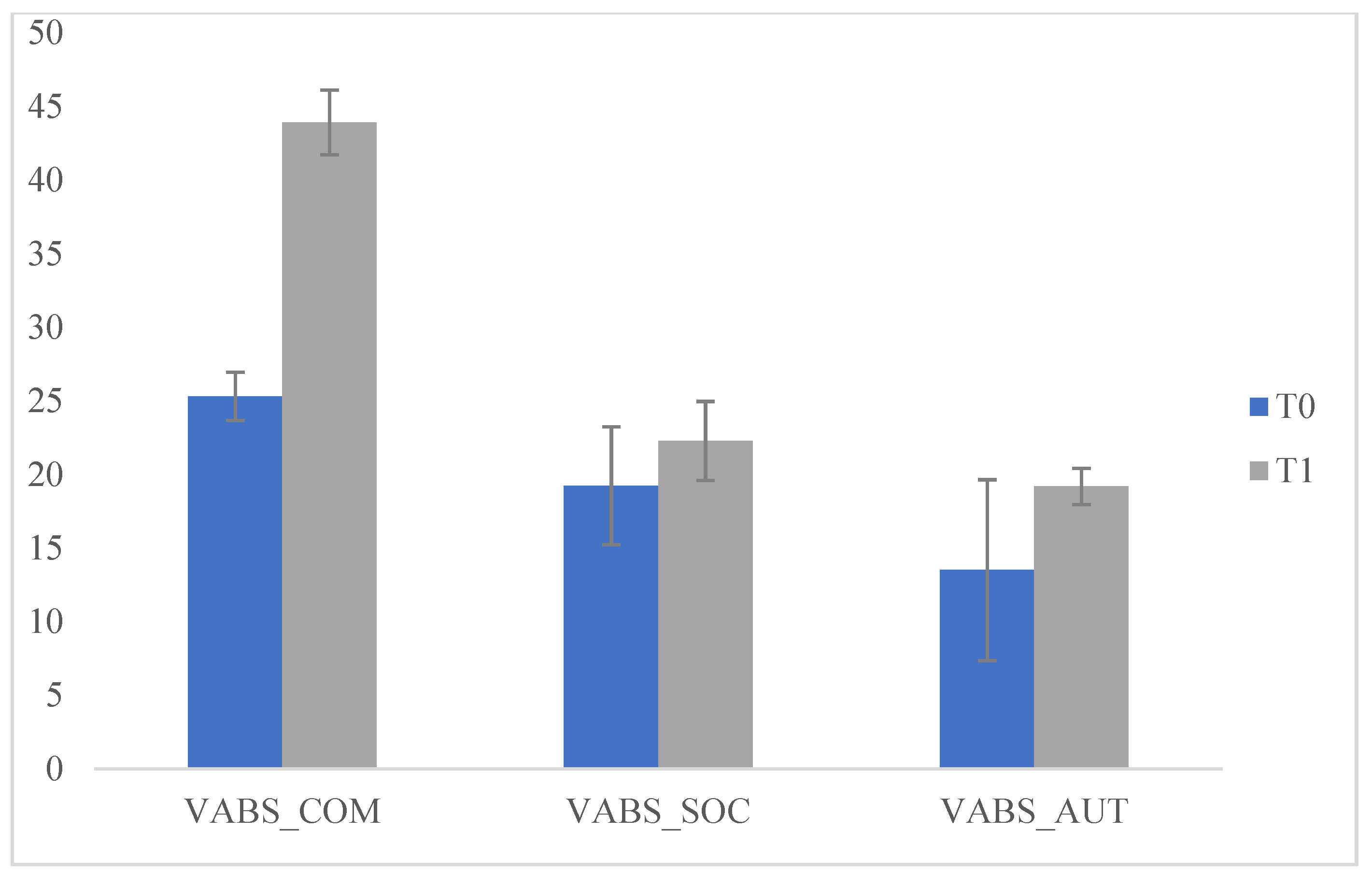
| T0 | T1 | |||||
|---|---|---|---|---|---|---|
| Means | SD | Means | SD | f | p | |
| VABS_COM | 25.31 | 1.65 | 43.92 | 2.20 | 3999.877 | 0.000 * |
| VABS_SOC | 19.24 | 4.01 | 22.28 | 2.69 | 34.912 | 0.000 * |
| VABS_AUT | 13.50 | 6.15 | 19.19 | 1.24 | 72.268 | 0.000 * |
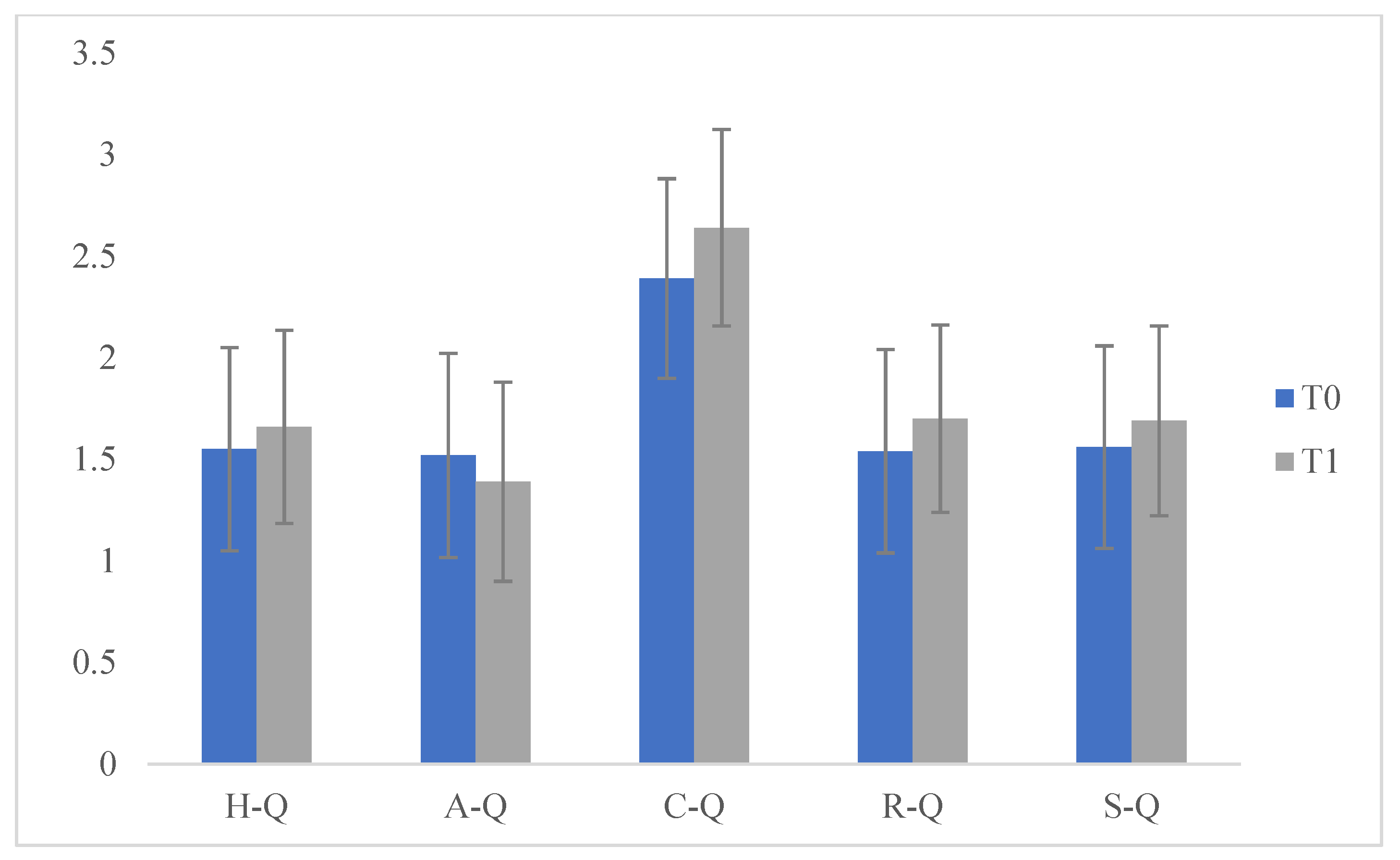
| H-Q | 1.55 | 0.500 | 1.66 | 0.475 | 2.286 | 0.132 |
| A-Q | 1.52 | 0.503 | 1.39 | 0.491 | 2.739 | 0.100 |
| C-Q | 2.39 | 0.491 | 2.64 | 0.483 | 11.578 | 0.001 * |
| R-Q | 1.54 | 0.501 | 1.70 | 0.462 | 4.633 | 0.033 |
| S-Q | 1.56 | 0.499 | 1.69 | 0.467 | 2.815 | 0.095 |
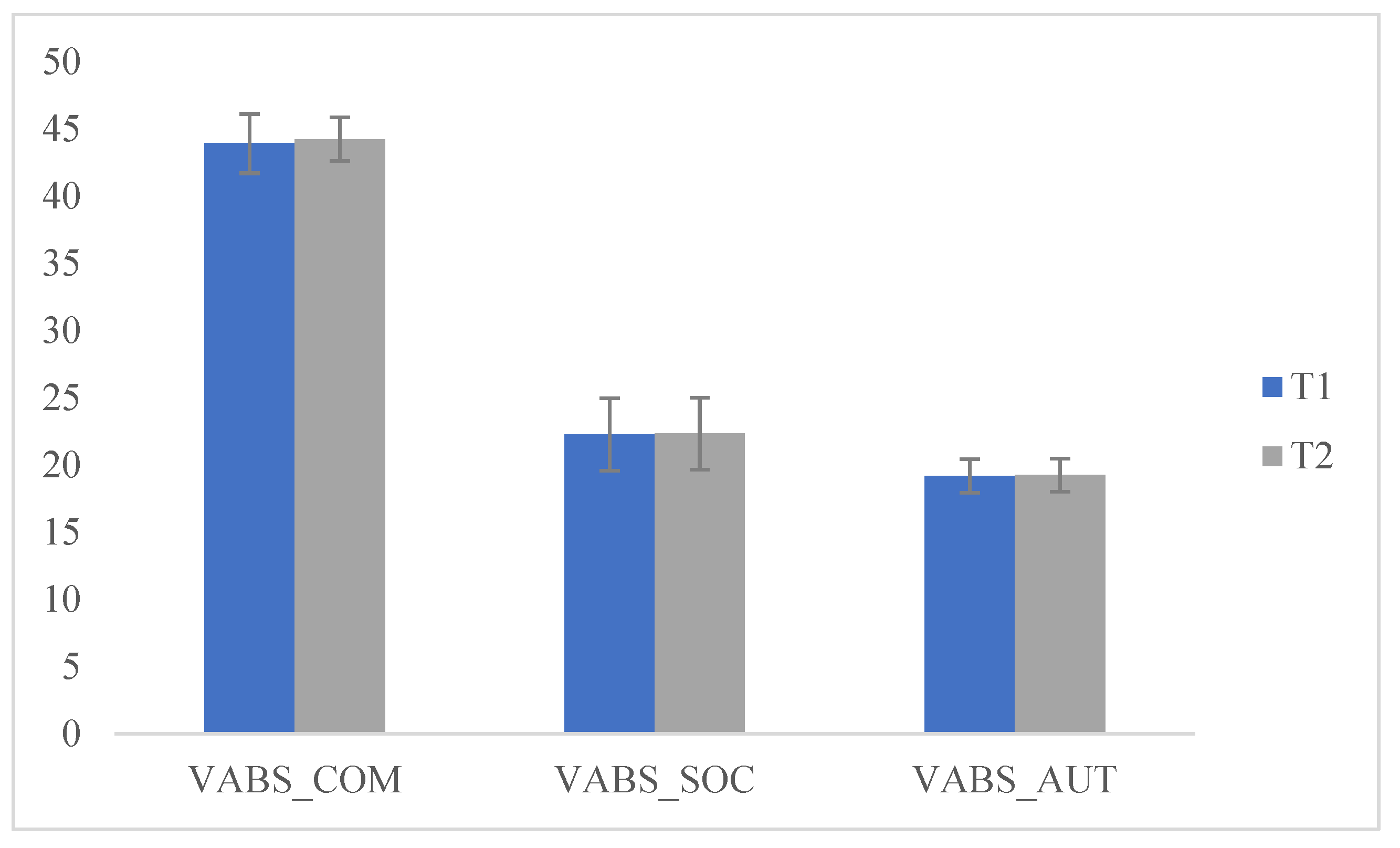
| T1 | T2 | |||||
|---|---|---|---|---|---|---|
| Means | SD | Means | SD | f | p | |
| VABS_COM | 43.92 | 2.20 | 44.23 | 1.62 | 1.102 | 0.295 |
| VABS_SOC | 22.28 | 2.69 | 22.33 | 2.67 | 0.013 | 0.911 |
| VABS_AUT | 19.19 | 1.24 | 19.25 | 1.24 | 0.091 | 0.763 |
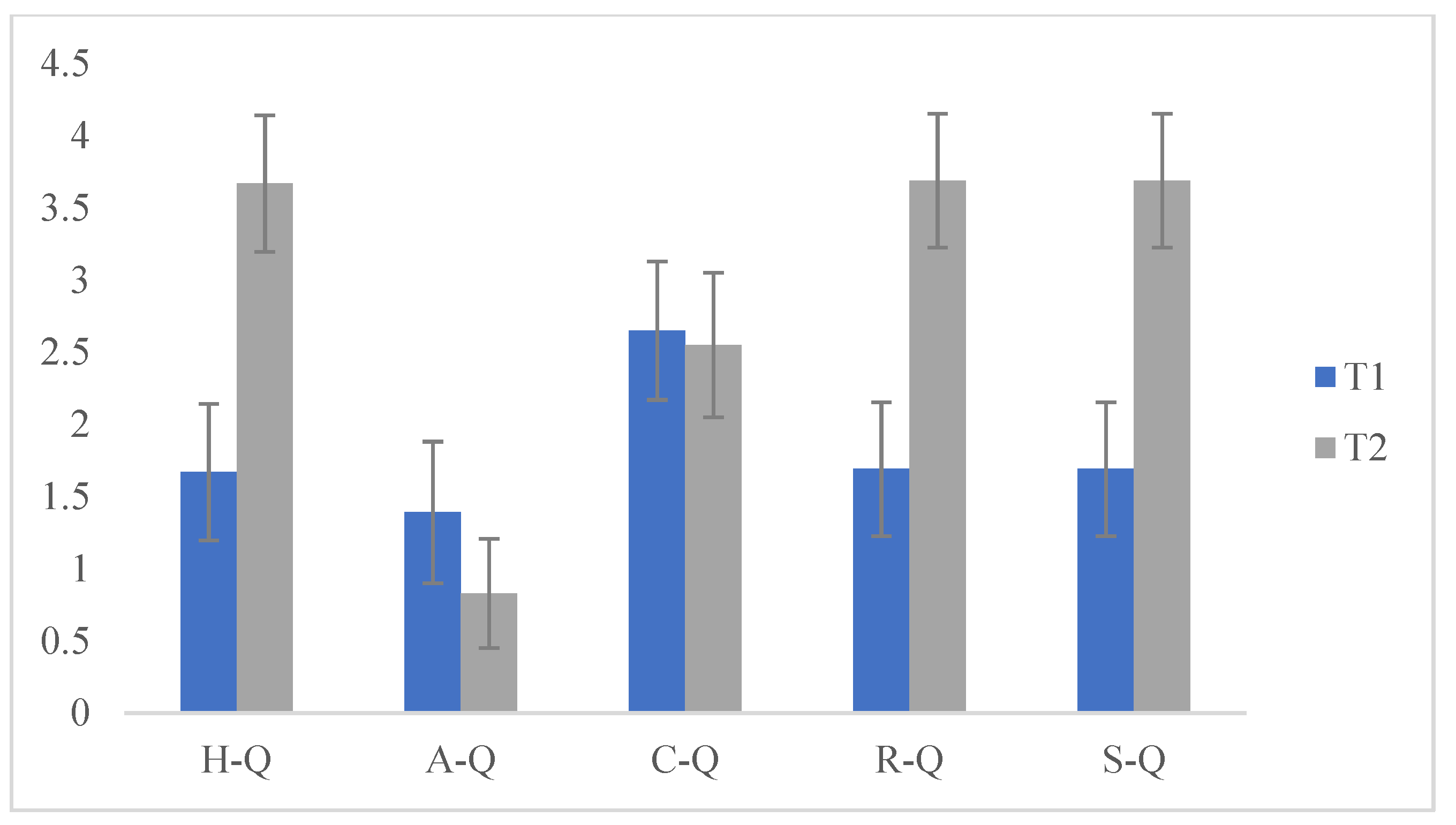
| H-Q | 1.67 | 0.473 | 3.67 | 0.473 | 787.525 | 0.000 * |
| A-Q | 1.39 | 0.490 | 0.83 | 0.378 | 71.268 | 0.000 * |
| C-Q | 2.65 | 0.480 | 2.55 | 0.501 | 1.911 | 0.169 |
| R-Q | 1.69 | 0.464 | 3.69 | 0.464 | 818.128 | 0.000 * |
| S-Q | 1.69 | 0.464 | 3.69 | 0.464 | 818.128 | 0.000 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sergi, L.; Mingione, E.; Ricci, M.C.; Cavallaro, A.; Russo, F.; Corrivetti, G.; Operto, F.F.; Frolli, A. Autism, Therapy and COVID-19. Pediatr. Rep. 2021, 13, 35-44. https://doi.org/10.3390/pediatric13010005
Sergi L, Mingione E, Ricci MC, Cavallaro A, Russo F, Corrivetti G, Operto FF, Frolli A. Autism, Therapy and COVID-19. Pediatric Reports. 2021; 13(1):35-44. https://doi.org/10.3390/pediatric13010005
Chicago/Turabian StyleSergi, Luana, Emanuele Mingione, Maria Carla Ricci, Antonella Cavallaro, Ferdinando Russo, Giulio Corrivetti, Francesca Felicia Operto, and Alessandro Frolli. 2021. "Autism, Therapy and COVID-19" Pediatric Reports 13, no. 1: 35-44. https://doi.org/10.3390/pediatric13010005
APA StyleSergi, L., Mingione, E., Ricci, M. C., Cavallaro, A., Russo, F., Corrivetti, G., Operto, F. F., & Frolli, A. (2021). Autism, Therapy and COVID-19. Pediatric Reports, 13(1), 35-44. https://doi.org/10.3390/pediatric13010005