
Parental Knowledge and Awareness about Shaken Baby Syndrome in Jeddah, Saudi Arabia: A Cross-Sectional Study

 , , ,
, , ,
Abstract
:1. Introduction
Subjects and Methods
2. Results
2.1. Sociodemographic Characteristics
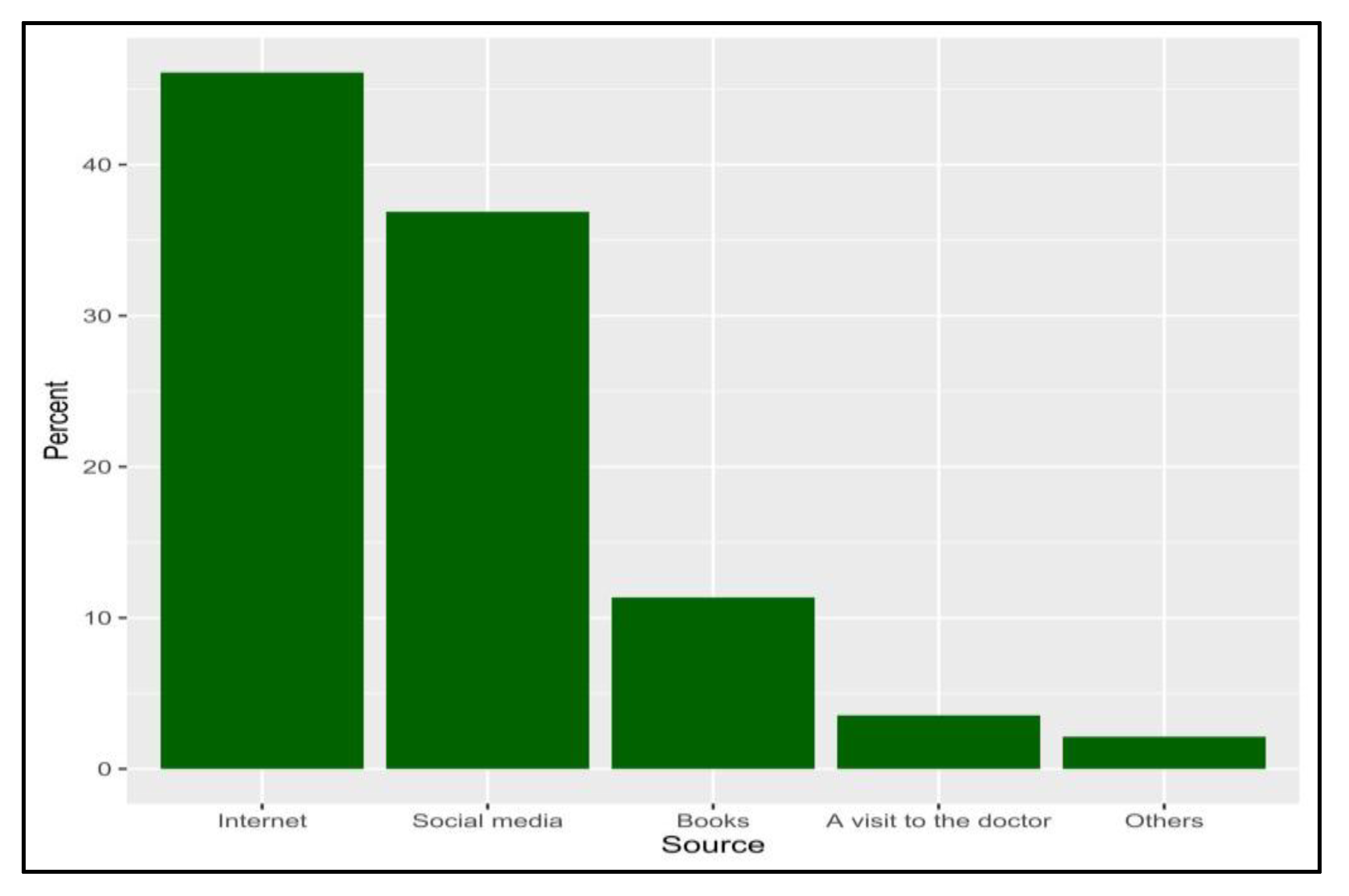
2.2. Description of Knowledge-Related Variables
2.3. Attitudes towards Shaken Baby Syndrome
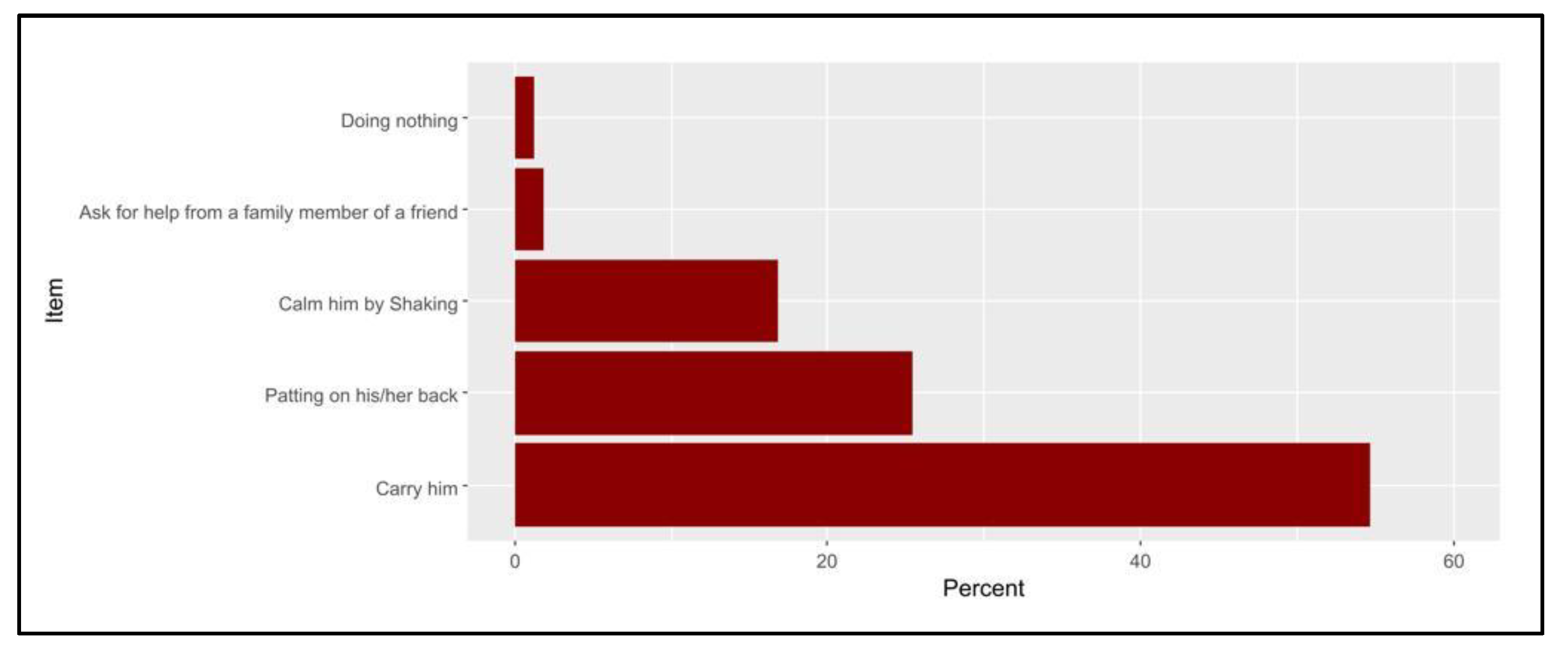
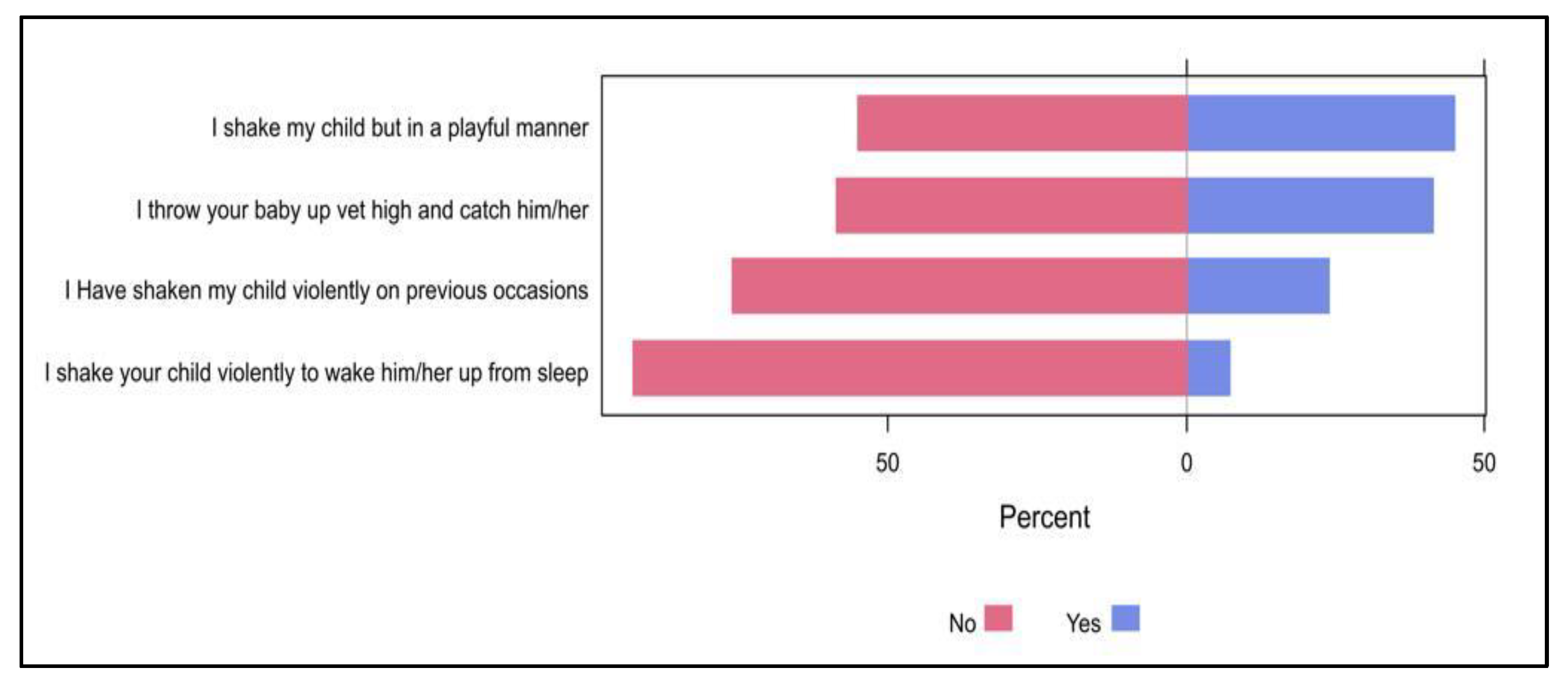
2.4. Practice towards Shaken Baby Syndrome
3. Discussion
4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Christian, C.W.; Block, R. Abusive head trauma in infants and children. Pediatrics 2009, 123, 1409–1411. [Google Scholar] [CrossRef]
- Stewart, T.C.; Polgar, D.; Gilliland, J.; Tanner, D.A.; Girotti, M.J.; Parry, N.; Fraser, D.D. Shaken baby syndrome and a triple dose strategy for its prevention. J. Trauma 2011, 71, 1801–1807. [Google Scholar] [CrossRef]
- Ludwig, S.; Warman, M. Shaken baby syndrome: A review of 20 cases. Ann. Emerg. Med. 1984, 13, 104–107. [Google Scholar] [CrossRef]
- Lopes, N.R.; Eisenstein, E.; Williams, L.C. Abusive head trauma in children: A literature review. J. Pediatr. 2013, 89, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Minns, R.A.; Jones, P.A.; Mok, J.Y.Q. Incidence and demography of non-accidental head injury in southeast Scotland from a national database. Am. J. Prev. Med. 2008, 34, S126–S133. [Google Scholar] [CrossRef] [PubMed]
- Kelly, P.; Farrant, B. Shaken baby syndrome in New Zealand, 2000–2002. J. Paediatr. Child Health 2008, 44, 99–107. [Google Scholar] [CrossRef]
- Gilbert, R.; Kemp, A.; Thoburn, J.; Sidebotham, P.; Radford, L.; Glaser, D.; MacMillan, H.L. Recognising and responding to child maltreatment. Lancet 2009, 373, 167–180. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, T.; Yamaoka, Y.; Morisaki, N. Self-Reported Prevalence and Risk Factors for Shaking and Smothering Among Mothers of 4-Month-Old Infants in Japan. J. Epidemiol. 2016, 26, 4–13. [Google Scholar] [CrossRef]
- Adamsbaum, C.; Grabar, S.; Mejean, N.; Rey-Salmon, C. Abusive head trauma: Judicial admissions highlight violent and repetitive shaking. Pediatrics 2010, 126, 546–555. [Google Scholar] [CrossRef] [PubMed]
- Radesky, J.S.; Zuckerman, B.; Silverstein, M.; Rivara, F.P.; Barr, M.; Taylor, J.A.; Lengua, L.J.; Barr, R.G. Inconsolable infant crying and maternal postpartum depressive symptoms. Pediatrics 2013, 131, e1857–e1864. [Google Scholar] [CrossRef]
- Miehl, N.J. Shaken baby syndrome. J. Forensic Nurs. 2005, 1, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.M. A case of shaken baby syndrome after discharge from the newborn intensive care unit. Adv. Neonatal Care 2005, 5, 135–146. [Google Scholar] [CrossRef] [PubMed]
- Black, D.A.; Heyman, R.E.; Slep, A.M.S. Risk factors for child physical abuse. Aggress. Violent Behav. 2001, 6, 121–188. [Google Scholar] [CrossRef]
- National Center for Injury Prevention and Control (USA); Centers for Disease Control and Prevention (USA). A Journalist’s Guide to Shaken Baby Syndrome: A Preventable Tragedy Centers for Disease Control and Prevention. 2010. Available online: www.cdc.gov (accessed on 4 February 2023).
- Berthold, O.; Clemens, V.; Witt, A.; Brähler, E.; Plener, P.L.; Fegert, J.M. Awareness of abusive head trauma in a German population-based sample: Implications for prevention. Pediatr. Res. 2019, 86, 537–541. [Google Scholar] [CrossRef] [PubMed]
- Foley, S.; Kovács, Z.; Rose, J.; Lamb, R.; Tolliday, F.; Simons-Coghill, M.; Stephens, A.; Scheiber, D.; Toma, A.; Asbóth, K.; et al. International collaboration on prevention of shaken baby syndrome–an ongoing project/intervention. Paediatr. Int. Child Health 2013, 33, 233–238. [Google Scholar] [CrossRef]
- Alshahrani, A.N.; Alshahrani, M.N.; Ahmed, A.B. Evaluation of knowledge regarding shaken baby syndrome among parents in Tabuk City. Egypt. J. Hosp. Med. 2018, 72, 5600–5603. [Google Scholar] [CrossRef]
- Alomran, H.I.; Alkharaan, Z.I.; Aldawsari, K.M.; Aldakkan, O.Z.; Alatif, H.M.; Mohamed, M.Z.E. Parental awareness, knowledge, and attitude about shaken baby syndrome in Riyadh, Saudi Arabia: A cross-sectional study. Pan Afr. Med. J. 2022, 41, 327–340. [Google Scholar] [CrossRef]
- American Academy of Pediatrics Committee on Child Abuse and Neglect Shaken baby syndrome: Rotational cranial injuries-technical report. Pediatrics 2001, 108, 206–210. [CrossRef]
- El Sayed, A.I.; Mohamed, S.A. Effect of Educational Materials on Mother’s Awareness, Knowledge and Behavior Regarding the Dangers of Shaken Baby Syndrome. IOSR J. Nurs. Health Sci. 2020, 9, 1–7. [Google Scholar]
- Mann, A.K.; Rai, B.; Sharif, F.; Vavasseur, C. Assessment of parental awareness of the shaken baby syndrome in Ireland. Eur. J. Pediatr. 2015, 174, 1339–1345. [Google Scholar] [CrossRef]
- Marcinkowska, U.; Tyrała, K.; Paniczek, M.; Ledwoń, M.; Jośko-Ochojska, J. Evaluation of knowledge regarding shaken baby syndrome among parents and medical staff. Minerva Pediatr. 2021, 73, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention; Prevention, National Center for Injury Prevention and Control. Preventing Shaken Baby Syndrome: A Guide for Health Departments and Community-Based Organizations; ErişimTarihi: Mayıs, Azerbaijan, 2013. Available online: www.cdc.gov/injury (accessed on 4 February 2023). [CrossRef]
- Bechtel, K.; Le, K.; Martin, K.; Shah, N.; Leventhal, J.; Colson, E. Impact of an educational intervention on caregivers’ beliefs about infant crying and knowledge of shaken baby syndrome. Acad. Pediatr. 2011, 11, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Simonnet, H.; Laurent-Vannier, A.; Yuan, W.; Hully, M.; Valimahomed, S.; Bourennane, M.; Chevignard, M. Parents’ behavior in response to infant crying: Abusive head trauma education. Child Abus. Negl. 2014, 38, 1914–1922. [Google Scholar] [CrossRef] [PubMed]
- Kelly, P.; Thompson, J.; Koh, J.; Ameratunga, S.; Jelleyman, T.; Percival, T.; Elder, H.; Mitchell, E.A. Perinatal risk and protective factors for pediatric abusive head trauma: A multicenter case-control study. J. Pediatr. 2017, 187, 240–246.e4. [Google Scholar] [CrossRef]
- Yildiz, D. Postpartum counseling needs and approaches of mothers regarding baby care. Gulhane Tip Jour 2008, 50, 294–298. [Google Scholar]
- Koc, F.; Aksit, S.; Turhan, T.; Ersahin, Y.; Tomba, A.; Halicioglu, O.; Aslan, A.; Koturoglu, G.; Aydin, C.; Cetin, S.; et al. Shaken baby syndrome: Case report. Turk. Klin. J. Med. Sci. 2012, 32, 1781–1785. [Google Scholar]
- Sahin, F.; Tasar, M.A. Shaken baby syndrome and prevention programme. Turk. Pediatry Arch. 2012, 47, 152–158. [Google Scholar]
- Crouch, J.L.; Hiraoka, R.; McCanne, T.R.; Reo, G.; Wagner, M.F.; Krauss, A.; Milner, J.S.; Skowronski, J.J. Heart Rate and Heart Rate Variability in Parents at Risk for Child Physical Abuse. J. Interpers. Violence 2018, 33, 1629–1652. [Google Scholar] [CrossRef]
- Abdulrazzaq, Y.M.; Al Kendi, A.; Nagelkerke, N. Soothing methods used to calm a baby in an Arab country. Acta Paediatr. 2009, 98, 392–396. [Google Scholar] [CrossRef]
- Howard, C.R.; Lanphear, N.; Lanphear, B.P.; Eberly, S.; Lawrence, R.A. Parental responses to infant crying and colic: The effect on breastfeeding duration. Breastfeed. Med. 2006, 1, 146–155. [Google Scholar] [CrossRef]
- Cansever, Z.; Tasar, M.A.; Sahin, F.; Camurdan, A.D.; Beyazova, U. Knowledge and attitudes of families about shaken baby syndrome. Gazi Med. J. 2012, 23, 39–45. [Google Scholar] [CrossRef]
- Susamma, T. Soothing Crying Babies and Preventing Shaken Baby Syndrome. Int. J. Nurs. Educ. 2016, 8, 34–38. [Google Scholar]
- Lekarski, P.; Talarowska, M.; Florkowski, A.; Mossakowska, J.; Gałecki, P. The shaken baby syndrome as a kind of domestic abuse. Polski Merkur. Lek. Organ Polskiego Towar. Lek 2010, 29, 70–73. [Google Scholar]
- Taşar, M.A.; Şahin, F.; Polat, S.; İlhan, M.; Çamurdan, A.; Dallar, Y.; Beyazova, U. Long-term outcomes of the shaken baby syndrome prevention program: Turkey’s experience. Turk. Arch. Pediatr. 2014, 49, 203–209. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Category | N (%) |
|---|---|---|
| Gender | Male | 73 (13.9%) |
| Female | 451 (86.1%) | |
| Age (years) | <20 | 14 (2.7%) |
| 20 to 29 | 142 (27.1%) | |
| 30 to 39 | 152 (29.0%) | |
| 40 or more | 216 (41.2%) | |
| Nationality | Saudi | 445 (84.9%) |
| Non-Saudi | 79 (15.1%) | |
| Marital status | Married | 429 (81.9%) |
| Divorced | 71 (13.5%) | |
| Widowed | 24 (4.6%) | |
| Educational level | High school or less | 101 (19.3%) |
| Diploma | 53 (10.1%) | |
| Bachelor’s | 315 (60.1%) | |
| Postgraduate | 55 (10.5%) | |
| Occupation | Employee | 260 (49.6%) |
| Non-employee | 76 (14.5%) | |
| Housewife | 188 (35.9%) | |
| Monthly income (SAR/USD) | <SAR 5000 (USD 1350) | 226 (43.1%) |
| SAR 5000 to 10,000 (USD 1350–2700) | 147 (28.1%) | |
| >SAR 10,000 (>USD 2700) | 151 (28.8%) | |
| Number of children | 1 to 5 | 366 (69.8%) |
| 5 to 7 | 128 (24.4%) | |
| >7 | 30 (5.7%) | |
| Have a chronically ill child at home | Yes | 56 (10.7%) |
| Have any mental disorders | None | 421 (80.3%) |
| Anxiety | 59 (11.3%) | |
| Depression | 20 (3.8%) | |
| Others | 24 (4.6%) |
| Parameter | Category | Knowledge Level | ||
|---|---|---|---|---|
| Poor, N = 109 | Good, N = 52 | p-Value | ||
| Gender | Male | 15 (75.0%) | 5 (25.0%) | 0.456 |
| Female | 94 (66.7%) | 47 (33.3%) | ||
| Age (years) | <20 | 2 (66.7%) | 1 (33.3%) | 0.762 |
| 20 to 29 | 25 (61.0%) | 16 (39.0%) | ||
| 30 to 39 | 39 (69.6%) | 17 (30.4%) | ||
| 40 or more | 43 (70.5%) | 18 (29.5%) | ||
| Nationality | Saudi | 91 (67.9%) | 43 (32.1%) | 0.900 |
| Non-Saudi | 18 (66.7%) | 9 (33.3%) | ||
| Marital status | Married | 86 (65.2%) | 46 (34.8%) | 0.155 |
| Divorced | 16 (72.7%) | 6 (27.3%) | ||
| Widowed | 7 (100.0%) | 0 (0.0%) | ||
| Educational level | High school or less | 23 (74.2%) | 8 (25.8%) | 0.134 |
| Diploma | 18 (85.7%) | 3 (14.3%) | ||
| Bachelor’s | 58 (63.7%) | 33 (36.3%) | ||
| Postgraduate | 10 (55.6%) | 8 (44.4%) | ||
| Occupation | Employee | 53 (61.6%) | 33 (38.4%) | 0.172 |
| Non-employee | 13 (81.2%) | 3 (18.8%) | ||
| Housewife | 43 (72.9%) | 16 (27.1%) | ||
| Monthly income (SAR/USD) | <SAR 5000 (USD 1350) | 46 (73.0%) | 17 (27.0%) | 0.371 |
| SAR 5000 to 10,000 (USD 1350–2700) | 34 (68.0%) | 16 (32.0%) | ||
| >SAR 10,000 (>USD 2700) | 29 (60.4%) | 19 (39.6%) | ||
| Number of children | 1 to 5 | 72 (63.7%) | 41 (36.3%) | 0.139 |
| 5 to 7 | 34 (79.1%) | 9 (20.9%) | ||
| >7 | 3 (60.0%) | 2 (40.0%) | ||
| Have a chronically ill child at home | 18 (75.0%) | 6 (25.0%) | ||
| Have any mental disorders | None | 84 (65.1%) | 45 (34.9%) | 0.347 |
| Anxiety | 15 (75.0%) | 5 (25.0%) | ||
| Depression | 4 (66.7%) | 2 (33.3%) | ||
| Others | 6 (100.0%) | 0 (0.0%) | ||
| Parameter | Category | N (%) |
|---|---|---|
| Want to know more about shaken baby syndrome | No | 84 (16.0%) |
| Yes | 440 (84.0%) | |
| If yes, from which source? | A doctor or medical staff during the vaccination period | 120 (28.6%) |
| Internet and social media | 156 (37.1%) | |
| Awareness campaign | 103 (24.5%) | |
| Medical books and bulletins | 41 (9.8%) | |
| Missing | 20 (4.5%) | |
| When is the preferred time period that you want to obtain information about shaken baby syndrome ¥ | Before pregnancy | 172 (40.1%) |
| During pregnancy | 147 (34.3%) | |
| A week after giving birth | 33 (7.7%) | |
| During vaccination visits to the child | 77 (17.9%) | |
| Missing | 11 (2.5%) |
| Parameter | Category | Attitude | ||
|---|---|---|---|---|
| Negative, N = 84 | Positive, N = 440 | p-Value | ||
| Gender | Male | 24 (32.9%) | 49 (67.1%) | <0.001 |
| Female | 60 (13.3%) | 391 (86.7%) | ||
| Age (years) | <20 | 1 (7.1%) | 13 (92.9%) | 0.502 |
| 20 to 29 | 21 (14.8%) | 121 (85.2%) | ||
| 30 to 39 | 30 (19.7%) | 122 (80.3%) | ||
| 40 or more | 32 (14.8%) | 184 (85.2%) | ||
| Nationality | Saudi | 64 (14.4%) | 381 (85.6%) | 0.015 |
| Non-Saudi | 20 (25.3%) | 59 (74.7%) | ||
| Marital status | Married | 55 (12.8%) | 374 (87.2%) | <0.001 |
| Divorced | 23 (32.4%) | 48 (67.6%) | ||
| Widow | 6 (25.0%) | 18 (75.0%) | ||
| Educational level | High school or less | 14 (13.9%) | 87 (86.1%) | 0.084 |
| Diploma | 15 (28.3%) | 38 (71.7%) | ||
| Bachelors | 47 (14.9%) | 268 (85.1%) | ||
| Postgraduate | 8 (14.5%) | 47 (85.5%) | ||
| Occupation | Employee | 42 (16.2%) | 218 (83.8%) | 0.776 |
| Non-employee | 14 (18.4%) | 62 (81.6%) | ||
| Housewife | 28 (14.9%) | 160 (85.1%) | ||
| Monthly income (SAR) | <5000 (SAR 1350) | 27 (11.9%) | 199 (88.1%) | 0.026 |
| 5000 to 10,000 (SAR 1350–2700) | 33 (22.4%) | 114 (77.6%) | ||
| >10,000 (>SAR 2700) | 24 (15.9%) | 127 (84.1%) | ||
| Number of children | 1 to 5 | 50 (13.7%) | 316 (86.3%) | 0.036 |
| 5 to 7 | 30 (23.4%) | 98 (76.6%) | ||
| >7 | 4 (13.3%) | 26 (86.7%) | ||
| Have a chronically ill child at home | No | 75 (16.0%) | 393 (84.0%) | 0.993 |
| Yes | 9 (16.1%) | 47 (83.9%) | ||
| Have any mental disorders | None | 55 (13.1%) | 366 (86.9%) | <0.001 |
| Anxiety | 16 (27.1%) | 43 (72.9%) | ||
| Depression | 2 (10.0%) | 18 (90.0%) | ||
| Others | 11 (45.8%) | 13 (54.2%) | ||
| Parameter | Category | OR | 95% CI | p-Value |
|---|---|---|---|---|
| Gender | Male | — | — | |
| Female | 2.32 | 1.23, 4.31 | 0.008 | |
| Nationality | Saudi | — | — | |
| Non-Saudi | 0.78 | 0.40, 1.59 | 0.485 | |
| Marital status | Divorced | — | — | |
| Married | 2.18 | 1.11, 4.14 | 0.019 | |
| Widow | 1.52 | 0.50, 5.15 | 0.478 | |
| Monthly income (SAR) | <5000 | — | — | |
| 5000 to 10,000 | 0.58 | 0.32, 1.06 | 0.075 | |
| >10,000 | 0.81 | 0.42, 1.58 | 0.536 | |
| Number of children | 1 to 5 | — | — | |
| 5 to 7 | 0.62 | 0.35, 1.10 | 0.099 | |
| >7 | 1.86 | 0.62, 7.14 | 0.308 | |
| Have any mental disorders | None | — | — | |
| Anxiety | 0.54 | 0.27, 1.13 | 0.090 | |
| Depression | 1.87 | 0.46, 12.9 | 0.444 | |
| Others | 0.37 | 0.14, 1.00 | 0.045 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alzahrani, F.; Al-Jabri, B.A.; Ramadan, S.A.L.; Alshehri, A.M.; Alsheikh, A.S.; Mushaeb, H.H.; Albisher, S.F.; AlSwealh, M.S. Parental Knowledge and Awareness about Shaken Baby Syndrome in Jeddah, Saudi Arabia: A Cross-Sectional Study. Pediatr. Rep. 2023, 15, 311-322. https://doi.org/10.3390/pediatric15020027
Alzahrani F, Al-Jabri BA, Ramadan SAL, Alshehri AM, Alsheikh AS, Mushaeb HH, Albisher SF, AlSwealh MS. Parental Knowledge and Awareness about Shaken Baby Syndrome in Jeddah, Saudi Arabia: A Cross-Sectional Study. Pediatric Reports. 2023; 15(2):311-322. https://doi.org/10.3390/pediatric15020027
Chicago/Turabian StyleAlzahrani, Fatma, Basma A. Al-Jabri, Salah Aldeen L. Ramadan, Abdulaziz M. Alshehri, Abdulaziz S. Alsheikh, Hanan Hassan Mushaeb, Sara Faisal Albisher, and Maab Sadek AlSwealh. 2023. "Parental Knowledge and Awareness about Shaken Baby Syndrome in Jeddah, Saudi Arabia: A Cross-Sectional Study" Pediatric Reports 15, no. 2: 311-322. https://doi.org/10.3390/pediatric15020027
APA StyleAlzahrani, F., Al-Jabri, B. A., Ramadan, S. A. L., Alshehri, A. M., Alsheikh, A. S., Mushaeb, H. H., Albisher, S. F., & AlSwealh, M. S. (2023). Parental Knowledge and Awareness about Shaken Baby Syndrome in Jeddah, Saudi Arabia: A Cross-Sectional Study. Pediatric Reports, 15(2), 311-322. https://doi.org/10.3390/pediatric15020027