

Custom-Made 3D Titanium Plate for Mandibular Reconstruction in Surgery of Ameloblastoma: A Novel Case Report


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
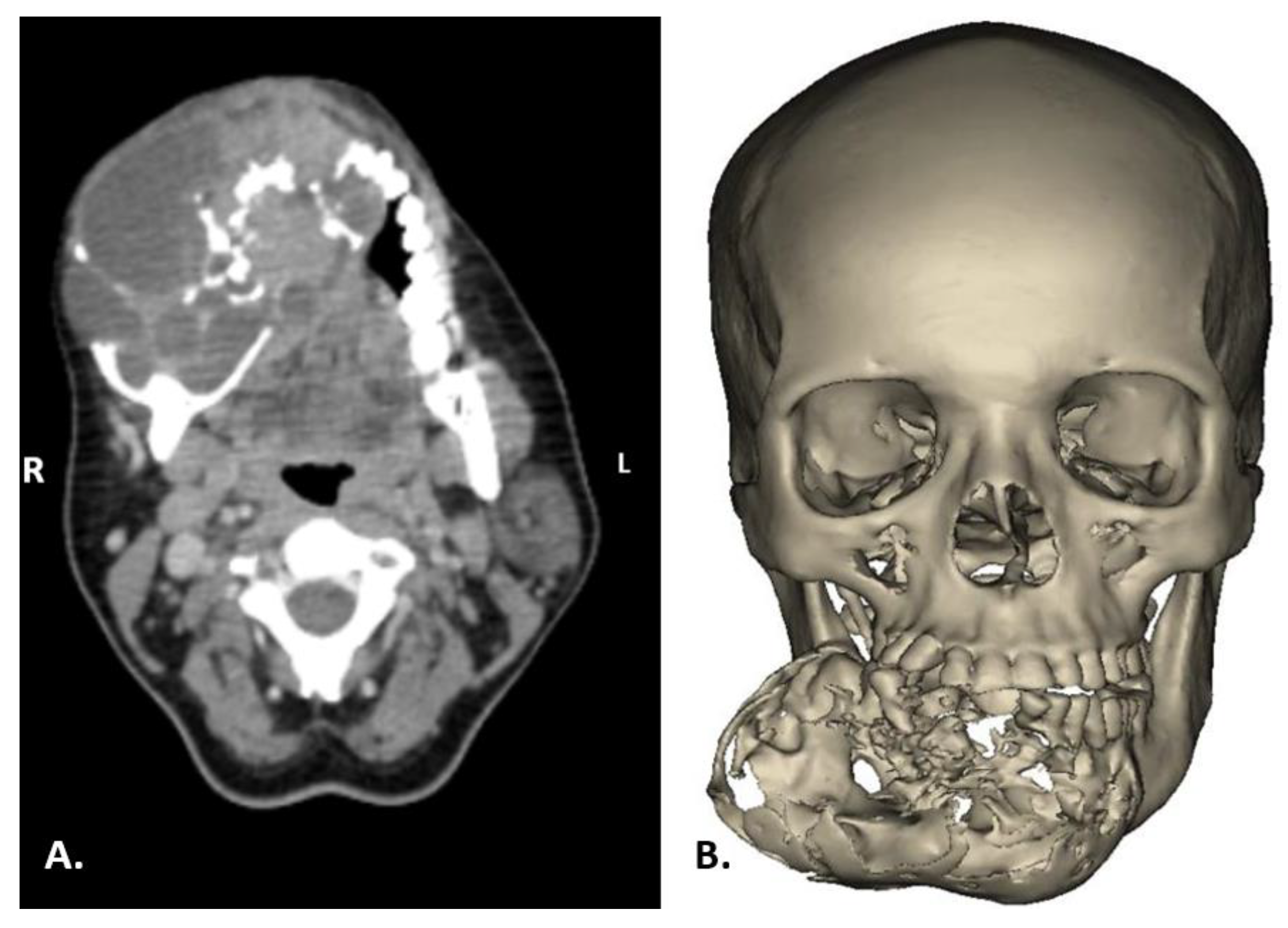
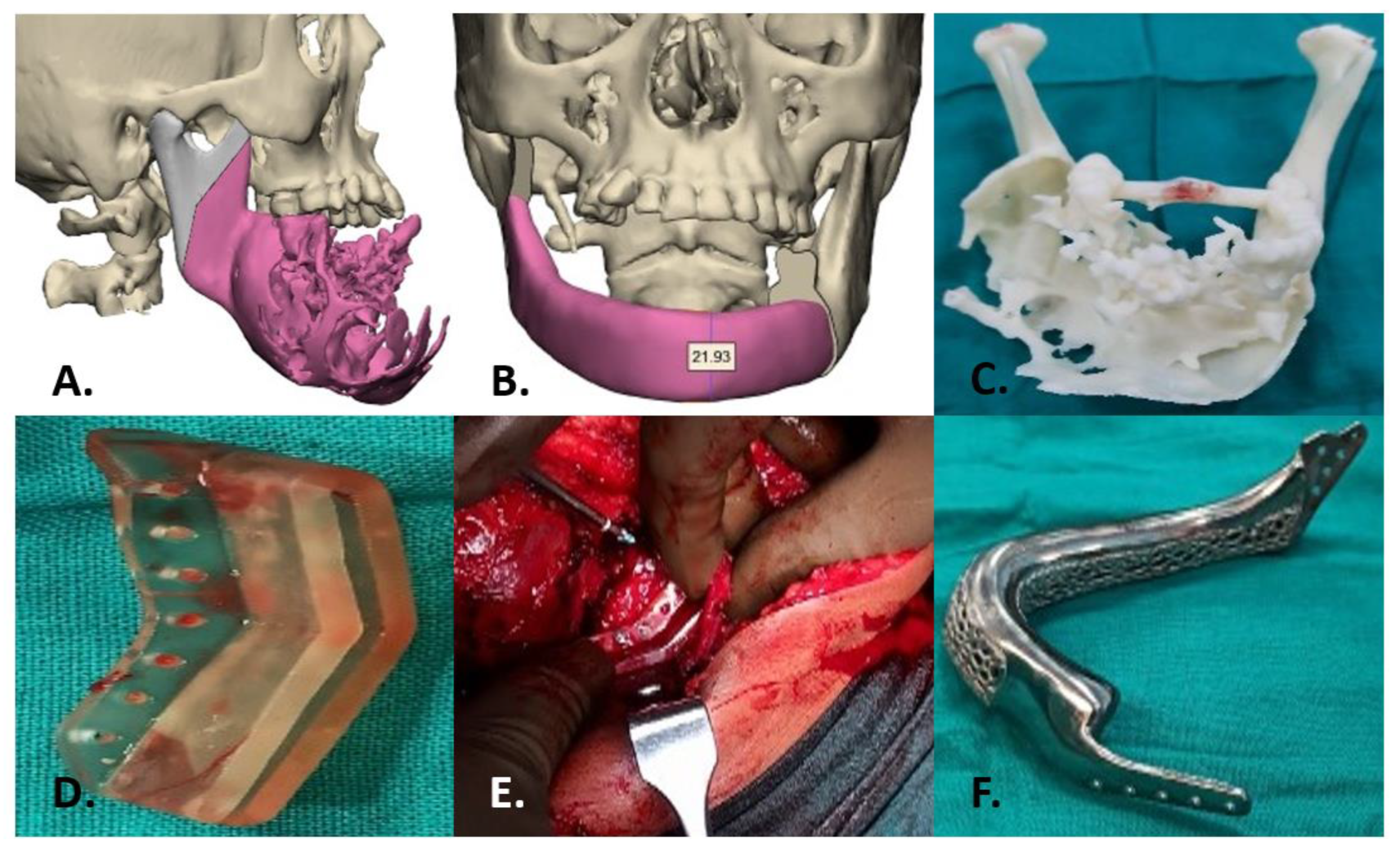
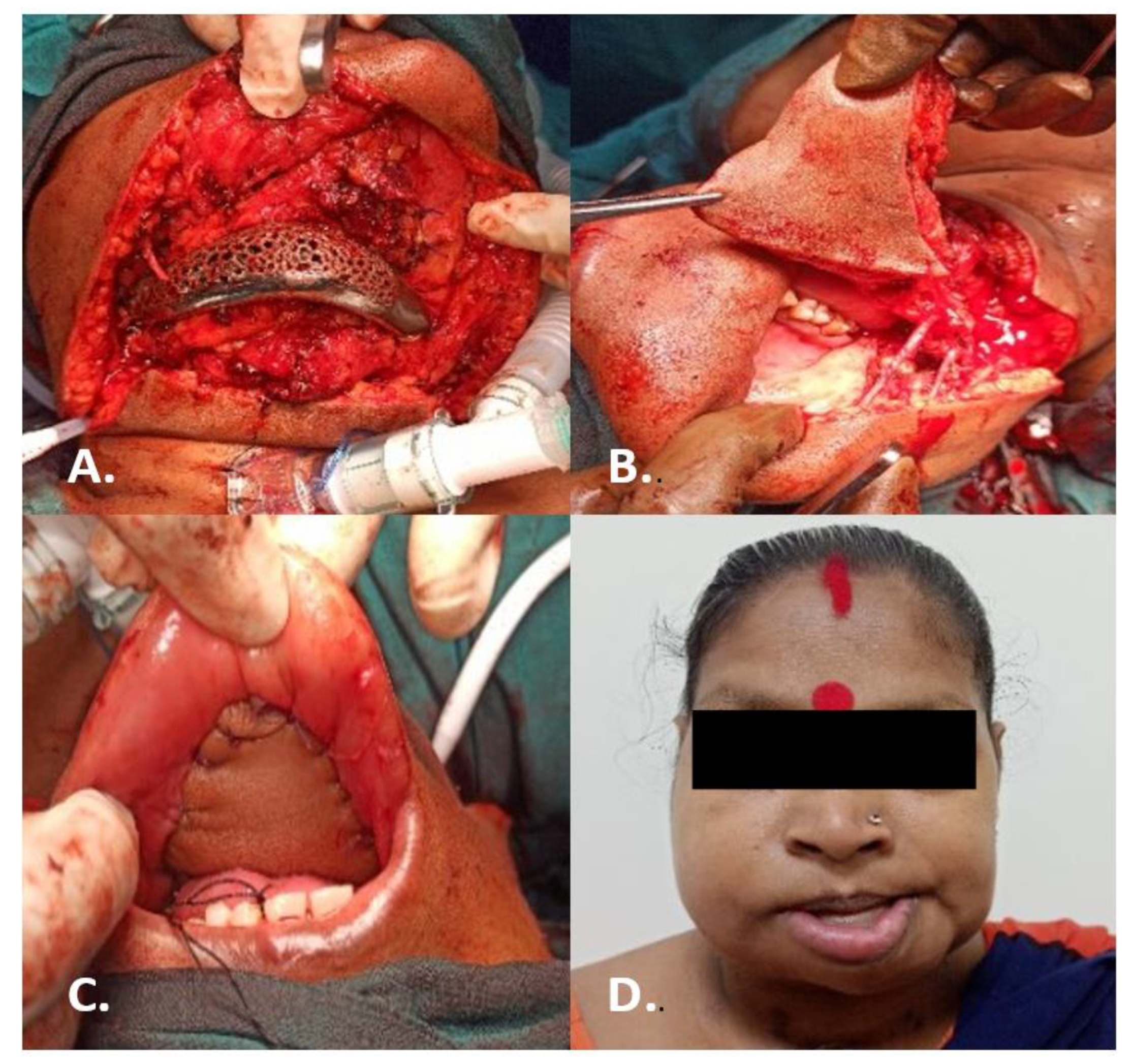
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lagares, D.T.; Cossío, P.I.; José, M.; Pérez, J.U.L. Mandibular ameloblastoma. Med. Oral Patol. Oral Cir. Bucal. 2005, 10, 231–238. [Google Scholar]
- Torres-Lagares, D.; Infante-Cossío, P.; Hernández-Guisado, J.M.; GutiérrezPérez, J.L. Mandibular ameloblastoma. A review of the literature and presentation of six cases. Med. Oral Patol. Oral Cir. Bucal. 2005, 10, 231–238. [Google Scholar] [PubMed]
- Corio, R.L.; Goldblatt, L.I.; Edwards, P.A.; Hartman, K.S. Ameloblastom carcinoma: A clinicopathologic study and assessment of eight cases. Oral Surg. Oral Med. Oral Pathol. 1987, 64, 570–576. [Google Scholar] [CrossRef]
- Adekeye, E.O. Ameloblastoma of the jaws: A survey of 109 Nigerian patients. J. Oral Surg. 1980, 38, 36–41. [Google Scholar] [PubMed]
- Vedtofte, P.; Hjorting-Hansen, E.; Jensen, B.N.; Roed-Peterson, B. Conservative surgical treatment of mandibular ameloblastomas. Int. J. Oral Surg. 1978, 7, 156–161. [Google Scholar] [CrossRef]
- Levin, M.P.; Kratochvil, F.J.; Nolan, J. Ameloblastoma of the mandible: A case report. J. Periodontol. 2003, 74, 883–886. [Google Scholar] [CrossRef] [PubMed]
- Takushima, A.; Harii, K.; Asato, H.; Nakatsuka, T.; Kimata, Y. Mandibular reconstruction using microvascular free flaps: A statistical analysis of 178 cases. Plast. Reconstr. Surg. 2001, 108, 1555–1563. [Google Scholar] [CrossRef] [PubMed]
- Jo, Y.Y.; Kim, S.G.; Kim, M.K.; Shin, S.H.; Ahn, J.; Seok, H. Mandibular reconstruction using a customized threedimensional titanium implant applied on the lingual surface of the mandible. J. Craniofacial Surg. 2018, 29, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Ardila, C.M.; Hernández-Arenas, Y.; Álvarez-Martínez, E. Mandibular Body Reconstruction Utilizing a Three-Dimensional Custom-Made Porous Titanium Plate: A Four-Year Follow-Up Clinical Report. Case Rep. Dent. 2022, 2022, 5702066. [Google Scholar] [CrossRef] [PubMed]
- Dandagi, S.; Mishra, V.; Jain, H.; Rao, D.; Verma, A. Visor approach for the total excision of a large multicystic ameloblastoma of the mandible. J. Cranio-Maxillary Dis. 2015, 4, 95. [Google Scholar]
- Qassemyar, Q.; Assouly, N.; Temam, S.; Kolb, F. Use of a three-dimensional custom-made porous titanium prosthesis for mandibular body reconstruction. Int. J. Oral Maxillofac. Surg. 2017, 46, 1248–1251. [Google Scholar] [CrossRef] [PubMed]
- Cohen, A.; Laviv, A.; Berman, P.; Nashef, R.; Abu-Tair, J. Mandibular reconstruction using stereolithographic 3-dimensional printing modeling technology. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2009, 108, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Matena, J.; Petersen, S.; Gieseke, M.; Kampmann, A.; Teske, M.; Beyerbach, M.; Escobar, H.M.; Haferkamp, H.; Gellrich, N.-C.; Nolte, I. SLM produced porous titanium implant improvements for enhanced vascularization and osteoblast seeding. Int. J. Mol. Sci. 2015, 16, 7478–7492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barbas, A.; Bonnet, A.S.; Lipinski, P.; Pesci, R.; Dubois, G. Development and mechanical characterization of porous titanium bone substitutes. J. Mech. Behav. Biomed. Mater. 2012, 9, 34–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, G.-S.; Su, Y.-X.; Liao, G.-Q.; Chen, Z.-F.; Wang, L.; Jiao, P.-F.; Liu, H.-C.; Zhong, Y.-Q.; Zhang, T.-H.; Liang, Y.-J. Mandible reconstruction assisted by preoperative virtual surgical simulation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 113, 604–611. [Google Scholar] [CrossRef] [PubMed]
- Sykes, L.M.; Parrott, A.M.; Owen, P.; Snaddon, D.R. Applications of rapid prototyping technology in maxillofacial prosthetics. Int. J. Prosthodont 2004, 17, 454–459. [Google Scholar] [PubMed]
- Touré, G.; Gouet, E. Use of a 3-dimensional custom-made porous titanium prosthesis for mandibular body reconstruction with prosthetic dental rehabilitation and lipofilling. J. Oral Maxillofac. Surg. 2019, 77, 1305–1313. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chakraborty, S.; Guha, R.P.; Naskar, S.; Banerjee, R. Custom-Made 3D Titanium Plate for Mandibular Reconstruction in Surgery of Ameloblastoma: A Novel Case Report. Surg. Tech. Dev. 2022, 11, 98-104. https://doi.org/10.3390/std11030009
Chakraborty S, Guha RP, Naskar S, Banerjee R. Custom-Made 3D Titanium Plate for Mandibular Reconstruction in Surgery of Ameloblastoma: A Novel Case Report. Surgical Techniques Development. 2022; 11(3):98-104. https://doi.org/10.3390/std11030009
Chicago/Turabian StyleChakraborty, Somangshu, Rajdeep P. Guha, Sukanya Naskar, and Rajarshi Banerjee. 2022. "Custom-Made 3D Titanium Plate for Mandibular Reconstruction in Surgery of Ameloblastoma: A Novel Case Report" Surgical Techniques Development 11, no. 3: 98-104. https://doi.org/10.3390/std11030009
APA StyleChakraborty, S., Guha, R. P., Naskar, S., & Banerjee, R. (2022). Custom-Made 3D Titanium Plate for Mandibular Reconstruction in Surgery of Ameloblastoma: A Novel Case Report. Surgical Techniques Development, 11(3), 98-104. https://doi.org/10.3390/std11030009