
Lateralization Pattern of the Weber Tuning Fork Test in Longstanding Unilateral Profound Hearing Loss: Implications for Cochlear Implantation


 and
and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Patient Cohort
3.2. Weber Test Lateralization Pattern and the Age of Onset
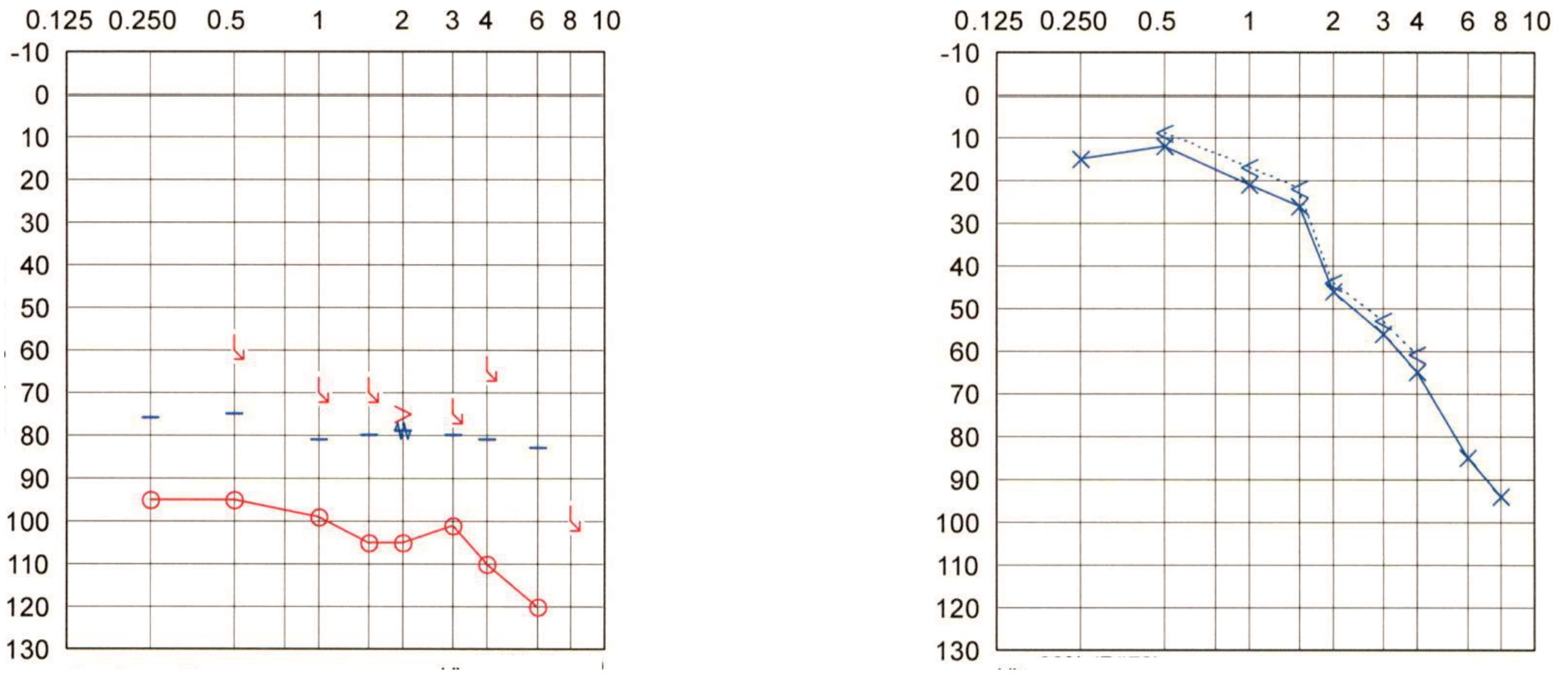
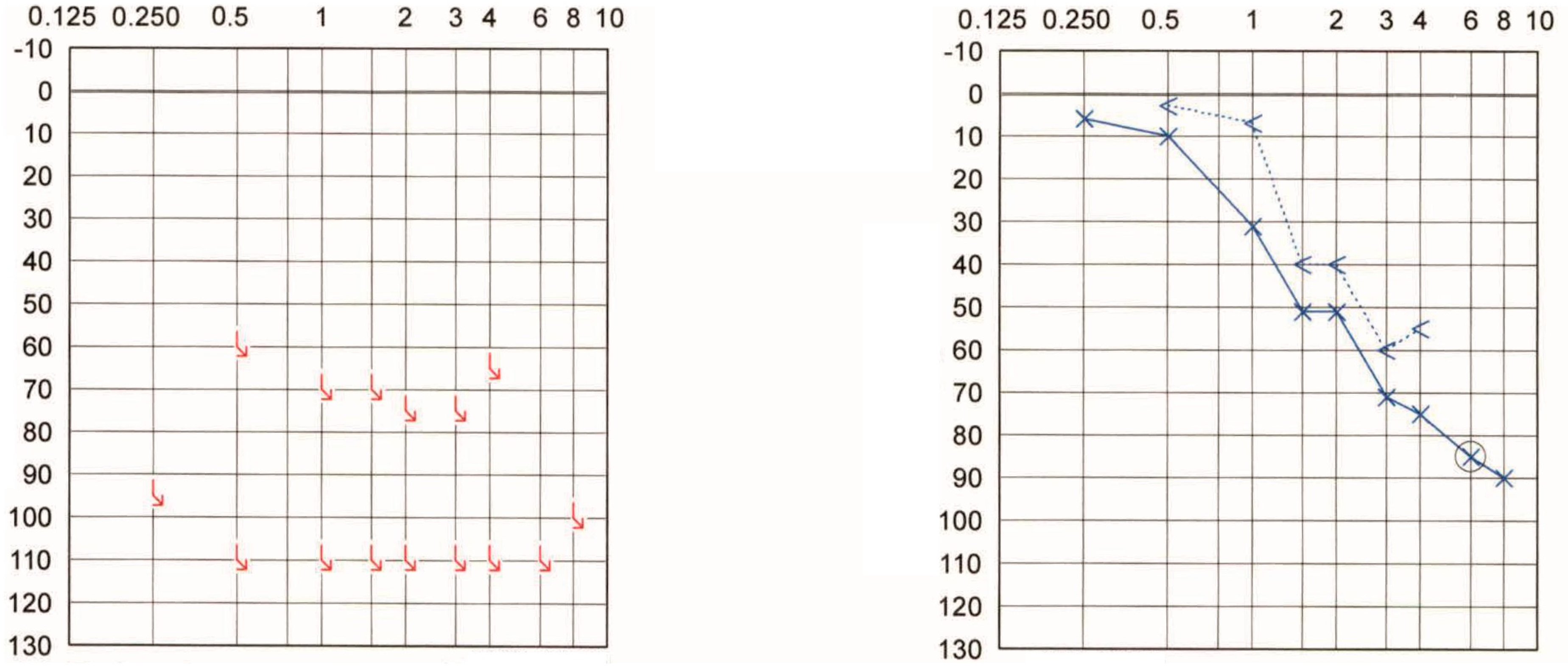
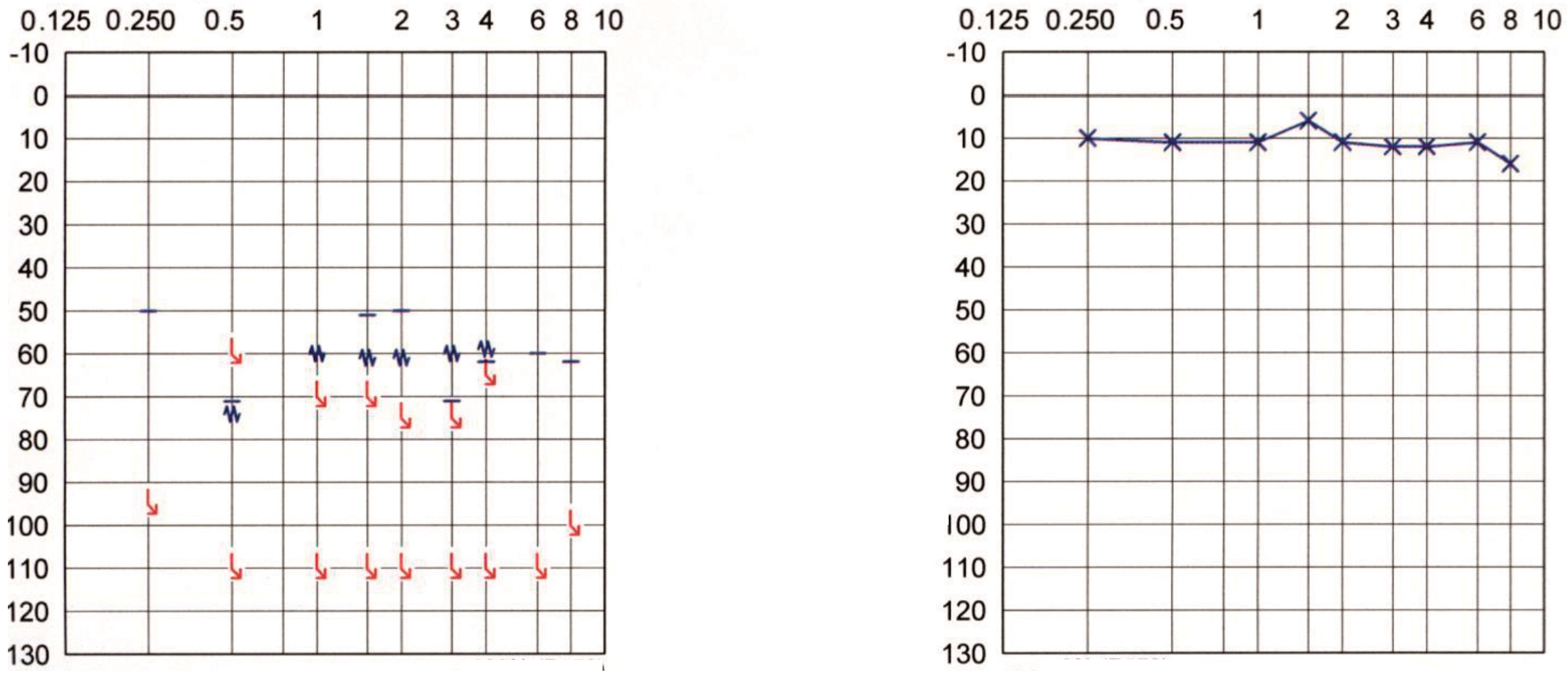
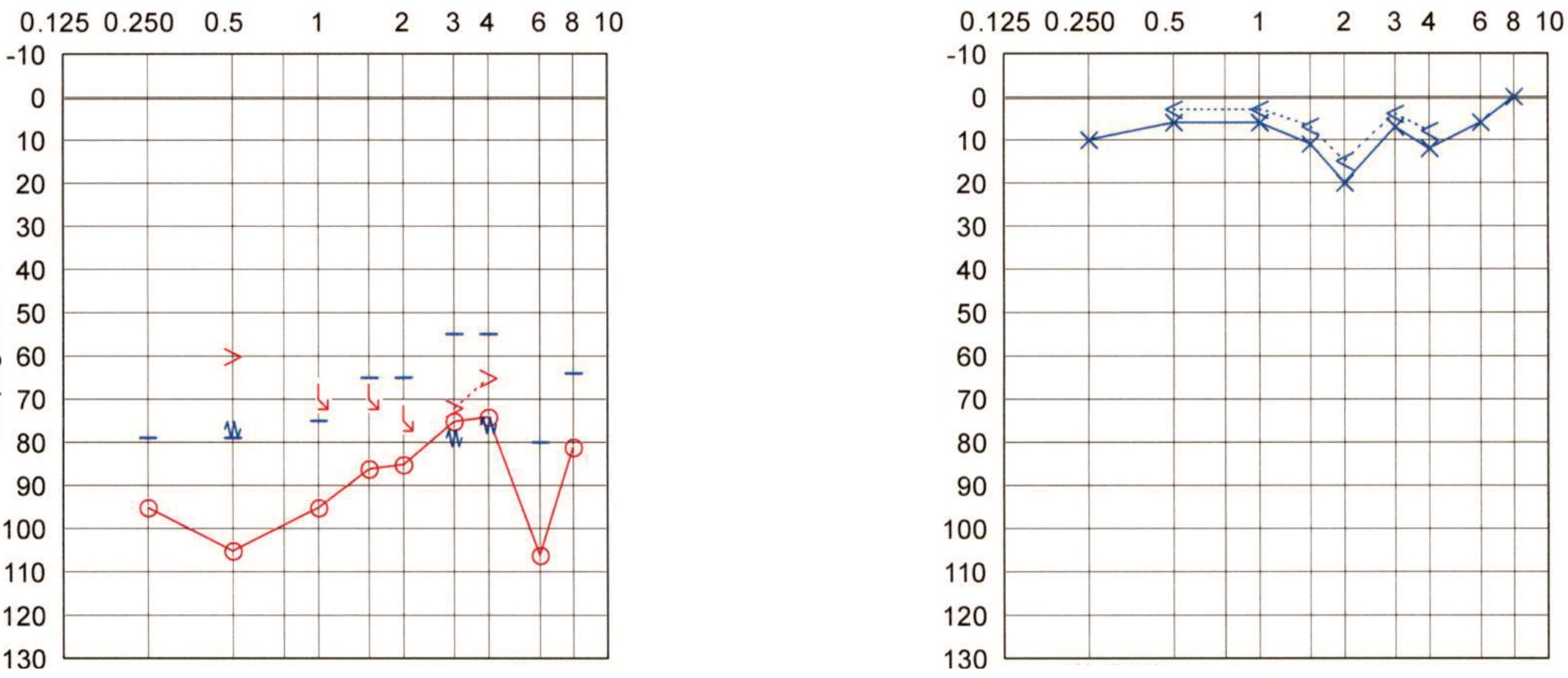
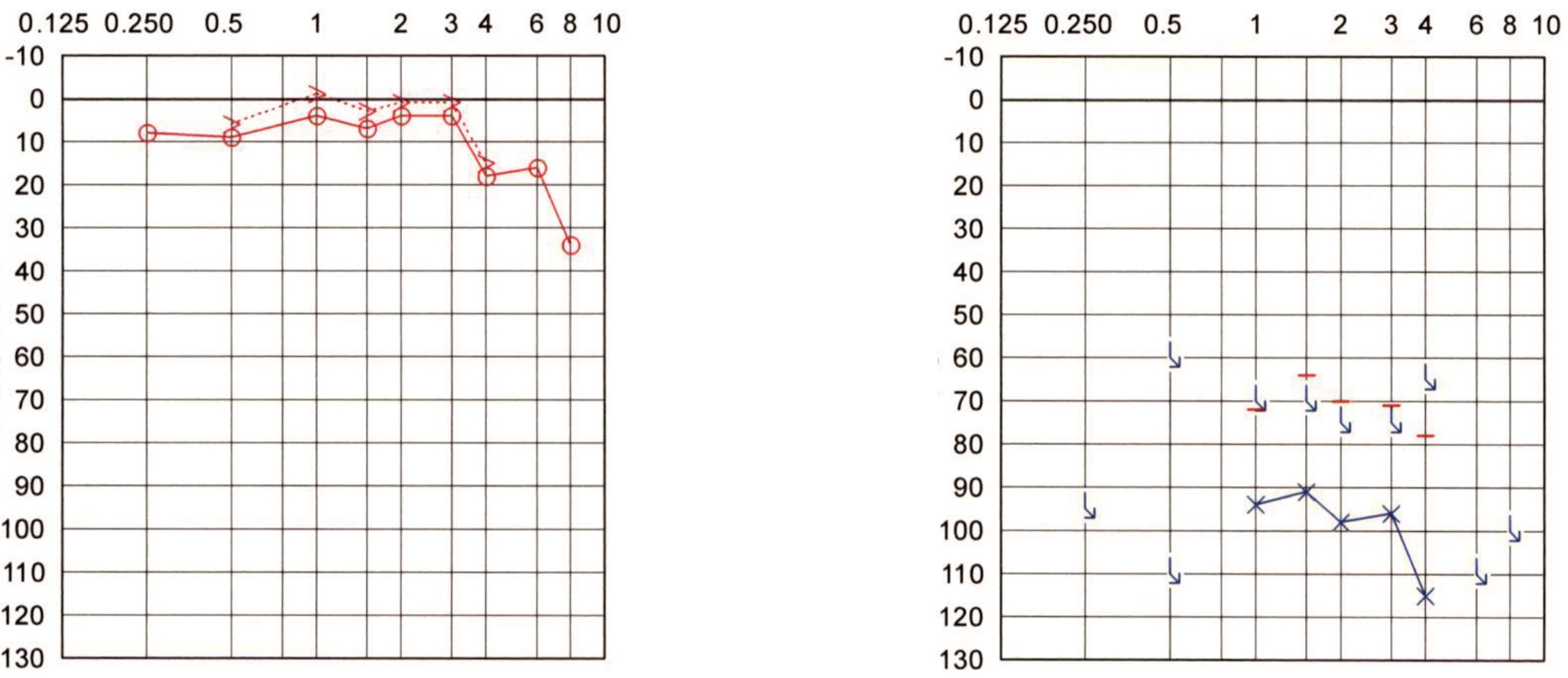
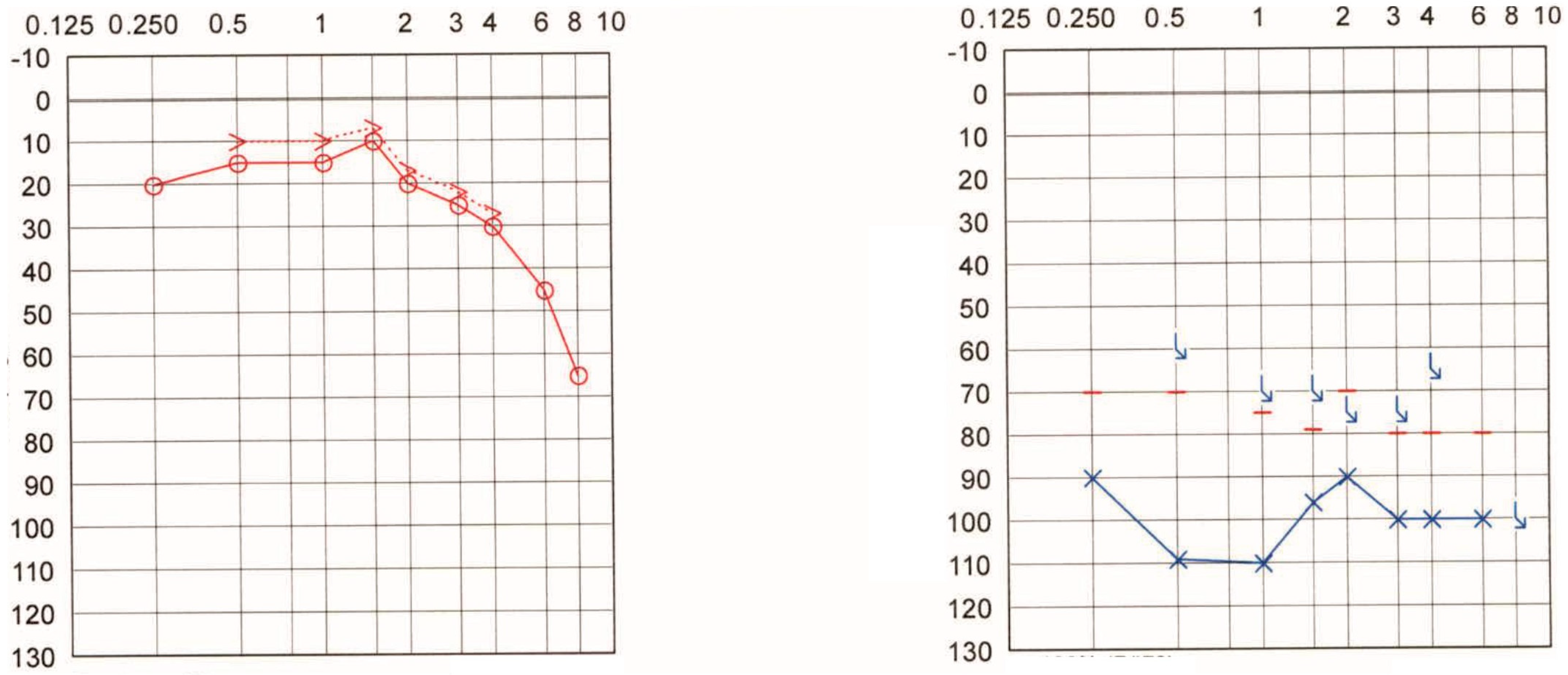
3.3. Case Presentations (Selected Cases)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Huizing, E.H. Lateralization of bone conduction into the better ear in conductive deafness. Paradoxical Weber test in unilaterally operated otosclerosis. Acta Otolaryngol. 1970, 69, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Guindi, G.M. Lateralization of the Weber response after stapedectomy. Br. J. Audiol. 1981, 15, 97–100. [Google Scholar] [CrossRef] [PubMed]
- Blakley, B.W.; Siddique, S. A qualitative explanation of the Weber test. Otolaryngol. Head Neck Surg. 1999, 120, 1–4. [Google Scholar] [CrossRef]
- Sichel, J.Y.; Freeman, S.; Sohmer, H. Lateralization during the Weber test: Animal experiments. Laryngoscope 2002, 112, 542–546. [Google Scholar] [CrossRef] [PubMed]
- Scott-Brown, W.G.; Ballantyne, J.; Groves, J. Scott-Brown’s Diseases of the Ear, Nose and Throat: The Ear; Butterworth: Oxford, UK, 1979. [Google Scholar]
- Ghosh, P. Weber-QUO vedis? Indian J. Otolaryngol. Head Neck Surg. 1995, 47, 140–141. [Google Scholar] [CrossRef]
- Goodman, A. Reference zero levels for pure-tone audiometers. J. Speech Lang. Hear. Res. 1965, 7, 7–16. [Google Scholar] [CrossRef]
- Clark, J.G. Uses and abuses of hearing loss classification. Asha 1981, 23, 493–500. [Google Scholar]
- Vincent, C.; Arndt, S.; Firszt, J.B.; Fraysse, B.; Kitterick, P.T.; Papsin, B.C.; Snik, A.; Van de Heyning, P.; Deguine, O.; Marx, M. Identification and evaluation of cochlear implant candidates with asymmetrical hearing loss. Audiol. Neurootol. 2015, 20, 87–89. [Google Scholar] [CrossRef]
- Van de Heyning, P.; Távora-Vieira, D.; Mertens, G.; Van Rompaey, V.; Rajan, G.P.; Müller, J.; Hempel, J.M.; Leander, D.; Polterauer, D.; Marx, M.; et al. Towards a Unified Testing Framework for Single-Sided Deafness Studies: A Consensus Paper. Audiol. Neurootol. 2016, 21, 391–398. [Google Scholar] [CrossRef]
- Curthoys, I.S.; Halmagyi, G.M. Vestibular compensation: A review of the oculomotor, neural, and clinical consequences of unilateral vestibular loss. J. Vestib. Res. Equilib. Orientat. 1995, 5, 67–107. [Google Scholar] [CrossRef]
- Strupp, M.; Arbusow, V.; Maag, K.P.; Gall, C.; Brandt, T. Vestibular exercises improve central vestibulospinal compensation after vestibular neuritis. Neurology 1998, 51, 838–844. [Google Scholar] [CrossRef] [PubMed]
- Dutia, M.B. Mechanisms of vestibular compensation: Recent advances. Curr. Opin. Otolaryngol. Head Neck Surg. 2010, 18, 420–424. [Google Scholar] [CrossRef] [PubMed]
- Gordon, K.; Kral, A. Animal and human studies on developmental monaural hearing loss. Hear. Res. 2019, 380, 60–74. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Zhou, M.; He, X.; Wang, N. Single-sided deafness and unilateral auditory deprivation in children: Current challenge of improving sound localization ability. J. Int. Med. Res. 2020, 48. [Google Scholar] [CrossRef]
- Sharma, A.; Glick, H.; Campbell, J.; Torres, J.; Dorman, M.; Zeitler, D.M. Cortical plasticity and reorganization in pediatric single-sided deafness pre- and postcochlear implantation: A case study. Otol. Neurotol. 2016, 37, e26–e34. [Google Scholar] [CrossRef]
- Polonenko, M.J.; Gordon, K.A.; Cushing, S.L.; Papsin, B.C. Cortical organization restored by cochlear implantation in young children with single sided deafness. Sci. Rep. 2017, 7, 16900. [Google Scholar] [CrossRef]
- Lee, H.J.; Smieja, D.; Polonenko, M.J.; Cushing, S.L.; Papsin, B.C.; Gordon, K.A. Consistent and chronic cochlear implant use partially reverses cortical effects of single sided deafness in children. Sci. Rep. 2020, 10, 21526. [Google Scholar] [CrossRef]
- Yamazaki, H.; Easwar, V.; Polonenko, M.J.; Jiwani, S.; Wong, D.D.E.; Papsin, B.C.; Gordon, K.A. Cortical hemispheric asymmetries are present at young ages and further develop into adolescence. Hum. Brain Mapp. 2018, 39, 941–954. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; Heo, H.; Kim, D.H.; Kim, H.J.; Oh, S.H. Neural plastic changes in the subcortical auditory neural pathway after single-sided deafness in adult mice: A MEMRI study. Biomed. Res. Int. 2018, 2018, 8624745. [Google Scholar] [CrossRef] [Green Version]
- Scheffler, K.; Bilecen, D.; Schmid, N.; Tschopp, K.; Seelig, J. Auditory cortical responses in hearing subjects and unilateral deaf patients as detected by functional magnetic resonance imaging. Cereb. Cortex 1998, 8, 156–163. [Google Scholar] [CrossRef]
- Bilecen, D.; Seifritz, E.; Radü, E.W.; Schmid, N.; Wetzel, S.; Probst, R.; Scheffler, K. Cortical reorganization after acute unilateral hearing loss traced by fMRI. Neurology 2000, 54, 765–767. [Google Scholar] [CrossRef] [PubMed]
- Peters, J.P.; Smit, A.L.; Stegeman, I.; Grolman, W. Review: Bone conduction devices and contralateral routing of sound systems in single-sided deafness. Laryngoscope 2015, 125, 218–226. [Google Scholar] [CrossRef]
- Kitterick, P.T.; Smith, S.N.; Lucas, L. Hearing Instruments for Unilateral Severe-to-Profound Sensorineural Hearing Loss in Adults: A Systematic Review and Meta-Analysis. Ear Hear 2016, 37, 495–507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabral Junior, F.; Pinna, M.H.; Alves, R.D.; Malerbi, A.F.; Bento, R.F. Cochlear Implantation and Single-sided Deafness: A Systematic Review of the Literature. Int. Arch. Otorhinolaryngol. 2016, 20, 69–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peters, J.P.M.; van Heteren, J.A.A.; Wendrich, A.W.; van Zanten, G.A.; Grolman, W.; Stokroos, R.J.; Smit, A.L. Short-term outcomes of cochlear implantation for single-sided deafness compared to bone conduction devices and contralateral routing of sound hearing aids-Results of a Randomised controlled trial (CINGLE-trial). PLoS ONE 2021, 16, e0257447. [Google Scholar] [CrossRef]
- Cohen, S.M.; Svirsky, M.A. Duration of unilateral auditory deprivation is associated with reduced speech perception after cochlear implantation: A single-sided deafness study. Cochlear Implant. Int. 2019, 20, 51–56. [Google Scholar] [CrossRef]
- Haussler, S.M.; Kopke, V.; Knopke, S.; Grabel, S.; Olze, H. Multifactorial positive influence of cochlear implantation on patients with single-sided deafness. Laryngoscope 2020, 130, 500–506. [Google Scholar] [CrossRef] [PubMed]
- Kurz, A.; Grubenbecher, M.; Rak, K.; Hagen, R.; Kuhn, H. The impact of etiology and duration of deafness on speech perception outcomes in SSD patients. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 3317–3325. [Google Scholar] [CrossRef]
- van Zon, A.; Peters, J.P.; Stegeman, I.; Smit, A.L.; Grolman, W. Cochlear implantation for patients with single-sided deafness or asymmetrical hearing loss: A systematic review of the evidence. Otol. Neurotol. 2015, 36, 209–219. [Google Scholar] [CrossRef]
- Blasco, M.A.; Redleaf, M.I. Cochlear implantation in unilateral sudden deafness improves tinnitus and speech comprehension: Meta-analysis and systematic review. Otol. Neurotol. 2014, 35, 1426–1432. [Google Scholar] [CrossRef] [Green Version]
- Nassiri, A.M.; Wallerius, K.P.; Saoji, A.A.; Neff, B.A.; Driscoll, C.L.W.; Carlson, M.L. Impact of duration of deafness on speech perception in single-sided deafness cochlear implantation in adults. Otol. Neurotol. 2022, 43, e45–e49. [Google Scholar] [CrossRef] [PubMed]
- Haussler, S.M.; Knopke, S.; Dudka, S.; Grabel, S.; Ketterer, M.C.; Battmer, R.D.; Ernst, A.; Olze, H. Improvement in tinnitus distress, health-related quality of life and psychological comorbidities by cochlear implantation in single-sided deaf patients. HNO 2020, 68, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Knipper, M.; van Dijk, P.; Schulze, H.; Mazurek, B.; Krauss, P.; Scheper, V.; Warnecke, A.; Schlee, W.; Schwabe, K.; Singer, W.; et al. The Neural Bases of Tinnitus: Lessons from Deafness and Cochlear Implants. J. Neurosci. 2020, 40, 7190–7202. [Google Scholar] [CrossRef]
- Eggermont, J.J.; Kral, A. Somatic memory and gain increase as preconditions for tinnitus: Insights from congenital deafness. Hear. Res. 2016, 333, 37–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.Y.; Nam, D.W.; Koo, J.W.; De Ridder, D.; Vanneste, S.; Song, J.J. No auditory experience, no tinnitus: Lessons from subjects with congenital- and acquired single-sided deafness. Hear. Res. 2017, 354, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.M.; Kim, Y.; Ji, J.Y.; Koo, J.W.; Song, J.J. Auditory experience, for a certain duration, is a prerequisite for tinnitus: Lessons from subjects with unilateral tinnitus in the better-hearing ear. Prog. Brain Res. 2021, 260, 223–233. [Google Scholar] [CrossRef]
- Muhlmeier, G.; Baguley, D.; Cox, T.; Suckfull, M.; Meyer, T. Characteristics and spontaneous recovery of tinnitus related to idiopathic sudden sensorineural hearing loss. Otol. Neurotol. 2016, 37, 634–641. [Google Scholar] [CrossRef]
- Liu, Y.W.; Cheng, X.; Chen, B.; Peng, K.; Ishiyama, A.; Fu, Q.J. Effect of tinnitus and duration of deafness on sound localization and speech recognition in noise in patients with single-sided deafness. Trends Hear. 2018, 22, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Kral, A.; Hubka, P.; Heid, S.; Tillein, J. Single-sided deafness leads to unilateral aural preference within an early sensitive period. Brain 2013, 136, 180–193. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (Years) | Gender | Weber Test | Residual Hearing | SSD vs. AHL | Etiology | Age of Onset (Years) | Onset Classification | Duration of UHL (Years) | Tinnitus | |
|---|---|---|---|---|---|---|---|---|---|---|
| #1 | 78 | F | No lateralization | Yes | AHL | Infectious (scarlet fever) | 6 | Childhood onset | 72 | No |
| #2 | 34 | M | Lateralized | No | SSD | Infectious (meningitis) | 4 | Childhood onset | 30 | No |
| #3 | 75 | F | Lateralized | No | AHL | Surgery | 22 | Adult onset | 53 | Yes |
| #4 | 54 | M | Lateralized | No | SSD | Surgery | 37 | Adult onset | 17 | Yes |
| #5 | 54 | M | No lateralization | Yes | SSD | Trauma | 7 | Childhood onset | 47 | No |
| #6 | 54 | M | No lateralization | No | SSD | Infectious (labyrinthitis) | 4 | Childhood onset | 50 | No |
| #7 | 56 | F | No lateralization | Yes | SSD | SSNHL | 46 | Adult onset | 10 | Yes |
| #8 | 36 | F | No lateralization | No | SSD | Congenital | 0 | Childhood onset | 36 | No |
| #9 | 54 | M | No lateralization | No | SSD | Congenital | 0 | Childhood onset | 54 | No |
| #10 | 51 | M | Lateralized | Yes | SSD | Menière’s disease | 33 | Adult onset | 18 | Yes |
| #11 | 44 | F | Lateralized | Yes | SSD | SSNHL | 22 | Adult onset | 22 | Yes |
| #12 | 26 | F | No lateralization | No | SSD | Infectious (mumps) | 3 | Childhood onset | 23 | No |
| #13 | 78 | F | No lateralization | Yes | AHL | Infectious | 5 | Childhood onset | 73 | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bassiouni, M.; Häußler, S.M.; Gräbel, S.; Szczepek, A.J.; Olze, H. Lateralization Pattern of the Weber Tuning Fork Test in Longstanding Unilateral Profound Hearing Loss: Implications for Cochlear Implantation. Audiol. Res. 2022, 12, 347-356. https://doi.org/10.3390/audiolres12040036
Bassiouni M, Häußler SM, Gräbel S, Szczepek AJ, Olze H. Lateralization Pattern of the Weber Tuning Fork Test in Longstanding Unilateral Profound Hearing Loss: Implications for Cochlear Implantation. Audiology Research. 2022; 12(4):347-356. https://doi.org/10.3390/audiolres12040036
Chicago/Turabian StyleBassiouni, Mohamed, Sophia Marie Häußler, Stefan Gräbel, Agnieszka J. Szczepek, and Heidi Olze. 2022. "Lateralization Pattern of the Weber Tuning Fork Test in Longstanding Unilateral Profound Hearing Loss: Implications for Cochlear Implantation" Audiology Research 12, no. 4: 347-356. https://doi.org/10.3390/audiolres12040036
APA StyleBassiouni, M., Häußler, S. M., Gräbel, S., Szczepek, A. J., & Olze, H. (2022). Lateralization Pattern of the Weber Tuning Fork Test in Longstanding Unilateral Profound Hearing Loss: Implications for Cochlear Implantation. Audiology Research, 12(4), 347-356. https://doi.org/10.3390/audiolres12040036