
How Cochlear Implant Rehabilitation Impacts the Therapeutic Strategy for Vestibular Schwannoma


Abstract
:1. Introduction
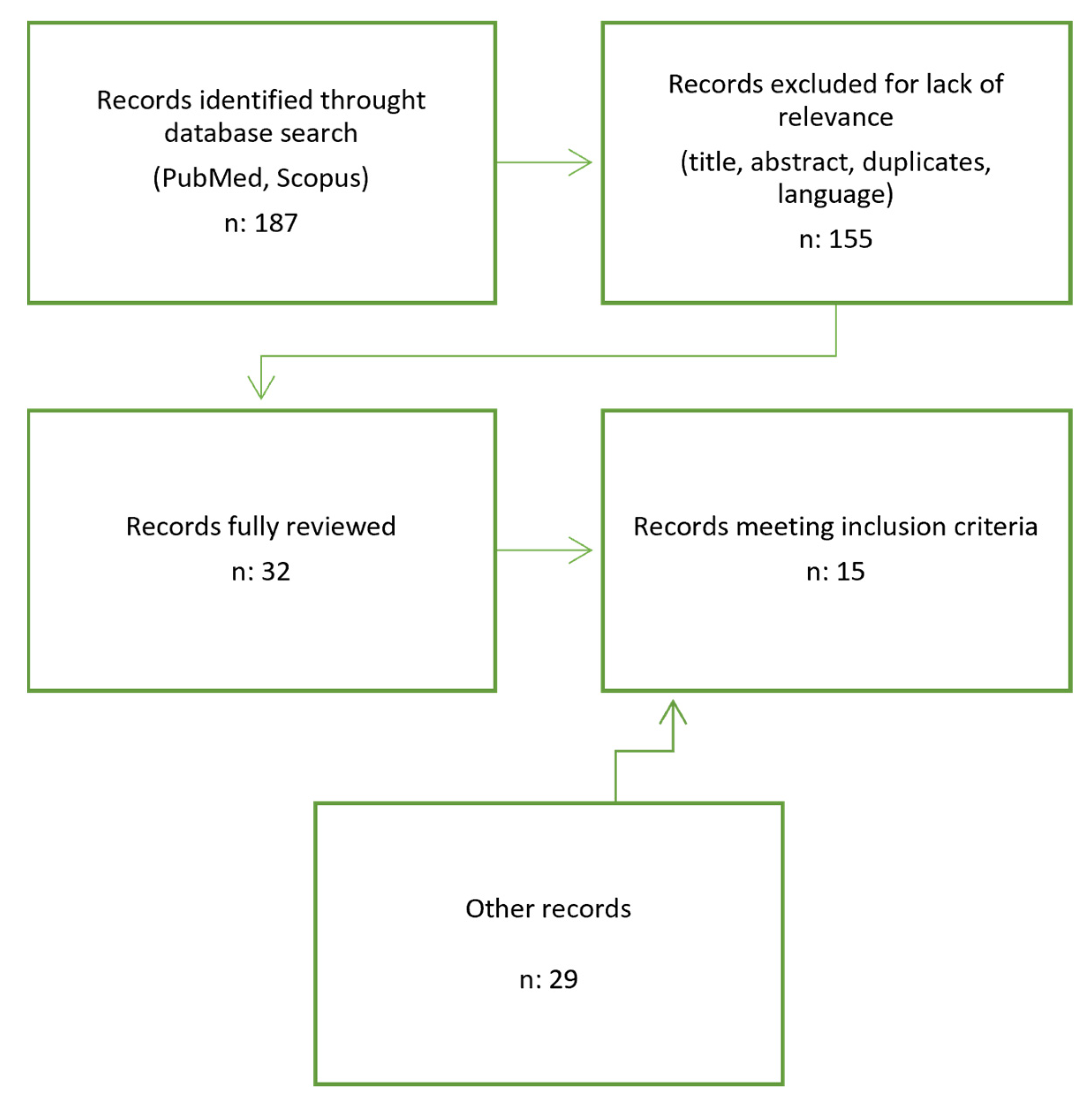
2. Materials and Methods
3. Results and Discussion
3.1. Prerequisites in Management of VS and CI
3.2. Sporadic VS and CI Rehabilitation
3.3. Neurofibromatosis Type 2 and CI
3.4. MRI Surveillance and CI
3.5. Intralabyrinthine Schwannoma and CI
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Marinelli, J.P.; Beeler, C.J.; Carlson, M.L.; Caye-Thomasen, P.; Spear, S.A.; Erbele, I.D. Global Incidence of Sporadic Vestibular Schwannoma: A Systematic Review. Otolaryngol. Neck Surg. 2022, 167, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Kanzaki, J.; Tos, M.; Sanna, M.; Moffat, D.A. New and Modified Reporting Systems from the Consensus Meeting on Systems for Reporting Results in Vestibular Schwannoma. Otol. Neurotol. 2003, 24, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Koos, W.T.; Day, J.D.; Matula, C.; Levy, D.I. Neurotopographic considerations in the microsurgical treatment of small acoustic neuri-nomas. J. Neurosurg. 1998, 88, 506–512. [Google Scholar] [CrossRef] [PubMed]
- Goldbrunner, R.; Weller, M.; Regis, J.; Lund-Johansen, M.; Stavrinou, P.; Reuss, D.; Evans, D.G.; Lefranc, F.; Sallabanda, K.; Falini, A.; et al. EANO guideline on the diagnosis and treatment of vestibular schwannoma. Neuro-Oncology 2020, 22, 31–45. [Google Scholar] [CrossRef]
- Kaltoft, M.; Stangerup, S.-E.; Caye-Thomasen, P. Facial Nerve Function After Vestibular Schwannoma Surgery Following Failed Conservative Management. Neurosurgery 2012, 70, 278–282. [Google Scholar] [CrossRef]
- Carlson, M.L.; Jacob, J.T.; Pollock, B.E.; Neff, B.A.; Tombers, N.M.; Driscoll, C.L.W.; Link, M.J. Long-term hearing outcomes following stereotactic radiosurgery for vestibular schwannoma: Patterns of hearing loss and variables influencing audiometric decline. J. Neurosurg. 2013, 118, 579–587. [Google Scholar] [CrossRef]
- Schwartz, M.S.; Lekovic, G.P.; Miller, M.E.; Slattery, W.H.; Wilkinson, E.P. Translabyrinthine microsurgical resection of small vestibular schwannomas. J. Neurosurg. 2018, 129, 128–136. [Google Scholar] [CrossRef]
- Zanoletti, E.; Mazzoni, A.; Chiumenti, F.A.; D’Avella, D.; Cazzador, D. Early Translabyrinthine Surgery for Small- and Medium-Sized Vestibular Schwannomas: Consecutive Cohort Analysis of Outcomes. Otol. Neurotol. 2022, 43, 962–967. [Google Scholar] [CrossRef]
- Brackmann, D.E.; Cullen, R.D.; Fisher, L.M. Facial Nerve Function after Translabyrinthine Vestibular Schwannoma Surgery. Otolaryngol. Neck Surg. 2007, 136, 773–777. [Google Scholar] [CrossRef]
- Falcioni, M.; Fois, P.; Taibah, A.; Sanna, M. Facial nerve function after vestibular schwannoma surgery. J. Neurosurg. 2011, 115, 820–826. [Google Scholar] [CrossRef]
- Prasad, S.C.; Patnaik, U.; Grinblat, G.; Giannuzzi, A.; Piccirillo, E.; Taibah, A.; Sanna, M. Decision Making in the Wait-and-Scan Approach for Vestibular Schwannomas: Is There a Price to Pay in Terms of Hearing, Facial Nerve, and Overall Outcomes? Neurosurgery 2018, 83, 858–870. [Google Scholar] [CrossRef]
- Lee, H.-J.; Kim, M.J.; Koh, S.H.; Chang, W.S.; Moon, I.S. Comparing Outcomes Following Salvage Microsurgery in Vestibular Schwannoma Patients Failing Gamma-knife Radiosurgery or Microsurgery. Otol. Neurotol. 2017, 38, 1339–1344. [Google Scholar] [CrossRef]
- Lerner, D.K.; Lee, D.; Naples, J.G.; Brant, J.A.; Bigelow, D.; Alonso-Basanta, M.; Ruckenstein, M.J. Factors Associated With Facial Nerve Paresis Following Gamma Knife for Vestibular Schwannoma. Otol. Neurotol. 2020, 41, E83–E88. [Google Scholar] [CrossRef]
- Do, R.M.C.; Tu, N.C.; Sioshansi, P.C.; Porps, S.L.; Schutt, C.A.; Hong, R.S.; Jacob, J.T.; Babu, S.C. Early Outcomes of Simultaneous Translabyrinthine Resection and Cochlear Implantation. Laryngoscope 2021, 131, E2312–E2317. [Google Scholar] [CrossRef]
- Sanna, M.; Medina, M.D.M.; Macak, A.; Rossi, G.; Sozzi, V.; Prasad, S.C. Vestibular Schwannoma Resection with Ipsilateral Simultaneous Cochlear Implantation in Patients with Normal Contralateral Hearing. Audiol. Neurotol. 2017, 21, 286–295. [Google Scholar] [CrossRef]
- Rooth, M.A.; Dillon, M.T.; Brown, K.D. Prospective Evaluation of Patients Undergoing Translabyrinthine Excision of Vestibular Schwannoma with Concurrent Cochlear Implantation. Otol. Neurotol. 2017, 38, 1512–1516. [Google Scholar] [CrossRef]
- Sorrentino, F.; Tealdo, G.; Cazzador, D.; Favaretto, N.; Brotto, D.; Montino, S.; Caserta, E.; Bovo, R.; Denaro, L.; Baro, V.; et al. Cochlear implant in vestibular schwannomas: Long-term outcomes and critical analysis of indications. Eur. Arch. Oto-Rhino-Laryngol. 2022, 279, 4709–4718. [Google Scholar] [CrossRef]
- Thompson, N.J.; O’Connell, B.P.; Brown, K.D. Translabyrinthine Excision of Vestibular Schwannoma with Concurrent Cochlear Implantation: Systematic Review. J. Neurol. Surg. Part B Skull Base 2019, 80, 187–195. [Google Scholar] [CrossRef]
- West, N.; Sass, H.; Cayé-Thomasen, P. Sporadic and NF2-associated vestibular schwannoma surgery and simultaneous cochlear implantation: A comparative systematic review. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 333–342. [Google Scholar] [CrossRef]
- Wick, C.C.; Butler, M.J.; Yeager, L.H.; Kallogjeri, D.; Durakovic, N.; McJunkin, J.L.; Shew, M.A.; Herzog, J.A.; Buchman, C.A. Cochlear Implant Outcomes Following Vestibular Schwannoma Resection. Otol. Neurotol. 2020, 41, 1190–1197. [Google Scholar] [CrossRef]
- Bartindale, M.R.; Tadokoro, K.; El-Kouri, N.; Moore, D.; Britt, C.; Kircher, M. Cochlear Implantation in Vestibular Schwannoma: A Systematic Literature Review. J. Neurol. Surg. Part B Skull Base 2021, 82, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Tian, L.; West, N.; Caye-Thomasen, P. Cochlear Implantation After Radiotherapy of Vestibular Schwannomas. J. Int. Adv. Otol. 2021, 17, 452–460. [Google Scholar] [CrossRef]
- Borsetto, D.; Hammond-Kenny, A.; Tysome, J.R.; Axon, P.R.; Donnelly, N.P.; Vijendren, A.; Phillips, V.; Bance, M.L. Hearing rehabilitation outcomes in cochlear implant recipients with vestibular schwannoma in observation or radiotherapy groups: A systematic review. Cochlea-Implant. Int. 2020, 21, 9–17. [Google Scholar] [CrossRef]
- Longino, E.S.; Manzoor, N.F.; Cass, N.D.; Tawfik, K.O.; Bennett, M.L.; O’Malley, M.R.; Haynes, D.S.; Perkins, E.L. Cochlear Implantation Outcomes in Observed Vestibular Schwannoma: A Preliminary Report. Otolaryngol.-Head Neck Surg. 2022, 167, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Urban, M.J.; Moore, D.M.; Kwarta, K.; Leonetti, J.; Rajasekhar, R.; Gluth, M.B.; Wiet, R.M. Ipsilateral Cochlear Implantation in the Presence of Observed and Irradiated Vestibular Schwannomas. Ann. Otol. Rhinol. Laryngol. 2020, 129, 1229–1238. [Google Scholar] [CrossRef] [PubMed]
- Arnoldner, C.; Schwarz-Nemec, U.; Auinger, A.B.; Yildiz, E.; Matula, C.; Dahm, V. A novel scoring system based on small vestibular schwannomas to determine consideration for cochlear implantation. Clin. Otolaryngol. 2021, 46, 1223–1228. [Google Scholar] [CrossRef] [PubMed]
- Laborai, A.; Ghiselli, S.; Cuda, D. Cochlear Implant in Patients with Intralabyrinthine Schwannoma without Tumor Removal. Audiol. Res. 2022, 12, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Jia, H.; Nguyen, Y.; De Seta, D.; Hochet, B.; Smail, M.; Wu, H.; Mosnier, I.; Kalamarides, M.; Sterkers, O. Management of sporadic vestibular schwannoma with contralateral nonserviceable hearing. Laryngoscope 2020, 130, E407–E415. [Google Scholar] [CrossRef]
- Bs, L.A.A.; Carlson, M.L.; Do, E.M.H.; Cueva, R.A.; Van Gompel, J.J. Electrode Alternative for Eighth Nerve Monitoring During Vestibular Schwannoma Resection. Laryngoscope 2021, 131, E759–E763. [Google Scholar] [CrossRef]
- Delgado-Vargas, B.; Medina, M.; Polo, R.; Lloris, A.; Vaca, M.; Pérez, C.; Cordero, A.; Cobeta, I. Ossificazione cocleare dopo l’approccio translabirintico e le sue implicazioni per l’impianto cocleare. Acta Otorhinolaryngol. Ital. 2018, 38, 56–60. [Google Scholar] [CrossRef]
- Fujita, T.; Saito, K.; Kashiwagi, N.; Sato, M.; Seo, T.; Doi, K. The prevalence of vestibular schwannoma among patients treated as sudden sensorineural hearing loss. Auris Nasus Larynx 2019, 46, 78–82. [Google Scholar] [CrossRef]
- Eggink, M.C.; Frijns, J.H.; Sagers, J.E.; O’Malley, J.T.; Liberman, M.C.; Stankovic, K.M. Human vestibular schwannoma reduces density of auditory nerve fibers in the osseous spiral lamina. Hear. Res. 2022, 418, 108458. [Google Scholar] [CrossRef]
- Marx, M.; Mosnier, I.; Venail, F.; Mondain, M.; Uziel, A.; Bakhos, D.; Lescanne, E.; N’Guyen, Y.; Bernardeschi, D.; Sterkers, O.; et al. Cochlear Implantation and Other Treatments in Single-Sided Deafness and Asymmetric Hearing Loss: Results of a National Multicenter Study Including a Randomized Controlled Trial. Audiol. Neurotol. 2021, 26, 414–424. [Google Scholar] [CrossRef]
- Achena, A.; Achena, F.; Dragonetti, A.G.; Sechi, S.; Pili, A.W.; Locci, M.C.; Turnu, G.; Maniaci, A.; Ferlito, S. Cochlear Implant Evolving Indications: Our Outcomes in Adult Patients. Audiol. Res. 2022, 12, 414–422. [Google Scholar] [CrossRef]
- Plotkin, S.R.; Merker, V.L.; Halpin, C.; Jennings, D.; McKenna, M.J.; Harris, G.J.; Barker, F.G.I. Bevacizumab for Progressive Vestibular Schwannoma in Neurofibromatosis Type 2. Otol. Neurotol. 2012, 33, 1046–1052. [Google Scholar] [CrossRef]
- Walton, J.; Donnelly, N.P.; Tam, Y.C.; Joubert, I.; Durie-Gair, J.; Jackson, C.; Mannion, R.A.; Tysome, J.R.; Axon, P.R.; Scoffings, D.J. MRI Without Magnet Removal in Neurofibromatosis Type 2 Patients With Cochlear and Auditory Brainstem Implants. Otol. Neurotol. 2014, 35, 821–825. [Google Scholar] [CrossRef]
- Schwartz, N.; Rooth, M.A.; Dillon, M.T.; O’Connell, B.P.; Dedmon, M.M.; Huang, B.Y.; Brown, K.D. MRI surveillance following concurrent cochlear implantation in cases of vestibular schwannoma resection. Am. J. Otolaryngol.-Head Neck Med. Surg. 2020, 41, 102518. [Google Scholar] [CrossRef]
- Ay, N.; Gehl, H.B.; Sudhoff, H.; Todt, I. Effect of head position on cochlear implant MRI artifact. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 2763–2767. [Google Scholar] [CrossRef]
- Todt, I.; Rademacher, G.; Mittmann, P.; Wagner, J.; Mutze, S.; Ernst, A. MRI Artifacts and Cochlear Implant Positioning at 3 T In Vivo. Otol. Neurotol. 2015, 36, 972–976. [Google Scholar] [CrossRef]
- Elias, T.G.A.; Neto, A.P.; Zica, A.T.S.; Antunes, M.L.; Penido, N.D.O. Different clinical presentation of intralabyrinthine schwannomas—A systematic review. Braz. J. Otorhinolaryngol. 2019, 85, 111–120. [Google Scholar] [CrossRef]
- Reda, J.D.; West, N.; Cayé-Thomasen, P. Intracochlear Vestibular Schwannoma Presenting with Mixed Hearing Loss. J. Int. Adv. Otol. 2021, 17, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Carlson, M.L.; Neff, B.A.; Sladen, D.P.; Link, M.J.; Driscoll, C.L. Cochlear Implantation in Patients With Intracochlear and Intralabyrinthine Schwannomas. Otol. Neurotol. 2016, 37, 647–653. [Google Scholar] [CrossRef] [PubMed]
- Plontke, S.K.; Fröhlich, L.; Cozma, S.; Koitschev, A.; Reimann, K.; Weiß, R.; Götze, G.; Seiwerth, I.; Kösling, S.; Rahne, T. Hearing rehabilitation after subtotal cochleoectomy using a new, perimodiolar malleable cochlear implant electrode array: A preliminary report. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 353–362. [Google Scholar] [CrossRef]
- Mazzoni, A.; Zanoletti, E.; Cazzador, D.; Calvanese, L.; D’Avella, D.; Martini, A. Transmeatal microsurgery for intralabyrinthine and intrameatal schwannomas: A reappraisal. Acta Otorhinolaryngol. Ital. 2020, 40, 390–395. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study | Study Design | Groups | Inclusion Criteria | Tumor Size (Mean) | Audiological Results | Follow-Up (Months) | Surgical Timing | Intraoperative Monitoring |
|---|---|---|---|---|---|---|---|---|
| Conway et al., 2021 [14] | PS | 14 (sporadic VS) | Size < or equal to 2 cm | 7 mm (3–16 mm) | Improvement in AzBIO quiet, +10, +5 SNR, and CNC affected | 3 | S (1 D) | no |
| Sanna et al., 2016 [15] | PS | 13 (sporadic VS) | Hearing classes A and B; intrameatal tumor or Kanzaki class I, 18 > age | - | Discrete improvement in PTA (low frequencies), disyllabic word recognition, sentence recognition, and common phrase comprehension (p > 0.05); Improvement in binaural hearing and subjective questionnaires | 6 | S | no |
| Rooth et al., 2017 [16] | PS | 7 (sporadic VS) | T size < 15 mm; contralateral PTA < or equal to 35 dB HL; | 4–15 mm | Five out of seven had auditory perception; improvement in localization abilities; Improvement in AzBIO scores at 0 dB SNR; CNC did not demonstrate any improvement; Improvements in tinnitus (THI) and SSQ | 6 | S | no |
| Sorrentino et al., 2021 [17] | RS | 17 (8 sporadic and 9 NF2-associated VSs) | Institution protocol for VS surgery and CI implantation | 10 mm (9.3 in sporadic VS, 13.0 in NF2) | 77.8% were active users; Median postoperative PTA 45.6 dB nHL, median WRS = 40%; median postoperative PTA in the implanted ear was better in the group with impaired contralateral hearing; Good preoperative contralateral hearing status was negative prognostic factor for CI performance | 24 | 10 S, 7 Dto failed HPS | no |
| Thompson et al., 2019 [18] | RS | 41 (29 sporadic VS, 12 NF2) | - | 13 mm (2–40 mm) | 85% of patients achieved audibility with CI (75% high-intermediate performers, 25% low performers); Improved sound localization and subjective benefits | - | - | - |
| West et al., 2019 [19] | RS | 86 (53 sporadic VS, 33 NF2) | Simultaneous (single-stage) VS removal and ipsilateral cochlear implantation, original study types including case reports | 18 mm (NF2) 5 mm (sporadic) | SDS mean performance scores (including patients with no audibility) were 65% for monosyllables, 58% for bisyllables, and 57% for sentences. Tumor size: 7 mm in high performers, 10 mm in low performers; 78% of the patients with preoperative hearing class A or B had postoperative high performance, while this was only the case for 51% of the patients with preoperative hearing class C or D; Improvement in tinnitus | - | - | - |
| Wick et al., 2020 [20] | RS | 93 (46 in Group 1, simultaneous; 47 in Group 2, sequential) | - | Group 1: 12 mm; Group 2: 15 mm | GROUP 1 VS. GROUP 2 Open-set speech reached in 50% VS. 59.6%; Word score mean 52% VS. 37.9%; Sentence score mean 65.4% VS. 49.6% | 32.3 (1); 36.9 (2) | 46 S/47 D | 3 cases eABR |
| Bartindale et al., 2021 [21] | RS | 45 (sporadic VS) | (1) Sporadic VS, (2) CI placed on the side of the VS, (3) at least 6-month follow-up after their CI was placed, (4) CI auditory outcomes reported, and (5) patients with NF2 were excluded | - | Average SDS was 56.4% with a standard deviation of 27.6; AzBio testing (Arizona Biomedical Institute sentence test) showed an average of 75%. The average postimplant audiometry threshold was 28.8 dB; Neither tumor resection status, tumor location, duration of deafness, ipsilateral PTA, nor timing of CI placement had a significant effect on patient outcomes | Mean 20.2 | S/D | ePS |
| Tian et al., 2021 [22] | RS | 33 | Ipsilateral cochlear implantation outcomes after radiotherapy (all types) of VS (both sporadic and NF2) were included. | 20.5 mm | HINT mean score 71%; BKB mean score 52%; CNC test mean score 51%; CUNY mean score 78%; Postoperative PTA mean value 35 dB | Mean 18.5 | - | ePS; eCAP |
| Borsetto et al., 2019 [23] | RS | 50 (5 sporadic vs, 45 NF2) GROUP 1: RT Group 2: Observation | (1) Had a VS, either sporadic or NF2-associated, (2) had undergone CI, (3) had not undergone surgical treatment for their VS prior to CI, and (4) had hearing outcome measures post-CI reported. Patients who received Bevacizumab to control tumor growth after CI were included in this review. | 21 mm (1) | The mean post-CI pure-tone average for the radiotherapy group was 33 ± 20 dB (n = 9) versus 39 ± 9 dB (n = 4) for the observation group. Furthermore, comparison of speech perception scores also revealed no consistent differences between the two groups (SRS, WRS, HINT, CUNY, CNC) | 12 (most studies) | - | - |
| Longino et al., 2021 [24] | RS | 7 | VS managed with observation alone and underwent ipsilateral CI without prior surgery or radiotherapy | - | Average improvement in CNC word score preimplantation to 12 months postimplantation was 49% (range, 24–88%). Average improvement in AzBio of 45% when compared with preimplantation testing (range, 23–80%; n = 6). | 12 | - | - |
| Urban et al., 2020 [25] | RS | 7 (4 sporadic VS, 3 NF2) | All cases of cochlear implantation in patients with unresected vestibular schwannomas | - | Mean postoperative sentence score was 63.9% (range 48–91). Average postimplant CNC word scores were available for five patients and averaged 59%. | 28 | ||
| Arnoldner et al., 2021 [26] | Clinical Experience | 10 | Sporadic VS showing growth on repeat imaging studies, no ipsilateral functional hearing, desire to undergo cochlear implantation, and general good health. | - | Mean aided pure-tone average was 38 dB HL. Mean WRS was 28% at 65 dB and 52% at 80 dB. | 6 | S | eABR |
| Laborai et al., 2021 [27] | Case report | 2 patients | Intralabyrinthine schwannoma without tumor removal | - |
| 6 | - | - |
| Jia et al., 2019 [28] | Retrospective case review | 3 patients | Patients with IVS in whom cochlear implantation had been performed. | - |
| 60 (except 3 patient) | S | - |
| Category | Definition | Points |
|---|---|---|
| Koos Grading | Koos 4 Koos 3 Koos 2 Koos 1 | 0 1 2 3 |
| Extension | Transmodiolar extension Infiltration of modiolus Contact with modiolus No contact, no infiltration of modiolus | 0 1 2 3 |
| Hearing | Complete hearing loss Some residual hearing (0% monosyllables) ≥1% monosyllables, any PTA | 0 1 |
| PS EABR | No response Unclear wave V Stable wave V | 0 1 2 |
| Total score | Class IV Class III Class II Class I | 0–3 4–5 6–7 8–10 |
| Tumor Size (mm) | Decision Factors: Hearing (Tokyo Hearing Class) and/or Growth | Treatment |
|---|---|---|
| T < 10 | Good hearing [< 30 PTA/>70% SDS (A-B Tokyo)] | Hearing preservation surgery (or Observation) (CI in HPS failures) |
| Good hearing surgical risk, not growing tumors; Good hearing surgical risk, growing tumors | Observation; Radiotherapy | |
| Bad hearing (C-D Tokyo), not growing tumors. Bad hearing, growing tumors | Observation; Surgery and CI rehabilitation | |
| T 10–15 | Not growing tumors | Surgery (or Observation) |
| Growing tumors | Surgery | |
| Not growing tumors + surgical risk Growing tumors + surgical risk | Observation; Radiotherapy | |
| T 15–25 | - | Surgery or Radiotherapy |
| T > 25 | - | Surgery |
| Surgical risk | Partial Surgery and Radiotherapy | |
| Any Size | Cystic tumor | Surgery |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iannacone, F.P.; Visconti, F.; Zanoletti, E. How Cochlear Implant Rehabilitation Impacts the Therapeutic Strategy for Vestibular Schwannoma. Audiol. Res. 2023, 13, 116-129. https://doi.org/10.3390/audiolres13010012
Iannacone FP, Visconti F, Zanoletti E. How Cochlear Implant Rehabilitation Impacts the Therapeutic Strategy for Vestibular Schwannoma. Audiology Research. 2023; 13(1):116-129. https://doi.org/10.3390/audiolres13010012
Chicago/Turabian StyleIannacone, Francesco P., Francesca Visconti, and Elisabetta Zanoletti. 2023. "How Cochlear Implant Rehabilitation Impacts the Therapeutic Strategy for Vestibular Schwannoma" Audiology Research 13, no. 1: 116-129. https://doi.org/10.3390/audiolres13010012
APA StyleIannacone, F. P., Visconti, F., & Zanoletti, E. (2023). How Cochlear Implant Rehabilitation Impacts the Therapeutic Strategy for Vestibular Schwannoma. Audiology Research, 13(1), 116-129. https://doi.org/10.3390/audiolres13010012