

A Protocol to Investigate Deep Brain Stimulation for Refractory Tinnitus: From Rat Model to the Set-Up of a Human Pilot Study

 , ,
, , 

Abstract
:1. Introduction
2. Methods
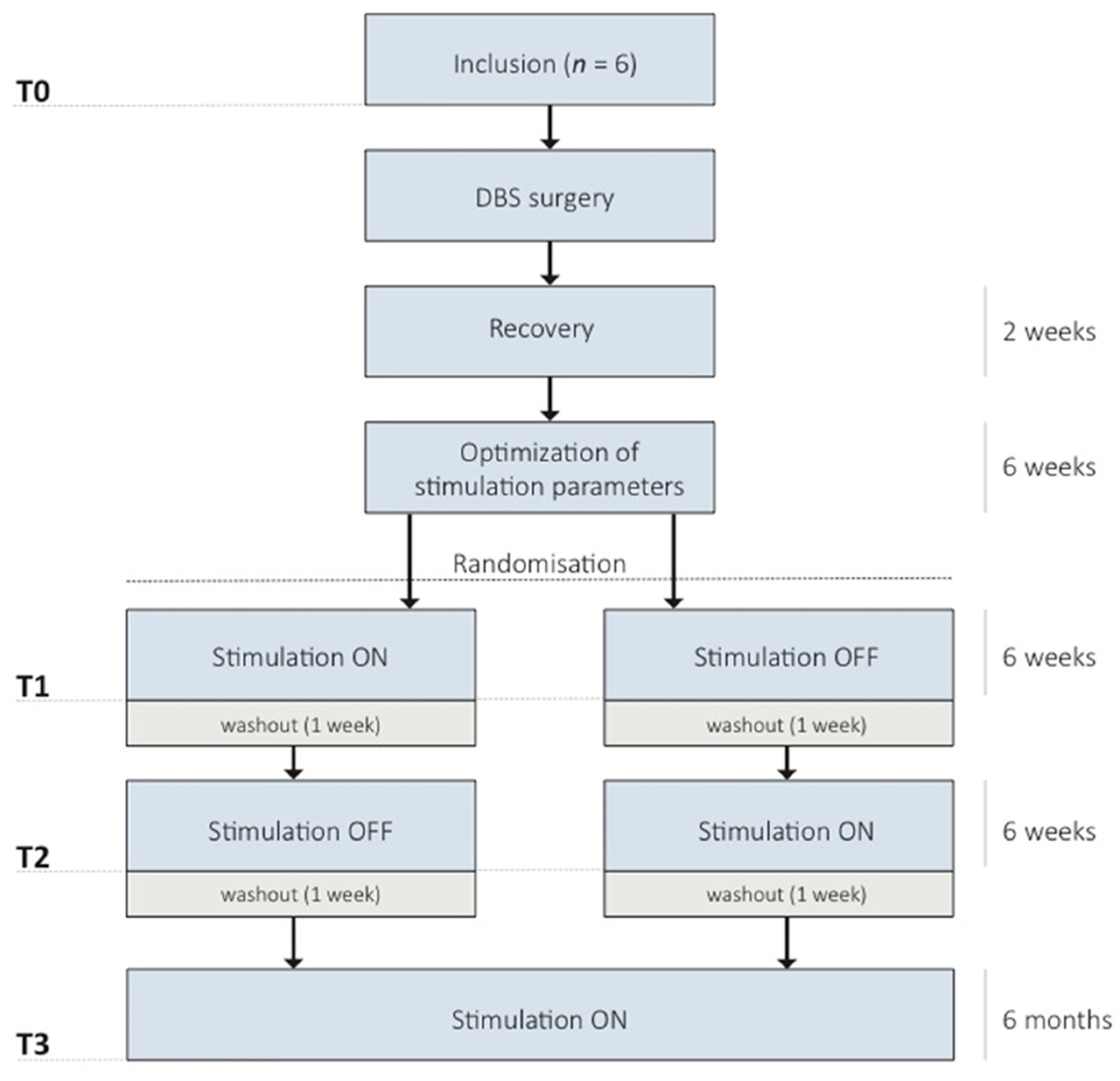
2.1. Study Design
2.2. Setting
2.3. Recruitment and Consent
2.4. Outcomes
2.4.1. Primary Outcomes
2.4.2. Secondary Outcomes
- Tinnitus severity will be assessed with the Tinnitus Functional Index (TFI) [62]. The TFI is a validated self-report questionnaire that measures the overall severity of tinnitus and provides coverage of multiple tinnitus severity domains. This questionnaire is the most appropriate responsive measure of treatment-related change. The TFI is translated and validated for Dutch native speakers [63].
- Tinnitus loudness and burden will be measured by VAS. This will be performed three times daily within a week, which is repeated four times during the study. Furthermore, these VAS scores will be used to assess the effect of stimulation on tinnitus during surgery. VAS ratings for tinnitus loudness and burden are often used in both clinical practice and experimental and descriptive research as a measure of subjective symptoms [64]. Both scales have been shown to correlate with the scores on Tinnitus Questionnaires [65].
- The hearing function will be assessed with pure tone and speech audiometry. These are clinical standard audiometric tests. Furthermore, subjective hearing will be evaluated using patient feedback.
- Cognitive functioning will be measured using a validated test battery for standard DBS care. These include the Boston Naming Test, Verbal Fluency, Letter Fluency, 15 Words Test, Trail Making Test part A and B, and the Stroop Color-Word Test.
- Quality of life and psychological functioning will be assessed by the following psychological questionnaires: 36-Item Short Form Health Survey (SF-36), Beck Depression Inventory II (BDI-II), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale (HADS).
- Neurophysiological measurements: electrophysiological data and auditory brainstem responses will be recorded before and after surgery (T0 and recovery) and at the end of treatment periods I and II (T1 and T2). Furthermore, local field potentials (LFP) will be recorded during surgery and before the implantation of the pulse generator. Details are described under ‘Neurophysiological assessments’.
3. Intervention
3.1. Implantation of DBS Electrodes and Internal Pulse Generator
3.2. Stimulation Parameters
3.3. Neurophysiological Assessments
3.4. Randomization and Blinding
3.5. Data Collection and Management
3.6. Statistical Analyses
3.7. Sample Size
3.8. Patient and Public Involvement
4. Discussion
5. Trial Status
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| DBS | Deep brain stimulation |
| MGB | Medial geniculate body |
| TFI | Tinnitus Functional Index |
| VAS | Visual Analogue Scales |
| MUMC+ | Maastricht University Medical Center |
| TQ | Tinnitus questionnaire |
| SF-36 | 36-Item Short Form Health Survey |
| BDI-II | Beck Depression Inventory II |
| BAI | Beck Anxiety Inventory |
| HADS | Hospital Anxiety and Depression Scale |
| LFP | Local field potentials |
| CTCM | Clinical Trial Center Maastricht |
| EDC | Electronic Data Capture |
| STN | subthalamic nucleus |
| AC-PC | Anterior Commissure-Posterior Commissure |
| ANT | Anterior Nucleus of the Thalamus |
| GPi | Globus Pallidus Internus |
References
- Henry, J.A.; Dennis, K.C.; Schechter, M.A. General review of tinnitus: Prevalence, mechanisms, effects, and management. J Speech Lang. Hear. Res. 2005, 48, 1204–1235. [Google Scholar] [CrossRef]
- American National Health and Nutrition Examination Survey, Audiometry section (AUQ_G). Data Documentation, Codebook, and Frequencies. 2011–2012. Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2011-2012/AUQ_G.htm (accessed on 1 December 2022).
- Andersson, G.; Freijd, A.; Baguley, D.M.; Idrizbegovic, E. Tinnitus distress, anxiety, depression, and hearing problems among cochlear implant patients with tinnitus. J. Am. Acad. Audiol. 2009, 20, 315–319. [Google Scholar] [CrossRef]
- Langguth, B.; Landgrebe, M.; Kleinjung, T.; Sand, G.P.; Hajak, G. Tinnitus and depression. World J. Biol. Psychiatry 2011, 12, 489–500. [Google Scholar] [CrossRef] [PubMed]
- Zoger, S.; Svedlund, J.; Holgers, K.M. Relationship between tinnitus severity and psychiatric disorders. Psychosomatics 2006, 47, 282–288. [Google Scholar] [CrossRef]
- Maes, I.H.; Cima, R.F.; Vlaeyen, J.W.; Anteunis, L.J.; Joore, M.A. Tinnitus: A cost study. Ear Hear. 2013, 34, 508–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Langguth, B.; Kreuzer, P.M.; Kleinjung, T.; De Ridder, D. Tinnitus: Causes and clinical management. Lancet Neurol. 2013, 12, 920–930. [Google Scholar] [CrossRef] [PubMed]
- Cima, R.F.F.; Mazurek, B.; Haider, H.; Kikidis, D.; Lapira, A.; Noreña, A.; Hoare, D.J. A multidisciplinary European guideline for tinnitus: Diagnostics, assessment, and treatment. HNO 2019, 67 (Suppl. 1), 10–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kochkin, S.; Tyler, R. Tinnitus treatment and the effectiveness of hearing aids: Hearing care professional perceptions. Hear. Rev. 2008, 15, 14–18. [Google Scholar]
- Trotter, M.I.; Donaldson, I. Hearing aids and tinnitus therapy: A 25-year experience. J. Laryngol. Otol. 2008, 122, 1052–1056. [Google Scholar] [CrossRef]
- Jastreboff, P.J. Tinnitus retraining therapy. Br. J. Audiol. 1999, 33, 68–70. [Google Scholar]
- Cima, R.F.; Andersson, G.; Schmidt, C.J.; Henry, J.A. Cognitive-behavioral treatments for tinnitus: A review of the literature. J. Am. Acad. Audiol. 2014, 25, 29–61. [Google Scholar] [CrossRef] [PubMed]
- Eggermont, J.J.; Roberts, L.E. The neuroscience of tinnitus: Understanding abnormal and normal auditory perception. Front. Syst. Neurosci. 2012, 6, 53. [Google Scholar] [CrossRef] [PubMed]
- Levine, R.A.; Nam, E.C.; Oron, Y.; Melcher, J.R. Evidence for a tinnitus subgroup responsive to somatosensory based treatment modalities. Prog. Brain Res. 2007, 166, 195–207. [Google Scholar] [PubMed]
- Durai, M.; Sanders, M.; Kobayashi, K.; Searchfield, G.D. Auditory streaming and prediction in tinnitus sufferers. Ear Hear. 2019, 40, 345–357. [Google Scholar] [CrossRef]
- Rauschecker, J.P.; May, E.S.; Maudoux, A.; Ploner, M. Frontostriatal gating of tinnitus and chronic pain. Trends Cogn. Sci. 2015, 19, 567–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norena, A.J. An integrative model of tinnitus based on a central gain controlling neural sensitivity. Neurosci. Biobehav. Rev. 2011, 35, 1089–1109. [Google Scholar] [CrossRef]
- Eggermont, J.J. Pathophysiology of tinnitus. Prog. Brain Res. 2007, 166, 19–35. [Google Scholar]
- Grill, W.M.; Snyder, A.N.; Miocinovic, S. Deep brain stimulation creates an informational lesion of the stimulated nucleus. Neuroreport 2004, 15, 1137–1140. [Google Scholar] [CrossRef]
- Chiken, S.; Nambu, A. Disrupting neuronal transmission: Mechanism of DBS? Front. Syst. Neurosci. 2014, 8, 33. [Google Scholar] [CrossRef] [Green Version]
- Cheung, S.W.; Larson, P.S. Tinnitus modulation by deep brain stimulation in locus of caudate neurons (area LC). Neuroscience 2010, 169, 1768–1778. [Google Scholar] [CrossRef]
- Shi, Y.; Burchiel, K.J.; Anderson, V.C.; Martin, W.H. Deep brain stimulation effects in patients with tinnitus. Otolaryngol. Head Neck Surg. 2009, 141, 285–287. [Google Scholar] [CrossRef] [PubMed]
- Smit, J.V.; Janssen, M.L.; Engelhard, M.; de Bie, R.M.; Schuurman, P.R.; Contarino, M.F.; Mosch, A.; Temel, Y.; Stokroos, R. The impact of deep brain stimulation on tinnitus. Surg. Neurol. Int. 2016, 7 (Suppl. 35), S848–S854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, S.W.; Racine, C.A.; Henderson-Sabes, J.; Demopoulos, C.; Molinaro, A.M.; Heath, S.; Nagarajan, S.S.; Bourne, A.L.; Rietcheck, J.E.; Wang, S.S.; et al. Phase I trial of caudate deep brain stimulation for treatment-resistant tinnitus. J. Neurosurg. 2019, 133, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Dijkstra, E.; Figee, M.; Schuurman, P.R.; Denys, D. Effective deep brain stimulation of intractable tinnitus: A case study. Brain Stimul. 2018, 11, 1205–1207. [Google Scholar] [CrossRef]
- De Ridder, D.; Joos, K.; Vanneste, S. Anterior cingulate implants for tinnitus: Report of 2 cases. J. Neurosurg. 2016, 124, 893–901. [Google Scholar] [CrossRef] [Green Version]
- Larson, P.S.; Cheung, S.W. Deep brain stimulation in area LC controllably triggers auditory phantom percepts. Neurosurgery 2012, 70, 398–405; discussion 6. [Google Scholar] [CrossRef]
- Arts, R.A.; George, E.L.; Stokroos, R.J.; Vermeire, K. Review: Cochlear implants as a treatment of tinnitus in single-sided deafness. Curr. Opin. Otolaryngol. Head Neck Surg. 2012, 20, 398–403. [Google Scholar] [CrossRef]
- Roberts, D.S.; Otto, S.; Chen, B.; Peng, K.A.; Schwartz, M.S.; Brackmann, D.E.; House, J.W. Tinnitus suppression after auditory brainstem implantation in patients with neurofibromatosis type-2. Otol. Neurotol. 2017, 38, 118–122. [Google Scholar] [CrossRef]
- Stegeman, I.; Velde, H.M.; Robe, P.; Stokroos, R.J.; Smit, A.L. Tinnitus treatment by vagus nerve stimulation: A systematic review. PLoS ONE 2021, 16, e0247221. [Google Scholar] [CrossRef]
- De Ridder, D.; De Mulder, G.; Verstraeten, E.; Van der Kelen, K.; Sunaert, S.; Smits, M. Primary and secondary auditory cortex stimulation for intractable tinnitus. ORL J. Otorhinolaryngol. Relat. Spec. 2006, 68, 48–54; discussion 5. [Google Scholar] [CrossRef]
- Deklerck, A.N.; Marechal, C.; Perez Fernandez, A.M.; Keppler, H.; Van Roost, D.; Dhooge, I.J.M. Invasive neuromodulation as a treatment for tinnitus: A systematic review. Neuromodulation 2020, 23, 451–462. [Google Scholar] [CrossRef] [PubMed]
- Kandler, K.; Kaltenbach, J.A.; Godfrey, D.A. The cochlear nucleus as a generator of tinnitus-related signals. In The Oxford Handbook of the Auditory Brainstem; Oxford University Press: Oxford, UK, 2019; pp. 188–222. [Google Scholar]
- Jacquemin, L.; Mertens, G.; Shekhawat, G.S.; Van de Heyning, P.; Vanderveken, O.M.; Topsakal, V. High definition transcranial direct current stimulation (HD-tDCS) for chronic tinnitus: Outcomes from a prospective longitudinal large cohort study. Prog. Brain Res. 2021, 263, 137–152. [Google Scholar] [PubMed]
- Hoekstra, C.E.; Versnel, H.; Neggers, S.F.; Niesten, M.E.; van Zanten, G.A. Bilateral low-frequency repetitive transcranial magnetic stimulation of the auditory cortex in tinnitus patients is not effective: A randomised controlled trial. Audiol. Neuro Otol. 2013, 18, 362–373. [Google Scholar] [CrossRef]
- Bergman, H.; Wichmann, T.; Karmon, B.; DeLong, M.R. The primate subthalamic nucleus. II. Neuronal activity in the MPTP model of parkinsonism. J. Neurophysiol. 1994, 72, 507–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benazzouz, A.; Breit, S.; Koudsie, A.; Pollak, P.; Krack, P.; Benabid, A.L. Intraoperative microrecordings of the subthalamic nucleus in Parkinson’s disease. Mov. Disord. 2002, 17 (Suppl. 3), S145–S149. [Google Scholar] [CrossRef]
- Janssen, M.L.; Zwartjes, D.G.; Tan, S.K.; Vlamings, R.; Jahanshahi, A.; Heida, T.; Hoogland, G.; Steinbusch, H.W.; Visser-Vandewalle, V.; Temel, Y. Mild dopaminergic lesions are accompanied by robust changes in subthalamic nucleus activity. Neurosci. Lett. 2012, 508, 101–105. [Google Scholar] [CrossRef]
- Kalappa, B.I.; Brozoski, T.J.; Turner, J.G.; Caspary, D.M. Single unit hyperactivity and bursting in the auditory thalamus of awake rats directly correlates with behavioural evidence of tinnitus. J. Physiol. 2014, 592, 5065–5078. [Google Scholar] [CrossRef] [Green Version]
- Bartlett, E.L. The organization and physiology of the auditory thalamus and its role in processing acoustic features important for speech perception. Brain Lang. 2013, 126, 29–48. [Google Scholar] [CrossRef] [Green Version]
- Turner, J.G.; Brozoski, T.J.; Bauer, C.A.; Parrish, J.L.; Myers, K.; Hughes, L.F.; Caspary, D.M. Gap detection deficits in rats with tinnitus: A potential novel screening tool. Behav. Neurosci. 2006, 120, 188–195. [Google Scholar] [CrossRef]
- Koch, M. The neurobiology of startle. Prog. Neurobiol. 1999, 59, 107–128. [Google Scholar] [CrossRef]
- Van Zwieten, G.; Jahanshahi, A.; van Erp, M.L.; Temel, Y.; Stokroos, R.J.; Janssen, M.L.F. Alleviation of tinnitus with high-frequency stimulation of the dorsal cochlear nucleus: A rodent study. Trends Hear. 2019, 23, 2331216519835080. [Google Scholar] [CrossRef] [Green Version]
- Luo, H.; Zhang, X.; Nation, J.; Pace, E.; Lepczyk, L.; Zhang, J. Tinnitus suppression by electrical stimulation of the rat dorsal cochlear nucleus. Neurosci. Lett. 2012, 522, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Ahsan, S.F.; Luo, H.; Zhang, J.; Kim, E.; Xu, Y. An animal model of deep brain stimulation for treating tinnitus: A proof of concept study. Laryngoscope 2018, 128, 1213–1222. [Google Scholar] [CrossRef]
- Smit, J.V.; Janssen, M.L.; van Zwieten, G.; Jahanshahi, A.; Temel, Y.; Stokroos, R.J. Deep brain stimulation of the inferior colliculus in the rodent suppresses tinnitus. Brain Res. 2016, 1650, 118–124. [Google Scholar] [CrossRef] [PubMed]
- Van Zwieten, G.; Janssen, M.L.F.; Smit, J.V.; Janssen, A.M.L.; Roet, M.; Jahanshahi, A. Inhibition of experimental tinnitus with high frequency stimulation of the rat medial geniculate body. Neuromodulation 2018, 22, 416–424. [Google Scholar] [CrossRef] [Green Version]
- Smit, J.V.; Jahanshahi, A.; Janssen, M.L.F.; Stokroos, R.J.; Temel, Y. Hearing assessment during deep brain stimulation of the central nucleus of the inferior colliculus and dentate cerebellar nucleus in rat. PeerJ 2017, 5, e3892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smit, J.V.; Janssen, M.L.; Schulze, H.; Jahanshahi, A.; Van Overbeeke, J.J.; Temel, Y.; Stokroos, R. Deep brain stimulation in tinnitus: Current and future perspectives. Brain Res. 2015, 1608, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Van Zwieten, G.; Smit, J.V.; Jahanshahi, A.; Temel, Y.; Stokroos, R.J. Tinnitus: Is there a place for brain stimulation? Surg. Neurol. Int. 2016, 7 (Suppl. 4), S125–S129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rammo, R.; Ali, R.; Pabaney, A.; Seidman, M.; Schwalb, J. Surgical neuromodulation of tinnitus: A review of current therapies and future applications. Neuromodulation 2018, 22, 380–387. [Google Scholar] [CrossRef]
- Leaver, A.M.; Renier, L.; Chevillet, M.A.; Morgan, S.; Kim, H.J.; Rauschecker, J.P. Dysregulation of limbic and auditory networks in tinnitus. Neuron 2011, 69, 33–43. [Google Scholar] [CrossRef] [Green Version]
- Rauschecker, J.P.; Leaver, A.M.; Muhlau, M. Tuning out the noise: Limbic-auditory interactions in tinnitus. Neuron 2010, 66, 819–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kraus, K.S.; Canlon, B. Neuronal connectivity and interactions between the auditory and limbic systems. Effects of noise and tinnitus. Hear. Res. 2012, 288, 34–46. [Google Scholar] [CrossRef] [PubMed]
- De Ridder, D.; Vanneste, S.; Weisz, N.; Londero, A.; Schlee, W.; Elgoyhen, A.B. An integrative model of auditory phantom perception: Tinnitus as a unified percept of interacting separable subnetworks. Neurosci. Biobehav. Rev. 2014, 44, 16–32. [Google Scholar] [CrossRef] [PubMed]
- Arts, R.A.; George, E.L.; Griessner, A.; Zierhofer, C.; Stokroos, R.J. Tinnitus suppression by intracochlear electrical stimulation in single-sided deafness: A prospective clinical trial—Part I. Audiol. Neuro Otol. 2015, 20, 294–313. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.; Vlamings, R.; Lim, L.; Sesia, T.; Janssen, M.L.; Steinbusch, H.W.; Visser-Vandewalle, V.; Temel, Y. Experimental deep brain stimulation in animal models. Neurosurgery 2010, 67, 1073–1079; discussion 80. [Google Scholar] [CrossRef]
- Ackermans, L.; Duits, A.; van der Linden, C.; Tijssen, M.; Schruers, K.; Temel, Y.; Kleijer, M.; Nederveen, P.; Bruggeman, R.; Tromp, S. Double-blind clinical trial of thalamic stimulation in patients with Tourette syndrome. Brain 2011, 134, 832–844. [Google Scholar] [CrossRef] [Green Version]
- Janssen, M.L.; Zwartjes, D.G.; Temel, Y.; van Kranen-Mastenbroek, V.; Duits, A.; Bour, L.J.; Veltink, P.H.; Heida, T.; Visser-Vandewalle, V. Subthalamic neuronal responses to cortical stimulation. Mov. Disord. 2012, 27, 435–438. [Google Scholar] [CrossRef]
- Joustra, J.; Buwalda, J.; Cima, R.; Free, R.H.; Hofman, R.; De Kleine, E. Dutch Tinnitus Guideline. Richtlijn Tinnitus. Nederlandse Vereniging voor Keel-Neus-Oorheelkunde en Heelkunde van het Hoofd-Halsgebied 2016. Available online: https://richtlijnendatabase.nl/richtlijn/tinnitus/tinnitus_-_startpagina.html (accessed on 1 December 2022).
- Hallam, R.S.; Jakes, S.C.; Hinchcliffe, R. Cognitive variables in tinnitus annoyance. Br. J. Clin. Psychol. 1988, 27, 213–222. [Google Scholar] [CrossRef]
- Meikle, M.B.; Henry, J.A.; Griest, S.E.; Stewart, B.J.; Abrams, H.B.; McArdle, R. The tinnitus functional index: Development of a new clinical measure for chronic, intrusive tinnitus. Ear Hear. 2012, 33, 153–176. [Google Scholar] [CrossRef]
- Rabau, S.; Wouters, K.; Van de Heyning, P. Validation and translation of the Dutch tinnitus functional index. B-ENT 2014, 10, 251–258. [Google Scholar]
- Cline, M.E.; Herman, J.; Shaw, E.R.; Morton, R.D. Standardization of the visual analogue scale. Nurs. Res. 1992, 41, 378–380. [Google Scholar] [CrossRef] [PubMed]
- Adamchic, I.; Langguth, B.; Hauptmann, C.; Tass, P.A. Psychometric evaluation of visual analog scale for the assessment of chronic tinnitus. Am. J.Audiol. 2012, 21, 215–225. [Google Scholar] [CrossRef]
- Schaper, F.; Zhao, Y.; Janssen, M.L.F.; Wagner, G.L.; Colon, A.J.; Hilkman, D.M.W.; Gommer, E.; Vlooswijk, M.C.G.; Hoogland, G.; Ackermans, L. Single-cell recordings to target the anterior nucleus of the thalamus in deep brain stimulation for patients with refractory epilepsy. Int. J. Neural. Syst. 2018, 29, 1850012. [Google Scholar] [CrossRef] [PubMed]
- Sherman, S.M. Thalamic relay functions. Prog. Brain Res. 2001, 134, 51–69. [Google Scholar]
- Schwartze, M.; Farrugia, N.; Kotz, S.A. Dissociation of formal and temporal predictability in early auditory evoked potentials. Neuropsychologia 2013, 51, 320–325. [Google Scholar] [CrossRef]
- Schwartze, M.; Tavano, A.; Schroger, E.; Kotz, S.A. Temporal aspects of prediction in audition: Cortical and subcortical neural mechanisms. Int. J. Psychophysiol. 2012, 83, 200–207. [Google Scholar] [CrossRef]
- Wilkinson, M.D.; Dumontier, M.; Aalbersberg, I.J.; Appleton, G.; Axton, M.; Baak, A.; Blomberg, N.; Boiten, J.W.; da Silva Santos, L.B.; Bourne, P.E. The FAIR Guiding Principles for scientific data management and stewardship. Sci. Data 2016, 3, 160018. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koek, R.J.; Langevin, J.P.; Krahl, S.E.; Kosoyan, H.J.; Schwartz, H.N.; Chen, J.W.; Melrose, R.; Mandelkern, M.J.; Sultzer, D. Deep brain stimulation of the basolateral amygdala for treatment-refractory combat post-traumatic stress disorder (PTSD): Study protocol for a pilot randomized controlled trial with blinded, staggered onset of stimulation. Trials 2014, 15, 356. [Google Scholar] [CrossRef] [Green Version]
- Devos, J.V.P.; Temel, Y.; Ackermans, L.; Visser-Vandewalle, V.; Onur, O.A.; Schruers, K.; Smit, J.; Janssen, M.L.F. Methodological considerations for setting up deep brain stimulation studies for new indications. J. Clin. Med. 2022, 11, 696. [Google Scholar] [CrossRef]
- Smit, J.V.; Pielkenrood, B.J.; Arts, R.; Janssen, M.L.; Temel, Y.; Stokroos, R.J. Patient acceptance of invasive treatments for tinnitus. Am. J. Audiol. 2018, 27, 184–196. [Google Scholar] [CrossRef]
- Grant, R.A.; Halpern, C.H.; Baltuch, G.H.; O’Reardon, J.P.; Caplan, A. Ethical considerations in deep brain stimulation for psychiatric illness. J. Clin. Neurosci. 2014, 21, 1–5. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Animal (Rodent) Studies | ||||||
|---|---|---|---|---|---|---|
| Reference | Design | Target | N | Uni/Bilateral | Stimulation | Outcome |
| Van Zwieten et al., 2019 [43] | Noise induced tinnitus, within-subject controlled | Dorsal Cochlear Nucleus | 10 | Bilateral | Continuous stimulation during test | GPIAS, tinnitus behavior was suppressed |
| Van Zwieten et al., 2018 [47] | Noise induced tinnitus, within-subject controlled | Medial Geniculate Body | 11 | Bilateral | Continuous stimulation during test | GPIAS, tinnitus behavior was suppressed |
| Ahsan et al., 2018 [45] | Noise induced tinnitus, within-subject controlled | Dorsal Cochlear Nucleus | 9 | Bilateral | Continuous stimulation during test | GPIAS, tinnitus behavior was suppressed |
| Smit et al., 2016 [46] | Noise induced tinnitus, within-subject controlled | Inferior Colliculus | 9 | Bilateral | Continuous stimulation during test | GPIAS, tinnitus behavior was suppressed |
| Luo et al., 2012 [44] | Noise induced tinnitus, within-subject controlled | Dorsal Cochlear Nucleus | 6 | Unilateral | Continuous stimulation during test | GPIAS, tinnitus behavior was suppressed |
| Human Studies | ||||||
| Reference | Design | Target | N | Uni/bilateral | Stimulation | Outcome |
| Cheung et al., 2019 [24] | Open-label, nonrandomized trial in refractory tinnitus patients | Caudate Nucleus | 6 | Bilateral | 24 weeks open label | TFI (3 responders), THI (4 responders) |
| Dijkstra et al., 2018 [25] | Case report in refractory tinnitus patients | Ventral anterior limb of the internal capsule & Nucleus Accumbens | 1 | Bilateral | 1 year | TFI (pre = 74, post = 46), THI (pre = 76, post = 32) |
| Inclusion Criteria | Exclusion Criteria |
|---|---|
|
|
| Inclusion (T0) | Surgery | Recovery | Optimization | Period I (T1) | Washout | Period II (T2) | Washout | Period III (T3) | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Visits and Procedures | ||||||||||
| Number of Outpatient visits | 2 | 6 | 1 | 1 | 1 | |||||
| Anesthesiology screening | • | |||||||||
| MRI | • | |||||||||
| CT | • | • | ||||||||
| Outcome Measures | ||||||||||
| Tinnitus severity | TFI | • | • | • | • | • | ||||
| Tinnitus loudness and burden: | VAS * | • | • | • | • | • | • | |||
| Hearing function: | Audiometry ABR | • | • | • | • | • | ||||
| • | • | • | • | • | ||||||
| Cognitive functioning ** | • | • | • | • | ||||||
| Psychological functioning *** | • | • | • | • | ||||||
| Neurophysiology: | EEG LFP | • | • | • | • | |||||
| • | • | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Zwieten, G.; Devos, J.V.P.; Kotz, S.A.; Ackermans, L.; Brinkmann, P.; Dauven, L.; George, E.L.J.; Janssen, A.M.L.; Kremer, B.; Leue, C.; et al. A Protocol to Investigate Deep Brain Stimulation for Refractory Tinnitus: From Rat Model to the Set-Up of a Human Pilot Study. Audiol. Res. 2023, 13, 49-63. https://doi.org/10.3390/audiolres13010005
van Zwieten G, Devos JVP, Kotz SA, Ackermans L, Brinkmann P, Dauven L, George ELJ, Janssen AML, Kremer B, Leue C, et al. A Protocol to Investigate Deep Brain Stimulation for Refractory Tinnitus: From Rat Model to the Set-Up of a Human Pilot Study. Audiology Research. 2023; 13(1):49-63. https://doi.org/10.3390/audiolres13010005
Chicago/Turabian Stylevan Zwieten, Gusta, Jana V. P. Devos, Sonja A. Kotz, Linda Ackermans, Pia Brinkmann, Lobke Dauven, Erwin L. J. George, A. Miranda L. Janssen, Bernd Kremer, Carsten Leue, and et al. 2023. "A Protocol to Investigate Deep Brain Stimulation for Refractory Tinnitus: From Rat Model to the Set-Up of a Human Pilot Study" Audiology Research 13, no. 1: 49-63. https://doi.org/10.3390/audiolres13010005
APA Stylevan Zwieten, G., Devos, J. V. P., Kotz, S. A., Ackermans, L., Brinkmann, P., Dauven, L., George, E. L. J., Janssen, A. M. L., Kremer, B., Leue, C., Schwartze, M., Temel, Y., Smit, J. V., & Janssen, M. L. F. (2023). A Protocol to Investigate Deep Brain Stimulation for Refractory Tinnitus: From Rat Model to the Set-Up of a Human Pilot Study. Audiology Research, 13(1), 49-63. https://doi.org/10.3390/audiolres13010005