
Ménière’s Disease: Insights from an Italian Nationwide Survey

 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
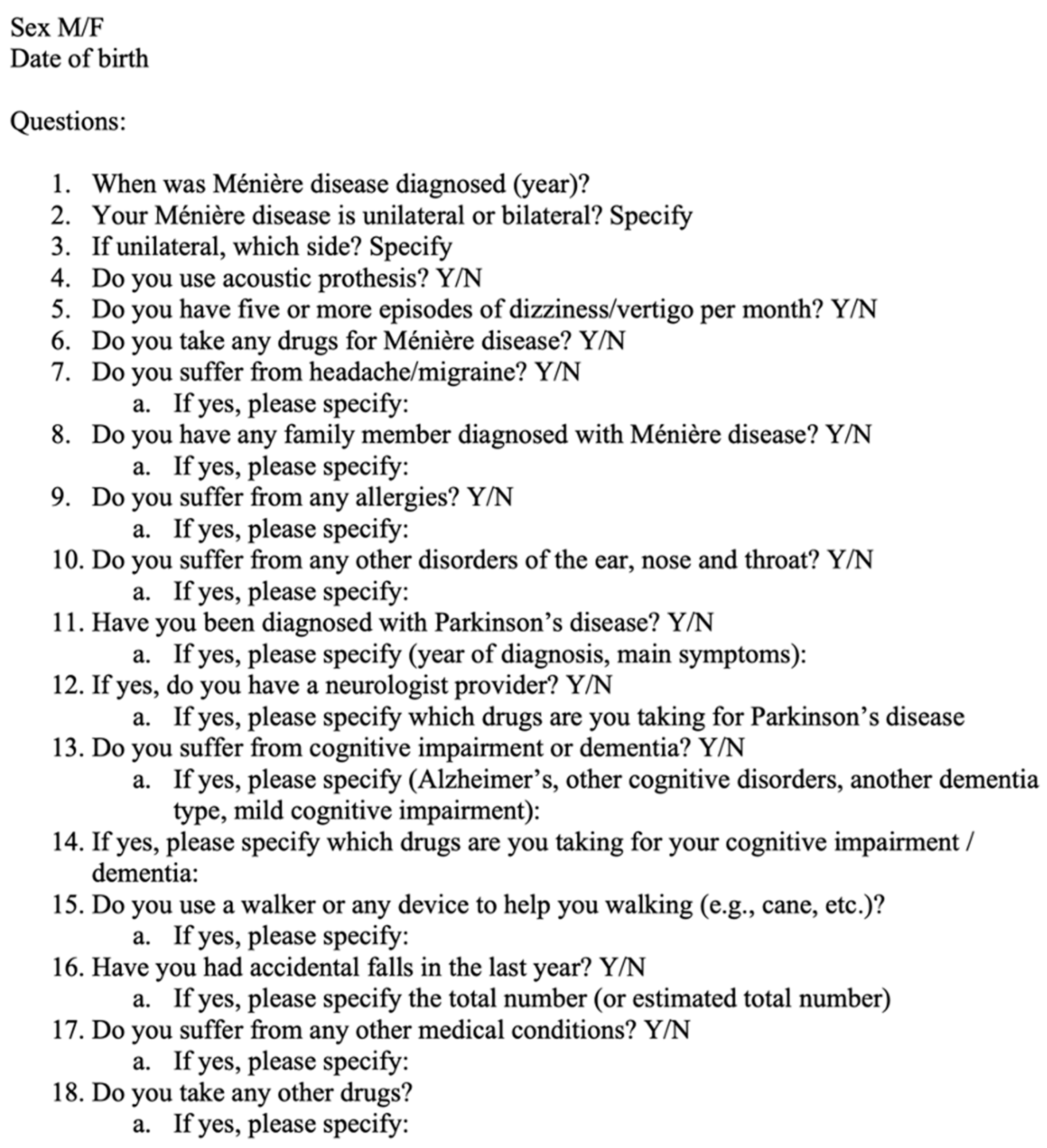
2. Materials and Methods
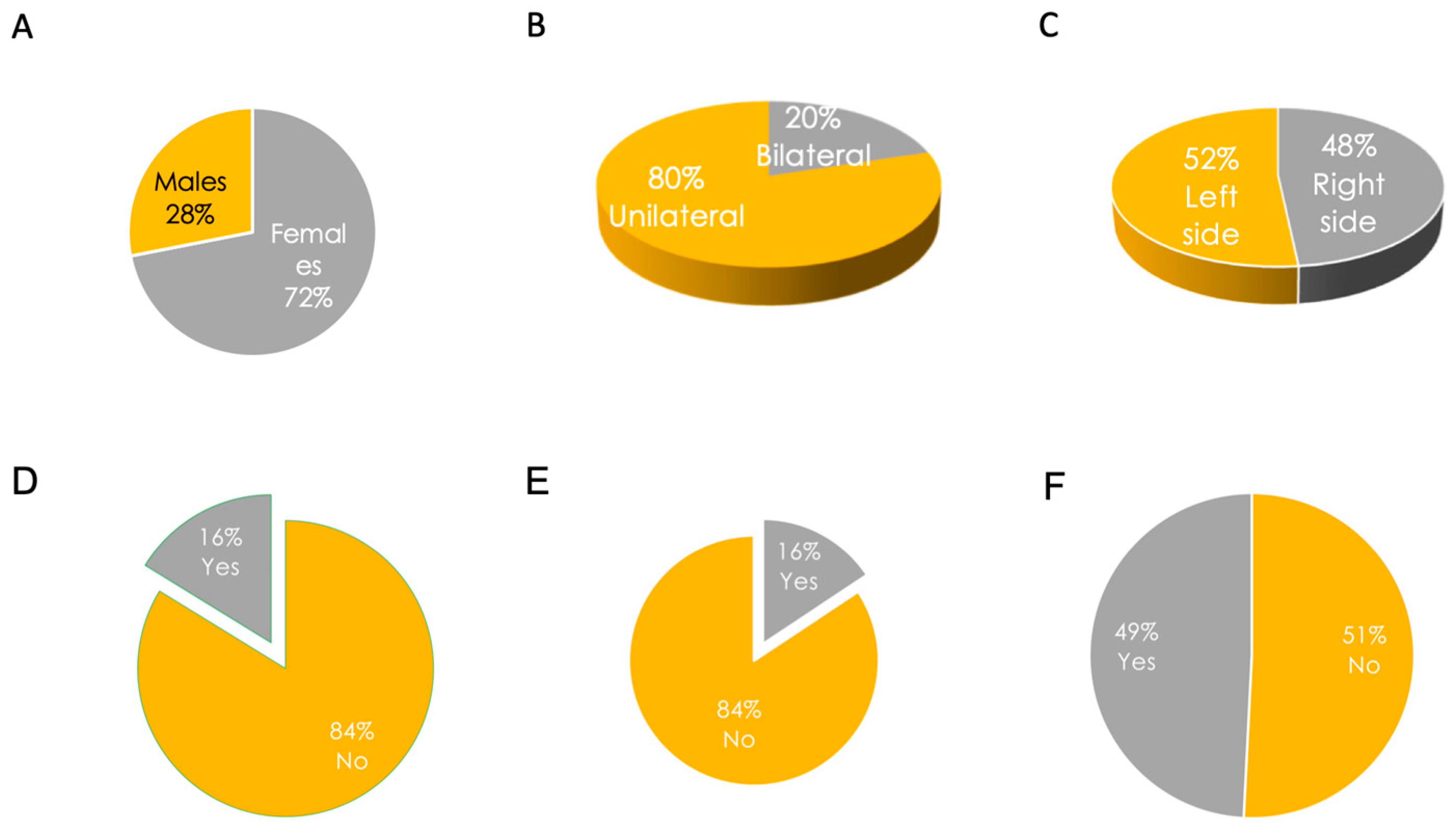
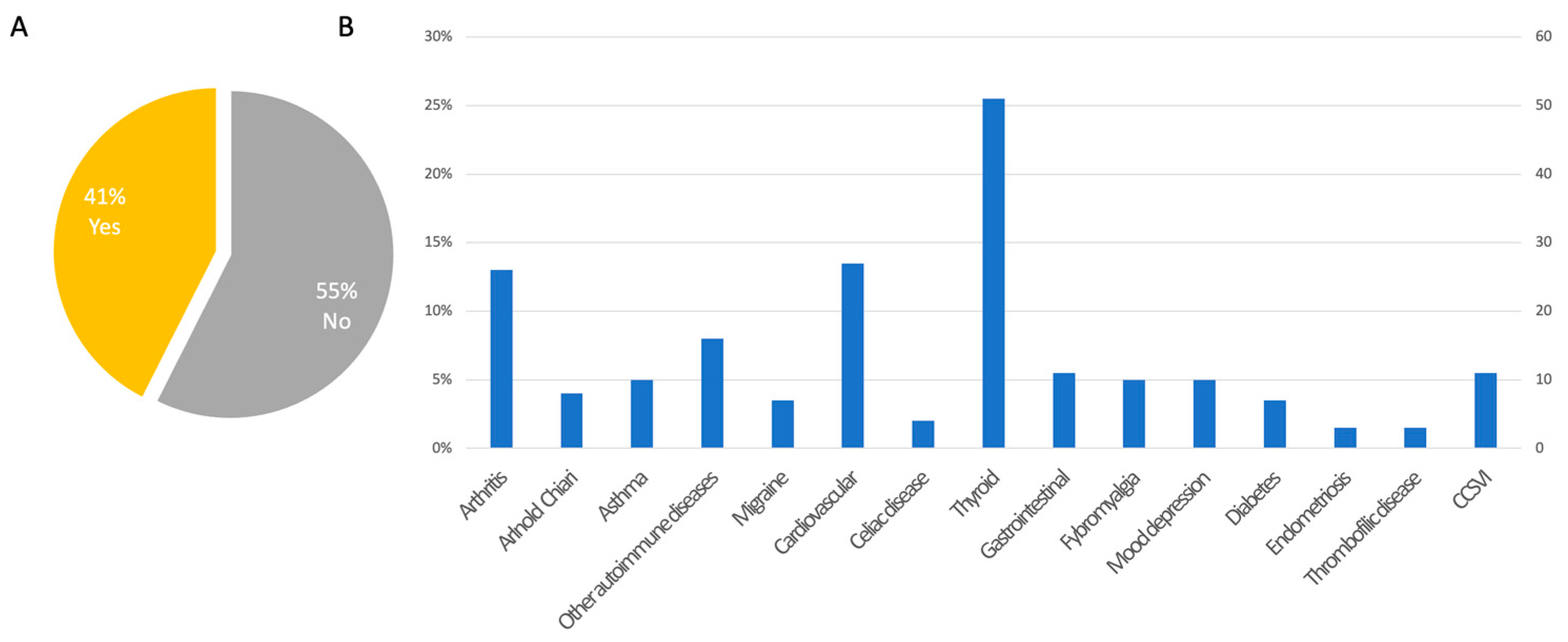
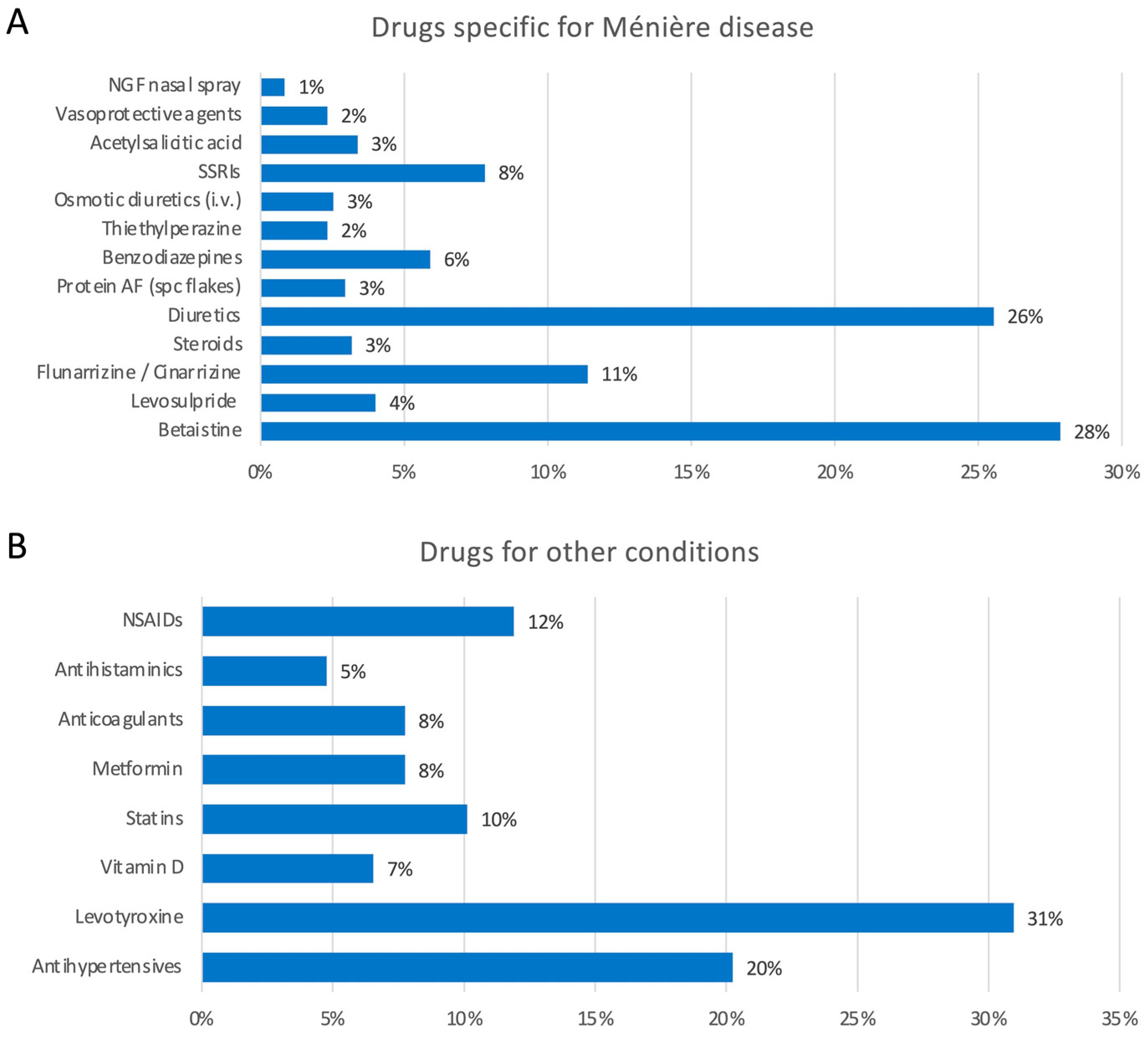
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Koenen, L.; Andaloro, C. Meniere Disease. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2022. [Google Scholar]
- Lopez-Escamez, J.A.; Carey, J.; Chung, W.-H.; Goebel, J.A.; Magnusson, M.; Mandalà, M.; Newman-Toker, D.E.; Strupp, M.; Suzuki, M.; Trabalzini, F.; et al. Diagnostic criteria for Menière’s disease. J. Vestib. Res. 2015, 25, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Balaker, A.E.; Ishiyama, P.; Lopez, I.A.; Ishiyama, G.; Ishiyama, A. Immunocytochemical Localization of the Translocase of the Outer Mitochondrial Membrane (Tom20) in the Human Cochlea. Anat. Rec. 2012, 296, 326–332. [Google Scholar] [CrossRef]
- Merchant, S.N.; Adams, J.C.; Nadol, J.B. Pathophysiology of Meniere’s Syndrome: Are Symptoms Caused by Endolymphatic Hydrops? Otol. Neurotol. 2005, 26, 74–81. [Google Scholar] [CrossRef] [Green Version]
- Morita, Y.; Takahashi, K.; Ohshima, S.; Yagi, C.; Kitazawa, M.; Yamagishi, T.; Izumi, S.; Horii, A. Is Vestibular Meniere’s Disease Associated With Endolymphatic Hydrops? Front. Surg. 2020, 7, 601692. [Google Scholar] [CrossRef]
- Foster, C.A.; Breeze, R.E. Endolymphatic Hydrops in Ménière’s Disease. Otol. Neurotol. 2013, 34, 1210–1214. [Google Scholar] [CrossRef]
- Woodworth, B.A.; Fitzpatrick, P.C.; Gianoli, G.J. Meniere’s disease. J. La. State Med. Soc. 2000, 152, 314–319. [Google Scholar]
- Ishiyama, G.; Lopez, I.A.; Sepahdari, A.R.; Ishiyama, A. Meniere’s disease: Histopathology, cytochemistry, and imaging. Ann. N. Y. Acad. Sci. 2015, 1343, 49–57. [Google Scholar] [CrossRef]
- Mahajan, A.; Marsili, L.; Dwivedi, A.K.; Situ-Kcomt, M.; Grimberg, M.B.; Wachter, N.; Abdelghany, E.; Duque, K.R.; Espay, A.J. Timing matters: Otological symptoms and Parkinson’s disease. Park. Relat. Disord. 2021, 90, 23–26. [Google Scholar] [CrossRef]
- Ohmen, J.D.; White, C.H.; Li, X.; Wang, J.; Fisher, L.M.; Zhang, H.; Derebery, M.J.; Friedman, R.A. Genetic Evidence for an Ethnic Diversity in the Susceptibility to Ménière’s Disease. Otol. Neurotol. 2013, 34, 1336–1341. [Google Scholar] [CrossRef]
- Frejo, L.; Martin-Sanz, E.; Teggi, R.; Trinidad, G.; Soto-Varela, A.; Santos-Perez, S.; Manrique, R.; Perez, N.; Aran, I.; Almeida-Branco, M.; et al. Extended phenotype and clinical subgroups in unilateral Meniere disease: A cross-sectional study with cluster analysis. Clin. Otolaryngol. 2017, 42, 1172–1180. [Google Scholar] [CrossRef]
- Belinchon, A.; Perez-Garrigues, H.; Tenias, J.M. Evolution of Symptoms in Ménière’s Disease. Audiol. Neurotol. 2011, 17, 126–132. [Google Scholar] [CrossRef]
- Oberman, B.; Patel, V.; Cureoglu, S.; Isildak, H. The aetiopathologies of Ménière’s disease: A contemporary review. Acta Otorhinolaryngol. Ital. 2017, 37, 250–263. [Google Scholar] [CrossRef]
- Frykholm, C.; Larsen, H.-C.; Dahl, N.; Klar, J.; Rask-Andersen, H.; Friberg, U. Familial Ménière’s Disease in Five Generations. Otol. Neurotol. 2006, 27, 681–686. [Google Scholar] [CrossRef]
- Wright, T. Menière’s disease. BMJ Clin. Evid. 2015, 2015, 0505. [Google Scholar] [PubMed]
- Mendis, S.; Longley, N.; Morley, S.; Korres, G.; Kaski, D. Autoimmune Vestibulopathy—A Case Series. Brain Sci. 2022, 12, 306. [Google Scholar] [CrossRef]
- Bruderer, S.G.; Bodmer, D.; Stohler, N.A.; Jick, S.S.; Meier, C.R. Population-Based Study on the Epidemiology of Ménière’s Disease. Audiol. Neurotol. 2017, 22, 74–82. [Google Scholar] [CrossRef]
- Da Costa, S.S.; de Sousa, L.C.A.; Piza, M.R.D.T. Meniere’s disease: Overview, epidemiology, and natural history. Otolaryngol. Clin. N. Am. 2002, 35, 455–495. [Google Scholar] [CrossRef]
- Kim, M.H.; Cheon, C. Epidemiology and Seasonal Variation of Ménière’s Disease: Data from a Population-Based Study. Audiol. Neurotol. 2020, 25, 224–230. [Google Scholar] [CrossRef]
- Vassar, M.; Matthew, H. The retrospective chart review: Important methodological considerations. J. Educ. Eval. Health Prof. 2013, 10, 12. [Google Scholar] [CrossRef]
- Requena, T.; Espinosa-Sanchez, J.M.; Cabrera, S.; Trinidad-Ruiz, G.; Soto-Varela, A.; Santos-Perez, S.; Teggi, R.; Perez, P.; Caletrio, A.B.; Fraile, J.; et al. Familial clustering and genetic heterogeneity in Meniere’s disease. Clin. Genet. 2013, 85, 245–252. [Google Scholar] [CrossRef]
- Morrison, A.W.; Bailey, M.E.S.; Morrison, G.A.J. Familial Ménière’s disease: Clinical and genetic aspects. J. Laryngol. Otol. 2008, 123, 29–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.Y.; Kim, H.; Oh, K.-W.; Oh, S.-I.; Koh, S.-H.; Baik, W.; Noh, M.Y.; Kim, K.S.; Kim, S.H. Biological Markers of Mesenchymal Stromal Cells as Predictors of Response to Autologous Stem Cell Transplantation in Patients With Amyotrophic Lateral Sclerosis: An Investigator-Initiated Trial and In Vivo Study. Stem Cells 2014, 32, 2724–2731. [Google Scholar] [CrossRef]
- Kim, M.H. Population-based study for the comorbidities and associated factors in Ménière’s disease. Sci. Rep. 2022, 12, 1–8. [Google Scholar] [CrossRef]
- Teggi, R.; Battista, R.A.; Di Berardino, F.; Familiari, M.; Cangiano, I.; Gatti, O.; Bussi, M. Evaluation of a large cohort of adult patients with Ménière’s disease: Bedside and clinical history. Acta Otorhinolaryngol. Ital. 2020, 40, 444–449. [Google Scholar] [CrossRef]
- Frejo, L.; Soto-Varela, A.; Santos-Perez, S.; Aran, I.; Batuecas-Caletrio, A.; Perez-Guillen, V.; Perez-Garrigues, H.; Fraile, J.; Martin-Sanz, E.; Tapia, M.C.; et al. Clinical Subgroups in Bilateral Meniere Disease. Front. Neurol. 2016, 7, 182. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.M.; Kim, M.J.; Jung, J.; Kim, H.J.; Seo, Y.J.; Kim, S.H. Genetic aspects and clinical characteristics of familial meniere’s disease in a South Korean population. Laryngoscope 2015, 125, 2175–2180. [Google Scholar] [CrossRef]
- House, J.W.; Doherty, J.K.; Fisher, L.M.; Derebery, M.J.; Berliner, K.I. Meniere’s Disease: Prevalence of Contralateral Ear Involvement. Otol. Neurotol. 2006, 27, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Requena, T.; Gazquez, I.; Moreno, A.; Batuecas, A.; Aran, I.; Soto-Varela, A.; Santos-Perez, S.; Perez, N.; Perez-Garrigues, H.; Lopez-Nevot, A.; et al. Allelic variants in TLR10 gene may influence bilateral affectation and clinical course of Meniere’s disease. Immunogenetics 2013, 65, 345–355. [Google Scholar] [CrossRef]
- Valente, M.; Mispagel, K.; Valente, M.L.; Hullar, T. Problems and Solutions for Fitting Amplification to Patients with Ménière’s Disease. J. Am. Acad. Audiol. 2006, 17, 006–015. [Google Scholar] [CrossRef] [Green Version]
- Villavisanis, D.F.; Mavrommatis, M.A.; Berson, E.R.; Bellaire, C.P.; Rutland, J.W.; Fan, C.J.; Wanna, G.B.; Cosetti, M.K. Cochlear Implantation in Meniere’s Disease: A Systematic Review and Meta-Analysis. Laryngoscope 2021, 131, 1845–1854. [Google Scholar] [CrossRef] [PubMed]
- Hwang, G.; Saadi, R.; Patel, V.A.; Liaw, J.; Isildak, H. Thyroid Dysfunction in Ménière’s Disease: A Comprehensive Review. Orl 2021, 83, 219–226. [Google Scholar] [CrossRef]
- Weinreich, H.M.; Agrawal, Y. The link between allergy and Menière′s disease. Curr. Opin. Otolaryngol. Head Neck Surg. 2014, 22, 227–230. [Google Scholar] [CrossRef]
- Marsili, L.; Rizzo, G.; Colosimo, C. Diagnostic Criteria for Parkinson’s Disease: From James Parkinson to the Concept of Prodromal Disease. Front. Neurol. 2018, 9, 156. [Google Scholar] [CrossRef] [PubMed]
- Marsili, L.; Mahajan, A. Clinical milestones in Parkinson’s disease: Past, present, and future. J. Neurol. Sci. 2021, 432, 120082. [Google Scholar] [CrossRef]
- Calzetti, S.; Negrotti, A. Permanent non-progressive cinnarizine and flunarizine-induced parkinsonism: An under-recognized tardive syndrome in the elderly? J. Neurol. Sci. 2022, 444, 120526. [Google Scholar] [CrossRef] [PubMed]
- Radtke, A.; Lempert, T.; Gresty, M.; Brookes, G.; Bronstein, A.; Neuhauser, H. Migraine and Meniere’s disease: Is there a link? Neurology 2002, 59, 1700–1704. [Google Scholar] [CrossRef]
- Murdin, L.; Schilder, A.G.M. Epidemiology of Balance Symptoms and Disorders in the Community. Otol. Neurotol. 2015, 36, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Van Esch, B.; van der Zaag-Loonen, H.; Bruintjes, T.; van Benthem, P.P. Betahistine in Ménière’s Disease or Syndrome: A Systematic Review. Audiol. Neurotol. 2021, 27, 1–33. [Google Scholar] [CrossRef] [PubMed]
- Nevoux, J.; Barbara, M.; Dornhoffer, J.; Gibson, W.; Kitahara, T.; Darrouzet, V. International consensus (ICON) on treatment of Ménière’s disease. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2018, 135, S29–S32. [Google Scholar] [CrossRef]
- Marsili, L.; Bologna, M.; Jankovic, J.; Colosimo, C. Long-term efficacy and safety of botulinum toxin treatment for cervical dystonia: A critical reappraisal. Expert Opin. Drug Saf. 2021, 20, 695–705. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mammarella, F.; Loperfido, A.; Keeling, E.G.; Bellocchi, G.; Marsili, L. Ménière’s Disease: Insights from an Italian Nationwide Survey. Audiol. Res. 2023, 13, 160-168. https://doi.org/10.3390/audiolres13020016
Mammarella F, Loperfido A, Keeling EG, Bellocchi G, Marsili L. Ménière’s Disease: Insights from an Italian Nationwide Survey. Audiology Research. 2023; 13(2):160-168. https://doi.org/10.3390/audiolres13020016
Chicago/Turabian StyleMammarella, Fulvio, Antonella Loperfido, Elizabeth G. Keeling, Gianluca Bellocchi, and Luca Marsili. 2023. "Ménière’s Disease: Insights from an Italian Nationwide Survey" Audiology Research 13, no. 2: 160-168. https://doi.org/10.3390/audiolres13020016
APA StyleMammarella, F., Loperfido, A., Keeling, E. G., Bellocchi, G., & Marsili, L. (2023). Ménière’s Disease: Insights from an Italian Nationwide Survey. Audiology Research, 13(2), 160-168. https://doi.org/10.3390/audiolres13020016