Updates in Hypertension Studies According to the Main Clinical Trials: A Review of the Past 45 Years about Pharmaceutical Intervention Effects


Abstract
:1. Introduction
2. Experimental Section
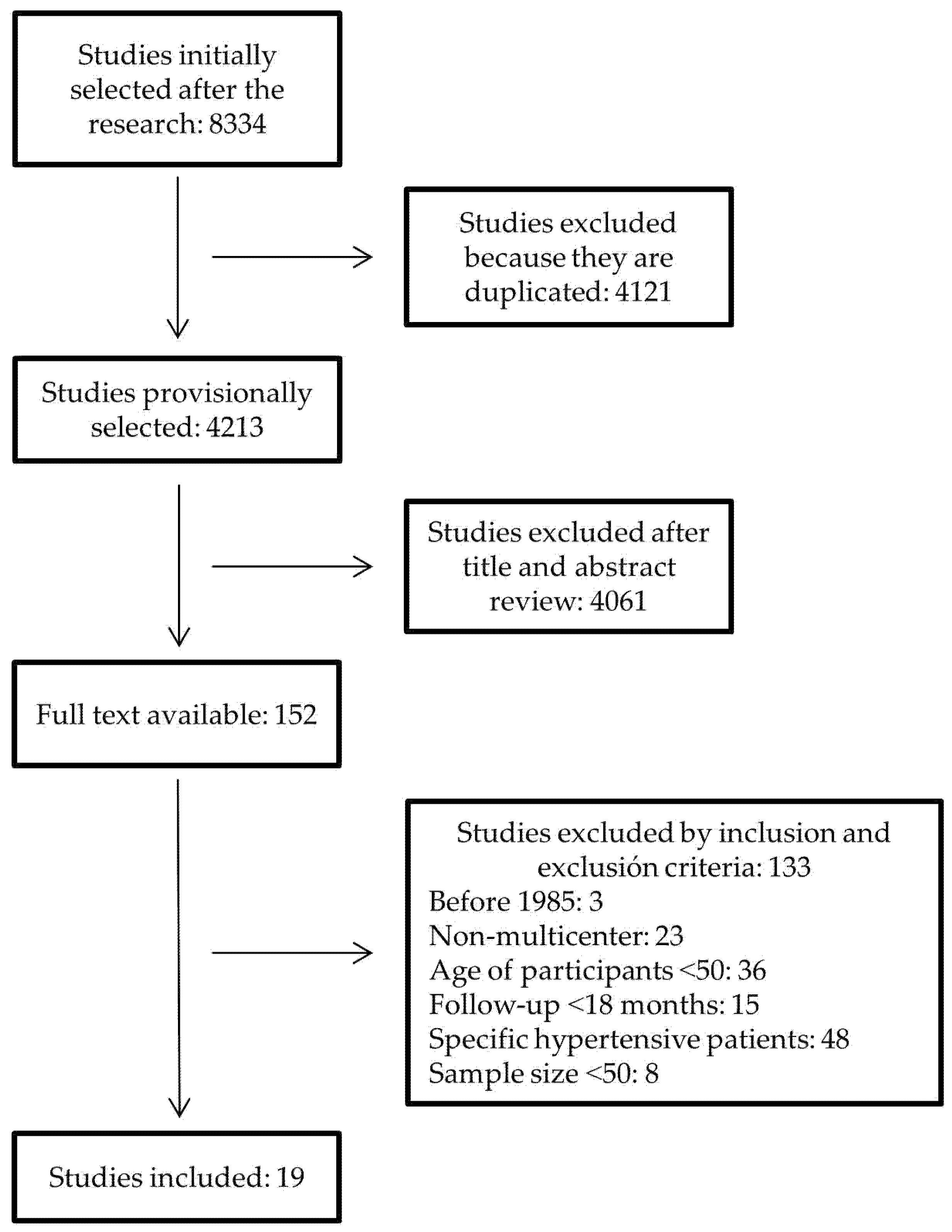
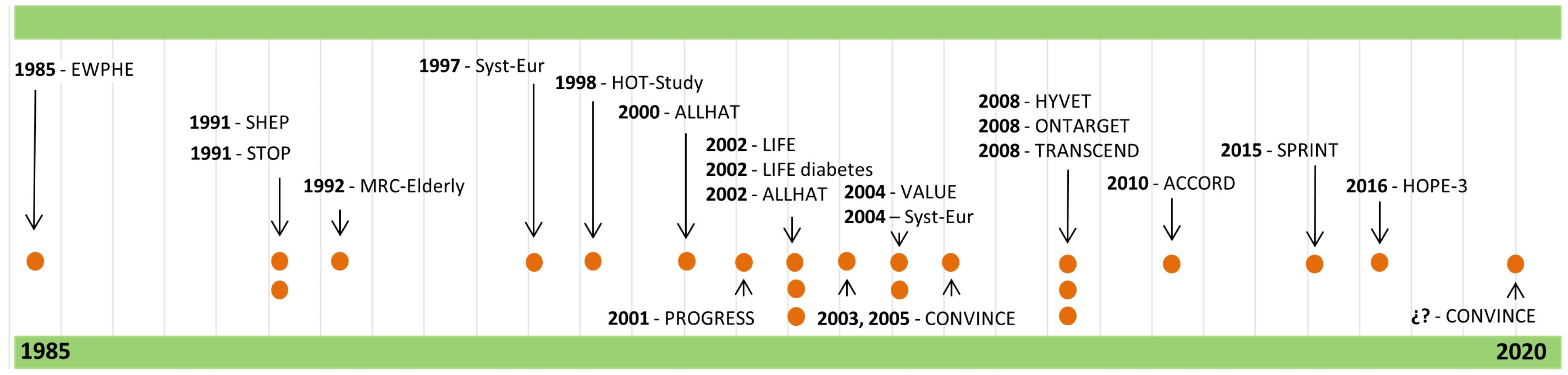
3. Results
4. Discussion
5. Conclusions
Funding
Conflicts of Interest
References
- Danaei, G.; Ding, E.L.; Mozaffarian, D.; Taylor, B.; Rehm, J.; Murray, C.J.L.; Ezzati, M. The Preventable Causes of Death in the United States: Comparative Risk Assessment of Dietary, Lifestyle, and Metabolic Risk Factors. PLoS Med. 2009, 6, e1000058. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; A AlMazroa, M.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [Green Version]
- Forouzanfar, M.H.; Liu, P.; Roth, G.A.; Ng, M.; Biryukov, S.; Marczak, L.; Alexander, L.; Estep, K.; Abate, K.H.; Akinyemiju, T.F.; et al. Global Burden of Hypertension and Systolic Blood Pressure of at Least 110 to 115 mm Hg, 1990–2015. JAMA 2017, 317, 165–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [PubMed]
- Blood Pressure Lowering Treatment Trialists’ Collaboration. Effects of different blood-pressure-lowering regimens on major cardiovascular events: Results of prospectively-designed overviews of randomised trials. Lancet 2003, 362, 1527–1535. [Google Scholar] [CrossRef]
- Gil-Extremera, B.; Jiménez-López, P.; Mediavilla-García, J.D. Clinical trials. A pending subject. Rev. Clin. Esp. 2018, 218, 137–141. [Google Scholar] [CrossRef]
- Rickham, P.P. Human experimentation. Code of ethics of the world medical association. Declaration of Helsinki. Br. Med. J. 1964, 2, 177. [Google Scholar]
- Amery, A.; Birkenhäger, W.; Brixko, P.; Bulpitt, C.; Clement, D.; Deruyttere, M.; De Schaepdryver, A.; Dollery, C.; Fagard, R.; Forette, F. Mortality and morbidity results from the European Working Party on High Blood Pressure in the Elderly trial. Lancet 1985, 1, 1349–1354. [Google Scholar] [CrossRef]
- MRC Working Party. Medical Research Council trial of treatment of hypertension in older adults: Principal results. BMJ 1992, 304, 405–412. [Google Scholar] [CrossRef] [Green Version]
- SHEP Cooperative Research Group. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension: Final results of the Systolic Hypertension in the Elderly Program (SHEP). JAMA 1991, 265, 3255–3264. [Google Scholar] [CrossRef]
- Dahlöf, B.; Lindholm, L.H.; Hansson, L.; Scherstén, B.; Ekbom, T.; Wester, P.O. Morbidity and mortality in the Swedish Trial in Old Patients with Hypertension (STOPHypertension). Lancet 1991, 338, 1281–1285. [Google Scholar] [CrossRef]
- Staessen, J.A.; Fagard, R.; Thijs, L.; Celis, H.; Arabidze, G.G.; Birkenhäger, W.H.; Bulpitt, C.J.; De Leeuw, P.W.; Dollery, C.T.; E Fletcher, A.; et al. Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. Lancet 1997, 350, 757–764. [Google Scholar] [CrossRef]
- Hansson, L.; Zanchetti, A.; Carruthers, S.G.; Dahlöf, B.; Elmfeldt, D.; Julius, S.; Menard, J.; Rahn, K.H.; Wedel, H.; Westerling, S. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: Principal results of the Hypertension Optimal Treatment (HOT) randomised trial. Lancet 1998, 351, 1755–1762. [Google Scholar] [CrossRef]
- The ALLHAT Collaborative Research Group. Major cardiovascular events in hypertensive patients randomized to doxazosin vs chlorthalidone: The antihypertensive and lipid-lowering treatment to prevent heart attack trial (ALLHAT). JAMA 2000, 283, 1967–1975. [Google Scholar] [CrossRef] [Green Version]
- PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6105 individuals with previous stroke or transient ischaemic attack. Lancet 2001, 358, 1033–1041. [Google Scholar] [CrossRef]
- Dahlöf, B.; Devereux, R.B.; Kjeldsen, S.E.; Julius, S.; Beevers, G.; Faire, U. Cardiovascular morbidity and mortality in the Losartan Intervention for Endpoint reduction in hypertension study (LIFE): A randomised trial against atenolol. Lancet 2002, 359, 995–1003. [Google Scholar] [CrossRef]
- The ALLHAT Officers and Coordinators for the ALLHAT Collaborative Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA 2002, 288, 2981–2997. [Google Scholar] [CrossRef]
- Black, H.R.; Elliott, W.J.; Grandits, G.; Grambsch, P.; Lucente, T.; White, W.B.; Neaton, J.D.; Grimm, R.H., Jr.; Hansson, L.; Lacourcière, Y.; et al. Principal Results of the Controlled Onset Verapamil Investigation of Cardiovascular End Points (CONVINCE) Trial. JAMA 2003, 289, 2073–2082. [Google Scholar] [CrossRef]
- Julius, S.; Kjeldsen, S.E.; Weber, M.; Brunner, H.R.; Ekman, S.; Hansson, L.; Hua, T.; Laragh, J.; Mclnnes, G.T.; Mitchell, L.; et al. Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: The VALUE randomised trial. Lancet 2004, 363, 2022–2031. [Google Scholar] [CrossRef]
- Staessen, J.A.; Thijs, L.; Fagard, R.; Celis, H.; Birkenhager, W.H.; Bulpitt, C.J. Effects of immediate versus delayed antihypertensive therapy on outcome in the Systolic Hypertension in Europe Trial. J. Hypertens. 2004, 22, 847–857. [Google Scholar] [CrossRef]
- Beckett, N.; Peters, R.; Fletcher, A.E.; Staessen, J.A.; Liu, L.; Dumitrascu, D.; Stoyanovsky, V.; Antikainen, R.L.; Nikitin, Y.; Anderson, C.S.; et al. Treatment of Hypertension in Patients 80 Years of Age or Older. N. Eng. J. Med. 2008, 358, 1887–1898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The ONTARGET Investigators. Telmisartan, Ramipril, or Both in Patients at High Risk for Vascular Events. N. Eng. J. Med. 2008, 358, 1547–1559. [Google Scholar] [CrossRef] [PubMed]
- The Telmisartan Randomised AssessmeNt Study in ACE iNtolerant subjects with cardiovascular Disease (TRANSCEND) Investigators. Effects of the angiotensin-receptor blocker telmisartan on cardiovascular events in high-risk patients intolerant to angiotensin-converting enzyme inhibitors: A randomised controlled trial. Lancet 2008, 372, 1174–1183. [Google Scholar] [CrossRef]
- The SPRINT Research Group. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N. Eng. J. Med. 2015, 373, 2103–2116. [Google Scholar] [CrossRef] [PubMed]
- Lonn, E.; Bosch, J.; Lopez-Jaramillo, P.; Zhu, J.; Liu, L.; Pais, P.; Diaz, R.; Xavier, D.; Sliwa, K.; Dans, A.; et al. Blood-Pressure Lowering in Intermediate-Risk Persons without Cardiovascular Disease. N. Eng. J. Med. 2016, 374, 2009–2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- U.S. National Library of Medicine. Clinical Trials.gov. COlchicine for PreventioN of Vascular Inflammation in Non-CardioEmbolic Stroke (CONVINCE). Available online: https://clinicaltrials.gov/ct2/show/NCT02898610 (accessed on 19 March 2020).
- Veterans Administration Cooperative Study Group on Antihypertensive Agents. Effects of treatment on mortality in hypertension III. Influence of age, diastolic blood pressure, and prior cardiovascular disease; further analysis of side effects. Circulation 1972, 45, 991–1004. [Google Scholar] [CrossRef] [Green Version]
- Khan, N.A.; Rabkin, S.W.; Zhao, Y.; McAlister, F.A.; Park, J.E.; Guan, M.; Chan, S.; Humphries, K.H. Effect of lowering diastolic pressure in patients with and without cardiovascular disease. Analysis of the SPRINT (Systolic Blood Pressure Intervention Trial). Hypertension 2018, 71, 840–847. [Google Scholar] [CrossRef]
- Sexto Grupo de Trabajo Conjunto de la Sociedad Europea de Cardiología y otras Sociedades sobre Prevención de Enfermedad Cardiovascular en la Práctica Clínica. Guía ESC 2016 sobre prevención de la enfermedad cardiovascular en la práctica clínica. Rev. Esp. Cardiol. 2016, 69, e1–e87. [Google Scholar]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, N.E.; Collins, K.J.; Himmelfarb, C.R.D.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2017. [Google Scholar] [CrossRef]
- Gil-Extremera, B.; Cía-Gómez, P. Hypertension in the Elderly. Int. J. Hypertens. 2012, 2012, 859176. [Google Scholar] [CrossRef]
- García, J.; Gil, B. Debemos tratar la hipertensión arterial en el muy anciano? Rev. Clin. Esp. 2008, 208, 481–482. [Google Scholar] [CrossRef] [PubMed]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R. Prospective studies collaboration. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913, Erratum in: Lancet 2003, 361, 1060. [Google Scholar]
- Van Bemmel, T.; Gussekloo, J.; Westendorp, R.G.J.; Blauw, G.J. In a population-based prospective study no association between high blood pressure and mortality after age 85 years. J. Hypertens. 2006, 24, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Gil, B. Tratamiento del paciente de 80 o más años con hipertensión arterial. Med. Clin. (Barc.) 2008, 131, 538–539. [Google Scholar]



{kind=link}
{kind=link}
| Clinical Trial (Publication Year) | Number of Participants, Their Age, and Country of Origin | Purposes | CRITERIA for Hypertension and Other Cardiovascular Risk Factors | Antihypertensive Treatment Used | Use of Placebo | Main Results | Conclusions |
|---|---|---|---|---|---|---|---|
| EWPHE [8], (1985) | 840, ≥60 years. European countries | Measure the effects of antihypertensive treatment in patients older than 60 years. | Systolic: 160–239 mmHg, Diastolic: 90–119 mmHg | Hydrochlorothiazide +Triamterene (+Methyldopa, if necessary) vs. placebo | Yes | Death, non-fatal subarachnoid haemorrhage, hypertensive retinopathy grade III or IV, dissecting aneurysm, congestive heart failure not controllable without diuretics or antihypertensive treatment, hypertensive encephalopathy, severe left ventricular hypertrophy, and a rise in blood pressure exceeding the defined limits. | 38% reduction in total cardiovascular mortality (p = 0.023) and 60% reduction in cardiovascular morbidity. |
| SHEP [9], (1991) | 4736, ≥60 years. United States | To establish whether an antihypertensive treatment reduces risk of fatal and non-fatal stroke in patients with isolated systolic hypertension. | Systolic: >160 mmHg, Diastolic: <90 mmHg | Chlorthalidone + Atenolol vs. placebo | Yes | Fatal stroke or not | 36% reduction in stroke risk (p < 0.01) and 32% reduction in all cardiovascular events (p < 0.05). |
| STOP [10], (1991) | 1627, 70–84 years. Sweden | To assess the ability of antihypertensive treatment to reduce the risk of non-fatal and fatal stroke, non-fatal and fatal acute myocardial infarction, and other deaths caused by cardiovascular events. | Systolic: 180–230 mmHg, Diastolic: 105–120 mmHg or ≥90 mmHg | Atenolol (+Hydrochlorothiazide and Amiloride, if necessary +Metropolol or Pindolol, if necessary) vs. placebo | Yes | Stroke, AMI, deaths from cardiovascular causes (sudden death, heart failure, and other fatal cardiovascular events) | 47% reduction in stroke risk (p < 0.01) and 43% reduction in mortality in general (p < 0.01). |
| MRC-Elderly [11], (1992) | 4961, 65–74 years. United Kingdom | To establish whether treatment with diuretic or beta blocker in hypertensive older adults reduces risk of stroke, coronary heart disease, and death. | Systolic: <200 mmHg, Diastolic: 90–109 mmHg | -Amiloride + Hydrochlorothiazide vs. placebo-Atenolol vs. placebo | Yes | Fatal and non-fatal stroke, sudden coronary death, fatal and non-fatal AMI, and death due to hypertension, to rupture or dissection of an aorticaneurysm, or to any other cardiovascular cause. | 25% reduction in stroke risk (p = 0.04) and 17% reduction in all cardiovascular events (p = 0.03). |
| Syst-Eur [12], (1997) | 4695, ≥60 years. 23 European countries | To assess whether the antihypertensive treatment reduces the rate of cardiovascular complications in isolated systolic hypertension. | Systolic: 160–219 mmHg, Diastolic: <95 mmHg | Nitrendipine and/or Enalapril and/or Hydrochlorothiazide vs. placebo | Yes | Death, stroke, retinal haemorrhage or exudates, AMI, congestive heart failure, dissecting aortic aneurysm, and renal insufficiency. | 42% reduction stroke risk (p = 0.03) and 31% reduction in all cardiovascular events (p < 0.001). |
| HOT-Study [13], (1998) | 18,790, 50–80 years. 26 countries of Europe, America and Asia | To establish the optimum target diastolic blood pressure and the potential benefit of a low dose of acetylsalicylic in the treatment of hypertension. | Diastolic: 100–115 mmHg | Felodipine (+ACE inhibitor +Beta-Blockers, if necessary) + Acetylsalicylic Acid vs. placebo | Yes | Fatal or non-fatal AMI, fatal or non-fatal stroke, and other deaths due to cardiovascular causes. | 15% reduction in risk of cardiovascular events (p = 0.03) and 36% reduction in AMI (p = 0.002). No effect on stroke. |
| ALLHAT [14], (2000) | 24,335, ≥55 years. United States and Canada | To compare the effect of doxazosin, a beta-blocker, with chlorthalidone, a diuretic, on incidence of cardiovascular diseases in patients with hypertension as part of a study of four types of antihypertensive drugs: chlorthalidone, doxazosin, amlodipine, and lisinopril. | Systolic: ≥140 mmHg, or Diastolic: ≥90 mmHg and one or more cardiovascular risk factors | Chlorthalidone vs. Doxazosin | No | Fatal coronary disease or non-fatal AMI | 25% reduction in risk of other cardiovascular diseases (p < 0.001) in chlorthalidone group. |
| PROGESS [15], (2001) | 6105, with no age limits Australia, Belgium, China, France, Italy, Ireland, Japan, New Zealand, Sweden, and the United Kingdom | To determine the effects of a flexible antihypertensive treatment based on perindopril and indapamide on stroke and other cardiovascular events in patients with a history of stroke or transient ischaemic attack. | Stroke or transient ischaemic attack. | Perindopril +Indapamide vs. placebo | Yes | Fatal stroke or not | 28% reduction in stroke risk (p < 0.001) and 26% reduction in all cardiovascular events. |
| LIFE [16], (2002) | 9193, 55–80 years. Scandinavia, the United Kingdom, and the United States | To establish whether an angiotensin II receptor blocker improves left ventricular hypertrophy beyond reducing blood pressure and, consequently, reduces cardiovascular morbidity and death. | Systolic: >160 mmHg, Diastolic: <90 mmHg and left ventricular hypertrophy | Losartan + Hydrochlorothiazide + another antihypertensive (if necessary) vs. Atenolol + Hydrochlorothiazide + another antihypertensive (if necessary) | No | Death due to cardiovascular causes, AMI, stroke | 13% reduction in risk of cardiovascular death, stroke and AMI (p = 0.021) in losartan group. |
| ALLHAT [17], (2002) | 33357, ≥55 years. The United States, Puerto Rico, Virgin Islands, and Canada | To determine whether treatment with a calcium channel blocker or an ACE inhibitor lowers the incidence of coronary heart disease or other cardiovascular disease events vs. treatment with a diuretic. | Systolic: ≥140 mmHg, or Diastolic: ≥90 mmHg and one or more cardiovascular risk factors | -Lisinopril vs. Chlorthalidone -Amlodipine vs. Chlorthalidone | No | Death due to coronary disease, non-fatal AMI. | No statistically significant differences in both groups. |
| CONVINCE [18], (2003) | 16,602, ≥55 years. The United States, Canada, Europe, Mexico, Brazil, and Israel | To establish the equivalence between an extended treatment with controlled onset verapamil and a standard treatment for preventing cardiovascular disease events. | Systolic: 140–190 mmHg, Diastolic: 90–110 mmHg and one or more cardiovascular risk factors | -Verapamil vs. Atenolol -Verapamil vs. Hydrochlorothiazide | Yes | AMI, stroke, sudden death due to coronary cause or death due to cardiovascular disease. | No statistically significant differences in both groups |
| VALUE [19], (2004) | 15,245, ≥50 years. 31 countries of America, Australia, Asia, Europe, and South Africa | To assess the efficacy of valsartan in the reduction of cardiovascular morbidity and mortality vs. amlodipine in hypertensive patients at high cardiovascular risk. | Systolic: 160–210 mmHg, and Diastolic: <115 mmHg | Valsartan + Hydrochlorothiazide (+another antihypertensive, if necessary) vs. Amlodipine + Hydrochlorothiazide (+another antihypertensive, if necessary) | No | Sudden cardiac death, fatal or non-fatal AMI, death after percutaneous coronary intervention or artery bypass, death due to heart failure, and death due to heart failure requiring hospital management. | No statistically significant differences |
| Syst-Eur [20], (2004) | 4695, ≥60 years. 23 European countries | To assess the outcome of immediate versus delayed antihypertensive treatment in older patients with isolated systolic hypertension. | Systolic: 160–219 mmHg, Diastolic: <95 mmHg | Nitrendipine and/or Enalapril and/or Hydrochlorothiazide vs. placebo | Yes | Death, stroke, retinal haemorrhage or exudates, AMI, congestive heart failure, dissecting aortic aneurysm, and renal insufficiency. | 28% reduction in stroke risk (p = 0.01) and 15% reduction in the rest of cardiovascular events (p = 0.03). |
| HYVET [21], (2008) | 3845, ≥80 years. Europe, China, Australia, New Zealand, and Tunisia | To establish whether the antihypertensive treatment is beneficial in different fatal and non-fatal cardiovascular events in patients who are 80 years of age or older. | Systolic: ≥160 mmHg | Indapamide (+Perindopril, if necessary) vs. placebo | Yes | Fatal or non-fatal stroke | 21% reduction in risk of death due to any cause (p = 0.02) |
| ONTARGET [22], (2008) | 25,620, ≥55 years. 40 countries of America, Australia, Asia, Europe, and South Africa | To evaluate whether treatment based on telmisartan is superior to treatment with ramipril and whether a combination of the two drugs was superior to ramipril alone as a treatment to prevent vascular events in high-risk patients who had cardiovascular disease or diabetes mellitus but did not have heart failure. | Coronary disease, peripheral artery or cerebrovascular disease, or diabetes mellitus. | Telmisartan vs. Ramipril vs. Telmisartan+ Ramipril | No | Death from cardiovascular cause, AMI, stroke, and hospitalization for heart failure. | No statistically significant differences |
| TRANSCEND * [23], (2008) | 5926, ≥55 years. 40 countries of America, Australia, Asia, Europe, and South Africa | To study whether extended telmisartan treatment reduces the rate of cardiovascular disease, AMI, stroke, or hospitalization for heart failure in patients with cardiovascular disease or at high risk of diabetes but did not have heart failure who are intolerant to ramipril, compared with placebo, in addition to other common therapies. | Coronary, peripheral artery or cerebrovascular disease, or diabetes mellitus. | Telmisartan vs. placebo | Yes | Death from cardiovascular cause, AMI, stroke, and hospitalization for heart failure. | No statistically significant differences |
| SPRINT [24], (2015) | 9361, ≥50 years. The United States | To compare the benefit of treatment of systolic blood pressure to a target of less than 140 mmHg with treatment to a target of less than 120 mmHg. | Systolic: 130–180 mmHg and other cardiovascular risk factors | Intensive antihypertensive treatment based on diuretics and/or ACE inhibitors or ARBs (not both) and/or calcium antagonist vs. common standard treatment (+diuretic, if necessary). | No | AMI, acute coronary syndrome, stroke, decompensated heart failure, death from cardiovascular causes or any cause. | 25% reduction in risk of AMI, acute coronary syndrome, stroke, heart failure, and death from cardiovascular causes (p < 0.001) and 27% reduction in death from any cause (p = 0.03) in intensive treatment group. |
| HOPE-3 [25], (2016) | 12,705, men aged ≥55 years and women aged ≥65 years. America, Asia, Oceania, Europe, and South Africa | To establish whether antihypertensive treatment reduces the risk of cardiovascular disease in patients with a systolic blood pressure of <160 mmHg and an intermediate risk (≈1%) of significant cardiovascular disease. | No cardiovascular disease known but at least one cardiovascular risk factor. | Candesartan + Hydrochlorothiazide vs. placebo | Yes | Death from cardiovascular cause, non-fatal AMI, non-fatal stroke, cardiopulmonary resuscitation, heart failure, and coronary revascularization. | No statistically significant differences |
| CONVINCE [26] | 2623 (non definitive) >40 years. European countries | To compare the efficacy of low dose colchicine plus common treatment with common treatment alone to prevent non-fatal recurrent ischaemic stroke and coronary events and death from vascular cause after transient ischaemic attack or cerebrovacular disease. | Cerebrovascular ischaemic disease without major disability or at high risk of transient ischaemic attack. | Colchicine vs. other treatment (antiplatelets, lipid-lowering agents, antihypertensives, and appropriate lifestyle). | No | Non-fatal ischaemic stroke, hospitalization for unstable angina not resulting in death, AMI, cardiac arrest, and death from cardiovascular cause. | Actually recruiting patients. |
© 2020 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Linares, J.M. Updates in Hypertension Studies According to the Main Clinical Trials: A Review of the Past 45 Years about Pharmaceutical Intervention Effects. Nurs. Rep. 2020, 10, 2-14. https://doi.org/10.3390/nursrep10010002
Martínez-Linares JM. Updates in Hypertension Studies According to the Main Clinical Trials: A Review of the Past 45 Years about Pharmaceutical Intervention Effects. Nursing Reports. 2020; 10(1):2-14. https://doi.org/10.3390/nursrep10010002
Chicago/Turabian StyleMartínez-Linares, Jose Manuel. 2020. "Updates in Hypertension Studies According to the Main Clinical Trials: A Review of the Past 45 Years about Pharmaceutical Intervention Effects" Nursing Reports 10, no. 1: 2-14. https://doi.org/10.3390/nursrep10010002
APA StyleMartínez-Linares, J. M. (2020). Updates in Hypertension Studies According to the Main Clinical Trials: A Review of the Past 45 Years about Pharmaceutical Intervention Effects. Nursing Reports, 10(1), 2-14. https://doi.org/10.3390/nursrep10010002