
Malnutrition and Inadequate Eating Behaviour during Hospital Stay in Geriatrics—An Explorative Analyses of NutritionDay Data in Two Hospitals


Abstract
:1. Introduction
- Nutritional status of the included patients, prevalence of malnutrition risk, and malnutrition,
- indicators of inadequate eating behaviour during hospital stay, prevalence and associated factors of inadequate eating behaviour,
- nutritional support offered to the patients by staff and the question of who gets this support will be the focus in this explorative analysis.
2. Materials and Methods
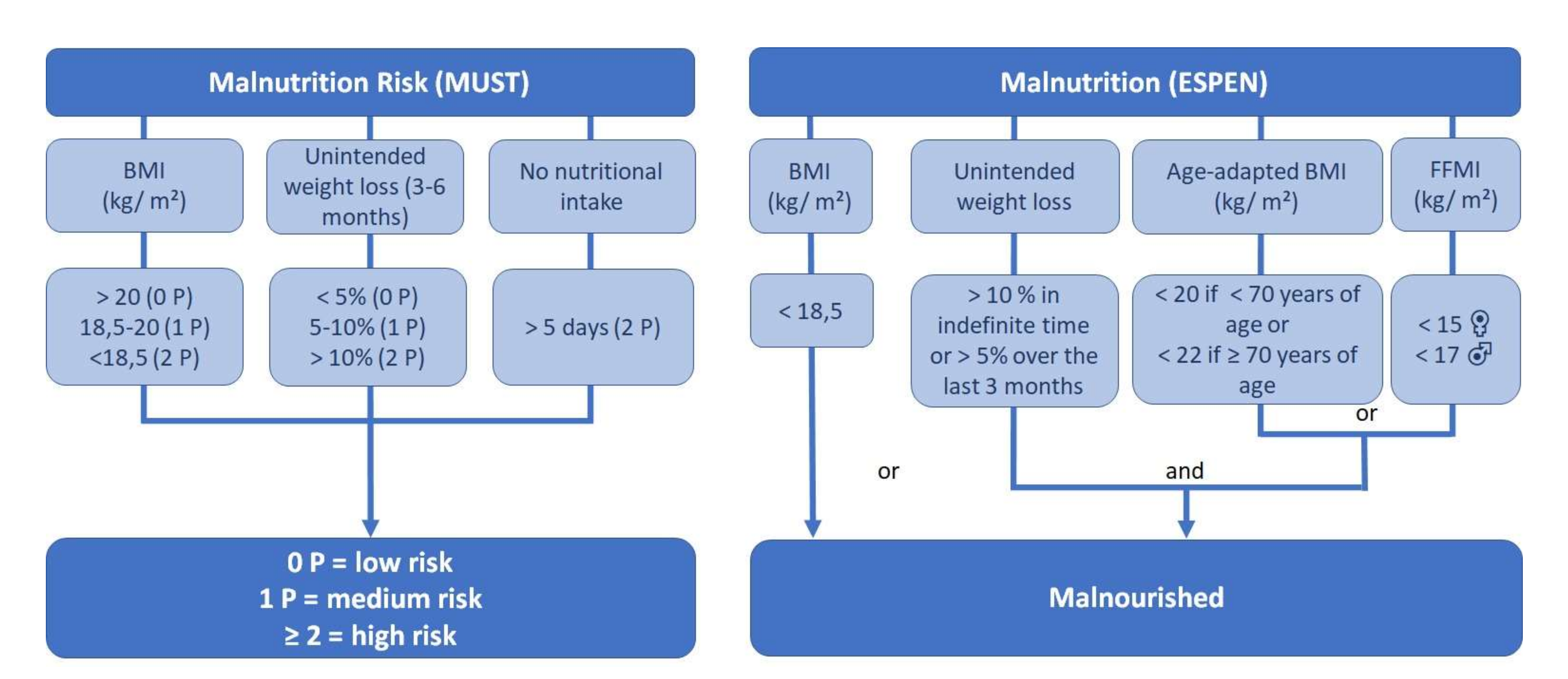
2.1. Nutritional Status
2.2. Inadequate Eating Behaviour
- Eating less than before admission (the week before hospitalization)
- Eating the same as before admission if the intake had already been reduced
- Not eating the whole meal on nutritionDay and the reason is not “I normally eat less than served”
- Not eating on nutritionDay and the reason is not “I had an exam, surgery or test or I was not allowed to eat”
2.3. Data Analysis and Informed Consent
3. Results
3.1. Health and Nutrition Status
3.2. Nutritional Status
3.3. Associations with Inadequate Eating Behaviour
4. Discussion
4.1. The Undetected Malnutrition and Inadequate Feeding Behaviour
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Henriksen, C.; Gjelstad, I.M.; Nilssen, H.; Blomhoff, R. A low proportion of malnourished patients receive nutrition treatment—Results from nutritionDay. Food Nutr. Res. 2017, 61, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Aotani, N.; Yasui-Yamada, S.; Kagiya, N.; Takimoto, M.; Oiwa, Y.; Matsubara, A.; Matsuura, S.; Tanimura, M.; Tani-Suzuki, Y.; Kashihara, H.; et al. Malnutrition by European Society for Clinical Nutrition and Metabolism criteria predicts prognosis in patients with gastrointestinal and hepatobiliary-pancreatic cancer. Clin. Nutr. ESPEN 2021, 42, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Ihle, C.; Freude, T.; Bahrs, C.; Zehendner, E.; Braunsberger, J.; Biesalski, H.K.; Lambert, C.; Stöckle, U.; Wintermeyer, E.; Grünwald, J.; et al. Malnutrition—An underestimated factor in the inpatient treatment of traumatology and orthopedic patients: A prospective evaluation of 1055 patients. Injury 2017, 48, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Alvarez Hernandez, J.; Leon Sanz, M.; Planas Vila, M.; Araujo, K.; Garcia de Lorenzo, A.; Celaya Perez, S. Prevalence and costs of malnutrition in hospitalized dysphagic patients: A subanalysis of the PREDyCES® study. Nutr Hosp. 2015, 32, 1830–1836. [Google Scholar]
- Budzyński, J.; Tojek, K.; Czerniak, B.; Banaszkiewicz, Z. Scores of nutritional risk and parameters of nutritional status assessment as predictors of in-hospital mortality and readmissions in the general hospital population. Clin Nutr. 2016, 35, 1464–1471. [Google Scholar] [CrossRef] [PubMed]
- Pirlich, M.; Schutz, T.; Norman, K.; Gastell, S.; Lubke, H.J.; Bischoff, S.C.; Bolder, U.; Frieling, T.; Guldenzoph, H.; Hahn, K.; et al. The German hospital malnutrition study. Clin. Nutr. 2006, 25, 563–572. [Google Scholar] [CrossRef] [PubMed]
- Cereda, E.; Klersy, C.; Hiesmayr, M.; Schindler, K.; Singer, P.; Laviano, A.; Caccialanza, R. Body mass index, age and in-hospital mortality: The NutritionDay multinational survey. Clin. Nutr. 2017, 36, 839–847. [Google Scholar] [CrossRef]
- Sanson, G.; Bertocchi, L.; Dal Bo, E.; Di Pasquale, C.L.; Zanetti, M. Identifying reliable predictors of protein-energy malnutrition in hospitalized frail older adults: A prospective longitudinal study. Int. J. Nurs. Stud. 2018, 82, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Abugroun, A.; Nayyar, A.; Abdel-Rahman, M.; Patel, P. Impact of Malnutrition on Hospitalization Outcomes for Older Adults Admitted for Sepsis. Am. J. Med. 2021, 134, 221–226. [Google Scholar] [CrossRef]
- Mendes, A.; Serratrice, C.; Herrmann, F.R.; Gold, G.; Graf, C.E.; Zekry, D.; Genton, L. Nutritional risk at hospital admission is associated with prolonged length of hospital stay in old patients with COVID-19. Clin. Nutr. 2021, 40. [Google Scholar] [CrossRef]
- Thomas, S.; Alexander, C.; Cassady, B.A. Nutrition risk prevalence and nutrition care recommendations for hospitalized and critically-ill patients with COVID-19. Clin. Nutr. ESPEN 2021, 44, 38–49. [Google Scholar] [CrossRef]
- Osuna-Padilla, I.A.; Rodríguez-Moguel, N.C.; Aguilar-Vargas, A.; Rodríguez-Llamazares, S. Asociación entre el riesgo nutricional evaluado a través de NUTRIC-Score y los desenlaces clínicos en pacientes en estado crítico con COVID-19. Nutr. Hosp. 2021, 38, 540–544. [Google Scholar] [PubMed]
- Kruizenga, H.; van Keeken, S.; Weijs, P.; Bastiaanse, L.; Beijer, S.; Huisman-de Waal, G.; Jager-Wittenaar, H.; Jonkers-Schuitema, C.; Klos, M.; Remijnse-Meester, W.; et al. Undernutrition screening survey in 564,063 patients: Patients with a positive undernutrition screening score stay in hospital 1.4 d longer. Am. J. Clin. Nutr. 2016, 103, 1026–1032. [Google Scholar] [CrossRef] [Green Version]
- Hiesmayr, M.; Tarantino, S.; Moick, S.; Laviano, A.; Sulz, I.; Mouhieddine, M.; Schuh, C.; Volkert, D.; Simon, J.; Schindler, K. Hospital Malnutrition, a Call for Political Action: A Public Health and NutritionDay Perspective. J. Clin. Med. 2019, 8, 2048. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aubry, E.; Mareschal, J.; Gschweitl, M.; Zvingelis, M.; Schuetz, P.; Stanga, Z. Facts zum Management der Klinischen Ernährung—Eine Online-Befragung. Aktuel Ernahr. 2018, 42, 452–460. [Google Scholar] [CrossRef]
- Schönherr, S.; Halfens, R.J.G.; Meijers, J.M.M.; Schols, J.M.G.A.; Lohrmann, C. Structural and process indicators of nutritional care: A comparison between Austrian hospitals and nursing homes. Nutrition 2012, 28, 868–873. [Google Scholar] [CrossRef]
- Graeb, F.; Wientjens, R.; Wolke, R. Der Ernährungsstatus von PatientInnen in der Akutversorgung und das Problem der nicht identifizierten Mangelernährung. Aktuel Ernahr. 2019, 44, 23–32. [Google Scholar] [CrossRef]
- Hébuterne, X.; Lemarié, E.; Michallet, M.; de Montreuil, C.B.; Schneider, S.M.; Goldwasser, F. Prevalence of malnutrition and current use of nutrition support in patients with cancer. J. Parenter. Enter. Nutr. 2014, 38, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Wientjens, R.; Graeb, F.; Elsbernd, A.; Wolke, R. Entwicklung, Umsetzung und Evaluation eines Konzeptes zu Prävention und Behandlung von Mangelernährung bei geriatrischen Patienten im Krankenhaus. Z. Gerontol. Geriatr. 2018, 51, 103. [Google Scholar]
- Wientjens, R.; Graeb, F.; Wolke, R. Interdisziplinäre Konzeptentwicklung in der Praxis am Beispiel von Mangelernährung bei älteren Menschen im Krankenhaus. In Aktuelle Pflegewissenschaftliche Entwicklungen im Gesundheitswesen: Beiträge des Wissenschaftlichen Nachwuchses der Hochschulen Hannover, Esslingen und Bielefeld; Bonse-Rohmann, M., Raschper, P., Wolke, R., Eds.; Jacobs: Lage, Germany, 2019; pp. 271–285. [Google Scholar]
- Schindler, K.; Pichard, C.; Sulz, I.; Volkert, D.; Streicher, M.; Singer, P.; Ljungqvist, O.; van Gossum, A.; Bauer, P.; Hiesmayr, M. Nutritionday: 10 years of growth. Clin. Nutr. 2017, 36, 1207–1214. [Google Scholar] [CrossRef] [PubMed]
- Schindler, K.; Themessl-Huber, M.; Hiesmayr, M.; Kosak, S.; Lainscak, M.; Laviano, A.; Ljungqvist, O.; Mouhieddine, M.; Schneider, S.; de van der Schueren, M.; et al. To eat or not to eat? Indicators for reduced food intake in 91,245 patients hospitalized on nutrition Days 2006–2014 in 56 countries worldwide: A descriptive analysis. Am. J. Clin. Nutr. 2016, 104, 1393–1402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondrup, J.; Allison, S.P.; Elia, M.; Vellas, B.; Plauth, M. ESPEN Guidelines for Nutrition Screening 2002. Clin. Nutr. 2003, 22, 415–421. [Google Scholar] [CrossRef]
- Poulia, K.-A.; Klek, S.; Doundoulakis, I.; Bouras, E.; Karayiannis, D.; Baschali, A.; Passakiotou, M.; Chourdakis, M. The two most popular malnutrition screening tools in the light of the new ESPEN consensus definition of the diagnostic criteria for malnutrition. Clin. Nutr. 2017, 36, 1130–1135. [Google Scholar] [CrossRef] [PubMed]
- Cederholm, T.; Bosaeus, I.; Barazzoni, R.; Bauer, J.; van Gossum, A.; Klek, S.; Muscaritoli, M.; Nyulasi, I.; Ockenga, J.; Schneider, S.M.; et al. Diagnostic criteria for malnutrition—An ESPEN Consensus Statement. Clin. Nutr. 2015, 34, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Hickson, M.; Frost, G. A comparison of three methods for estimating height in the acutely ill elderly population. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2003, 16, 13–20. [Google Scholar] [CrossRef]
- Powell-Tuck, J. A comparison of mid upper arm circumference, body mass index and weight loss as indices of undernutrition in acutely hospitalized patients. Clin. Nutr. 2003, 22, 307–312. [Google Scholar] [CrossRef]
- Volkert, D.; Weber, J.; Kiesswetter, E.; Sulz, I.; Hiesmayr, M. Nutritional situation in German hospitals—Results of the nutrition Day project 2018. Ernähr. Umsch. 2019, 66, 204–211. [Google Scholar]
- Eglseer, D.; Schoberer, D.; Halfens, R.; Lohrmann, C. The impact of using a malnutrition screening tool in a hospital setting: A mixed methods study. Eur. J. Clin. Nutr. 2019, 73, 284–292. [Google Scholar] [CrossRef]
- Graeb, F.; Wientjens, R.; Wolke, R.; Essig, G. Veränderungen des Ernährungsstatus geriatrischer PatientInnen während der stationären Krankenhausbehandlung. Akt. Ernähr. Med. 2020, 45, 16–24. [Google Scholar] [CrossRef]
- IQM Initiative Qualitätsmedizin. Available online: https://www.initiative-qualitaetsmedizin.de/ (accessed on 10 June 2020).
- Blumenschein, B.; Kalde, S.; Heick, V. Wegweiser für das Kodieren krankheitsbedingter Mangelernährung. Aktuel Ernahr. 2017, 42, 36–50. [Google Scholar] [CrossRef]
- Graeb, F.; Reiber, P.; Wolke, R. Malnutrition risk in obese geriatric patients? A routine data based analysis for patients living in nursing homes. Ernähr. Umsch. 2021, 68, 95–101. [Google Scholar]
- Barazzoni, R.; Sulz, I.; Schindler, K.; Bischoff, S.C.; Gortan Cappellari, G.; Hiesmayr, M. A negative impact of recent weight loss on in-hospital mortality is not modified by overweight and obesity. Clin. Nutr. 2020, 39, 2510–2516. [Google Scholar] [CrossRef]
- Collins, K.H.; Herzog, W.; MacDonald, G.Z.; Reimer, R.A.; Rios, J.L.; Smith, I.C.; Zernicke, R.F.; Hart, D.A. Obesity, Metabolic Syndrome, and Musculoskeletal Disease: Common Inflammatory Pathways Suggest a Central Role for Loss of Muscle Integrity. Front. Physiol. 2018, 9, 112. [Google Scholar] [CrossRef] [PubMed]
- Deutz, N.E.P.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the ESPEN Expert Group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [Green Version]
- Deutz, N.E.P.; Ashurst, I.; Ballesteros, M.D.; Bear, D.E.; Cruz-Jentoft, A.J.; Genton, L.; Landi, F.; Laviano, A.; Norman, K.; Prado, C.M. The Underappreciated Role of Low Muscle Mass in the Management of Malnutrition. J. Am. Med. Dir. Assoc. 2019, 20, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Volkert, D.; Beck, A.M.; Cederholm, T.; Cruz-Jentoft, A.; Goisser, S.; Hooper, L.; Kiesswetter, E.; Maggio, M.; Raynaud-Simon, A.; Sieber, C.C.; et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin. Nutr. 2019, 38, 10–47. [Google Scholar] [CrossRef] [Green Version]
- Felder, S.; Lechtenboehmer, C.; Bally, M.; Fehr, R.; Deiss, M.; Faessler, L.; Kutz, A.; Steiner, D.; Rast, A.C.; Laukemann, S.; et al. Association of nutritional risk and adverse medical outcomes across different medical inpatient populations. Nutrition 2015, 31, 1385–1393. [Google Scholar] [CrossRef] [PubMed]
- Merker, M.; Felder, M.; Gueissaz, L.; Bolliger, R.; Tribolet, P.; Kägi-Braun, N.; Gomes, F.; Hoess, C.; Pavlicek, V.; Bilz, S.; et al. Association of Baseline Inflammation With Effectiveness of Nutritional Support Among Patients With Disease-Related Malnutrition: A Secondary Analysis of a Randomized Clinical Trial. JAMA Netw. Open 2020, 3, e200663. [Google Scholar] [CrossRef]
- Jensen, G.L.; Cederholm, T.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; de Baptista, G.A.; Barazzoni, R.; Blaauw, R.; Coats, A.J.S.; et al. GLIM Criteria for the Diagnosis of Malnutrition: A Consensus Report From the Global Clinical Nutrition Community. J. Parenter. Enter. Nutr. 2019, 43, 32–40. [Google Scholar] [CrossRef] [Green Version]
- Schuetz, P.; Fehr, R.; Baechli, V.; Geiser, M.; Deiss, M.; Gomes, F.; Kutz, A.; Tribolet, P.; Bregenzer, T.; Braun, N.; et al. Individualised nutritional support in medical inpatients at nutritional risk: A randomised clinical trial. Lancet 2019, 393, 2312–2321. [Google Scholar] [CrossRef]
- Baumgartner, A.; Pachnis, D.; Parra, L.; Hersberger, L.; Bargetzi, A.; Bargetzi, L.; Kaegi-Braun, N.; Tribolet, P.; Gomes, F.; Hoess, C.; et al. The impact of nutritional support on malnourished inpatients with aging-related vulnerability. Nutrition 2021, 89, 111279. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Questionnaire | Asked Variables |
|---|---|
| 2 a/b About your patient (taken from the patient files) | year of birth, sex |
| weight/ height at admission | |
| diagnosis at admission (by ICD-10 maingroups), main reason for admission, comorbidities (e. a. cancer, dementia) | |
| surgery during hospital stay, admission to Intensive Care Unit (ICU), number of different medications, identified as malnourished or at risk of malnutrition | |
| nutrition intake/diet (e.g., regular food, special diets), nutritional interventions (e.g., recording nutrition intake, developing a nutrition treatment plan) | |
| 3 a/b Patient questionnaire (by interviewing the patients) | typical dietary habits (e.g., no special habits, vegetarian, gluten-free diet) |
| living before hospital admission, general ability to walk, subjective health state in general | |
| contact with doctor and hospital stays in the last 12 months, numbers of daily different medications (prior to hospital stay) | |
| weight five years ago, weight lost within the last three months (if yes, amount of kg), get any nutritional information or intervention | |
| eating in the week before admission, satisfaction with the hospital food | |
| Today: getting help with eating, eating interruption, ordered portion size, how much ate for lunch, reasons for eating less/nothing | |
| changed food intake since admission, todays subjective condition, walking ability today | |
| Outcome Evaluation (taken from the patient files) | 30 days after nutritionDay: discharge date, discharge diagnosis, outcome (e.g., still in hospital, rehabilitation, death) |
| Variable | n | Mdn | (IQR) | % | (n) | |
|---|---|---|---|---|---|---|
| Age | 156 | 79.0 | (13.0) | |||
| Sex | 156 | male | 41.7 | (65) | ||
| female | 55.8 | (87) | ||||
| Length of stay (days) | 156 | 12.0 | (11) | |||
| Admission diagnosis, ICD-10 groups | 156 | Respiratory system | 18.6 | (29) | ||
| Musculoskeletal system and connective tissue | 17.9 | (28) | ||||
| Nervous system | 15.4 | (24) | ||||
| Circulatory system | 10.3 | (16) | ||||
| Admission | 156 | Emergency | 68.6 | (107) | ||
| Comorbidities | 156 | Cardiac insufficiency | 24.4 | (38) | ||
| Diabetes | 22.4 | (35) | ||||
| Cancer | 22.4 | (35) | ||||
| Chronic kidney disease | 21.8 | (34) | ||||
| Peripheral vascular disease | 21.2 | (33) | ||||
| Chronic lung disease | 18.6 | (29) | ||||
| Dementia | 16.7 | (26) | ||||
| Unit Specialty | 156 | Internal Medicine/Geriatrics | 35.9 | (56) | ||
| Internal Medicine/General | 21.8 | (34) | ||||
| Surgery/Orthopedic | 16.0 | (25) | ||||
| Neurology | 20.5 | (32) | ||||
| Interdisciplinary (Surgery/Internal) | 5.8 | (9) | ||||
| ICU stay (≥1 day) | 156 | 13.5 | (21) | |||
| Surgery (any) | 156 | 14.8 | (23) | |||
| Outcome after 4 weeks | 156 | Still in the hospital/transferred to another hospital | 10.3 | (16) | ||
| Transferred to long term care | 20.5 | (32) | ||||
| Rehabilitation | 8.3 | (23) | ||||
| Discharged home | 59.6 | (93) | ||||
| Death | 1.3 | (2) |
| Variable | n | Mdn | (IQR) | % | (n) | |
|---|---|---|---|---|---|---|
| Living before admission | 156 | at home | 80.1 | (125) | ||
| in nursing home or other live-in facilities | 14.1 | (22) | ||||
| Other/no answers | 5.8 | (9) | ||||
| General ability to walk | 156 | no information | 0.6 | (1) | ||
| No, I’m bedridden | 5.1 | (8) | ||||
| No, I have a wheelchair | 9.0 | (14) | ||||
| Yes, using a cane, walker or crutches | 26.9 | (42) | ||||
| Yes, with someone’s help | 14.7 | (23) | ||||
| Yes | 43.6 | (68) | ||||
| Ability to walk today | 156 | no information | 9.0 | (14) | ||
| No, I’m bedridden | 11.5 | (18) | ||||
| No, only with assistance | 34.6 | (54) | ||||
| Yes | 44.9 | (70) | ||||
| Using health care over the last 12 months | 144 | Seen a doctor | 4.0 | (4.0) | ||
| 150 | been admitted to hospital | 1.0 | (2.0) | |||
| 138 | nights spent in hospital | 7.0 | (20.0) | |||
| prescribed medication | 156 | on nutritionDay | 8.0 | (5.0) | ||
| Self-reported health status | 156 | no information | 0.6 | (1) | ||
| very poor | 7.1 | (11) | ||||
| poor | 30.1 | (47) | ||||
| fair | 37.8 | (59) | ||||
| good | 22.4 | (35) | ||||
| very good | 1.9 | (3) | ||||
| Eating behaviour before admission | 156 | no information | 3.2 | (5) | ||
| more than normal | 1.9 | (3) | ||||
| normal | 59.6 | (93) | ||||
| ¾ of normal | 10.3 | (16) | ||||
| ½ of normal | 16.0 | (25) | ||||
| ¼ of normal to nothing | 9.0 | (14) | ||||
| Eating behaviour on nutritionDay | 156 | no information | 1.9 | (3) | ||
| all | 48.1 | (75) | ||||
| ¾ portion | 0.6 | (1) | ||||
| ½ portion | 33.3 | (52) | ||||
| ¼ portion | 10.3 | (16) | ||||
| nothing | 5.8 | (9) | ||||
| Satisfaction with offered hospital food | 156 | no information | 7.1 | (11) | ||
| very/somewhat satisfied | 66.0 | (103) | ||||
| neutral | 17.9 | (28) | ||||
| dissatisfied/very dissatisfied | 9.0 | (14) | ||||
| Weight in kg | 134 | 69.1 | (22.2) | |||
| BMI in kg/m2 | 125 | 24.2 | (6.7) | |||
| Unintended weight lost | 61 | last 3 months, kg | 6.0 | (7.0) | ||
| 54 | last 3 months, % of body weight | 10.3 | (8.8) | |||
| Malnutrition risk (MUST) | 136 | medium risk | 16.9 | (23) | ||
| high risk | 33.8 | (46) | ||||
| Malnourished | 136 | ESPEN guidelines | 28.1 | (38) |
| n | Get Any Nutritional Intervention | p | r | |||
|---|---|---|---|---|---|---|
| % | (n) | |||||
| MUST | 136 | Low risk | 10.4 | (7) | 0.023 | 0.235 |
| Medium risk | 8.7 | (2) | ||||
| High risk | 28.3 | (13) | ||||
| Malnutrition ESPEN | 135 | Not malnourished | 12.4 | (12) | 0.103 | |
| Malnourished | 23.7 | (9) | ||||
| BMI < 18.5 kg/m2 | 135 | BMI ≥ 18.5 kg/m2 | 12.9 | (15) | 0.038 | 0.179 |
| BMI < 18.5 kg/m2 | 31.6 | (6) | ||||
| Inadequate eating behaviour | 156 | No | 12.1 | (6) | 0.081 | |
| Yes | 23.5 | (23) | ||||
| Malnourished, identified by staff | 156 | not malnourished | 11.5 | (15) | <0.001 | 0.453 |
| At risk | 46.2 | (6) | ||||
| malnourished | 69.2 | (9) | ||||
| n | Mdn (IQR) | p | r | ||
|---|---|---|---|---|---|
| Inadequate | Not Inadequate | ||||
| Age | 98/58 | 79.5 (12.3) | 77.0 (15) | 0.144 | |
| Weight | 83/51 | 67.8 (21.1) | 71.0 (25.4) | 0.608 | |
| BMI | 79/46 | 23.8 (6.5) | 24.8 (8.2) | 0.868 | |
| Eating before admission | 98/58 | 4.0 (2.0) | 4.0 (0.0) | <0.001 | −0.313 |
| MUST Score | 85/51 | 1.0 (2.0) | 0.0 (2.0) | 0.079 | |
| Number of different medications (on nutritionDay) | 98/58 | 8.0 (5.0) | 8.0 (6.0) | 0.775 | |
| Self reported health | 98/58 | 3.0 (1.0) | 3.0 (2.0) | 0.001 | −0.276 |
| Times seen a doctor | 88/56 | 4.0 (3.7) | 3.5 (7.5) | 0.650 | |
| Times been in hospital | 95/55 | 1.0 (2.0) | 1.0 (2.0) | 0.555 | |
| Number of nights in hospital | 84/54 | 7.0 (21.0) | 4.5 (17.8) | 0.302 | |
| Number of chronic diseases | 98/58 | 2.0 (2.0) | 2.0 (2.2) | 0.121 | |
| Unintended weight loss last 3 months (kg) | 46/15 | 6.0 (7.0) | 5.0 (3.0) | 0.480 | |
| Unintended weight loss last 3 months (%) | 40/14 | 10.6 (6.8) | 8.4 (7.3) | 0.407 | |
| Satisfaction with the offered meal | 98/58 | 4.0 (2.0) | 4.0 (1.0) | 0.175 | |
| Length of stay | 92/53 | 14.0 (11.0) | 10.0 (11.5) | 0.036 | −0.174 |
| General walking ability | 97/58 | 2.0 (2.0) | 2.0 (2.0) | 0.422 | |
| Walking ability today | 90/54 | 2.0 (1.0) | 1.0 (1.0) | 0.002 | −0.255 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Graeb, F.; Wolke, R. Malnutrition and Inadequate Eating Behaviour during Hospital Stay in Geriatrics—An Explorative Analyses of NutritionDay Data in Two Hospitals. Nurs. Rep. 2021, 11, 929-941. https://doi.org/10.3390/nursrep11040085
Graeb F, Wolke R. Malnutrition and Inadequate Eating Behaviour during Hospital Stay in Geriatrics—An Explorative Analyses of NutritionDay Data in Two Hospitals. Nursing Reports. 2021; 11(4):929-941. https://doi.org/10.3390/nursrep11040085
Chicago/Turabian StyleGraeb, Fabian, and Reinhold Wolke. 2021. "Malnutrition and Inadequate Eating Behaviour during Hospital Stay in Geriatrics—An Explorative Analyses of NutritionDay Data in Two Hospitals" Nursing Reports 11, no. 4: 929-941. https://doi.org/10.3390/nursrep11040085
APA StyleGraeb, F., & Wolke, R. (2021). Malnutrition and Inadequate Eating Behaviour during Hospital Stay in Geriatrics—An Explorative Analyses of NutritionDay Data in Two Hospitals. Nursing Reports, 11(4), 929-941. https://doi.org/10.3390/nursrep11040085