
Facilitators and Barriers to Implementation of a Childhood Tuberculosis Control Program in Bangladesh: A Mixed-Methods Study from BRAC Urban DOTS Centres in Dhaka

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
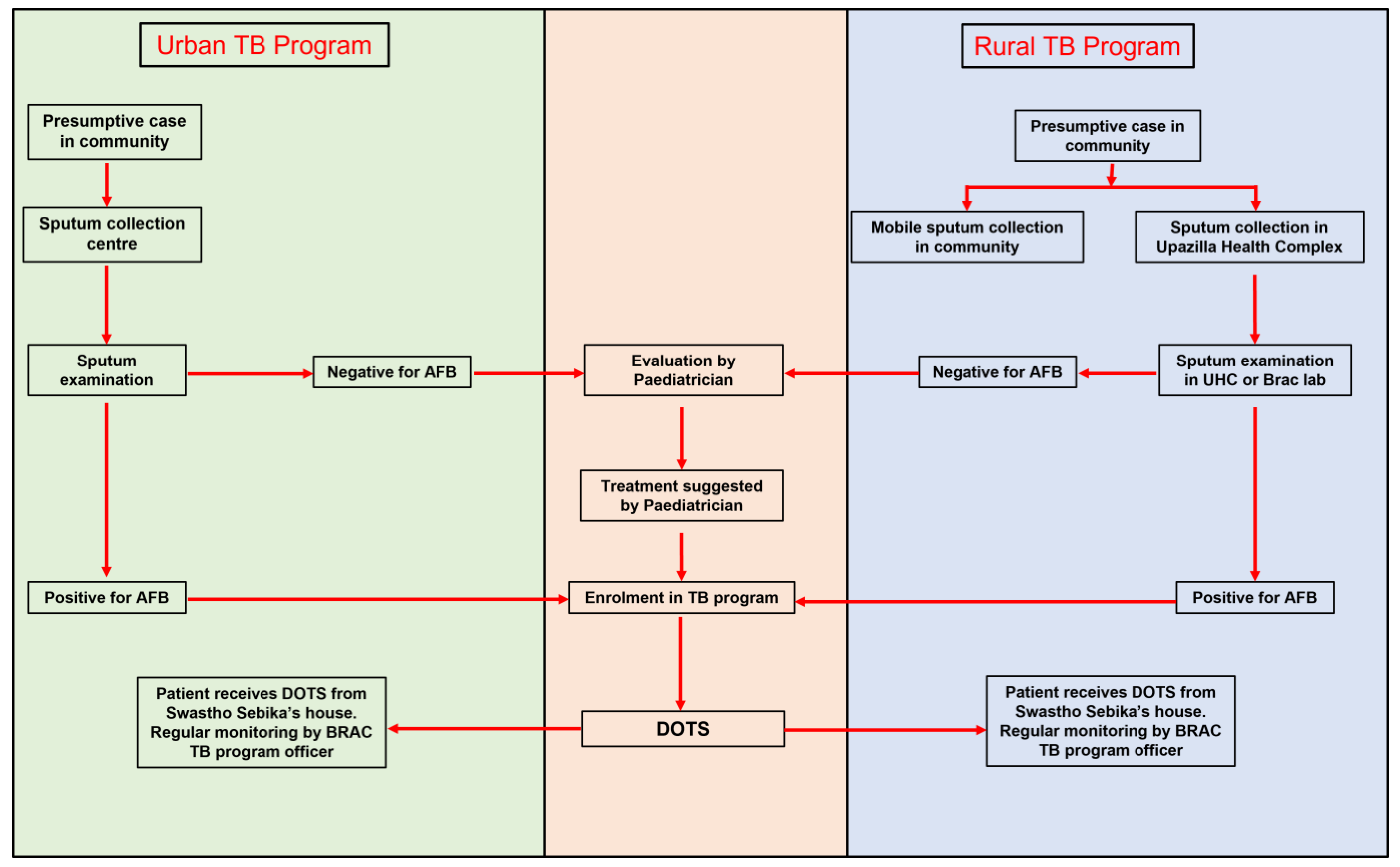
2.1. Implementation of Childhood TB in Bangladesh
2.2. Study Design and Setting
2.2.1. Quantitative Component
2.2.2. Qualitative Component
2.3. Study Tools
2.4. Data Collection
2.5. Data Analysis
2.5.1. Quantitative Data Analysis
2.5.2. Qualitative Data Analysis
2.6. Ethics
3. Results
3.1. Survey Findings
3.1.1. Knowledge on Childhood TB
3.1.2. Attitude on Childhood TB
3.1.3. Practice Regarding Childhood TB
3.1.4. Bivariate Analysis
3.2. Qualitative Findings
3.2.1. Pillar 1: Integrated Patient-Centred Care
Training and Capacity Building
“In the field level, their (community volunteers’) role is to identify the suspects; they need to learn these criteria (for diagnosis) … they need to know how to refer these cases and when diagnosed, how to link these cases to DOTS provider...”(KII 4)
The Complexity of Diagnosis of Childhood TB
“When other diagnosis cannot prove, then the physician will be thinking that it might be a case of tuberculosis”(KII 1)
Guideline for Childhood TB
Financial Assistance
“…financial support is big term… We started this journey around 2012. If you see the case trend from 2013 there is big jump in 2013, a sharp jump (in the number of TB patients)”(KII 10).
Awareness of Childhood TB
Underreporting of TB Cases
“…now we have covered around 62% of the estimated cases under detection. So, we are thinking that those missing cases may be in private sectors. Either not diagnosed at all or if diagnosed may be in the private sectors…”(KII 6).
“So, then government circulated that gadget as mandatory notification. But only gadget cannot ensure. We have to make it functional (operationalize) this”(KII 6).
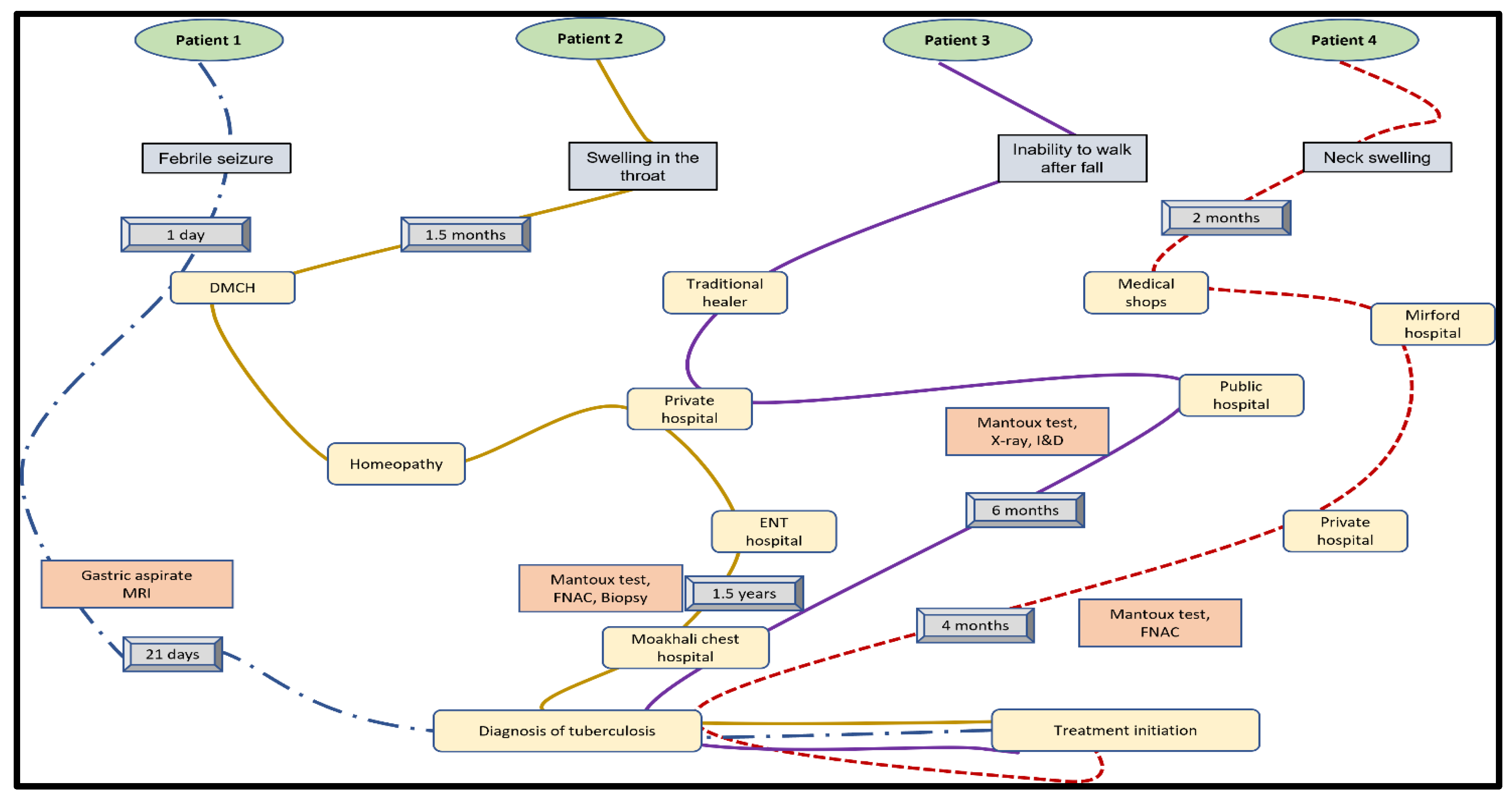
Delay in Diagnosis
Child Friendly Regimen
“Children don’t want to take it, they want to throw away. And different types of problem”(IDI 26).
Active Surveillance during Diagnosis and Treatment
“To ensure they go for diagnosis, I go with them and help them with it, and if I can’t go, I contact them and ask whether they visited the doctor or not”(IDI 27).
“The medicine is for 6 months. After completing the dose for 2 months, the child starts feeling better. That time child does not want to continue medicine. These are the barriers. That is why our duty (supervision) is going on”(IDI-3).
3.2.2. Pillar 2: Bold Policies and Supportive Systems
“In Bangladesh the government and non-government collaboration is excellent… the whole TB program in Bangladesh is being implemented by NGOs where government stewards the program”(KII 3).
3.2.3. Pillar 3: Intensified Research and Innovations
4. Discussion
5. Strength and Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- Petersen, E.; Al-Abri, S.; Chakaya, J.; Goletti, D.; Parolina, L.; Wejse, C.; Mucheleng’Anga, L.A.; Khalili, S.A.; Yeboah-Manu, D.; Chanda-Kapata, P.; et al. World TB Day 2022: Revamping and Reshaping Global TB Control Programs by Advancing Lessons learnt from the COVID-19 pandemic. Int. J. Infect. Dis. 2022. [Google Scholar] [CrossRef]
- Kyu, H.H.; Maddison, E.R.; Henry, N.J.; Ledesma, J.R.; Wiens, K.E.; Reiner, R., Jr.; Biehl, M.H.; Shields, C.; Osgood-Zimmerman, A.; Ross, J.M.; et al. Global, regional, and national burden of tuberculosis, 1990–2016: Results from the Global Burden of Diseases, Injuries, and Risk Factors 2016 Study. Lancet Infect. Dis. 2018, 18, 1329–1349. [Google Scholar] [CrossRef] [Green Version]
- Nkereuwem, E.; Kampmann, B.; Togun, T. The need to prioritise childhood tuberculosis case detection. Lancet 2021, 397, 1248–1249. [Google Scholar] [CrossRef]
- Basnyat, B.; Caws, M.; Udwadia, Z. Tuberculosis in South Asia: A tide in the affairs of men. Multidiscip. Respir. Med. 2018, 13, 10. [Google Scholar] [CrossRef] [Green Version]
- Kanabus, A. Information about Tuberculosis. Available online: https://tbfacts.org/tb-statistics/ (accessed on 14 April 2021).
- World Health Organization. Global Tuberculosis Report; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Dodd, P.J.; Gardiner, E.; Coghlan, R.; Seddon, J.A. Burden of childhood tuberculosis in 22 high-burden countries: A mathematical modelling study. Lancet Glob. Health 2014, 2, e453–e459. [Google Scholar] [CrossRef] [Green Version]
- Perez-Velez, C.M.; Marais, B.J. Tuberculosis in Children. N. Engl. J. Med. 2012, 367, 348–361. [Google Scholar] [CrossRef] [Green Version]
- Fry, S.; Barnabas, S.; Cotton, M. Update on trends in childhood tuberculosis. Curr. Opin. Pediatr. 2018, 30, 152–160. [Google Scholar] [CrossRef]
- National Tuberculosis Program. Tuberculosis Control in Bangladesh Annual Report 2015; National Tuberculosis Control Program, Directorate General of Health Services: Dhaka, Bangladesh, 2015. [Google Scholar]
- National Tuberculosis Program. Tuberculosis Control in Bangladesh Annual Report 2016; National Tuberculosis Control Program, Directorate General of Health Services: Dhaka, Bangladesh, 2016. [Google Scholar]
- National Tuberculosis Control Program. Tuberculosis Control in Bangladesh Annual Report 2020; National Tuberculosis Control Program, Directorate General of Health Services: Dhaka, Bangladesh, 2020. [Google Scholar]
- World Health Organization. The End TB Strategy; WHO: Geneva, Switzerland, 2015; p. 20. [Google Scholar]
- Bjerrum, S.; Rose, M.V.; Bygbjerg, I.C.; Mfinanga, S.G.; Tersboel, B.P.; Ravn, P. Primary health care staff’s perceptions of childhood tuberculosis: A qualitative study from Tanzania. BMC Health Serv. Res. 2012, 12, 6. [Google Scholar] [CrossRef] [Green Version]
- Arifeen, S.; Christou, A.; Reichenbach, L.; Osman, F.A.; Azad, K.; Islam, K.S.; Ahmed, F.; Perry, H.B.; Peters, D. Community-based approaches and partnerships: Innovations in health-service delivery in Bangladesh. Lancet 2013, 382, 2012–2026. [Google Scholar] [CrossRef]
- Islam, Z.; Sanin, K.I.; Ahmed, T. Improving case detection of tuberculosis among children in Bangladesh: Lessons learned through an implementation research. BMC Public Health 2017, 17, 131. [Google Scholar] [CrossRef] [Green Version]
- Chiang, S.S.; Swanson, D.S.; Starke, J.R. New Diagnostics for Childhood Tuberculosis. Infect. Dis. Clin. N. Am. 2015, 29, 477–502. [Google Scholar] [CrossRef]
- Marais, B.J. Improving access to tuberculosis preventive therapy and treatment for children. Int. J. Infect. Dis. 2017, 56, 122–125. [Google Scholar] [CrossRef] [Green Version]
- Nataprawira, H.M.; Wonoputri, N. Obstacles Facing Tuberculosis Treatment in Children from a Developing Country: A Hospital-based Study. Am. J. Epidemiol. Infect. Dis. 2014, 2, 8–12. [Google Scholar]
- Okwara, F.; Oyore, J.; Were, F. The challenges fraughting isoniazid prophylaxis as a child tuberculosis prevention strategy in high burden settings in Nairobi, Kenya. East Cent. Afr. Med. J. 2015, 2, 39–45. [Google Scholar]
- Aung, K.; Van Deun, A.; Declercq, E.; Sarker, M.; Das, P.; Hossain, M.; Rieder, H. Successful ‘9-month Bangladesh regimen’ for multidrug-resistant tuberculosis among over 500 consecutive patients. Int. J. Tuberc. Lung Dis. 2014, 18, 1180–1187. [Google Scholar] [CrossRef]
- World Health Organization. Guidance for National Tuberculosis Programmes on the Management of Tuberculosis in Children; WHO: Geneva, Switzerland, 2006; p. 50. [Google Scholar]
- World Health Organization. Roadmap for Childhood Tuberculosis: Towards Zero Deaths; WHO: Geneva, Switzerland, 2013; p. 39. [Google Scholar]
- National Tuberculosis Program. National Guidelines for the Management of Tuberculosis in Children, 2nd ed.; National Tuberculosis Control Program, Directorate General of Health Services: Dhaka, Bangladesh, 2012. [Google Scholar]
- Creswell, J.W.; Fetters, M.D.; Ivankova, N.V. Designing A Mixed Methods Study in Primary Care. Ann. Fam. Med. 2004, 2, 7–12. [Google Scholar] [CrossRef] [Green Version]
- Jick, T.D. Mixing Qualitative and Quantitative Methods: Triangulation in Action. Adm. Sci. Q. 1979, 24, 602–611. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, S.M. Taking healthcare where the community is: The story of the Shasthya Sebikas of BRAC in Bangladesh. BRAC Univ. J. 2008, 5, 39–45. [Google Scholar]
- World Health Organization. Advocacy, Communication and Social Mobilization for TB Control: A Guide to Developing Knowledge, Attitude and Practice Surveys; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Noé, A.; Ribeiro, R.M.; Anselmo, R.; Maixenchs, M.; Sitole, L.; Munguambe, K.; Blanco, S.; Souef, P.L.; García-Basteiro, A.L. Knowledge, attitudes and practices regarding tuberculosis care among health workers in Southern Mozambique. BMC Pulm. Med. 2017, 17, 2. [Google Scholar] [CrossRef] [Green Version]
- Bacay-Domingo, M.C.N.; Ong-Lim, A.L. A Descriptive Study of the Knowledge, Attitudes and Practices on Tuberculosis among Treatment Partners of Pediatric Patients in Tarlac City. Pediatr. Infect. Dis. Soc. Philipp. J. 2009, 10, 28–34. [Google Scholar]
- Kanjee, Z.; Catterick, K.; Moll, A.; Amico, K.; Friedland, G. Tuberculosis infection control in rural South Africa: Survey of knowledge, attitude and practice in hospital staff. J. Hosp. Infect. 2011, 79, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Pinnock, H.; Barwick, M.; Carpenter, C.; Eldridge, S.; Grandes, G.; Griffiths, C.J.; Rycroft-Malone, J.; Meissner, P.; Murray, E.; Patel, A.; et al. Standards for Reporting Implementation Studies (StaRI) Statement. BMJ 2017, 356, i6795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awofeso, N.; Schelokova, I.; Dalhatu, A. Training of front-line health workers for tuberculosis control: Lessons from Nigeria and Kyrgyzstan. Hum. Resour. Health 2008, 6, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kc, A.; Nelin, V.; Raaijmakers, H.; Kim, H.J.; Singh, C.; Målqvist, M. Increased immunization coverage addresses the equity gap in Nepal. Bull. World Health Organ. 2017, 95, 261–269. [Google Scholar] [CrossRef]
- Paul, S.; Akter, R.; Aftab, A.; Khan, A.M.; Barua, M.; Islam, S.; Islam, A.; Husain, A.; Sarker, M. Knowledge and attitude of key community members towards tuberculosis: Mixed method study from BRAC TB control areas in Bangladesh. BMC Public Health 2015, 15, 52. [Google Scholar] [CrossRef] [Green Version]
- Weyer, K.; Mirzayev, F.; Migliori, G.B.; Van Gemert, W.; D’Ambrosio, L.; Zignol, M.; Floyd, K.; Centis, R.; Cirillo, D.M.; Tortoli, E.; et al. Rapid molecular TB diagnosis: Evidence, policy making and global implementation of Xpert MTB/RIF. Eur. Respir. J. 2013, 42, 252–271. [Google Scholar] [CrossRef] [Green Version]
- Giang, D.C.; Duong, T.N.; Thanh, P.D.; Nhan, H.T.; Wolbers, M.; Nhu, N.T.Q.; Heemskerk, D.; Quang, N.D.; Phuong, D.T.; Hang, P.T.; et al. Prospective evaluation of GeneXpert for the diagnosis of HIV- negative pediatric TB cases. BMC Infect. Dis. 2015, 15, 70. [Google Scholar] [CrossRef] [Green Version]
- Sisay, S.; Mengistu, B.; Erku, W.; Woldeyohannes, D. Directly Observed Treatment Short-course (DOTS) for tuberculosis control program in Gambella Regional State, Ethiopia: Ten years experience. BMC Res. Notes 2014, 7, 44. [Google Scholar] [CrossRef] [Green Version]
- Van Deun, A.; Maug, A.K.J.; Salim, A.H.; Das, P.K.; Sarker, M.R.; Daru, P.; Rieder, H.L. Short, Highly Effective, and Inexpensive Standardized Treatment of Multidrug-resistant Tuberculosis. Am. J. Respir. Crit. Care Med. 2010, 182, 684–692. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Methods | Respondents | Objectives Addressed | |
|---|---|---|---|
| Quantitative Component | Survey | Shasthya Shebika * (SS) (n = 116) | To find out the knowledge, attitude and practices for diagnosis and treatment of childhood TB among front-line health care workers |
| Qualitative Component | In-depth interview (IDI) (n = 32) | SS (n = 18), Program Organizers (n = 6), Laboratory Technicians (n = 2), Area Managers (n = 2), Mother of children with active TB (n = 4) | To explore the field level challenges in diagnosis and treatment of childhood TB |
| Key informant interview (KII) (n = 9) | BRAC (n = 4), National Tuberculosis Program (n = 2), Damien Foundation (n = 1), WHO National Professional Officer (n = 1), Tuberculosis Research Specialist (n = 1) | To explore the implementation pathway, strategic policies around diagnosis and treatment of childhood TB | |
| A-Priori Codes | Code | Sub-Code |
|---|---|---|
| Facilitators for Diagnosis (FD) | Human Resource | Availability of Pediatrician, doctors, health care workers, lab technicians, SS |
| Lab Facilities | Chest X-ray, Mantoux test, Sputum AFB, Availability of GeneXpert | |
| Monetary | Financial Benefits to clients, Stipend, Incentives to service providers | |
| Barriers for Diagnosis (BD) | Socio-economic Condition | Poverty, Education, |
| Awareness | Lack of awareness, doubts about staff’s competency, belief that BCG vaccine protects children | |
| Human Resources | Availability of Pediatrician, doctors, health care workers, lab technicians, SS | |
| Lab Facilities | Chest X-ray, Mantoux test, Sputum AFB, GeneXpert | |
| Program Activities | Active case detection, Contact tracing, Screening Camps | |
| Compliance | Lack of adherence to National Guidelines | |
| Facilitators for Treatment (FT): | Medicine | Childhood TB regimen, Child friendly drugs, Free access, Availability |
| Service Delivery | Medicine delivery at home, Supervision by SS | |
| Monetary | Treatment bond money, Incentives to patient, Incentives to service provider | |
| Barriers for Treatment (BT) | Socio-economic Condition | Location from DOTS center, Education, Poverty, |
| Awareness | Stigma, feeling of weakness of child, belief that medicines will harm child | |
| Physical Conditions | Difficult in swallowing, Vomiting, Nausea, children being difficult patients, poor compliance | |
| Drug Properties | Taste, Size, Side effects (red urine, jaundice), lack of child friendly regimens (syrup, dispersible tablets), long treatment duration, many tablets | |
| Supply side | Lack of child regimen, stock out of drugs, delay in procurement |
| Category (n = 111 Expect Otherwise Stated) | Total Respondents n (%) | High Performing Centres n (%) | Low Performing Centres n (%) |
|---|---|---|---|
| Age | |||
| <30 years | 10 (9.0) | 6 (11) | 4 (7) |
| 30–50 years | 80 (72.1) | 38 (70) | 42 (74) |
| >50 years | 21 (18.9) | 10 (18) | 11 (19) |
| Education | |||
| Never Attended | 23 (20.8) | 11 (20) | 12 (21) |
| Primary | 41 (36.9) | 18 (33) | 23 (40) |
| Secondary | 41 (36.9) | 23 (43) | 18 (32) |
| Higher Secondary or Above | 6 (5.4) | 2 (6) | 4 (7) |
| Number of adult cases who completed treatment in past 12 months | |||
| <2 | 8 (7) | 2 (6) | 6 (10) |
| “2–5” | 42 (38) | 23 (43) | 19 (33) |
| “5–10” | 40 (36) | 18 (33) | 22 (39) |
| > = 10 | 21 (19) | 11 (20) | 10 (18) |
| Duration of providing medicine to child tuberculosis cases (n = 40) | |||
| <2 years | 14 (35) | 5 (33) | 9 (36) |
| 2–5 years | 15 (38) | 5 (33) | 10 (40) |
| 5–10 years | 4 (10) | 3 (20) | 1 (4) |
| > = 10 years | 7 (17) | 2 (14) | 5 (20) |
| Duration of Work | |||
| <5 years | 11 (10) | 5 (9) | 6 (10) |
| 5–10 years | 35 (31) | 21 (39) | 14 (25) |
| > = 10 years | 65 (59) | 28 (52) | 37 (65) |
| Name of the Pillar | Facilitator | Barrier |
| Patient-Centered Care (Pillar 1) |
|
|
| Bold Policies and Supportive System (Pillar 2) |
|
|
| Intensified research ((Pillar 3) |
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pantha, S.; Aguinaldo, M.J.; Hasan-ul-Bari, S.M.; Chowdhury, S.; Dendup, U.; Gupta, R.D.; Sutradhar, I.; Bari, R.; Sarker, M. Facilitators and Barriers to Implementation of a Childhood Tuberculosis Control Program in Bangladesh: A Mixed-Methods Study from BRAC Urban DOTS Centres in Dhaka. Nurs. Rep. 2022, 12, 371-386. https://doi.org/10.3390/nursrep12020036
Pantha S, Aguinaldo MJ, Hasan-ul-Bari SM, Chowdhury S, Dendup U, Gupta RD, Sutradhar I, Bari R, Sarker M. Facilitators and Barriers to Implementation of a Childhood Tuberculosis Control Program in Bangladesh: A Mixed-Methods Study from BRAC Urban DOTS Centres in Dhaka. Nursing Reports. 2022; 12(2):371-386. https://doi.org/10.3390/nursrep12020036
Chicago/Turabian StylePantha, Sandesh, Ma. Jennylyn Aguinaldo, S. M. Hasan-ul-Bari, Sayantan Chowdhury, Ugyen Dendup, Rajat Das Gupta, Ipsita Sutradhar, Rahamatul Bari, and Malabika Sarker. 2022. "Facilitators and Barriers to Implementation of a Childhood Tuberculosis Control Program in Bangladesh: A Mixed-Methods Study from BRAC Urban DOTS Centres in Dhaka" Nursing Reports 12, no. 2: 371-386. https://doi.org/10.3390/nursrep12020036
APA StylePantha, S., Aguinaldo, M. J., Hasan-ul-Bari, S. M., Chowdhury, S., Dendup, U., Gupta, R. D., Sutradhar, I., Bari, R., & Sarker, M. (2022). Facilitators and Barriers to Implementation of a Childhood Tuberculosis Control Program in Bangladesh: A Mixed-Methods Study from BRAC Urban DOTS Centres in Dhaka. Nursing Reports, 12(2), 371-386. https://doi.org/10.3390/nursrep12020036