

A Novel Approach to Managing a COVID-19 Outbreak at a Farm in Outer Regional Victoria, Australia

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Outbreak Investigation Team
2.2. Outbreak Detection and Case Finding
2.3. Analysis
2.4. Public Health Interventions
3. Results
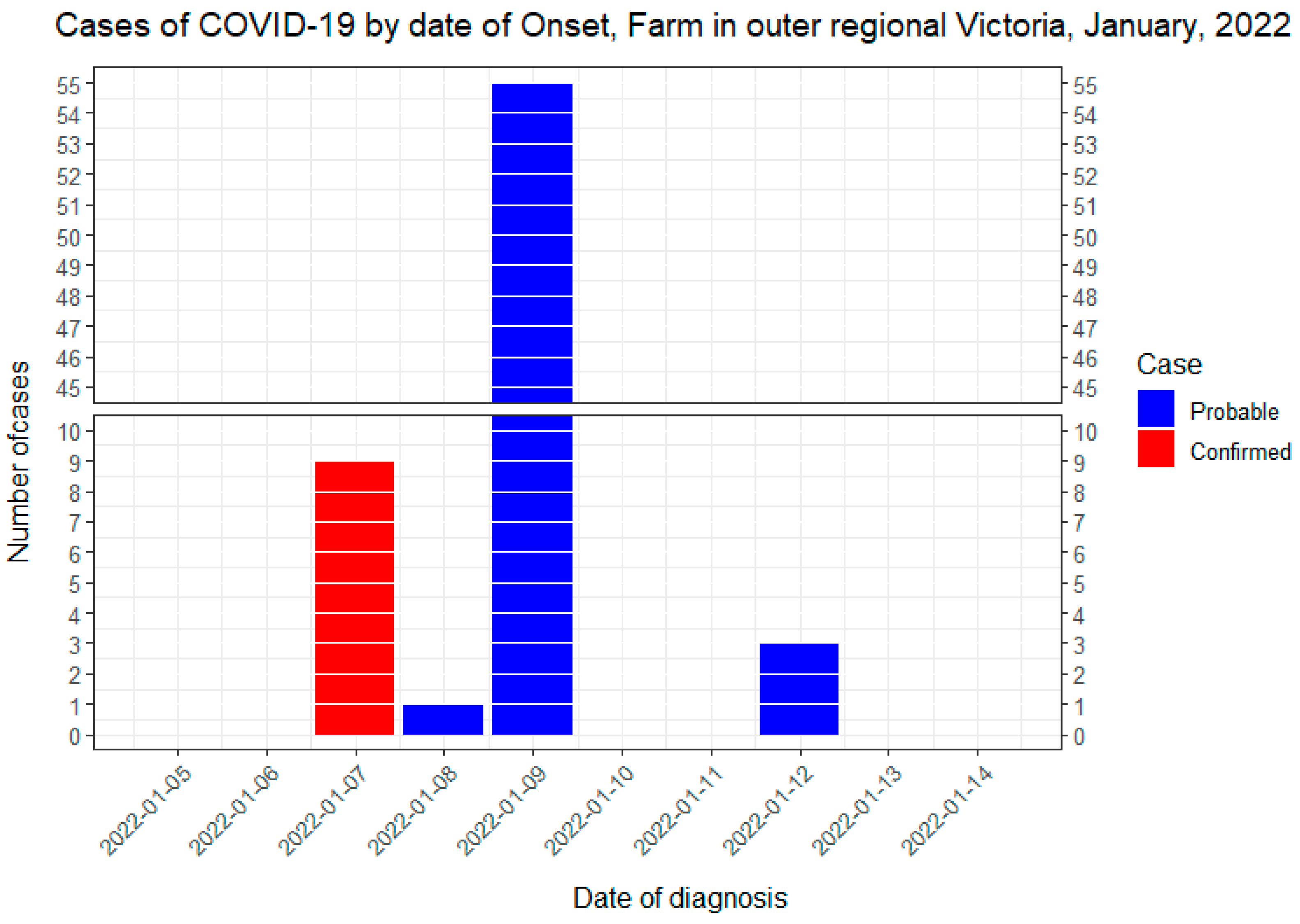
3.1. Epidemiological Investigation and Case Identification
3.2. Outbreak Management and Implementation of Cohorting
4. Discussion
Lessons Learned
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lawrence, G.; Richards, C.; Lyons, K. Food security in Australia in an era of neoliberalism, productivism and climate change. J. Rural Stud. 2013, 29, 30–39. [Google Scholar] [CrossRef] [Green Version]
- Millar, J.; Roots, J. Changes in Australian agriculture and land use: Implications for future food security. Int. J. Agric. Sustain. 2011, 10, 25–39. [Google Scholar] [CrossRef]
- Holley, A.; Coatsworth, N.; Lipman, J. The Australian response to the COVID-19 pandemic: A co-ordinated and effective strategy. Anaesth. Crit. Care Pain Med. 2021, 40, 100859. [Google Scholar] [CrossRef] [PubMed]
- Department of Health—Victorian Government. COVIDSafe Plan. 2022. Available online: https://www.coronavirus.vic.gov.au/covidsafe-plan#creating-a-covidsafe-plan (accessed on 23 June 2022).
- Murray, L.R. Sick and Tired of Being Sick and Tired: Scientific Evidence, Methods, and Research Implications for Racial and Ethnic Disparities in Occupational Health. Am. J. Public Health 2003, 93, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Etienne, C.F. COVID-19 has revealed a pandemic of inequality. Nat. Med. 2022, 28, 17. [Google Scholar] [CrossRef] [PubMed]
- Australian Beureau of Statistics. Characteristics of Employment, Australia. 2021. Available online: https://www.abs.gov.au/statistics/labour/earnings-and-working-conditions/characteristics-employment-australia/latest-release#data-download (accessed on 23 June 2022).
- Parliament of Australia. COVID-19: A Chronology of State and Territory Government Announcements (up until 30 June 2020). 2020. Available online: https://www.aph.gov.au/About_Parliament/Parliamentary_Departments/Parliamentary_Library/pubs/rp/rp2021/Chronologies/COVID-19StateTerritoryGovernmentAnnouncements#_Toc52275792 (accessed on 23 June 2022).
- MacLellan, N.; Mares, P. Labour Mobility in the Pacific: Creating seasonal work programs in Australia. In Globalization and Governance in the Pacific Islands; ANU E Press: Canberra, Australia, 2006; pp. 137–171. ISBN 192094298X. [Google Scholar]
- Pacific Australia Labour Mobility. Supporting Workers While They Are in Australia. 2022. Available online: https://www.palmscheme.gov.au/ (accessed on 23 June 2022).
- Nangiloc; Colignan; Iraak. Nangiloc, Colignan and Iraak. 2022. Available online: https://nangiloc.vic.au/ (accessed on 23 June 2022).
- Department of Health—Victorian Government. Transmission and Response Epidemiology Victorian (TREVI) System; Department of Health—Victorian Government: Melbourne, Australia.
- Victorian Department of Health. Coronavirus (COVID-19) Victoria. Available online: https://www.coronavirus.vic.gov.au/ (accessed on 23 June 2022).
- Jamaludin, S.; Azmir, N.A.; Ayob, A.F.M.; Zainal, N. COVID-19 exit strategy: Transitioning towards a new normal. Ann. Med. Surg. 2020, 59, 165–170. [Google Scholar] [CrossRef] [PubMed]
- Department of Health—Victorian Government. Coronavirus (COVID-19) Guidance Note for the Victorian Public Service and Sector. 16 August 2021. Available online: https://www.vic.gov.au/coronavirus-covid-19-guidance-note-victorian-public-service-and-sector (accessed on 23 June 2022).
- Mema, S.; Frosst, G.; Hanson, K.; Yates, C.; Anderson, A.; Jacobsen, J.; Guinar, C.; Lima, A.; Andersen, T.; Roe, M. COVID-19 outbreak among temporary foreign workers in British Columbia, March to May 2020. Can. Commun. Dis. Rep. = Relev. des Mal. Transm. au Can. 2021, 47, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Maslo, C.; Friedland, R.; Toubkin, M.; Laubscher, A.; Akaloo, T.; Kama, B. Characteristics and outcomes of hospitalized patients in South Africa during the COVID-19 Omicron wave compared with previous waves. JAMA 2022, 327, 583–584. [Google Scholar] [CrossRef] [PubMed]
- Veneti, L.; Bøås, H.; Kristoffersen, A.B.; Stålcrantz, J.; Bragstad, K.; Hungnes, O.; Storm, N.L.; Aasand, N.; Rø, G.; Starrfelt, J.; et al. Reduced risk of hospitalisation among reported COVID-19 cases infected with the SARS-CoV-2 Omicron BA. 1 variant compared with the Delta variant, Norway, December 2021 to January 2022. Eurosurveillance 2022, 27, 2200077. [Google Scholar] [CrossRef]
- Ward, I.L.; Bermingham, C.; Ayoubkhani, D.; Gethings, O.J.; Pouwels, K.; Yates, T.; Khunti, K.; Hippisley-Cox, J.; Banerjee, A.; Walker, A.S.; et al. Risk of COVID-19 related deaths for SARS-CoV-2 omicron (B.1.1.529) compared with delta (B.1.617.2): Retrospective cohort study. BMJ 2022, 378, e070695. [Google Scholar] [CrossRef] [PubMed]
- Castañeda, H.; Carrion, I.V.; Kline, N.; Tyson, D.M. False hope: Effects of social class and health policy on oral health inequalities for migrant farmworker families. Soc. Sci. Med. 2010, 71, 2028–2037. [Google Scholar] [CrossRef] [PubMed]
- McElfish, P.A.; Hallgren, E.; Yamada, S. Effect of US Health Policies on Health Care Access for Marshallese Migrants. Am. J. Public Health 2015, 105, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Okonkwo, N.E.; Aguwa, U.T.; Jang, M.; Barré, I.A.; Page, K.R.; Sullivan, P.S.; Beyrer, C.; Baral, S. COVID-19 and the US response: Accelerating health inequities. BMJ Evid.-Based Med. 2020, 26, 176–179. [Google Scholar] [CrossRef] [PubMed]
- Jeewandara, C.; Guruge, D.; Pushpakumara, P.D.; Madhusanka, D.; Jayadas, T.T.; Chaturanga, I.P.; Aberathna, I.S.; Danasekara, S.; Pathmanathan, T.; Jayathilaka, D.; et al. Sensitivity and specificity of two WHO approved SARS-CoV2 antigen assays in detecting patients with SARS-CoV2 infection. BMC Infect. Dis. 2022, 22, 276. [Google Scholar] [CrossRef]
- Peña, M.; Ampuero, M.; Garcés, C.; Gaggero, A.; García, P.; Velasquez, M.S.; Luza, R.; Alvarez, P.; Paredes, F.; Acevedo, J.; et al. Performance of SARS-CoV-2 rapid antigen test compared with real-time RT-PCR in asymptomatic individuals. Int. J. Infect. Dis. 2021, 107, 201–204. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics of COVID-19 Cases | Number of Cases | Percent of Total |
|---|---|---|
| Cases | ||
| Confirmed | 9 | 13.8% |
| Probable | 59 | 86.8% |
| Clinical Assessment | ||
| No symptoms | 58 | 85.3% |
| Symptomatic | 10 | 14.7% |
| Hospitalisations | 0 | 0.0% |
| Deaths | 0 | 0.0% |
| Sex | ||
| Men | 57 | 83.8% |
| Women | 11 | 16.2% |
| Age Groups | ||
| 18–29 | 24 | 35.3% |
| 30–39 | 35 | 51.5% |
| 40–49 | 9 | 13.2% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kabwe, M.; Dittmer, J.L.; Oxford, J.; Eyres, C.; Thomas, A.; Mahony, A.; Bolam, B. A Novel Approach to Managing a COVID-19 Outbreak at a Farm in Outer Regional Victoria, Australia. Nurs. Rep. 2022, 12, 717-725. https://doi.org/10.3390/nursrep12040071
Kabwe M, Dittmer JL, Oxford J, Eyres C, Thomas A, Mahony A, Bolam B. A Novel Approach to Managing a COVID-19 Outbreak at a Farm in Outer Regional Victoria, Australia. Nursing Reports. 2022; 12(4):717-725. https://doi.org/10.3390/nursrep12040071
Chicago/Turabian StyleKabwe, Mwila, Jennifer L. Dittmer, Jaimee Oxford, Catina Eyres, Ancara Thomas, Andrew Mahony, and Bruce Bolam. 2022. "A Novel Approach to Managing a COVID-19 Outbreak at a Farm in Outer Regional Victoria, Australia" Nursing Reports 12, no. 4: 717-725. https://doi.org/10.3390/nursrep12040071
APA StyleKabwe, M., Dittmer, J. L., Oxford, J., Eyres, C., Thomas, A., Mahony, A., & Bolam, B. (2022). A Novel Approach to Managing a COVID-19 Outbreak at a Farm in Outer Regional Victoria, Australia. Nursing Reports, 12(4), 717-725. https://doi.org/10.3390/nursrep12040071