
Problematic Internet Use and Resilience: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Systematic Search
2.2. Inclusion Criteria
2.3. Methodological Quality of Included Studies
2.4. Data Coding
2.5. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Section/Topic | # | Checklist Item | Reported on Page # |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review, meta-analysis, or both. | 1 |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary including, as applicable: background; objectives; data sources; study eligibility criteria, participants, and interventions; study appraisal and synthesis methods; results; limitations; conclusions and implications of key findings; systematic review registration number. | 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. | 1–2 |
| Objectives | 4 | Provide an explicit statement of questions being addressed with reference to participants, interventions, comparisons, outcomes, and study design (PICOS). | 2 |
| METHODS | |||
| Protocol and registration | 5 | Indicate if a review protocol exists, if and where it can be accessed (e.g., Web address), and, if available, provide registration information including registration number. | 2 |
| Eligibility criteria | 6 | Specify study characteristics (e.g., PICOS, length of follow-up) and report characteristics (e.g., years considered, language, publication status) used as criteria for eligibility, giving rationale. | 2 |
| Information sources | 7 | Describe all information sources (e.g., databases with dates of coverage, contact with study authors to identify additional studies) in the search and date last searched. | 2 |
| Search | 8 | Present full electronic search strategy for at least one database, including any limits used, such that it could be repeated. | Table A1 |
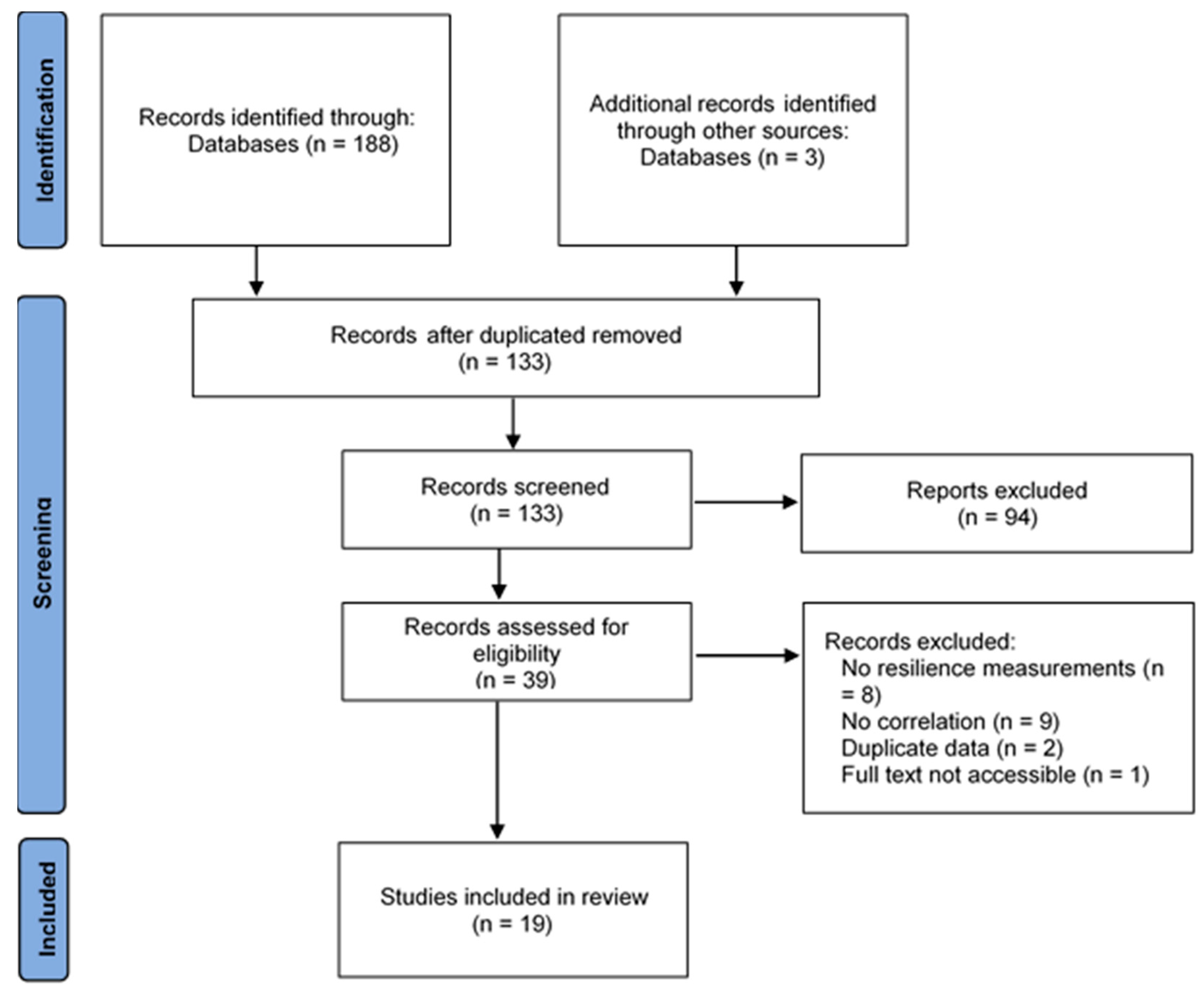
| Study selection | 9 | State the process for selecting studies (i.e., screening, eligibility, included in systematic review, and, if applicable, included in the meta-analysis). | 2 |
| Data collection process | 10 | Describe method of data extraction from reports (e.g., piloted forms, independently, in duplicate) and any processes for obtaining and confirming data from investigators. | 2–3 |
| Data items | 11 | List and define all variables for which data were sought (e.g., PICOS, funding sources) and any assumptions and simplifications made. | 2–3 |
| Risk of bias in individual studies | 12 | Describe methods used for assessing risk of bias of individual studies (including specification of whether this was done at the study or outcome level), and how this information is to be used in any data synthesis. | 2 |
| Summary measures | 13 | State the principal summary measures (e.g., risk ratio, difference in means). | 3 |
| Synthesis of results | 14 | Describe the methods of handling data and combining results of studies, if done, including measures of consistency (e.g., I2) for each meta-analysis. | 3 |
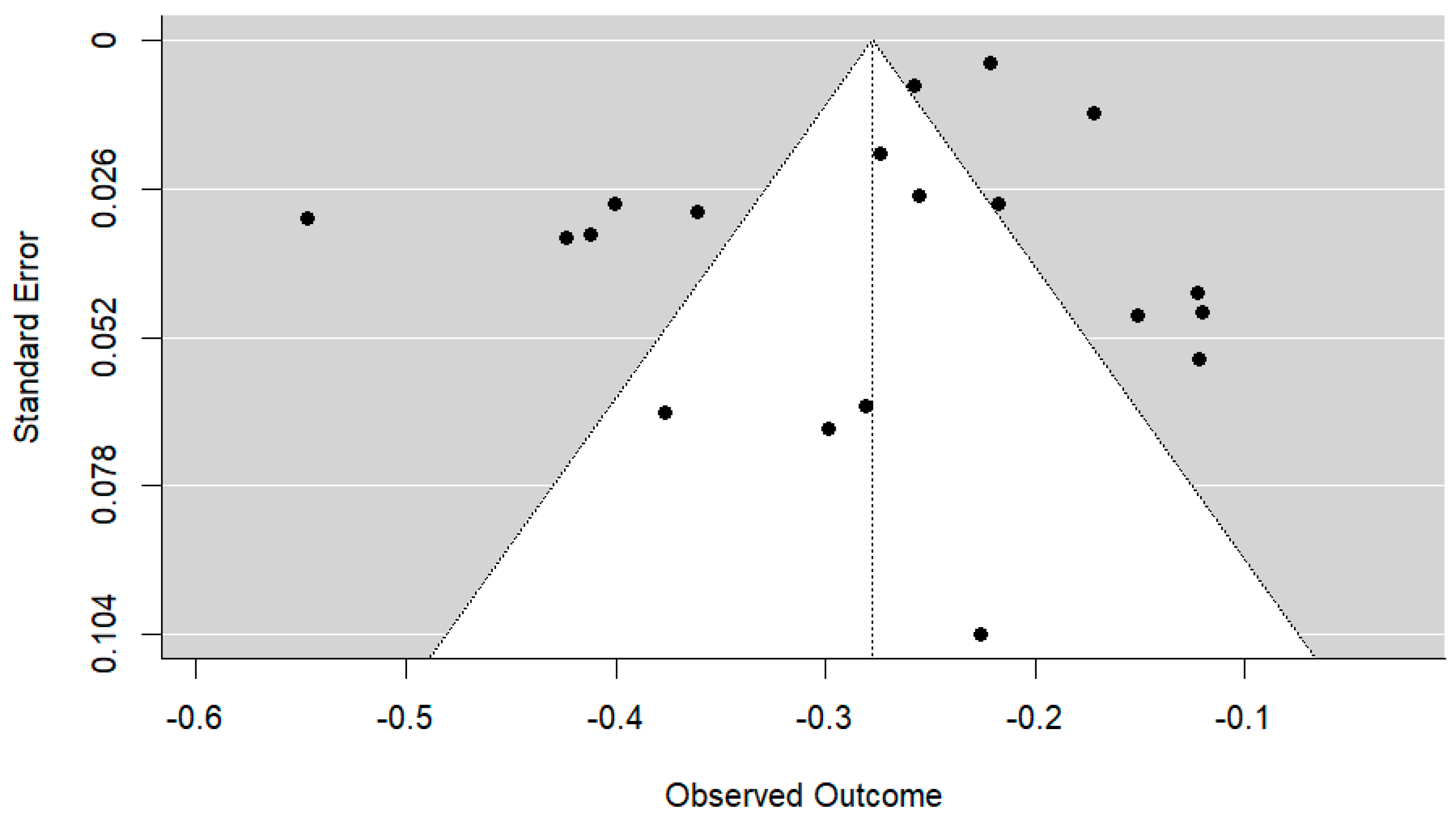
| Risk of bias across studies | 15 | Specify any assessment of risk of bias that may affect the cumulative evidence (e.g., publication bias, selective reporting within studies). | 3 |
| Additional analyses | 16 | Describe methods of additional analyses (e.g., sensitivity or subgroup analyses, meta-regression), if done, indicating which were pre-specified. | 3 |
| RESULTS | |||
| Study selection | 17 | Give numbers of studies screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally with a flow diagram. | 3–4 |
| Study characteristics | 18 | For each study, present characteristics for which data were extracted (e.g., study size, PICOS, follow-up period) and provide the citations. | 4–5 |
| Risk of bias within studies | 19 | Present data on risk of bias of each study and, if available, any outcome level assessment (see item 12). | 4–5 |
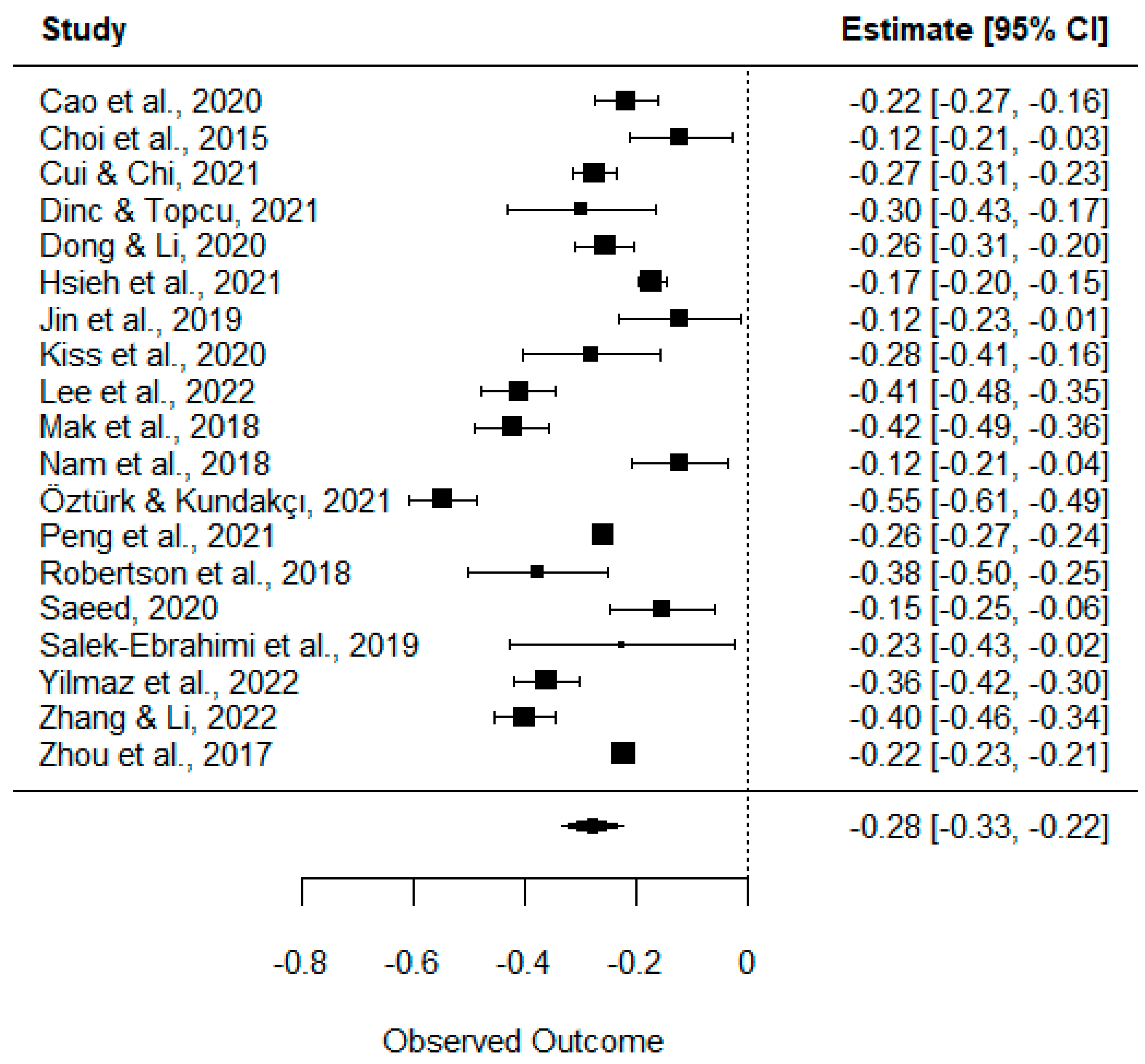
| Results of individual studies | 20 | For all outcomes considered (benefits or harms), present, for each study: (a) simple summary data for each intervention group (b) effect estimates and confidence intervals, ideally with a forest plot. | 5 |
| Synthesis of results | 21 | Present results of each meta-analysis done, including confidence intervals and measures of consistency. | 5–6 |
| Risk of bias across studies | 22 | Present results of any assessment of risk of bias across studies (see Item 15). | 5–6 |
| Additional analysis | 23 | Give results of additional analyses, if done (e.g., sensitivity or subgroup analyses, meta-regression [see Item 16]). | 6–7 |
| DISCUSSION | |||
| Summary of evidence | 24 | Summarize the main findings including the strength of evidence for each main outcome; consider their relevance to key groups (e.g., healthcare providers, users, and policy makers). | 7 |
| Limitations | 25 | Discuss limitations at study and outcome level (e.g., risk of bias), and at review-level (e.g., incomplete retrieval of identified research, reporting bias). | 7 |
| Conclusions | 26 | Provide a general interpretation of the results in the context of other evidence, and implications for future research. | 7–8 |
| FUNDING | |||
| Funding | 27 | Describe sources of funding for the systematic review and other support (e.g., supply of data); role of funders for the systematic review. | N/A |
References
- Miniwatts Marketing Group. Internet World Stats: Usage and Population Statistics. Available online: https://www.intenetworldstats.com/stats.htm (accessed on 25 October 2022).
- Statista Research Department. Global Digital Population as of January 2021. Available online: https://www.statista.com/statistics/617136/digital-population-worldwide/ (accessed on 25 October 2022).
- Brooks, S.; Wang, X.; Schneider, C. Technology Addictions and Technostress: An Examination of the U.S. and China. J. Organ. End User Comput. 2020, 32, 1–19. [Google Scholar] [CrossRef]
- Beard, K.W.; Wolf, E.M. Modification in the Proposed Diagnostic Criteria for Internet Addiction. Cyberpsychol. Behav. 2001, 4, 377–383. [Google Scholar] [CrossRef]
- Young, K.S. Internet Addiction: The Emergence of a New Clinical Disorder. Cyberpsychol. Behav. 1998, 1, 237–244. [Google Scholar] [CrossRef] [Green Version]
- Brand, M.; Young, K.S.; Laier, C.; Wölfling, K.; Potenza, M.N. Integrating Psychological and Neurobiological Considerations Regarding the Development and Maintenance of Specific Internet-Use Disorders: An Interaction of Person-Affect-Cognition-Execution (I-PACE) Model. Neurosci. Biobehav. Rev. 2016, 71, 252–266. [Google Scholar] [CrossRef] [Green Version]
- Kardefelt-Winther, D. Conceptualizing Internet Use Disorders: Addiction or Coping Process?: Conceptualizing Internet Use Disorders. Psychiatry Clin. Neurosci. 2017, 71, 459–466. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spada, M.M. An Overview of Problematic Internet Use. Addict. Behav. 2014, 39, 3–6. [Google Scholar] [CrossRef]
- Starcevic, V.; Aboujaoude, E. Internet Addiction: Reappraisal of an Increasingly Inadequate Concept. CNS Spectr. 2017, 22, 7–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5, 5th ed.; American Psychiatric Association, Ed.; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 9780890425541. [Google Scholar]
- World Health Organization. International Classification of Diseases 11th Revision (ICD-11). Available online: https://icd.who.int/ (accessed on 27 October 2022).
- Li, G.; Hou, G.; Yang, D.; Jian, H.; Wang, W. Relationship between Anxiety, Depression, Sex, Obesity, and Internet Addiction in Chinese Adolescents: A Short-Term Longitudinal Study. Addict. Behav. 2019, 90, 421–427. [Google Scholar] [CrossRef]
- Mo, P.K.; Chan, V.W.; Wang, X.; Lau, J.T. Gender difference in the association between internet addiction, self-esteem and academic aspirations among adolescents: A structural equation modelling. Comput. Educ. 2020, 155, 103921. [Google Scholar] [CrossRef]
- Alimoradi, Z.; Lin, C.-Y.; Broström, A.; Bülow, P.H.; Bajalan, Z.; Griffiths, M.D.; Ohayon, M.M.; Pakpour, A.H. Internet Addiction and Sleep Problems: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2019, 47, 51–61. [Google Scholar] [CrossRef] [Green Version]
- Hidalgo-Fuentes, S. Uso Problemático de Internet y Alexitimia: Un Meta-Análisis. Apunt. Univ. 2022, 12, 162–180. [Google Scholar] [CrossRef]
- Aghasi, M.; Matinfar, A.; Golzarand, M.; Salari-Moghaddam, A.; Ebrahimpour-Koujan, S. Internet Use in Relation to Overweight and Obesity: A Systematic Review and Meta-Analysis of Cross-Sectional Studies. Adv. Nutr. 2020, 11, nmz073. [Google Scholar] [CrossRef] [PubMed]
- Gecaite-Stonciene, J.; Saudargiene, A.; Pranckeviciene, A.; Liaugaudaite, V.; Griskova-Bulanova, I.; Simkute, D.; Naginiene, R.; Dainauskas, L.L.; Ceidaite, G.; Burkauskas, J. Impulsivity Mediates Associations Between Problematic Internet Use, Anxiety, and Depressive Symptoms in Students: A Cross-Sectional COVID-19 Study. Front. Psychiatry 2021, 12, 634464. [Google Scholar] [CrossRef] [PubMed]
- Ramón-Arbués, E.; Granada-López, J.M.; Martínez-Abadía, B.; Echániz-Serrano, E.; Antón-Solanas, I.; Nash, M. Prevalence and Factors Associated with Problematic Internet Use in a Population of Spanish University Students. Int. J. Environ. Res. Public Health 2021, 18, 7620. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Public Health Implications of Excessive Use of the Internet, Computers, Smartphones and Similar Electronic Devices: Meeting Report; Main Meeting Hall, Foundation for Promotion of Cancer Research, National Cancer Research Centre: Tokyo, Japan, 2015; ISBN 9789241509367. [Google Scholar]
- Meng, S.-Q.; Cheng, J.-L.; Li, Y.-Y.; Yang, X.-Q.; Zheng, J.-W.; Chang, X.-W.; Shi, Y.; Chen, Y.; Lu, L.; Sun, Y.; et al. Global Prevalence of Digital Addiction in General Population: A Systematic Review and Meta-Analysis. Clin. Psychol. Rev. 2022, 92, 102128. [Google Scholar] [CrossRef]
- Pan, Y.-C.; Chiu, Y.-C.; Lin, Y.-H. Systematic Review and Meta-Analysis of Epidemiology of Internet Addiction. Neurosci. Biobehav. Rev. 2020, 118, 612–622. [Google Scholar] [CrossRef]
- Fletcher, D.; Sarkar, M. Psychological Resilience: A Review and Critique of Definitions, Concepts, and Theory. Eur. Psychol. 2013, 18, 12–23. [Google Scholar] [CrossRef] [Green Version]
- Ryff, C.D.; Friedman, E.M.; Morozink, J.A.; Tsenkova, V. Psychological Resilience in Adulthood and Later Life: Implications for Health. Annu. Rev. Gerontol. Geriatr. 2012, 32, 73–92. [Google Scholar] [CrossRef]
- Luthar, S.S.; Cicchetti, D.; Becker, B. The Construct of Resilience: A Critical Evaluation and Guidelines for Future Work. Child Dev. 2000, 71, 543–562. [Google Scholar] [CrossRef]
- Hu, T.; Zhang, D.; Wang, J. A Meta-Analysis of the Trait Resilience and Mental Health. Personal. Individ. Differ. 2015, 76, 18–27. [Google Scholar] [CrossRef]
- Oei, T.P.S.; Goh, Z. Interactions Between Risk and Protective Factors on Problem Gambling in Asia. J. Gambl. Stud. 2015, 31, 557–572. [Google Scholar] [CrossRef]
- Tudehope, L.; Lee, P.; Wiseman, N.; Dwirahmadi, F.; Sofija, E. The Effect of Resilience on the Relationship between Perceived Stress and Change in Alcohol Consumption during the COVID-19 Pandemic in Queensland, Australia. J. Health Psychol. 2022, 27, 2696–2713. [Google Scholar] [CrossRef] [PubMed]
- Van Gils, Y.; Dom, G.; Dierckx, E.; Van Alphen, S.P.J.; Franck, E. Resilience, Depression and Anxiety and Hazardous Alcohol Use Behaviour among Community Dwelling Older Adults. Aging Ment. Health 2022, 26, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.; Xia, M.; Han, M.; Liang, Y. Social Support and Resilience as Mediators between Stress and Life Satisfaction among People with Substance Use Disorder in China. Front. Psychiatry 2018, 9, 436. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.; Zhou, Y.; Cao, Q.; Xia, M.; An, J. The relationship between self-control and self-efficacy among patients with substance use disorders: Resilience and self-esteem as mediators. Front. Psychiatry 2019, 10, 388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, P.-C.; Yen, J.-Y.; Lin, H.-C.; Chou, W.-P.; Liu, T.-L.; Ko, C.-H. Coping, Resilience, and Perceived Stress in Individuals with Internet Gaming Disorder in Taiwan. J. Environ. Res. Public Health 2021, 18, 1771. [Google Scholar] [CrossRef]
- Yen, J.-Y.; Lin, H.-C.; Chou, W.-P.; Liu, T.-L.; Ko, C.-H. Associations Among Resilience, Stress, Depression, and Internet Gaming Disorder in Young Adults. J. Environ. Res. Public Health 2019, 16, 3181. [Google Scholar] [CrossRef] [Green Version]
- Dinc, M.; Topcu, F. The Relation between Resilience and Problematic Internet Use among Youth. Dusunen. Adam. 2021, 34, 337–345. [Google Scholar] [CrossRef]
- Öztürk, A.; Kundakçı, N. Perceived Social Support, and Psychological Resilience as Predictors of Internet Addiction: A CrossSectional Study with a Sample of Turkish Undergraduates. Psychiatry Clin. Psychopharmacol. 2021, 31, 449–456. [Google Scholar] [CrossRef]
- Robertson, T.W.; Yan, Z.; Rapoza, K.A. Is Resilience a Protective Factor of Internet Addiction? Comput. Hum. Behav. 2018, 78, 255–260. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Deng, J.; Zhou, F.; Hou, W.; Silver, Z.; Wong, C.Y.; Chang, O.; Huang, E.; Zuo, Q.K. The Prevalence of Depression, Anxiety, and Sleep Disturbances in COVID-19 Patients: A Meta-analysis. Ann. N. Y. Acad. Sci. 2021, 1486, 90–111. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis, 2nd ed.; Wiley & Sons: Hoboken, NJ, USA, 2021; ISBN 9780470057247. [Google Scholar]
- Field, A.P. Meta-Analysis of Correlation Coefficients: A Monte Carlo Comparison of Fixed- and Random-Effects Methods. Psychol. Methods 2001, 6, 161–180. [Google Scholar] [CrossRef]
- Hedges, L.V.; Vevea, J.L. Fixed- and Random-Effects Models in Meta-Analysis. Psychol. Methods 1998, 3, 486–504. [Google Scholar] [CrossRef]
- Schmidt, F.L.; Oh, I.-S.; Hayes, T.L. Fixed- versus Random-Effects Models in Meta-Analysis: Model Properties and an Empirical Comparison of Differences in Results. Br. J. Math. Stat. Psychol. 2009, 62, 97–128. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thompson, S.G. Quantifying Heterogeneity in a Meta-Analysis. Statist. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef]
- Polanin, J.R.; Tanner-Smith, E.E.; Hennessy, E.A. Estimating the Difference Between Published and Unpublished Effect Sizes: A Meta-Review. Rev. Educ. Res. 2016, 86, 207–236. [Google Scholar] [CrossRef]
- Botella-Ausina, J.; Sánchez-Meca, J. Meta-Análisis en Ciencias Sociales y de la Salud, 1st ed.; Síntesis: Madrid, España, 2015; ISBN 9788490771242. [Google Scholar]
- Egger, M.; Smith, G.D.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating Characteristics of a Rank Correlation Test for Publication Bias. Biometrics 1994, 50, 1088. [Google Scholar] [CrossRef]
- Fu, R.; Gartlehner, G.; Grant, M.; Shamliyan, T.; Sedrakyan, A.; Wilt, T.J.; Griffith, L.; Oremus, M.; Raina, P.; Ismaila, A.; et al. Conducting Quantitative Synthesis When Comparing Medical Interventions: AHRQ and the Effective Health Care Program. J. Clin. Epidemiol. 2011, 64, 1187–1197. [Google Scholar] [CrossRef]
- Viechtbauer, W. Conducting Meta-Analyses in R with the Metafor Package. J. Stat. Soft. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Cao, Q.; An, J.; Yang, Y.; Peng, P.; Xu, S.; Xu, X.; Xiang, H. Correlation among Psychological Resilience, Loneliness, and Internet Addiction among Left-behind Children in China: A Cross-Sectional Study. Curr. Psychol. 2020, 41, 4566–4573. [Google Scholar] [CrossRef]
- Choi, S.-W.; Kim, D.-J.; Choi, J.-S.; Ahn, H.; Choi, E.-J.; Song, W.-Y.; Kim, S.; Youn, H. Comparison of Risk and Protective Factors Associated with Smartphone Addiction and Internet Addiction. J. Behav. Addict. 2015, 4, 308–314. [Google Scholar] [CrossRef]
- Cui, X.; Chi, X. The Relationship Between Social Support and Internet Addiction Among Chinese Adolescents during the COVID-19 Pandemic: A Multiple Mediation Model of Resilience and Post-Traumatic Stress Disorder Symptoms. Psychol. Res. Behav. Manag. 2021, 14, 1665–1674. [Google Scholar] [CrossRef]
- Dong, Y.; Li, H. The Relationship between Social Support and Depressive Symptoms among the College Students of Liaoning, China: A Moderated Mediated Analysis. Psychol. Health Med. 2020, 25, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.-P.; Hwa, H.-L.; Shen, A.C.-T.; Wei, H.-S.; Feng, J.-Y.; Huang, C.-Y. Ecological Predictors and Trajectory of Internet Addiction from Childhood through Adolescence: A Nationally Representative Longitudinal Study. J. Environ. Res. Public Health 2021, 18, 6253. [Google Scholar] [CrossRef]
- Jin, S.W.; Jones, T.V.; Lee, Y. Does Resilience Mediate the Link between Depression and Internet Addiction among African American University Students? J. Negro Educ. 2019, 88, 114. [Google Scholar] [CrossRef]
- Kiss, H.; Fitzpatrick, K.M.; Piko, B.F. The Digital Divide: Risk and Protective Factors and the Differences in Problematic Use of Digital Devices among Hungarian Youth. Child. Youth Serv. Rev. 2020, 108, 104612. [Google Scholar] [CrossRef]
- Lee, J.; Won, S.; Chang, S.M.; Kim, B.-S.; Lee, S.J. Prevalence of Addictive Behaviors in Medical Students and Their Association With Stress. Psychiatry Investig. 2022, 19, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Mak, K.K.; Jeong, J.; Lee, H.-K.; Lee, K. Mediating Effect of Internet Addiction on the Association between Resilience and Depression among Korean University Students: A Structural Equation Modeling Approach. Psychiatry Investig. 2018, 15, 962–969. [Google Scholar] [CrossRef]
- Nam, C.; Lee, D.; Lee, J.; Choi, A.; Chung, S.; Kim, D.-J.; Bhang, S.-Y.; Kwon, J.-G.; Kweon, Y.-S.; Choi, J.-S. The Role of Resilience in Internet Addiction among Adolescents between Sexes: A Moderated Mediation Model. J. Clin. Med. 2018, 7, 222. [Google Scholar] [CrossRef] [Green Version]
- Peng, C.; Wang, M.; Cheng, J.; Tan, Y.; Huang, Y.; Rong, F.; Kang, C.; Ding, H.; Wang, Y.; Yu, Y. Mediation of Internet Addiction on Association between Childhood Maltreatment and Suicidal Behaviours among Chinese Adolescents. Epidemiol. Psychiatr. Sci. 2021, 30, e64. [Google Scholar] [CrossRef]
- Saeed, M. The role of loneliness as a predictor of internet addiction with a mediating effect of self esteem and moderating effect of resilience among international students in China. Int. J. Psychosoc. Rehabil. 2020, 24, 4729–4748. [Google Scholar] [CrossRef]
- Salek Ebrahimi, L.; Ahmadi, G.; Masjedi Arani, A.; Mousavi, S.E. Predicting Internet Addiction in Medical Students by General Self-Efficacy, Difficulty in Emotion Regulation, and Resilience. Pract. Clin. Psychol. 2019, 7, 167–174. [Google Scholar] [CrossRef]
- Yilmaz, R.; Karaoglan Yilmaz, F.G. Problematic Internet Use in Adults: The Role of Happiness, Psychological Resilience, Dispositional Hope, and Self-Control and Self-Management. J. Ration.-Emot. Cogn.-Behav. Ther. 2022. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Li, D. Stressful Life Events and Problematic Internet Use in Adolescence: Mediation of Psychological Capital and Moderation of School Level. J. Adolesc. 2022, 94, 718–727. [Google Scholar] [CrossRef]
- Zhou, P.; Zhang, C.; Liu, J.; Wang, Z. The Relationship Between Resilience and Internet Addiction: A Multiple Mediation Model Through Peer Relationship and Depression. Cyberpsychol. Behav. Soc. Netw. 2017, 20, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; L. Erlbaum Associates: New York, NY, USA, 1988; ISBN 9780805802832. [Google Scholar]
- Rumpf, H.-J.; Effertz, T.; Montag, C. The Cost Burden of Problematic Internet Usage. Curr. Opin. Behav. Sci. 2022, 44, 101107. [Google Scholar] [CrossRef]
- Davydov, D.M.; Stewart, R.; Ritchie, K.; Chaudieu, I. Resilience and Mental Health. Clin. Psychol. Rev. 2010, 30, 479–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carli, V.; Durkee, T.; Wasserman, D.; Hadlaczky, G.; Despalins, R.; Kramarz, E.; Wasserman, C.; Sarchiapone, M.; Hoven, C.W.; Brunner, R.; et al. The Association between Pathological Internet Use and Comorbid Psychopathology: A Systematic Review. Psychopathology 2013, 46, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Marciano, L.; Camerini, A.-L.; Schulz, P.J. Neuroticism and Internet Addiction: What Is next? A Systematic Conceptual Review. Personal. Individ. Differ. 2022, 185, 111260. [Google Scholar] [CrossRef]
- Prizant-Passal, S.; Shechner, T.; Aderka, I.M. Social Anxiety and Internet Use—A Meta-Analysis: What Do We Know? What Are We Missing? Comput. Hum. Behav. 2016, 62, 221–229. [Google Scholar] [CrossRef]
- Yadav, P.; Banwari, G.; Parmar, C.; Maniar, R. Internet Addiction and Its Correlates among High School Students: A Preliminary Study from Ahmedabad, India. Asian J. Psychiatry 2013, 6, 500–505. [Google Scholar] [CrossRef] [PubMed]
- Joyce, S.; Shand, F.; Tighe, J.; Laurent, S.J.; Bryant, R.A.; Harvey, S.B. Road to Resilience: A Systematic Review and Meta-Analysis of Resilience Training Programmes and Interventions. BMJ Open 2018, 8, e017858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wisniewski, P.; Jia, H.; Wang, N.; Zheng, S.; Xu, H.; Rosson, M.B.; Carroll, J.M. Resilience mitigates the negative effects of adolescent internet addiction and online risk exposure. In Proceedings of the Conference on Human Factors in Computing Systems, Seoul, Republic of Korea, 18–23 April 2015; pp. 4029–4038. [Google Scholar]



| Study | Country | Continent | Sample | Age | Sex (% Men) | PIU Test | Resilience Test | Risk of Bias | r |
|---|---|---|---|---|---|---|---|---|---|
| Cao et al., 2020 [49] | China | Asia | 1218 | 11.8 | 55.25 | YDQ | CD-RISC 10 | Under | −0.214 |
| Choi et al., 2015 [50] | South Korea | Asia | 448 | 20.89 | 39.7 | IAT | CD-RISC | Under | −0.12 |
| Cui & Chi, 2021 [51] | China | Asia | 2544 | 16.49 | 42.7 | YDQ | CD-RISC 10 | Under | −0.267 |
| Dinc & Topcu, 2021 [33] | Australia | Oceania | 220 | 14.16 | 44.5 | CIUS | CYRM-28 | High | −0.29 |
| Dong & Li, 2020 [52] | China | Asia | 1362 | 53.9 | IAII | CD-RISC 10 | Under | −0.25 | |
| Hsieh et al., 2021 [53] | China | Asia | 6233 | 51 | CIAS | CD-RISC 10 | Under | −0.17 | |
| Jin et al., 2019 [54] | USA | America | 326 | 23.4 | 20.6 | IAT | BRS | Under | −0.121 |
| Kiss et al., 2020 [55] | Hungary | Europe | 249 | 22.5 | 37.8 | PIU-Q | CD-RISC 10 | High | −0.274 |
| Lee et al., 2022 [56] | South Korea | Asia | 866 | 70.8 | IAPS | CD-RISC | High | −0.39 | |
| Mak et al., 2018 [57] | South Korea | Asia | 837 | 22.13 | 43.13 | IAT | CD-RISC | High | −0.4 |
| Nam et al., 2018 [58] | South Korea | Asia | 519 | 51.64 | IAT | CD-RISC | High | −0.122 | |
| Öztürk & Kundakçı, 2021 [34] | Turkey | Europe | 1028 | 20.17 | 39.7 | IAT | BRS | Under | −0.498 |
| Peng et al., 2021 [59] | China | Asia | 16,130 | 15.22 | 51.9 | IAT | RSCA | Under | −0.252 |
| Robertson et al., 2018 [35] | USA | America | 240 | 25.05 | 65 | IAT | CD-RISC | High | −0.36 |
| Saeed, 2020 [60] | China | Asia | 436 | 23.81 | IAT | BRS | High | −0.15 | |
| Salek-Ebrahimi et al., 2019 [61] | Iran | Asia | 96 | 19.73 | 21.1 | IAT | CD-RISC | Under | −0.222 |
| Yilmaz et al., 2022 [62] | Turkey | Europe | 1123 | 46.7 | 58 | YIAT-SF | BRS | Under | −0.346 |
| Zhang & Li, 2022 [63] | China | Asia | 1228 | YDQ | PPQ | High | −0.38 | ||
| Zhou et al., 2017 [64] | China | Asia | 58,756 | 10.83 | 54.5 | YDQ | RRS | High | −0.218 |
| Zr | 95% CI | p | p Subgroup | |
|---|---|---|---|---|
| Risk of individual bias | 0.48 | |||
| High | −0.30 | −0.38, −0.22 | <0.001 | |
| Under | −0.26 | −0.33, −0.18 | <0.001 | |
| Continent | 0.15 | |||
| Asia | −0.25 | −0.32, −0.19 | <0.001 | |
| Other | −0.34 | −0.44, −0.24 | <0.001 | |
| PIU test | 0.90 | |||
| IAT | −0.27 | −0.35, −0.18 | <0.001 | |
| YDQ | −0.28 | −0.40, −0.16 | <0.001 | |
| Other | −0.30 | −0.40, −0.19 | <0.001 | |
| Resilience test | 0.87 | |||
| BRS | −0.30 | −0.43, −0.18 | <0.001 | |
| CD-RISC | −0.28 | −0.39, −0.18 | <0.001 | |
| CD-RISC 10 | −0.24 | −0.35, −0.13 | <0.001 | |
| Other | −0.29 | −0.42, −0.17 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hidalgo-Fuentes, S.; Martí-Vilar, M.; Ruiz-Ordoñez, Y. Problematic Internet Use and Resilience: A Systematic Review and Meta-Analysis. Nurs. Rep. 2023, 13, 337-350. https://doi.org/10.3390/nursrep13010032
Hidalgo-Fuentes S, Martí-Vilar M, Ruiz-Ordoñez Y. Problematic Internet Use and Resilience: A Systematic Review and Meta-Analysis. Nursing Reports. 2023; 13(1):337-350. https://doi.org/10.3390/nursrep13010032
Chicago/Turabian StyleHidalgo-Fuentes, Sergio, Manuel Martí-Vilar, and Yolanda Ruiz-Ordoñez. 2023. "Problematic Internet Use and Resilience: A Systematic Review and Meta-Analysis" Nursing Reports 13, no. 1: 337-350. https://doi.org/10.3390/nursrep13010032
APA StyleHidalgo-Fuentes, S., Martí-Vilar, M., & Ruiz-Ordoñez, Y. (2023). Problematic Internet Use and Resilience: A Systematic Review and Meta-Analysis. Nursing Reports, 13(1), 337-350. https://doi.org/10.3390/nursrep13010032