
Factors Associated with Obstetric Violence Implicated in the Development of Postpartum Depression and Post-Traumatic Stress Disorder: A Systematic Review

 ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Search Strategy of the Studies
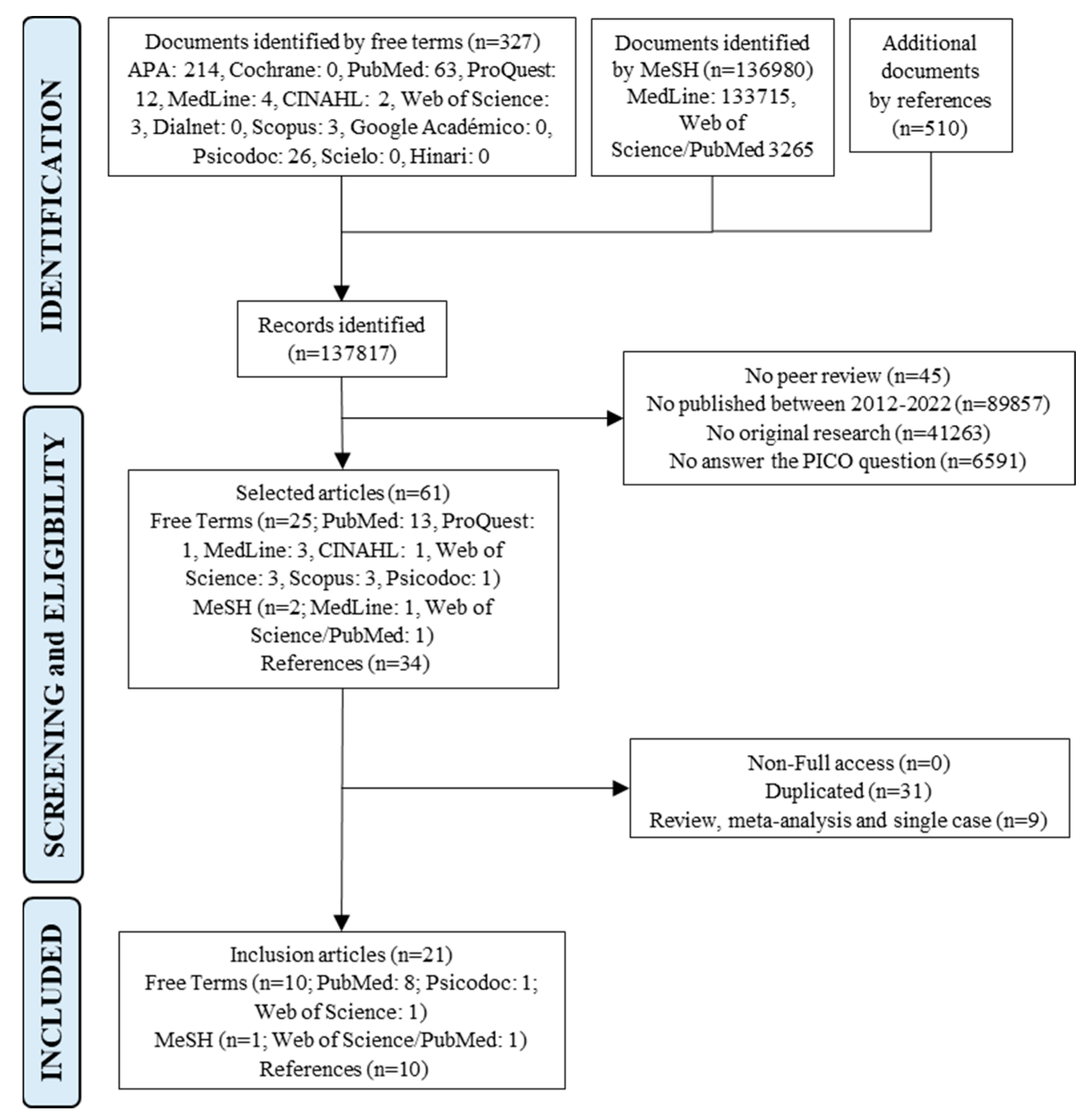
2.3. Selection Process of the Studies
2.4. Data Collection
2.5. Evaluation of the Quality of the Studies
3. Results
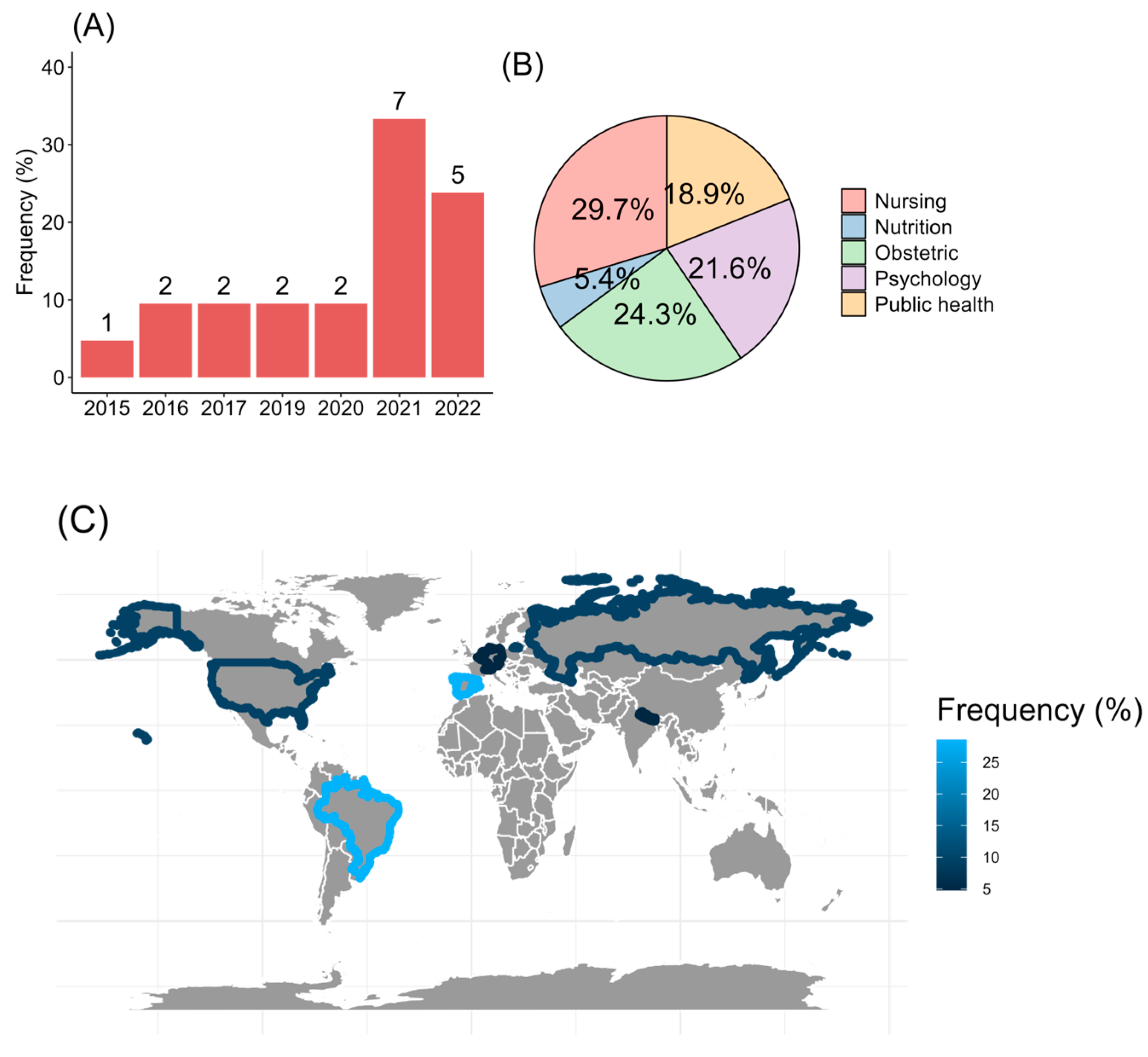
3.1. Demographic Analysis of the Studies
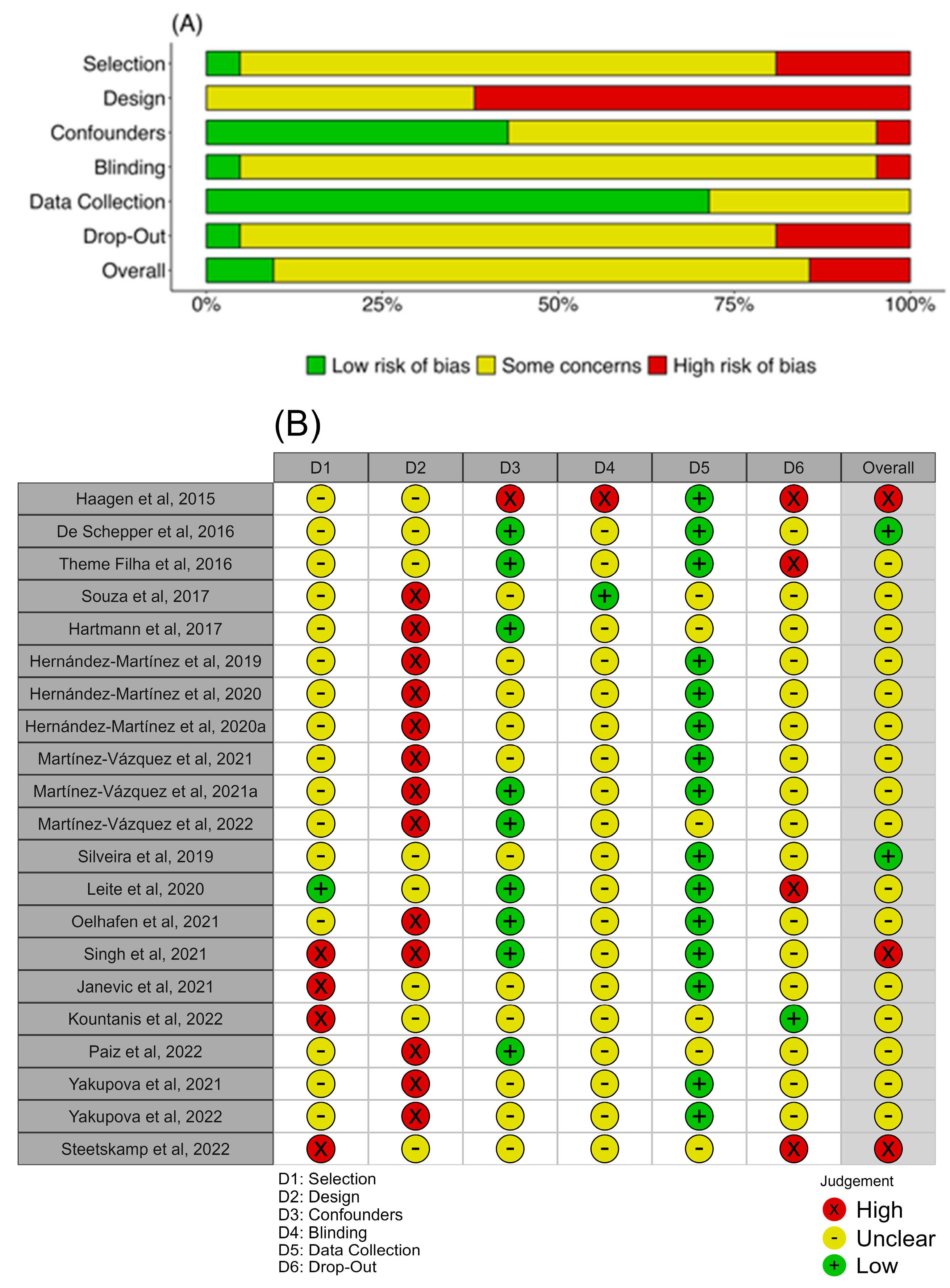
3.2. Quality Analysis of the Studies
3.3. Postpartum Depression and Post-Traumatic Stress Disorder Outcomes
3.4. Obstetric Violence Explored in the Articles
3.5. Factors Associated with Obstetric Violence and Contribution to Develop PPD and PTSD
4. Discussion
4.1. Strengths, Limitations, and Future Perspectives
4.2. Recommendations to Prevent Obstetric Violence or Vulnerability
- To systematically and chronologically review all obstetrical and postpartum protocols;
- To design humanized protocols based on women-centered healthcare models;
- To implement evaluation protocols for PPD and PTSD, at least at 6 months and 1 year postpartum;
- To develop OV scales adjusted by social vulnerability factors;
- To study the modulation of OV by psychosocial factors such as educational level, nationality, or gender violence.
- To train in the gender field;
- To inform the women of each intervention during pregnancy, childbirth, and postpartum;
- To prepare the women for potential change that can happen during childbirth;
- To consider routine screening of PPD and PTSD reflecting maternal age, educational level, economic status, and social support;
- To establish a diagnosis of PPD and PTSD using specific scales with appropriate cut-offs, complemented with clinical and interview observations.
- To express difficulties and emotions and request help if necessary;
- To prioritize management control and autonomy;
- To reinforce social support.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement:
Guidelines and Standards Statement:
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). The Prevention and Elimination of Disrespect and Abuse during Facility-Based Childbirth: WHO Statement. Available online: https://www.who.int/publications/i/item/WHO-RHR-14.23 (accessed on 16 August 2023).
- Corral-Manzano, G.M. El Derecho Penal Como Medio de Prevención de La Violencia Obstétrica En México. Resultados al 2018. MUSAS 2019, 4, 2. [Google Scholar] [CrossRef]
- Mihret, M.S. Obstetric Violence and Its Associated Factors among Postnatal Women in a Specialized Comprehensive Hospital, Amhara Region, Northwest Ethiopia. BMC Res. Notes 2019, 12, 600. [Google Scholar] [CrossRef] [PubMed]
- Jojoa-Tobar, E.; Cuchumbe-Sánchez, Y.D.; Ledesma-Rengifo, J.B.; Muñoz-Mosquera, M.C.; Suarez-Bravo, J.P. Violencia Obstétrica: Haciendo Visible Lo Invisible. Rev. Univ. Ind. Santander Salud 2019, 51, 136–147. [Google Scholar] [CrossRef]
- Castro, R.; Frías, S.M. Obstetric Violence in Mexico: Results From a 2016 National Household Survey. Violence Against Women 2020, 26, 555–572. [Google Scholar] [CrossRef] [PubMed]
- Pereira, C.J.; Domínguez, A.L.; Toro Merlo, J. Violencia Obstétrica Desde La Perspectiva de La Paciente. Rev. Obstet. Ginecol. Venez. 2015, 75, 81–90. [Google Scholar]
- Martínez-Galiano, J.M.; Martinez-Vazquez, S.; Rodríguez-Almagro, J.; Hernández-Martinez, A. The Magnitude of the Problem of Obstetric Violence and Its Associated Factors: A Cross-Sectional Study. Women Birth 2021, 34, e526–e536. [Google Scholar] [CrossRef]
- Fernández Clemente, L.; Olza Fernández, I. Treatment of Postpartum Post-Traumatic Stress Disorder: A Systematic Review. Psicosom. Psiquiatr. 2018, 5, 29–39. [Google Scholar]
- Reshef, S.; Mouadeb, D.; Sela, Y.; Weiniger, F.C.; Freedman, S.A. Childbirth, Trauma and Family Relationships. Eur. J. Psychotraumatol. 2023, 14. [Google Scholar] [CrossRef]
- Shorey, S.; Chee, C.Y.I.; Ng, E.D.; Chan, Y.H.; Tam, W.W.S.; Chong, Y.S. Prevalence and Incidence of Postpartum Depression among Healthy Mothers: A Systematic Review and Meta-Analysis. J. Psychiatr. Res. 2018, 104, 235–248. [Google Scholar] [CrossRef]
- Ortiz Martinez, R.A.; Gallego Betancourt, C.X.; Buitron Zuñiga, E.L.; Meneses Valdés, Y.D.; Muñoz Fernandez, N.F.; Gonzales Barrera, M.A. Prevalencia de Tamiz Positivo Para Depresión Postparto En Un Hospital de Tercer Nivel y Posibles Factores Asociados. Rev. Colomb. Psiquiatr. 2016, 45, 253–261. [Google Scholar] [CrossRef]
- Moya, E.; Mzembe, G.; Mwambinga, M.; Truwah, Z.; Harding, R.; Ataide, R.; Larson, L.M.; Fisher, J.; Braat, S.; Pasricha, S.; et al. Prevalence of Early Postpartum Depression and Associated Risk Factors among Selected Women in Southern Malawi: A Nested Observational Study. BMC Pregnancy Childbirth 2023, 23, 229. [Google Scholar] [CrossRef]
- Brazeau, N.; Reisz, S.; Jacobvitz, D.; George, C. Understanding the Connection between Attachment Trauma and Maternal Self-Efficacy in Depressed Mothers. Infant. Ment. Health J. 2018, 39, 30–43. [Google Scholar] [CrossRef]
- Macedo-Poma, K.; Marquina-Curasma, P.G.; Corrales-Reyes, I.E.; Mejía, C.R. Factors Associated to Depressive Symptoms in Mothers with Children Hospitalized in Pediatric and Neonatology Units of Peru: A Case-Control Study. Medwave 2019, 19, e7649. [Google Scholar] [CrossRef]
- Motrico, E.; Domínguez-Salas, S.; Rodríguez-Domínguez, C.; Gómez-Gómez, I.; Rodríguez-Muñoz, M.F.; Gómez-Baya, D. The Impact of the COVID-19 Pandemic on Perinatal Depression and Anxiety: A Large Cross-Sectional Study in Spain. Psicothema 2022, 34, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Upadhyay, R.P.; Chowdhury, R.; Salehi, A.; Sarkar, K.; Singh, S.K.; Sinha, B.; Pawar, A.; Rajalakshmi, A.K.; Kumar, A. Postpartum Depression in India: A Systematic Review and Meta-Analysis. Bull. World Health Organ. 2017, 95, 706–717C. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Galiano, J.M.; Delgado-Rodríguez, M. The Relegated Goal of Health Institutions: Sexual and Reproductive Health. Int. J. Environ. Res. Public Health 2021, 18, 1767. [Google Scholar] [CrossRef] [PubMed]
- Heyne, C.-S.; Kazmierczak, M.; Souday, R.; Horesh, D.; Lambregtse-van den Berg, M.; Weigl, T.; Horsch, A.; Oosterman, M.; Dikmen-Yildiz, P.; Garthus-Niegel, S. Prevalence and Risk Factors of Birth-Related Posttraumatic Stress among Parents: A Comparative Systematic Review and Meta-Analysis. Clin. Psychol. Rev. 2022, 94, 102157. [Google Scholar] [CrossRef] [PubMed]
- Grekin, R.; O’Hara, M.W. Prevalence and Risk Factors of Postpartum Posttraumatic Stress Disorder: A Meta-Analysis. Clin. Psychol. Rev. 2014, 34, 389–401. [Google Scholar] [CrossRef]
- Rodriguez, D.C.; Ceriani-Cernadas, J.M.; Abarca, P.; Edwards, E.; Barrueco, L.; Lesta, P.; Durán, P. Chronic Post-Traumatic Stress in Mothers of Very Low Birth Weight Preterm Infants Born before 32 Weeks of Gestation. Arch. Argent. Pediatr. 2020, 118, 306–312. [Google Scholar]
- Organización Panamericana de la Salud (PAHO). Salud Mental Perinatal, 1st ed.; Maldonado-Durán, J.M., Ed.; World Health Organization (WHO): Washington, DC, USA, 2011. [Google Scholar]
- Bauer, A.; Garman, E.; Besada, D.; Field, S.; Knapp, M.; Honikman, S. Costs of Common Perinatal Mental Health Problems in South Africa. Glob. Ment. Health 2022, 9, 429–438. [Google Scholar] [CrossRef]
- Huffhines, L.; Coe, J.L.; Busuito, A.; Seifer, R.; Parade, S.H. Understanding Links between Maternal Perinatal Posttraumatic Stress Symptoms and Infant Socioemotional and Physical Health. Infant. Ment. Health J. 2022, 43, 474–492. [Google Scholar] [CrossRef]
- Williams, C.; Patricia Taylor, E.; Schwannauer, M. A Web-Based Survey of Mother-Infant Bond, Attachment Experiences, and Metacognition in Post-Traumatic Stress Following Childbirth. Infant. Ment. Health J. 2016, 37, 259–273. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Batt, M.M.; Duffy, K.A.; Novick, A.M.; Metcalf, C.A.; Epperson, C.N. Is Postpartum Depression Different From Depression Occurring Outside of the Perinatal Period? A Review of the Evidence. Focus 2020, 18, 106–119. [Google Scholar] [CrossRef]
- Loveland Cook, C.A.; Flick, L.H.; Homan, S.M.; Campbell, C.; McSweeney, M.; Gallagher, M.E. Posttraumatic Stress Disorder in Pregnancy: Prevalence, Risk Factors, and Treatment. Obstet. Gynecol. 2004, 103, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Basque Office for Health Technology Assessment Fichas de Lectura Crítica (OSTEBA). Available online: http://www.lecturacritica.com/es/ (accessed on 19 September 2023).
- Díaz-Gutiérrez, M.J.; Martínez-Cengotitabengoa, M.; Sáez de Adana, E.; Cano, A.I.; Martínez-Cengotitabengoa, M.T.; Besga, A.; Segarra, R.; González-Pinto, A. Relationship between the Use of Benzodiazepines and Falls in Older Adults: A Systematic Review. Maturitas 2017, 101, 17–22. [Google Scholar] [CrossRef]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of Study Quality for Systematic Reviews: A Comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological Research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef]
- Deeks, J.; Dinnes, J.; D’Amico, R.; Sowden, A.; Sakarovitch, C.; Song, F.; Petticrew, M.; Altman, D. Evaluating Non-Randomised Intervention Studies. Health Technol. Assess. 2003, 7. [Google Scholar] [CrossRef]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (Robvis): An R Package and Shiny Web App for Visualizing Risk-of-bias Assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Haagen, J.F.G.; Moerbeek, M.; Olde, E.; van der Hart, O.; Kleber, R.J. PTSD after Childbirth: A Predictive Ethological Model for Symptom Development. J. Affect. Disord. 2015, 185, 135–143. [Google Scholar] [CrossRef]
- De Schepper, S.; Vercauteren, T.; Tersago, J.; Jacquemyn, Y.; Raes, F.; Franck, E. Post-Traumatic Stress Disorder after Childbirth and the Influence of Maternity Team Care during Labour and Birth: A Cohort Study. Midwifery 2016, 32, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Martínez, A.; Rodríguez-Almagro, J.; Molina-Alarcón, M.; Infante-Torres, N.; Donate Manzanares, M.; Martínez-Galiano, J.M. Postpartum Post-Traumatic Stress Disorder: Associated Perinatal Factors and Quality of Life. J. Affect. Disord. 2019, 249, 143–150. [Google Scholar] [CrossRef]
- Hernández-Martínez, A.; Rodríguez-Almagro, J.; Molina-Alarcón, M.; Infante-Torres, N.; Rubio-Álvarez, A.; Martínez-Galiano, J.M. Perinatal Factors Related to Post-Traumatic Stress Disorder Symptoms 1–5 Years Following Birth. Women Birth 2020, 33, e129–e135. [Google Scholar] [CrossRef] [PubMed]
- Hernández-Martínez, A.; Martínez-Vazquez, S.; Rodríguez-Almagro, J.; Delgado-Rodríguez, M.; Martínez-Galiano, J. Elaboration and Validation of Two Predictive Models of Postpartum Traumatic Stress Disorder Risk Formed by Variables Related to the Birth Process: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2020, 18, 92. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Vázquez, S.; Rodríguez-Almagro, J.; Hernández-Martínez, A.; Martínez-Galiano, J.M. Factors Associated with Postpartum Post-Traumatic Stress Disorder (PTSD) Following Obstetric Violence: A Cross-Sectional Study. J. Pers. Med. 2021, 11, 338. [Google Scholar] [CrossRef]
- Martínez-Vazquez, S.; Rodríguez-Almagro, J.; Hernández-Martínez, A.; Delgado-Rodríguez, M.; Martínez-Galiano, J.M. Long-Term High Risk of Postpartum Post-Traumatic Stress Disorder (PTSD) and Associated Factors. J. Clin. Med. 2021, 10, 488. [Google Scholar] [CrossRef]
- Kountanis, J.A.; Kirk, R.; Handelzalts, J.E.; Jester, J.M.; Kirk, R.; Muzik, M. The Associations of Subjective Appraisal of Birth Pain and Provider-Patient Communication with Postpartum-Onset PTSD. Arch. Womens Ment. Health 2022, 25, 171–180. [Google Scholar] [CrossRef]
- Steetskamp, J.; Treiber, L.; Roedel, A.; Thimmel, V.; Hasenburg, A.; Skala, C. Post-Traumatic Stress Disorder Following Childbirth: Prevalence and Associated Factors—A Prospective Cohort Study. Arch. Gynecol. Obstet. 2022, 306, 1531–1537. [Google Scholar] [CrossRef]
- Yakupova, V.; Suarez, A. Postpartum PTSD and Birth Experience in Russian-Speaking Women. Midwifery 2022, 112, 103385. [Google Scholar] [CrossRef]
- Theme Filha, M.M.; Ayers, S.; da Gama, S.G.N.; Leal, M.D.C. Factors Associated with Postpartum Depressive Symptomatology in Brazil: The Birth in Brazil National Research Study, 2011/2012. J. Affect. Disord. 2016, 194, 159–167. [Google Scholar] [CrossRef]
- De Souza, K.J.; Rattner, D.; Gubert, M.B. Institutional Violence and Quality of Service in Obstetrics Are Associated with Postpartum Depression. Rev. Saúde Pública 2017, 51, 6549. [Google Scholar] [CrossRef]
- Hartmann, J.M.; Mendoza-Sassi, R.A.; Cesar, J.A. Depressão Entre Puérperas: Prevalência e Fatores Associados. Cad. Saude Publica 2017, 33, e00094016. [Google Scholar] [CrossRef] [PubMed]
- Silveira, M.F.; Mesenburg, M.A.; Bertoldi, A.D.; De Mola, C.L.; Bassani, D.G.; Domingues, M.R.; Stein, A.; Coll, C.V.N. The Association between Disrespect and Abuse of Women during Childbirth and Postpartum Depression: Findings from the 2015 Pelotas Birth Cohort Study. J. Affect. Disord. 2019, 256, 441–447. [Google Scholar] [CrossRef]
- Leite, T.H.; Pereira, A.P.E.; Leal, M.d.C.; da Silva, A.A.M. Disrespect and Abuse towards Women during Childbirth and Postpartum Depression: Findings from Birth in Brazil Study. J. Affect. Disord. 2020, 273, 391–401. [Google Scholar] [CrossRef] [PubMed]
- Oelhafen, S.; Trachsel, M.; Monteverde, S.; Raio, L.; Cignacco, E. Informal Coercion during Childbirth: Risk Factors and Prevalence Estimates from a Nationwide Survey of Women in Switzerland. BMC Pregnancy Childbirth 2021, 21, 369. [Google Scholar] [CrossRef]
- Singh, D.R.; Sunuwar, D.R.; Adhikari, S.; Singh, S.; Karki, K. Determining Factors for the Prevalence of Depressive Symptoms among Postpartum Mothers in Lowland Region in Southern Nepal. PLoS ONE 2021, 16, e0245199. [Google Scholar] [CrossRef] [PubMed]
- Paiz, J.C.; de Jezus Castro, S.M.; Giugliani, E.R.J.; dos Santos Ahne, S.M.; Aqua, C.B.D.; Giugliani, C. Association between Mistreatment of Women during Childbirth and Symptoms Suggestive of Postpartum Depression. BMC Pregnancy Childbirth 2022, 22, 664. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Vázquez, S.; Hernández-Martínez, A.; Rodríguez-Almagro, J.; Delgado-Rodríguez, M.; Martínez-Galiano, J.M. Relationship between Perceived Obstetric Violence and the Risk of Postpartum Depression: An Observational Study. Midwifery 2022, 108, 103297. [Google Scholar] [CrossRef]
- Yakupova, V.; Suarez, A.; Kharchenko, A. Birth Experience, Postpartum PTSD and Depression before and during the Pandemic of COVID-19 in Russia. Int. J. Environ. Res. Public Health 2021, 19, 335. [Google Scholar] [CrossRef]
- Janevic, T.; Maru, S.; Nowlin, S.; McCarthy, K.; Bergink, V.; Stone, J.; Dias, J.; Wu, S.; Howell, E.A. Pandemic Birthing: Childbirth Satisfaction, Perceived Health Care Bias, and Postpartum Health During the COVID-19 Pandemic. Matern. Child. Health J. 2021, 25, 860–869. [Google Scholar] [CrossRef]
- World Health Organization. Women and Health: Today’s Evidence Tomorrow’s Agenda, 1st ed.; World Health Organization (WHO): Geneva, Switzerland, 2009. [Google Scholar]
- World Health Organization WHO. Recommendations on Antenatal Care for a Positive Pregnancy Experience. Available online: https://www.who.int/publications/i/item/9789241549912 (accessed on 16 August 2023).
- Álvarez-Villaseñor, A. Percepción Del Parto Humanizado En Pacientes En Periodo de Puerperio. Rev. Med. Inst. Mex. Seguro Soc. 2021, 58, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, L.B.E.; Jonas, E.; Amaral, L.R.O.G.d. Violência Obstétrica Em Maternidades Públicas Do Estado Do Tocantins. Rev. Estud. Fem. 2018, 26, 143278. [Google Scholar] [CrossRef]
- Santarelli, N. Discursos Médicos Disciplinadores y Experiencias Emocionales de Aborto Farmacológico de Mujeres En Cuyo, Argentina. MUSAS 2019, 4, 78–99. [Google Scholar] [CrossRef]
- Brigidi, S.; Busquets-Gallego, M. Interseccionalidades de Género y Violencias Obstétricas. MUSAS 2019, 4, 37–52. [Google Scholar] [CrossRef]
- Sadler, M.; Santos, M.J.; Ruiz-Berdún, D.; Rojas, G.L.; Skoko, E.; Gillen, P.; Clausen, J.A. Moving beyond Disrespect and Abuse: Addressing the Structural Dimensions of Obstetric Violence. Reprod. Health Matters 2016, 24, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Paravic-Klijn, T.; Burgos-Moreno, M. Prevalencia de Violencia Física, Abuso Verbal y Factores Asociados En Trabajadores/as de Servicios de Emergencia En Establecimientos de Salud Públicos y Privados. Rev. Med. Chil. 2018, 146, 727–736. [Google Scholar] [CrossRef]
- Jardim, D.M.B.; Modena, C.M. Obstetric Violence in the Daily Routine of Care and Its Characteristics. Rev. Lat. Am. Enferm. 2018, 26, e3069. [Google Scholar] [CrossRef]
- Yildiz, P.D.; Ayers, S.; Phillips, L. The Prevalence of Posttraumatic Stress Disorder in Pregnancy and after Birth: A Systematic Review and Meta-Analysis. J. Affect. Disord. 2017, 208, 634–645. [Google Scholar] [CrossRef]
- Ramiro-Cortijo, D.; de la Calle, M.; Gila-Díaz, A.; Moreno-Jiménez, B.; Martin-Cabrejas, M.A.; Arribas, S.M.; Garrosa, E. Maternal Resources, Pregnancy Concerns, and Biological Factors Associated to Birth Weight and Psychological Health. J. Clin. Med. 2021, 10, 695. [Google Scholar] [CrossRef]
- Camuñas, N.; Mavrou, E.; Miguel Tobal, J.J. Ansiedad y Tristeza-Depresión: Una Aproximación Desde La Teoría de La Indefensión-Desesperanza. Rev. Psicopatología Psicol. Clínica 2019, 24, 23003. [Google Scholar] [CrossRef]
- Schroll, A.-M.; Kjærgaard, H.; Midtgaard, J. Encountering Abuse in Health Care; Lifetime Experiences in Postnatal Women—A Qualitative Study. BMC Pregnancy Childbirth 2013, 13, 74. [Google Scholar] [CrossRef] [PubMed]
- Sandoz, V.; Hingray, C.; Stuijfzand, S.; Lacroix, A.; El Hage, W.; Horsch, A. Measurement and Conceptualization of Maternal PTSD Following Childbirth: Psychometric Properties of the City Birth Trauma Scale—French Version (City BiTS-F). Psychol. Trauma. 2022, 14, 696–704. [Google Scholar] [CrossRef]
- Downe, S.; Finlayson, K.; Oladapo, O.; Bonet, M.; Gülmezoglu, A.M. What Matters to Women during Childbirth: A Systematic Qualitative Review. PLoS ONE 2018, 13, e0194906. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013; ISBN 0-89042-555-8. [Google Scholar]
- Barthel, D.; Göbel, A.; Barkmann, C.; Helle, N.; Bindt, C. Does Birth-Related Trauma Last? Prevalence and Risk Factors for Posttraumatic Stress in Mothers and Fathers of VLBW Preterm and Term Born Children 5 Years After Birth. Front. Psychiatry 2020, 11, 575429. [Google Scholar] [CrossRef] [PubMed]
- Brum, E.H.M. de Depressão Pós-Parto: Discutindo o Critério Temporal Do Diagnóstico. Cad. Pós-Grad. Distúrbios Desenvolv. 2017, 17, 92–100. [Google Scholar] [CrossRef]
- Holm, D.-M.L.; Wohlfahrt, J.; Rasmussen, M.-L.H.; Corn, G.; Melbye, M. A Quantitative Comparison of Two Measures of Postpartum Depression. BMC Psychiatry 2022, 22, 202. [Google Scholar] [CrossRef]
- Macías-Cortés, E.d.C.; Lima-Gómez, V.; Asbun-Bojalil, J. Exactitud Diagnóstica de La Escala de Depresión Posnatal de Edimburgo: Consecuencias Del Tamizaje En Mujeres Mexicanas. Gac. Med. Mex. 2020, 156. [Google Scholar] [CrossRef]
- Hernández-Martínez, A.; Martínez-Vázquez, S.; Rodríguez-Almagro, J.; Khan, K.S.; Delgado-Rodríguez, M.; Martínez-Galiano, J.M. Validation of Perinatal Post-Traumatic Stress Disorder Questionnaire for Spanish Women during the Postpartum Period. Sci. Rep. 2021, 11, 5567. [Google Scholar] [CrossRef]
- Komurcu Akik, B. Perinatal Post Traumatic Stress Disorder Questionnaire-II (PPQ-II): Adaptation, Validity, and Reliability Study. Dusunen Adam:J. Psychiatry Neurol. Sci. 2020, 33, 340–350. [Google Scholar] [CrossRef]
- Ayers, S.; Wright, D.B.; Thornton, A. Development of a Measure of Postpartum PTSD: The City Birth Trauma Scale. Front. Psychiatry 2018, 9, 409. [Google Scholar] [CrossRef]
- Fameli, A.; Costa, D.S.J.; Coddington, R.; Hawes, D.J. Assessment of Childbirth-Related Post Traumatic Stress Disorder in Australian Mothers: Psychometric Properties of the City Birth Trauma Scale. J. Affect. Disord. 2023, 324, 559–565. [Google Scholar] [CrossRef]
- González-de la Torre, H.; González-Artero, P.N.; Muñoz de León-Ortega, D.; Lancha-de la Cruz, M.R.; Verdú-Soriano, J. Cultural Adaptation, Validation and Evaluation of the Psychometric Properties of an Obstetric Violence Scale in the Spanish Context. Nurs. Rep. 2023, 13, 1368–1387. [Google Scholar] [CrossRef] [PubMed]
- Limmer, C.M.; Stoll, K.; Vedam, S.; Leinweber, J.; Gross, M.M. Measuring Disrespect and Abuse during Childbirth in a High-Resource Country: Development and Validation of a German Self-Report Tool. Midwifery 2023, 126, 103809. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.; Jerez, C.; Klein, K.; Correa, M.; Belizán, J.; Cormick, G. Obstetric Violence: A Latin American Legal Response to Mistreatment during Childbirth. BJOG 2018, 125, 1208–1211. [Google Scholar] [CrossRef]
- Sudhinaraset, M.; Giessler, K.; Nakphong, M.K.; Roy, K.P.; Sahu, A.B.; Sharma, K.; Montagu, D.; Green, C. Can Changes to Improve Person-Centred Maternity Care Be Spread across Public Health Facilities in Uttar Pradesh, India? Sex. Reprod. Health Matters 2021, 29, 394–408. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Document | Method | Sample | Period | Tool | Criteria | Definition of OV | Measurements of OV |
|---|---|---|---|---|---|---|---|
| Theme Filha et al., 2016 [43] | Longitudinal | 23,894 * 11,925 ** | 6 h after birth, 45 days to 6 months postpartum, and 6 to 18 months postpartum | AdHoc-SC AdHoc-OV EPDS CH | EPDS ≥ 13 | Not established | INT-PD ACT-PH PER-SC |
| De Souza et al., 2017 [44] | Cross-sectional | 432 | 0–3 months postpartum | AdHoc-SC AdHoc-OV EPDS-6 | EPDS-6 ≥ 6 | Institutional violence in birth due to failure to act or omission in healthcare | INT-PD ACT-PH |
| Hartmann et al., 2017 [45] | Cross-sectional | 2.687 | 48 h postpartum | AdHoc-SC AdHoc-Ps EPDS | EPDS ≥ 10 | Not established | PER-SC |
| Silveira et al., 2019 [46] | Longitudinal | 4275 * 3065 ** | Between 16 and 22 weeks of gestation. 3 months postpartum | AdHoc-SC AdHoc-OV EPDS | EPDS antenatal ≥ 10; EPDS postpartum ≥ 13 | Human rights violations during childbirth associated with interactions between patient and provider of healthcare and expressed as verbal, physical, sexual abuse, discrimination, or neglect | ACT-PH |
| Leite et al., 2020 [47] | Longitudinal | 23,378 | 24 h postpartum, between 43 days and 6 months postpartum, and between 6 and 12 months postpartum | AdHoc-SC AdHoc-VC EPDS CH | EPDS ≥ 13 | Institutional violence against women during labor and birth. Physical, sexual, or verbal violence, stigmatization and discrimination, failure to meet standards of care | ACT-PH |
| Oelhafen et al., 2021 [48] | Cross-sectional | 6054 | 0–12 months postpartum | AdHoc-OV SIL WQ | WQ = NI | Loss of autonomy due to coercion to accept obstetric interventions. Verbal violence during healthcare | ACT-PH |
| Singh et al., 2021 [49] | Cross-sectional | 415 | 10 weeks postpartum | AdHoc-SC EPDS 11-IS | EPDS ≥ 10 | Not established | ACT-PH PER-SC |
| Janevic et al., 2021 [53] | Cross-sectional | 237 | 0–2 months postpartum | AdHoc-SC BSS-R DMS PHQ-2 C-DSM-V | PHQ-2 ≥ 3 | Not established | ACT-PH PER-SC |
| Paiz et al., 2022 [50] | Cross-sectional | 287 | 31–37 days postpartum | AdHoc-SC AdHoc-OV EPDS | EPDS ≥ 8 | Mistreatment, disrespect, and abuse during childbirth. Gender violence by physical and psychological abuse, discrimination, neglect, lack of privacy, unconsented procedures, and poor information | ACT-PH PER-SC |
| Yakupova et al., 2021 [52] | Cross-sectional | 611 | 14 months postpartum | AdHoc-SC AdHoc-OV EPDS CBTS | EPDS ≥ 10 | Not established | INT-PD ACT-PH |
| Martínez-Vázquez et al., 2022 [51] | Cross-sectional | 782 | 0–12 months postpartum | AdHoc-SC AdHoc-VC AdHoc-OV EPDS | EPDS ≥ 10 | Violation of physical, verbal, or psycho-affective through disrespectful treatment, medical coercion, and specific clinical practices | INT-PD ACT-PH |
| Document | Method | Sample | Period | Tool | Criteria | Definition of OV | Measurements of OV |
|---|---|---|---|---|---|---|---|
| Haagen et al., 2015 [33] | Longitudinal | 385 * 284 ** | Pregnancy, first week postpartum, 3 months postpartum, and 10 months postpartum | AdHoc-SC AdHoc-OV PSS-SR SF-MB | PSS-SR ≥ 18 | Not established | INT-PD ACT-PH |
| De Schepper et al., 2016 [44] | Longitudinal | 340 * 229 ** | 1 and 6 weeks postpartum | AdHoc-SC AdHoc-VC IES-R TES | IES-R ≥ 24 | Not established | INT-PD ACT-PH |
| Hernández-Martínez et al., 2019 [35] | Cross-sectional | 2.990 | 4 and 6 months postpartum | AdHoc-SC AdHoc-VC PPQ | PPQ ≥ 19 | Not established | INT-PD ACT-PH |
| Hernández-Martínez et al., 2020 [36] | Cross-sectional | 1531 | 1 to 5 years postpartum | AdHoc-SC AdHoc-VC PPQ | PPQ ≥ 19 | Not established | INT-PD ACT-PH |
| Hernández-Martínez et al., 2020a [37] | Cross-sectional | 1752 derivation cohort 875 validation cohort | NI | PPQ CH | PPQ = NI | Not established | INT-PD ACT-PH |
| Martínez-Vázquez et al., 2021 [38] | Cross-sectional | 899 | 0 to 12 months postpartum | AdHoc-SC AdHoc-VC AdHoc-OV PPQ | PPQ ≥ 19 | Inadequate healthcare or treatment. Break of autonomy | INT-PD ACT-PH |
| Martínez-Vázquez et al., 2021a [39] | Cross-sectional | 1.301 | 12 to 36 months postpartum | AdHoc-SC AdHoc-VC AdHoc-OV PPQ | PPQ ≥ 19 | Verbal, physical, and psycho-affective abuse during care at delivery | INT-PD ACT-P |
| Janevic et al., 2021 [53] | Cross-sectional | 237 | 0 to 2 months postpartum | AdHoc-SC BSS-R DMS PHQ-2 C-DSM-V | C-DSM-V at least one criterion | Not established | ACT-PH PER-SC |
| Kountanis et al., 2022 [40] | Longitudinal | 112 | 6 weeks postpartum, 3 months postpartum, 6 months postpartum, and 1 year postpartum | AdHoc-SC AdHoc-OV PPQ CH | PPQ ≥ 13 | Not established | PER-SC |
| Yakupova et al., 2021 [52] | Cross-sectional | 611 | 14 months postpartum | AdHoc-SC AdHoc-OV EPDS CBTS | CBTS = NI | Not established | INT-PD ACT-PH |
| Steetskamp et al., 2022 [41] | Longitudinal | 589 * 278 ** | 1 day postpartum and 6 months postpartum | AdHoc-SC AdHoc-VC IES-R | IES-R ≥ 0 | Unsatisfied expectations during delivery and non-adaptation to reactions of the obstetric teams in complications during delivery | INT-PD ACT-PH |
| Yakupova et al., 2022 [42] | Cross-sectional | 611 | 0 to 6 months postpartum | AdHoc-SC AdHoc-OV CBTS | CBTS = NI | Not established | INT-PD ACT-PH |
| Document | Prevalence of PPD | Prevalence of Different Forms of OV | Factors Associated with OV Contributing to PPD Development |
|---|---|---|---|
| Theme Filha et al., 2016 [43] | 26.3% after 6 h postpartum, 25.7% at 45 days to 6 months postpartum, and 27.1% at between 6 and 18 months postpartum | Not social support during labor and birth = 24.4%. Not painful labor analgesia = 20.8%. Self-rated bad or very bad care during birth = 2.4%. Self-rated bad or very bad care of the newborn = 1.7%. | Risk factors associated: Not allowed social support during labor (aOR: 1.18 [0.91; 1.54]), allow partner for a short time (aOR: 1.24 [0.98; 1.56]). Poor self-rated care during birth (OR: 2.02 [1.28; 3.20]) and poor self-rated newborn (OR: 2.16 [1.51; 3.10]). |
| De Souza et al., 2017 [44] | 18.4% | Physical violence = 59.0%. Violence by negligence = 51.8%. Verbal violence = 50.3%. Violence from the institution = 26.1%. Violence from the health system = 19.6%. | Risk factors associated: Physical violence (aOR: 5.83 [4.95; 6.87]). Violence by negligence (aOR: 7.66 [6.37; 9.23]). Verbal violence (aOR: 5.93 [5.14; 6.87]). The physical violence was the main risk factor, being modified by women’s age. Protective factors associated: The social support during labor (OR: 0.39 [0.30; 0.34]). The age modified the effect of negligence (aOR: 0.10 [0.03; 0.15]). |
| Hartmann et al., 2017 [45] | 14% | Low support from health team = 10.2%. Poor monitoring for healthcare staff = 2.3%. | Protective factors associated: The support from health team during birth (OR: 0.77 [0.61; 0.96]) and professional monitoring during hospitalization (partial = OR: 0.90 [0.57; 1.43]; continuous = OR: 0.47 [0.29; 0.74]). |
| Silveira et al., 2019 [46] | 30% with depressive symptoms during pregnancy (EPDS ≥ 10). 9.4% with moderate postpartum depression (EPDS ≥ 13). 5.7% with severe postpartum depression (EPDS ≥ 15). | Any disrespect and abuse during childbirth = 18.0%. Verbal abuse = 9.0% Physical mistreatment = 5.0%, Denial of care = 6.0%. Undesirable procedures = 6.0%. | Risk factors associated: The verbal abuse was for moderate PPD (aOR: 1.58 [1.06; 2.33]), 1 type of abuse to severe PPD (aOR: 1.56 [1.07; 2.27]), being higher for physical abuse (aOR: 2.26 [1.26; 4.08]). The verbal abuse to severe PPD (aOR: 1.69 [1.06; 2.70]). Experience 3 or more types of disrespect with moderate PPD (aOR: 2.90 [1.30; 6.48]) and with severe PPD (aOR: 3.86 [1.58; 9.42]). |
| Leite et al., 2020 [47] | 26.3% In women with vaginal birth, being in the public sector 27.0% and in the private sector 16.0%. 23.8% of women with C-section, in the private sector, 16.0%, and in the public sector, 28.7%. | Vaginal: in the public sector = 30.3% vs. in the private sector = 45.2%. C-section: in the public sector = 36.2% vs. in the private sector = 25.3%. | Risk factors associated: The disrespect was the major factor in the public (vaginal: β = 0.22; C-section: β = 0.26) and private health systems (vaginal: β = 0.25; C-section: β = 0.219). In women with vaginal labor, pressure during labor (β = 0.13) was associated with disrespect. In women with C-section, disrespect was associated with maternal hospitalization (β = 0.153) and perform a C-section when the desire was vaginal birth (β = 0.125). In the private sector, disrespect was associated with does not follow the women’s desire for birth (vaginal: β = 0.448; C-section: β = 0.144). Protective factors associated: The social support (β = −0.228) and good practices (β = −0.104). The disrespect and abuse were lower when the women were accompanied (β = −0.143). |
| Oelhafen et al., 2021 [48] | 27% | Informal coercion (intimidation or manipulation) = 26.7% Pressured to consent (inadequate information, insufficient time to make a decision, and disrespect at the opposition) = 16.3%. Misinformation of the professional healthcare provider = 9.5%. | Risk factors associated: Experiencing informal coercion (RR: 1.35 [1.19; 1.54]). Women had risk of informal coercion in urban areas (RR: 1.16 [1.09; 1.23]), preferred to have autonomy in decisions (RR: 1.15 [1.10; 1.21]), high-risk pregnancy (RR: 1.25 [1.10; 1.41]), not give birth where they had initially planned (RR: 1.47 [1.25; 1.73]). |
| Singh et al., 2021 [49] | 33.7% | Disrespect treatment = 54.9%. not explanation about treatment = 40.9%. Dissatisfied with the newborn care = 46.2%. | Risk factors associated: The dissatisfaction with newborn care (OR: 2.91 [1.91; 4.44]). |
| Janevic et al., 2021 [53] | 13 women with 69.2% satisfaction and 35.7% with at least one discriminatory event in medical care during childbirth. | Women who delivered vaginally: Low birth satisfaction = 41.4%. At least 1 discriminatory event in medical care during childbirth = 15.0%. Women who delivered by C-section: Low birth satisfaction = 73.1% At least 1 discriminatory event in medical care during childbirth = 40.4%. | Protective factors associated: The birth satisfaction (aOR 0.1 [0.03; 0.70]). |
| Paiz et al., 2022 [50] | 28.6% | Not feeling comfortable asking questions = 15.1%. Not understanding received information = 12.5%. Not allowing newborn skin-to-skin contact = 32.0%. Not feeling welcome in the birth unit = 21.7%. Not feeling safe in the birth unit = 25.9%. Lack of privacy during birth = 16.1%. | Risk factors associated: Mistreatment during the birth (RR: 1.58 [1.09; 2.29]). |
| Yakupova et al., 2021 [52] | 45.7% | At least 1 case of obstetric violence = 22.6%. Verbal aggression = 11.3%. Medical interventions without consent = 6.2%. Threats and accusations = 4.4%. Pain relief denial = 3.1%. Use of Kristeller technique = 3.1%. Ignoring the needs of the woman = 2.9%. Not social support = 42.1%. Amniotomy = 45.7%. | Risk factors associated: Experienced obstetric violence (β = 2.08 [1.39; 2.78]). |
| Martinez-Vázquez et al., 2022 [51] | 25.4% | Verbal violence = 24.4%. Physical violence = 53.5%. Psycho-affective violence = 35.2%. Induction of labor = 40.2%. Instrumental birth = 19.4%. Emergency C-section = 14.2%. Several perineal tear = 3.3%. Not allowing newborn skin-to-skin contact = 20.7%. Not partner support during childbirth = 1.9%. | Risk factors associated: Verbal violence (aOR: 2.02 [1.35; 3.02]), and psycho-affective violence (aOR: 2.65 [1.79; 3.93]). |
| Document | Prevalence of PTSD | Prevalence of Different Forms of OV | Factors Associated with OV Contributing to PTSD Development |
|---|---|---|---|
| Haagen et al., 2015 [33] | 0.57% at 3 months postpartum and 0.35% at 10 months postpartum | Vaginal labor = 12.1%. Vacuum extraction = 8.1%. | Risk factors associated: Poor perinatal information by staff (β = 0.16) and mode of delivery (β = 0.15). The indirect effect of negative emotion was somatic (β = 0.14) and psychological dissociation (β = 0.041). |
| De Schepper et al., 2016 [34] | 0.3% (TES) y 5.7% (IES-R) at first week postpartum. 0% (TES) and 4% (IES-R) at 6 weeks postpartum | Unplanned C-section = 39.0%. Induction of labor = 33.0%. Episiotomy = 41.4%. Instrumental delivery = 10.9%. | Protective factors associated: In the first week postpartum, the women´s locus of control during the birth (β = −0.274). At 6 weeks postpartum, the perception of women about the midwife having control during labor and birth (β = −0.25) and the possibility of asking questions during labor (β = −0.153). Women with spontaneous labor had 88% reduction in developing PTSD. |
| Hernández- Martínez et al., 2019 [35] | 10.6% | Unfollow the birth plan = 79.4%. Kristeller technique = 30.8%. Episiotomy = 36.4%. Perineal tears = 4.2%. Not allowing newborn skin-to-skin contact = 32.4%. Not using analgesia = 22.5%. Not using anesthesia = 96.3%. | Risk factors associated: Instrumental delivery (aOR: 2.50 [1.70; 3.69]), C-section (aOR: 3.79 [2.43; 5.92]), Kristeller technique, (aOR: 1.48 [1.12; 1.97]), perineal tears (aOR: 2.77 [1.71; 4.49]), and use anesthesia (aOR: 1.92 [1.21; 3.05]). Protective factors associated: Respected birth plan (aOR: 0.52 [0.34; 0.80]), using epidural analgesia (aOR: 0.64 [0.44; 0.92]) and skin-to-skin contact (aOR: 0.37 [0.28; 0.50]). |
| Hernández-Martínez et al., 2020 [36] | 7.2% in women between 1 and 3 years postpartum. 8.1% in women between 4 and 5 years postpartum 5.9%. | Unfollow the birth plan = 18.9%. Induced birth = 32.9%. Fundal pressure = 31.0%. Instrumental delivery = 17.7%. C-section = 24.9%. Episiotomy = 40.0%. Perineal tears = 4.4%. Not allowing newborn skin-to-skin contact = 35.5%. Not using analgesia = 22.9%. Not using anesthesia = 96.4%. | Risk factors associated: Instrumental delivery (aOR: 3.32 [1.73; 3.39]), C-section (aOR: 4.80 [2.51; 9.15]), fundal pressure (aOR: 1.72 [1.08; 2.74]) and perineal tears (aOR: 2.73 [1.27; 5.86]). Protective factors associated: Respected birth plan (aOR: 0.44 [0.19; 0.99]), use of epidural (aOR: 0.44 [0.24; 0.80]), and skin-to-skin contact at birth (aOR: 0.33 [0.20; 0.55]). |
| Hernández-Martínez et al., 2020a [37] | 14.2% | Labor induction = 40.6%. Instrumental delivery = 18.6%. Episiotomy = 28.9%. Perineal tear = 3.9%. Not allowing newborn skin-to-skin contact = 23.6%. Disrespect birth plan = 14.3%. | Risk factors associated: Several perineal tear (OR: 2.21 [1.17; 4.19]) and instrumental delivery (OR: 1.62 [1.10–2.41]). Protective factors associated: Perception of respect from healthcare professionals (OR: 0.42 [0.37; 0.48]) and allow skin-to-skin (OR: 0.65 [0.45–0.96]). |
| Martinez-Vázquez et al., 2021 [38] | 12.7% | Verbal violence = 32.3%. Physical violence = 17.6%. Psycho-affective violence = 27.0%. Disrespect birth plan = 39.2%. Induction of labor = 16.5%. Instrumental delivery = 11.8%. Emergency C-section = 33.1%. Episiotomy = 9.5%. Perineal tear = 16.5%. | Risk factors associated: Disrespect birth plan (aOR: 2.85 [1.56; 5.21]), scheduled C-section (aOR: 2.53 [1.02; 2.26]), emergency C-section (aOR: 3.58 [1.83; 6.99]), verbal violence (aOR: 5.07 [2.98; 8.63]) and psycho-affective violence (aOR: 2.61 [1.45; 4.67]). |
| Martínez-Vazquez et al., 2021a [39] | 13.1% | Verbal violence = 31.2%. Physical violence = 16.9%. Psycho-affective violence = 25.4%. Disrespect birth plan = 31.3%. Induction of labor = 16.0%. Instrumental delivery = 17.0%. Emergency C-section = 24.9%. Episiotomy = 15.4%. Perineal tear = 27.5%. Not allowing newborn skin-to-skin contact = 23.8%. Not breastfeeding 1 h after childbearing = 22.4%. Feeling disrespect by health professionals = 65.5%. | Risk factors associated: Disrespect birth plan (aOR: 1.89 [1.21; 2.94]), verbal (aOR: 3.73 [2.52; 5.53]), and physical violence (aOR: 3.98 [2.48; 6.39]). Induction of labor (OR: 1.50 [1.09; 2.06]), instrumental delivery (OR: 2.20 [1.42; 3.39]), emergency C-section (OR: 3.57 [2.41; 5.28]), and several perineal tears (OR: 2.26 [1.18; 4.30]). |
| Janevic et al., 2021 [53] | 100% reported low birth satisfaction, and 63.6% reported at least 1 discriminatory event in medical care. | Women who delivered vaginally: Low birth satisfaction = 41.4%. At least 1 discriminatory event in medical care during childbirth = 15.0%. Women who delivered by C-section: Low birth satisfaction = 73.1% At least 1 discriminatory event in medical care during childbirth = 40.4%. | Risk factors associated: Experiencing any discrimination during childbirth (aOR: 3.2 [1.1; 9.4]). |
| Kountanis et al., 2022 [40] | 20.7% at 6 weeks, 18.7% at 3 months, 17% at 6 months, and 24.5% at 12 months postpartum. | Perceived negative communication with the medical staff = 26.4%. | Protective factors associated: Positive perception of communication with the medical staff at 6 months (OR: 0.29) and 12 months postpartum (OR: 0.20). |
| Yakupova et al., 2021 [52] | 15.1% | Experienced at least 1 case of obstetric violence = 22.6%. Verbal aggression = 11.3%. Medical interventions without consent = 6.2%. Threats and accusations = 4.4%. Pain relief denial = 3.1%. Use of Kristeller technique = 3.1%. Ignoring the needs of the woman = 2.9%. Not social support = 42.1%. Episiotomy = 19%. Amniotomy = 45.7%. C-section = 22.6%. | Risk factors associated: Experienced obstetric violence (β = 5.09 [3.81; 6.38]). |
| Steetskamp et al., 2022 [41] | 2.9% | Not social support during labor = 35.0%. Birth injury = 55.0%. C-section = 17.0%. Vacuum extraction = 5.9%. | Risk factors associated: The mode of delivery (C-section: RR = 0.103). Protective factors associated: The assistant companion (social support: RR = −0.369). |
| Yakupova et al., 2022 [42] | 15.0% | Bullying = 11.3%. Intervention without consent = 6.2%, Threats and accusations = 4.4%. Use of Kristeller technique = 3.1%. Denial of pain relief = 3.1%. Amniotomy = 45.7%. Episiotomy = 19.0%. C-section = 22.6%. | Risk factors associated: Increased medical interventions (β = 1.03 [0.23; 1.84]) and perception of obstetric violence (β = 5.08 [3.80; 6.37]). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva-Fernandez, C.S.; de la Calle, M.; Arribas, S.M.; Garrosa, E.; Ramiro-Cortijo, D. Factors Associated with Obstetric Violence Implicated in the Development of Postpartum Depression and Post-Traumatic Stress Disorder: A Systematic Review. Nurs. Rep. 2023, 13, 1553-1576. https://doi.org/10.3390/nursrep13040130
Silva-Fernandez CS, de la Calle M, Arribas SM, Garrosa E, Ramiro-Cortijo D. Factors Associated with Obstetric Violence Implicated in the Development of Postpartum Depression and Post-Traumatic Stress Disorder: A Systematic Review. Nursing Reports. 2023; 13(4):1553-1576. https://doi.org/10.3390/nursrep13040130
Chicago/Turabian StyleSilva-Fernandez, Claudia Susana, Maria de la Calle, Silvia M. Arribas, Eva Garrosa, and David Ramiro-Cortijo. 2023. "Factors Associated with Obstetric Violence Implicated in the Development of Postpartum Depression and Post-Traumatic Stress Disorder: A Systematic Review" Nursing Reports 13, no. 4: 1553-1576. https://doi.org/10.3390/nursrep13040130
APA StyleSilva-Fernandez, C. S., de la Calle, M., Arribas, S. M., Garrosa, E., & Ramiro-Cortijo, D. (2023). Factors Associated with Obstetric Violence Implicated in the Development of Postpartum Depression and Post-Traumatic Stress Disorder: A Systematic Review. Nursing Reports, 13(4), 1553-1576. https://doi.org/10.3390/nursrep13040130