



Methodological Proposal for the Adaptation of the Living with Long-Term Conditions Scale to the Family Caregiver


Abstract
:1. Introduction
Background
2. Materials and Methods
- Objective of the Delphi study: It is indispensable to clearly and specifically establish the objective of the Delphi study. In the present study, the objective was to find the essential, clear, and relevant elements that constitute the process of living with LTC from the perspective of the family caregivers. These elements were identified through an integrative review that was previously conducted [7].
- Delphi study participants: The adequate selection of the participants in a Delphi study is a determining factor, although there is no consensus on the recommended number in the selection of experts to be included [19,23,24]. Romero-Collado [24] includes results similar to Carretero-Dios and Pérez in [24], who argued for a minimum of 3 experts; on their part, Yánez and Cuadra (2008) in [24] recommend between 10 and 18, and on the contrary, Humphrey-Murto [20] recommend a minimum of 6 and more than 12 in the case that the experts come from the same discipline, and lastly, Toronto in [24] considers that 12 to 20 experts is sufficient. Therefore, given the lack of consensus in the literature consulted, the guidelines used in the development of the original EC-PC scale [1] were followed. These were the selection of a group of experts that met the following inclusion criteria: post-graduate/doctorate degree; professional experience of more than 10 years in the area of health or social care, teaching, and/or research; and the ability to provide comprehensive opinions and suggestions, and motivation for participating in the study. In the present study, 12 healthcare professionals were included (M = 25%; F = 75%), including experts in the care of chronic diseases (50%), psychometry (25%), and family caregivers (25%). Two had professional experience and postgraduate education in social intervention psychology. Considering the area of work, 66.6% were associated with areas of teaching and research, and 33% with the area of healthcare, with 91.6% having a PhD in their specialty, and 8.3% a master’s degree. More specifically, the following were included: two psychologists who were experts in chronic diseases, a social care psychologist who was an expert in psychometry, a family doctor who was an expert in chronic diseases, four nurses who were experts in chronic diseases, a nurse who specialized in psychometry, two nurses who specialized in family caregivers, and a social care psychologist who was an expert in family caregivers.
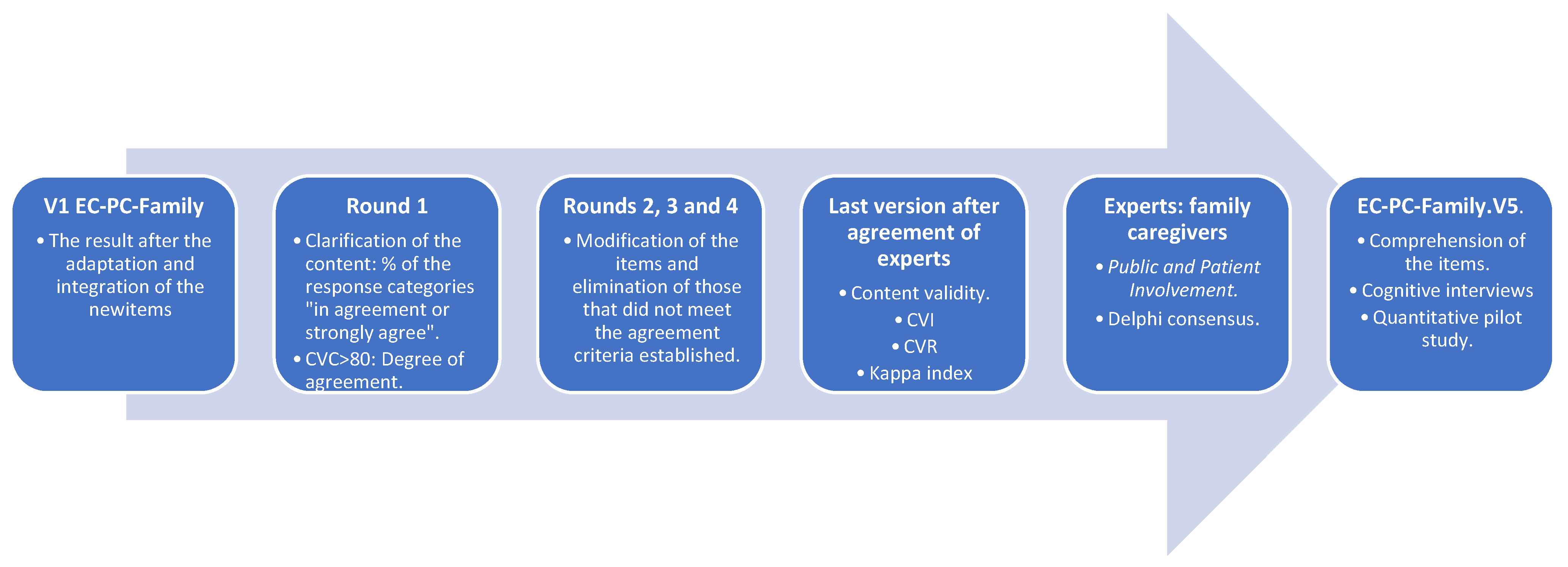
- Delphi study process: The Google Forms (eDelphi) tool was used for this. The questionnaire was structured into various sections. The first section contained a brief description of the study, the name of the project and its aim, the contact information of the principal researcher, in case any doubts arose during the process and the consent for their free participation. The second part included sociodemographic data of the individuals polled (age, profession, education, years of experience, area). The third part included the initial list of the items in the scale [19], with the possibility of scaled responses, considering the degree of adaptation for the inclusion of the item, which oscillated from 1 to 5, with 1 being “Not adequate”, and 5 “Very adequate”. The last section was reserved for the experts to provide suggestions, observations, or any related matter. The qualitative data provided by the experts were grouped according to themes in order to include the necessary modifications in the EC-PC-Family scale throughout the different versions created, including the perceptions, suggestions, or modifications proposed [12]. After four rounds with the experts, once an agreement was reached, the questionnaire was sent to a group of family caregiver representatives (n = 6), selected ad hoc to promote the active participation of the population of interest: public and patient involvement (PPI) [28]. This family caregiver group of PPI was composed of 2 men (33.3%) and 4 women (66.6%), with a mean age of 61 years old (±17.5), of which 4/6 (66.6%) had played the role of family caregiver for less than 3 years, while 33.3% had played the role for more than 3 years. In the first round, to clarify the suitability of the content, the measurements oriented towards the identification of the degree of agreement between the experts were used as criteria. More specifically, two criteria were utilized: in the first place, the percentage of one or some of the response categories. This criterion was used in the case of scalable questions, in which two contiguous categories can be considered [19]; an item was accepted if it obtained a score such as in agreement (4) or very much in agreement (5) from 70% of the experts [20]. In the second place, the content validity coefficient (CVC) > 80 was utilized, specifically designed to assess the degree of agreement with respect to each of the different items and the instrument in general [29], associating the error assigned to each item to minimize the possible bias introduced by any of the judges [30]. Next, to evaluate the evidence of the expert’s judgment in relation to the final content of the scale, the content validity was measured. Validity is defined as the extent to which any instrument measures what is intended [21]. For this, two empirical measurements were utilized: the Content Validity Index (Item-CVI and Scale-CVI), and Content Validity Reason (CVR) [20,29,30,31]. The Item-CVI (I-CVI) is computed as the number of experts providing a rating of “very relevant” for each item divided by the total number of experts. Values range from 0 to 1: when I-CVI > 0.79 the item is relevant, between 0.70 and 0.79 the item needs revisions, and if the value is below 0.70 the item is eliminated [31]. Likewise, the Scale-CVI (S-CVI) was obtained using the universal agreement method (UA), dividing the number of items that have obtained a “very relevant” rating by experts (S-CVI/UA). Values ranging from S-CVI/UA ≥ 0.8 have an excellent content validity [32]. The CVR was calculated for each item of the instrument, considering those with a CVR > 0.59 as essential items. This value, according to Lawshe [33], is determined as a function of the number of experts who participated. Although the CVI is commonly used to estimate content validity, Wynd, Schmidt, and Schaefer [34] suggest that a Kappa statistic must also be associated, aside from the CVI, to avoid agreement by chance. Kappa is calculated with the following formula: K = (I-CVI − Pc)/(1 − Pc), where Pc = [N!/A! (N − A)!] × 0.5 N. In this formula, Pc = the probability of fortuitous agreement; N = number of experts; and A = number of experts who agree that the subject is relevant. The results of the process are also shown as scores, frequencies, and/or percentages in each response category, as well as dispersion measurements and means.
2.1. Data Sources
2.2. Ethical Considerations
3. Results
- 1.
- Phase 1. Adaptation of the EC-PC scale to the family caregiver.
- 2.
- Phase 2: Consensus through panel of experts.
- S-CVI results (relevance of the general questionnaire): The S-CVI was calculated by adding all the I-CVI divided by 34, obtaining a value of S-CVI = 0.95, while the S-CVI/UA was calculated by adding all the items equal to 1.00 (19 items), divided by 34, with the result obtained being S-CVI/UA = 0.56. These results indicate that according to the Universal Agreement method, the instrument has a moderate content validity (0.56), while the mean approach shows a high validity (0.95).
- Kappa: The Kappa values higher than 0.74 are considered excellent. All the items in V5 of the EC-PC-Family showed Kappa results >0.82 (see Table 3).
- Clarity results (individual items and general questionnaire): The mean clarity results for the individual items varied between 2.54 and 3.00. More specifically, fourteen items obtained a mean clarity score of 3.00, ten obtained a score of 2.83, eight obtained a score of 2.73, and one a score of 2.54 (see Table 3). The general clarity score of V5 of the EC-PC-Family was 2.8.
- CVR results: In this case, none of the items included in V5 of the EC-PC-Family were eliminated, with a mean CVR of 0.88 maintained. Thirteen of the items obtained a CVR of 1.00, eighteen obtained a score of 0.88, and two obtained a score of 0.64.
- 3.
- Phase 3: Pre-test of the instrument.
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Public Involvement Statement
Guidelines and Standards Statement
Conflicts of Interest
References
- Ambrosio, L.; Portillo, M.C.; Rodríguez-Blázquez, C.; Rodriguez-Violante, M.; Castrillo, J.C.M.; Arillo, V.C.; Martínez-Martín, P. Living with chronic illness scale: International validation of a new self-report measure in Parkinson’s disease. NPJ Park. Dis. 2016, 2, 16022. [Google Scholar] [CrossRef]
- Portillo, M.C.; Senosiain, J.M.; Arantzamendi, M.; Zaragoza, A.; Navarta, M.V.; Díaz de Cerio, S.; Moreno, V. ReNACE project. patients and relatives living with parkinson’s disease: Preliminary results of phase 1. Enfermería Neurológica 2012, 36, 31–38. [Google Scholar] [CrossRef]
- Årestedt, L.; Persson, C.; Rämgård, M.; Benzein, E. Experiences of encounters with healthcare professionals through the lenses of families living with chronic illness. J. Clin. Nurs. 2018, 27, 4. [Google Scholar] [CrossRef]
- European Commission. Report on Informal Care in the European Union; European Commission: Brussels, Belgium, 2018. [Google Scholar]
- NICE. Dementia: Assessment, management and support for people living with dementia and their carers (NICE guidline, NG97). Seishin Igaku. Clin. Psychiatry 2020, 62, 682–688. [Google Scholar] [CrossRef]
- NICE. Supporting Adult Carers (NG150). Available online: https://www.nice.org.uk/guidance/ng150 (accessed on 25 July 2022).
- Marín-Maicas, P.; Corchón, S.; Ambrosio, L.; Portillo, M.C. Living with long term conditions from the perspective of family caregivers. A scoping review and narrative synthesis. Int. J. Environ. Res. Public Health 2021, 18, 7294. [Google Scholar] [CrossRef]
- World Health Organization. Global Status Report on Noncommunicable Diseases; World Health Organization: Geneva, Switzerland, 2021.
- Canca-Sánchez, J.C.; García-Mayor, S.; Morales-Asencio, J.M.; Gómez-Gónzalez, A.J.; Kaknani-Uttumchandani, S.; Cuevas Fernández-Gallego, M.; Lupiáñez-Pérez, I.; Caro-Bautista, J.; León-Campos, Á. Predictors of health service use by family caregivers of persons with multimorbidity. J. Clin. Nurs. 2021, 30, 3045–3051. [Google Scholar] [CrossRef] [PubMed]
- Toptas, S.; Oz, F. Family Caregivers’ Involvement in Caring with Cancer and their Quality of Life. Asian Pac. J. Cancer Prec. 2019, 20, 1735–1741. [Google Scholar] [CrossRef]
- Ambrosio, L.; Perez-Manchon, D.; Carvajal-Carrascal, G.; Fuentes-Ramirez, A.; Caparros, N.; de Ocenda, R.; Ignacio, M.; Rodriguez-Blazquez, C. Psychometric validation of the living with chronic illness scale in patients with chronic heart failure. Int. J. Environ. Res. Public Health 2021, 18, 572. [Google Scholar] [CrossRef] [PubMed]
- Ambrosio, L.; Navarta-Sánchez, M.V.; Carvajal, A.; Garcia-Vivar, C. Living with Chronic Illness from the Family Perspective: An Integrative Review. Clin. Nurs. Res. 2021, 30, 579–590. [Google Scholar] [CrossRef] [PubMed]
- International Test Commission. The ITC Guidelines for Translating and Adapting Tests, 2nd ed.; International Test Commission: Chessington, UK, 2017. [Google Scholar]
- Heggestad, E.; Scheaf, D.; Banks, G.; Hausfeld, M.M.; Tonidandel, S.; Williams, E.B. Scale adaptation in organizational science research: A review and best-practice recommendations. J. Manag. 2019, 45, 2596–2627. [Google Scholar] [CrossRef]
- Li, Q.; Lin, Y.; Xu, Y.; Zhou, H.; Yang, L.; Xu, Y. Construct validity of the 17-item Benefit Finding Scale in Chinese cancer patients and their family caregivers. Healthcare 2021, 9, 512. [Google Scholar] [CrossRef]
- Orozco-Beltrán, D.; De Toro, J.; Galindo, M.J.; Marín-Jiménez, I.; Casellas, F.; Fuster-RuizdeApodaca, M.J.; García-Vivar, M.L.; Hormigo-Pozo, A.; Guilabert, M.; Sánchez-Vega, N.; et al. Healthcare experience and their relationship with demographic, disease and healthcare-related variables: A cross-sectional survey of patients with chronic diseases using the IEXPAC scale. Patient-Patient-Centered Outcomes Res. 2019, 12, 307–317. [Google Scholar] [CrossRef]
- Derogatis, L.R. The psychosocial adjustment to illness scale (PAIS). J. Psychosom. Res. 1986, 30, 77–91. [Google Scholar] [CrossRef] [PubMed]
- Casu, G.; Gremigni, P.; Sommaruga, M. The Patient-Professional Interaction Questionnaire (PPIQ) to assess patient centered care from the patient’s perspective. Patient Educ. Couns. 2019, 102, 126–133. [Google Scholar] [CrossRef]
- Piñeiro, E.M. Vista de La Técnica Delphi como estrategia de consulta a los implicados en la evaluación de programas. Rev. Investig. Educ. 2003, 21, 449–463. [Google Scholar]
- Humphrey-Murto, S.; Wood, T.J.; Gonsalves, C.; Mascioli, K.; Varpio, L. The Delphi Method. Acad. Med. 2020, 95, 168. [Google Scholar] [CrossRef]
- Stone, D.H. Design a questionnaire. BMJ 1993, 307, 1264–1266. [Google Scholar] [CrossRef] [PubMed]
- Devellis, R. Scale Development Theory and Applications; Sage Publications: Thousand Oaks, CA, USA, 2012. [Google Scholar]
- Nasa, P.; Jain, R.; Juneja, D. Delphi methodology in healthcare research: How to decide its appropriateness. World J. Methodol. 2021, 11, 116–129. [Google Scholar] [CrossRef] [PubMed]
- Romero-Collado, A. Elementos esenciales para elaborar un estudio con el método (e)Delphi. Enfermería Intensiv. 2020, 32, 100–104. [Google Scholar] [CrossRef]
- Falzarano, M.; Pinto Zipp, G. Seeking consensus through the use of the Delphi technique in health sciences research. J. Allied Health 2013, 42, 99–105. [Google Scholar]
- Helmer, O. Analysis of the Future: The Delphi Method; Rand Corp.: Santa Monica, CA, USA, 1967. [Google Scholar]
- Diamond, I.R.; Grant, R.C.; Feldman, B.M.; Pencharz, P.B.; Ling, S.C.; Moore, A.M.; Wales, P.W. Defining consensus: A systematic review recommends methodologic criteria for reporting of Delphi studies. J. Clin. Epidemiol. 2014, 67, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Barham, L. Public and Patient Involvement at the UK National Institute for Health and Clinical Excellence. Patient-Patient-Centered Outcomes Res. 2011, 4, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Pedrosa, I.; Suárez-Álvarez y García-Cueto, E. Evidencias sobre la Validez de Contenido: Avances Teóricos y Métodos para su Estimación [Content Validity Evidences: Theoretical Advances and Esti-mation Methods]. Acción Psicológica 2013, 10, 1578–1908. [Google Scholar] [CrossRef]
- Zamanzadeh, V.; Ghahramanian, A.; Rassouli, M.; Abbaszadeh, A.; Alavi-Majd, H.; Nikanfar, A.R. Design and implementation content validity study: Development of an instrument for measuring patient-centered communication. J. Caring Sci. 2015, 4, 165. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, I.B.; Adachi, J.D.; Beattie, K.A.; MacDermid, J.C. Development and validation of a new tool to measure the facilitators, barriers and preferences to exercise in people with osteoporosis. BMC Musculoskelet. Disord. 2017, 18, 1–9. [Google Scholar] [CrossRef]
- Shi, J.; Mo, X.; Sun, Z. Content validity index in scale development. Zhong Nan Da Xue Xue Bao. Yi Xue Ban J. Cent. South Univ. Med. Sci. 2012, 37, 152–155, (era 33). [Google Scholar]
- Lawshe, C.H. A quantitative approach to content validity. Pers. Psychol. 1975, 28, 563–575, (era 32). [Google Scholar] [CrossRef]
- Wynd, C.A.; Schmidt, B.; Schaefer, M.A. Two Quantitative Approaches for Estimating Content Validity. West. J. Nurs. Res. 2003, 25, 508–518. [Google Scholar] [CrossRef]
- Wilson, M. Constructing Measures: An Item Response Modeling Approach; Routledge: London, UK, 2004. [Google Scholar]
- Willis, G.B. Analysis of the Cognitive Interview in Questionnaire Design; Oxford University Press: London, UK, 2015. [Google Scholar]
- Caicedo Cavagnis, E.E.; Zalazar Jaime, M.F. Entrevistas cognitivas: Revisión, directrices de uso y aplicación en investigaciones psicológicas. Aval. Psicológica 2018, 17, 362–370. [Google Scholar]
- Drennan, J. Cognitive interviewing: Verbal data in the design and pretesting of questionnaires. J. Adv. Nurs. 2003, 42, 57–63. [Google Scholar] [CrossRef]
- Muñiz, J.; Fonseca-Pedrero, E. Diez pasos para la construcción de un test. Psicothema 2019, 31, 7. [Google Scholar] [PubMed]
- Saunders, B.; Sim, J.; Kingstone, T.; Baker, S.; Waterfield, J.; Bartlam, B.; Burroughs, H.; Jinks, C. Saturation in qualitative research: Exploring its conceptualization and operationalization. Qual. Quant. 2018, 52, 1893–1907. [Google Scholar] [CrossRef]
- Boateng, G.O.; Neilands, T.B.; Frongillo, E.A.; Melgar-Quiñonez, H.R.; Young, S.L. Best Practices for Developing and Validating Scales for Health, Social, and Behavioral Research: A Primer. Front. Public Health 2018, 6, 149. [Google Scholar] [CrossRef] [PubMed]
- Rattray, J.; Jones, M.C. Essential elements of questionnaire design and development. J. Clin. Nurs. 2007, 16, 234–243. [Google Scholar] [CrossRef]
- Sánchez-Villena, A.R.; de La Fuente-Figuerola, V. Estandarización, adaptación y validación de pruebas psicométricas: Diferencias necesarias. An. Pediatría 2020, 93, 353–354. [Google Scholar] [CrossRef] [PubMed]
- García de Yébenes Prous, M.J.; Rodríguez Salvanés, F.; Carmona Ortells, L. Validación de cuestionarios. Reumatol. Clín. 2009, 5, 171–177. [Google Scholar] [CrossRef]
- Hernández, A.; Elosua, P.; Fernández-Hermida, J.R.; Muñiz, J. Comisión de Test: Veinticinco años velando por la calidad de los test. Papeles Del Psicólogo 2022, 43, 55–62. [Google Scholar]
- Ambrosio, L.; Navarta-Sánchez, M.V.; Meneses, A.; Rodríguez-Blázquez, C. Escala de convivencia con un proceso crónico: Estudio piloto en pacientes con enfermedades crónicas. Atención Primaria 2020, 52, 142–150. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Type of Question | Question Utilized |
|---|---|
| Paraphrase | In our own words, how would you define living with LTC? |
| Judgment/confidence | What were you thinking about when answering what are the reasons for…? |
| Specific | In this specific question, what is the sense of the words living with LTC? |
| EC-PC | EC-PC-Family |
|---|---|
| In my day-to-day, I have integrated the ___(LTC) and everything associated with it. For example, treatment, symptoms, changes experienced, etc.). | In my day-to-day, I have integrated the family member’s ___(LTC) and everything associated with it. For example, treatment, symptoms, changes experienced, etc.). |
| I know the disease and I know what I have to do to control it at all times. | I know the family member’s disease and I know what I have to do to control it at all times. |
| Item | I-CVI 1 Relevance | Interpretation | I-CVI 1 Clarity | Interpretation | Kappa | Interpretation | CVR 2 | Interpretation | |
|---|---|---|---|---|---|---|---|---|---|
| Acceptance | 1 | 1 | Relevant | 0.91 | Clear | 1.00 | Excellent | 1 | Agreement |
| 2 | 0.91 | Relevant | 0.91 | Clear | 0.91 | Excellent | 0.82 | Agreement | |
| 3 | 1 | Relevant | 0.91 | Clear | 1.00 | Excellent | 0.82 | Agreement | |
| 4 | 0.82 | Relevant | 0.91 | Clear | 0.82 | Excellent | 0.64 | Agreement | |
| Coping | 1 | 1 | Relevant | 0.82 | Clear | 1.00 | Excellent | 0.82 | Agreement |
| 2 | 1 | Relevant | 1 | Clear | 1.00 | Excellent | 1.00 | Agreement | |
| 3 | 1 | Relevant | 0.91 | Clear | 1.00 | Excellent | 1.00 | Agreement | |
| 4 | 0.91 | Relevant | 0.82 | Clear | 0.91 | Excellent | 0.82 | Agreement | |
| 5 | 0.91 | Relevant | 0.91 | Clear | 0.91 | Excellent | 0.82 | Agreement | |
| 6 | 0.91 | Relevant | 1 | Clear | 0.91 | Excellent | 0.82 | Agreement | |
| 7 | 1 | Relevant | 1 | Clear | 1.00 | Excellent | 1.00 | Agreement | |
| Self-management | 1 | 1 | Relevant | 1 | Clear | 1.00 | Excellent | 1.00 | Agreement |
| 2 | 1 | Relevant | 0.91 | Clear | 1.00 | Excellent | 1.00 | Agreement | |
| 3 | 0.91 | Relevant | 0.82 | Clear | 0.91 | Excellent | 0.82 | Agreement | |
| 4 | 1 | Relevant | 0.91 | Clear | 1.00 | Excellent | 1.00 | Agreement | |
| 5 | 1 | Relevant | 0.73 | Clear | 1.00 | Excellent | 1.00 | Agreement | |
| 6 | 1 | Relevant | 1 | Clear | 1.00 | Excellent | 1.00 | Agreement | |
| 7 | 0.91 | Relevant | 1 | Clear | 0.91 | Excellent | 0.82 | Agreement | |
| 8 | 0.91 | Relevant | 1 | Clear | 0.91 | Excellent | 0.82 | Agreement | |
| Integration | 1 | 1 | Relevant | 0.91 | Clear | 1.00 | Excellent | 1.00 | Agreement |
| 2 | 0.91 | Relevant | 0.91 | Clear | 0.91 | Excellent | 0.82 | Agreement | |
| 3 | 1 | Relevant | 0.91 | Clear | 1.00 | Excellent | 0.82 | Agreement | |
| 4 | 0.91 | Relevant | 1 | Clear | 0.91 | Excellent | 0.82 | Agreement | |
| 5 | 0.91 | Relevant | 1 | Clear | 0.91 | Excellent | 0.82 | Agreement | |
| 6 | 0.91 | Relevant | 1 | Clear | 0.91 | Excellent | 0.82 | Agreement | |
| 7 | 1 | Relevant | 0.82 | Clear | 1.00 | Excellent | 0.82 | Agreement | |
| 8 | 0.91 | Relevant | 0.91 | Clear | 0.91 | Excellent | 0.82 | Agreement | |
| 9 | 0.82 | Relevant | 1 | Clear | 0.82 | Excellent | 0.64 | Agreement | |
| Adaptation | 1 | 1 | Relevant | 1 | Clear | 1.00 | Excellent | 1.00 | Agreement |
| 2 | 1 | Relevant | 0.82 | Clear | 1.00 | Excellent | 0.64 | Agreement | |
| 3 | 0.91 | Relevant | 0.91 | Clear | 0.91 | Excellent | 0.82 | Agreement | |
| 4 | 1 | Relevant | 0.91 | Clear | 1.00 | Excellent | 0.82 | Agreement | |
| 5 | 1 | Relevant | 1 | Clear | 1.00 | Excellent | 1 | Agreement | |
| 6 | 1 | Relevant | 1 | Clear | 1.00 | Excellent | 1 | Agreement |
| Key Concepts Analyzed, Themes | Sub-Themes | Quote | Definitions after Thematic Analysis and Inductive Deduction |
|---|---|---|---|
| Meaning of Living |
| P2: “Continuously living with a person, and try to help by living with her”. P9. “Experience, along with the person, how the disease process is, learning and helping with whatever is needed”. P10. “Care for a person attentively” P11. “Try to manage it as best possible, and adapt to living day to day. Experience with the person the disease process, how it changes, and the worsening process”. P14 “Live in a healthy way with the disease”. | Pay attention to and care for another person, knowing what to do at each moment in time, despite the changes created in you. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marín-Maicas, P.; Portillo, M.C.; Corchón, S.; Ambrosio, L. Methodological Proposal for the Adaptation of the Living with Long-Term Conditions Scale to the Family Caregiver. Nurs. Rep. 2024, 14, 532-544. https://doi.org/10.3390/nursrep14010041
Marín-Maicas P, Portillo MC, Corchón S, Ambrosio L. Methodological Proposal for the Adaptation of the Living with Long-Term Conditions Scale to the Family Caregiver. Nursing Reports. 2024; 14(1):532-544. https://doi.org/10.3390/nursrep14010041
Chicago/Turabian StyleMarín-Maicas, Patricia, Mari Carmen Portillo, Silvia Corchón, and Leire Ambrosio. 2024. "Methodological Proposal for the Adaptation of the Living with Long-Term Conditions Scale to the Family Caregiver" Nursing Reports 14, no. 1: 532-544. https://doi.org/10.3390/nursrep14010041
APA StyleMarín-Maicas, P., Portillo, M. C., Corchón, S., & Ambrosio, L. (2024). Methodological Proposal for the Adaptation of the Living with Long-Term Conditions Scale to the Family Caregiver. Nursing Reports, 14(1), 532-544. https://doi.org/10.3390/nursrep14010041