An Uncommon Tooth Fusion of Mandibular Primary Lateral Incisor with Canine

{kind=link}
Abstract
:1. Introduction
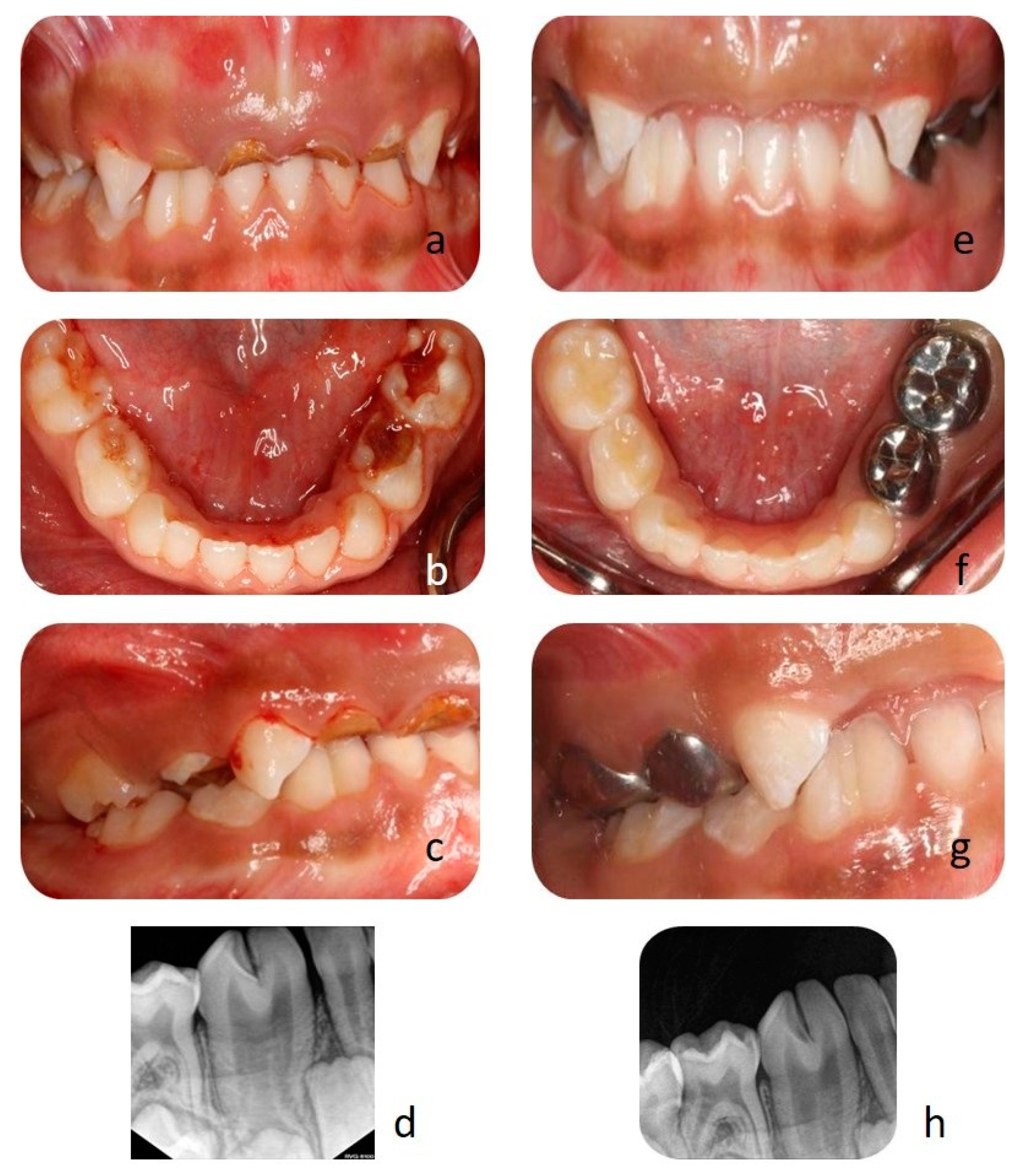
2. Case Report
3. Discussion
- Type I: bifid crown, single root;
- Type II: large crown, large root;
- Type III: two fused crowns, double conical root;
- Type IV: two fused crowns, two fused roots.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hagman, F. Fused primary teeth: A documented familial report of case. ASDC J. Dent. Child. 1985, 52, 459–460. [Google Scholar]
- Tasa, G.L.; Lukacs, J.R. The prevalence and expression of primary double teeth in western India. J. Dent. Child. 2001, 68, 196–200. [Google Scholar]
- Tomizawa, M.; Shimizu, A.; Hayashi, S.; Noda, T. Bilateral maxillary fused primary incisors accompanied by succedaneous supernumerary teeth: Report of a case. Int. J. Paediatr. Dent. 2002, 12, 223–227. [Google Scholar] [CrossRef]
- Uÿs, H.; Morris, D. ‘Double’ Teeth—A Diagnostic Conundrum. Dent. Update 2005, 32, 237–239. [Google Scholar] [CrossRef] [PubMed]
- Golabi, M.; Ito, M.; Hall, B.D.; Opitz, J.M. A new X-linked multiple congenital anomalies/mental retardation syndrome. Am. J. Med. Genet. 1984, 17, 367–374. [Google Scholar] [CrossRef]
- Schuurs, A.; Van Loveren, C. Double teeth: Review of the literature. ASDC J. Dent. Child. 2000, 67, 313. [Google Scholar]
- Gupta, T.; Manuja, N. Bilateral fusion of primary mandibular incisors: A rare case report. J. Clin. Diagn. Res. JCDR 2015, 9, ZJ01. [Google Scholar] [CrossRef]
- Zhu, M.; Liu, C.; Ren, S.; Lin, Z.; Miao, L.; Sun, W. Fusion of a supernumerary tooth to right mandibular second molar: A case report and literature review. Int. J. Clin. Exp. Med. 2015, 8, 11890. [Google Scholar]
- Chunawalla, Y.K.; Bijle, M.N.A. Pulp therapy in Maxillary fused primary central and lateral incisor: A Case Report. Int. J. Contemp. Dent. 2011, 2, 21–24. [Google Scholar]
- Duncan, W.K.; Helpin, M.L. Bilateral fusion and gemination: A literature analysis and case report. Oral Surg. Oral Med. Oral Pathol. 1987, 64, 82–87. [Google Scholar] [CrossRef]
- Aguilo, L.; Gandia, J.; Cibrian, R.; Catala, M. Primary double teeth. A retrospective clinical study of their morphological characteristics and associated anomalies. Int. J. Paediatr. Dent. 1999, 9, 175–183. [Google Scholar] [CrossRef]
- Brook, A.; Winter, G. Double teeth. A retrospective study of ‘geminated’ and ‘fused’ teeth in children. Br. Dent. J. 1970, 129, 123–130. [Google Scholar] [CrossRef]
- Kapur, R.; Kapur, R.; Gupta, R.; Kapur, R. Bilateral mandibular fusion in primary dentition—A case report. Indian J. Dent. 2011, 2, 57–59. [Google Scholar] [CrossRef]
- Walker, R.T. Root form and canal anatomy of mandibular second molars in a southern Chinese population. J. Endod. 1988, 14, 325–329. [Google Scholar] [CrossRef]
- Walker, R.T. Root form and canal anatomy of maxillary first premolars in a southern Chinese population. Dent. Traumatol. 1987, 3, 130–134. [Google Scholar] [CrossRef]
- King, N.M.; Tongkoom, S.; Wong, H. Morphological and numerical characteristics of the Southern Chinese dentitions. Part III: Anomalies in the primary dentition. Open Anthropol. J. 2010, 3, 25–36. [Google Scholar] [CrossRef] [Green Version]
- King, N.M.; Tsai, J.S.; Wong, H. Morphological and numerical characteristics of the southern chinese dentitions. Part II: Traits in the permanent dentition. Open Anthropol. J. 2010, 3, 71–84. [Google Scholar] [CrossRef] [Green Version]
- King, N.M.; Tsai, J.S.; Wong, H. Morphological and numerical characteristics of the southern Chinese dentitions. Part I: Anomalies in the permanent dentition. Open Anthropol. J. 2010, 3, 54–64. [Google Scholar] [CrossRef]
- King, N.M.; Tongkoom, S.; Wong, H. Morphological and numerical characteristics of the southern Chinese dentitions. Part IV: Traits in the primary dentition. Open Anthropol. J. 2010, 3, 37–53. [Google Scholar] [CrossRef]
- Kamminga, J.; Wright, R. The Upper Cave at Zhoukoudian and the origins of the Mongoloids. J. Hum. Evol. 1988, 17, 739–767. [Google Scholar] [CrossRef]
- Açıkel, H.; İbiş, S.; Tunç, E.Ş. Primary fused teeth and findings in permanent dentition. Med Princ. Pract. 2018, 27, 129–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zengin, A.; Celenk, P.; Gunduz, K.; Canger, M. Primary double teeth and their effect on permanent successors. Eur. J. Paediatr. Dent. 2014, 15, 309–312. [Google Scholar] [PubMed]
- Yuen, S.; Chan, J.; Wei, S. Double primary teeth and their relationship with the permanent successors: A radiographic study of 376 cases. Pediatric Dent. 1987, 9, 42. [Google Scholar]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlKlayb, S.A.; Devang Divakar, D. An Uncommon Tooth Fusion of Mandibular Primary Lateral Incisor with Canine. Clin. Pract. 2021, 11, 106-109. https://doi.org/10.3390/clinpract11010016
AlKlayb SA, Devang Divakar D. An Uncommon Tooth Fusion of Mandibular Primary Lateral Incisor with Canine. Clinics and Practice. 2021; 11(1):106-109. https://doi.org/10.3390/clinpract11010016
Chicago/Turabian StyleAlKlayb, Saleh Ali, and Darshan Devang Divakar. 2021. "An Uncommon Tooth Fusion of Mandibular Primary Lateral Incisor with Canine" Clinics and Practice 11, no. 1: 106-109. https://doi.org/10.3390/clinpract11010016
APA StyleAlKlayb, S. A., & Devang Divakar, D. (2021). An Uncommon Tooth Fusion of Mandibular Primary Lateral Incisor with Canine. Clinics and Practice, 11(1), 106-109. https://doi.org/10.3390/clinpract11010016