

Palliative Care and Multi-Agent Systems: A Necessary Paradigm Shift

 ,
,  ,
, 
Abstract
:1. Introduction
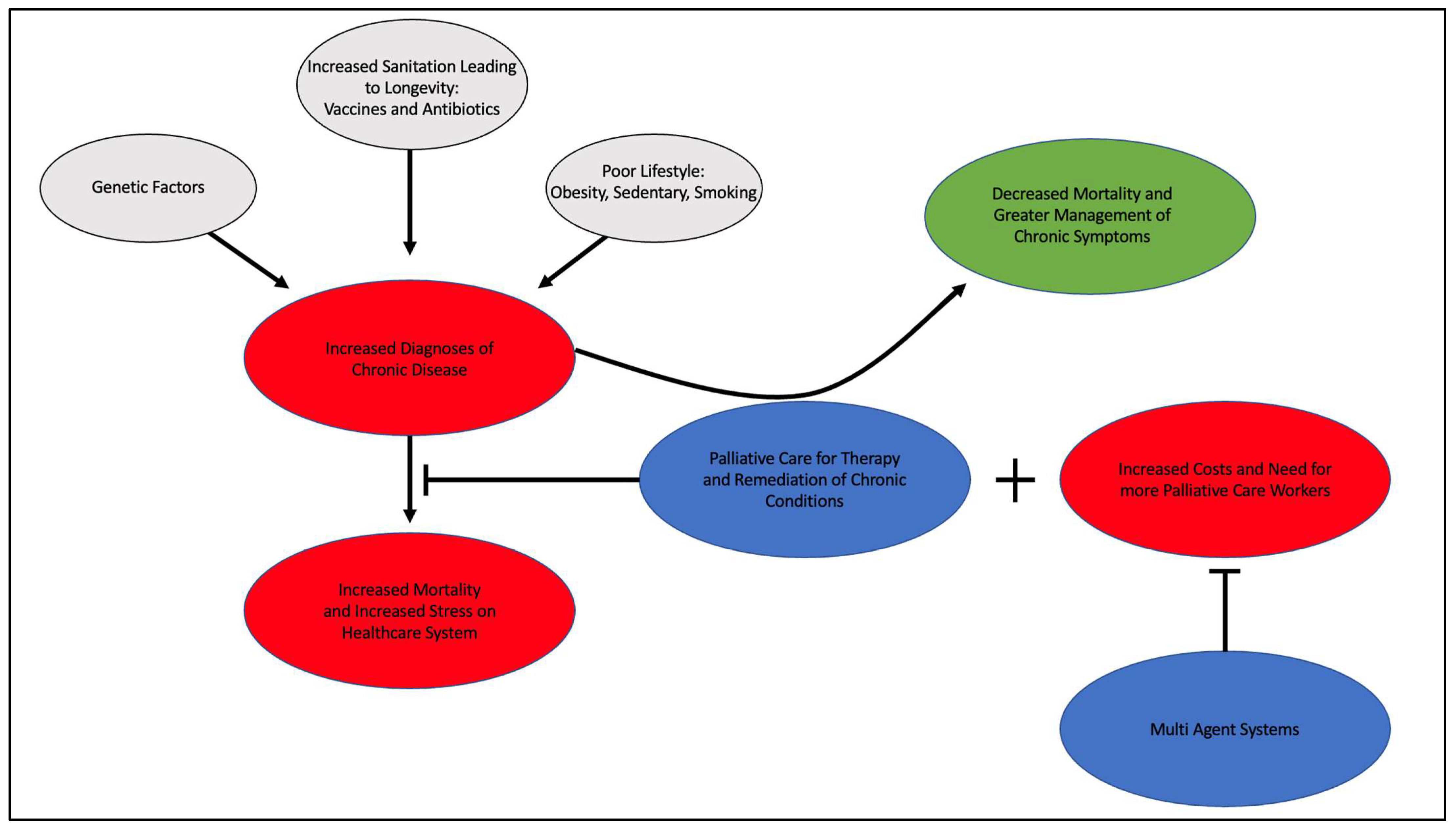
2. Chronic Disease and Contributing Factors
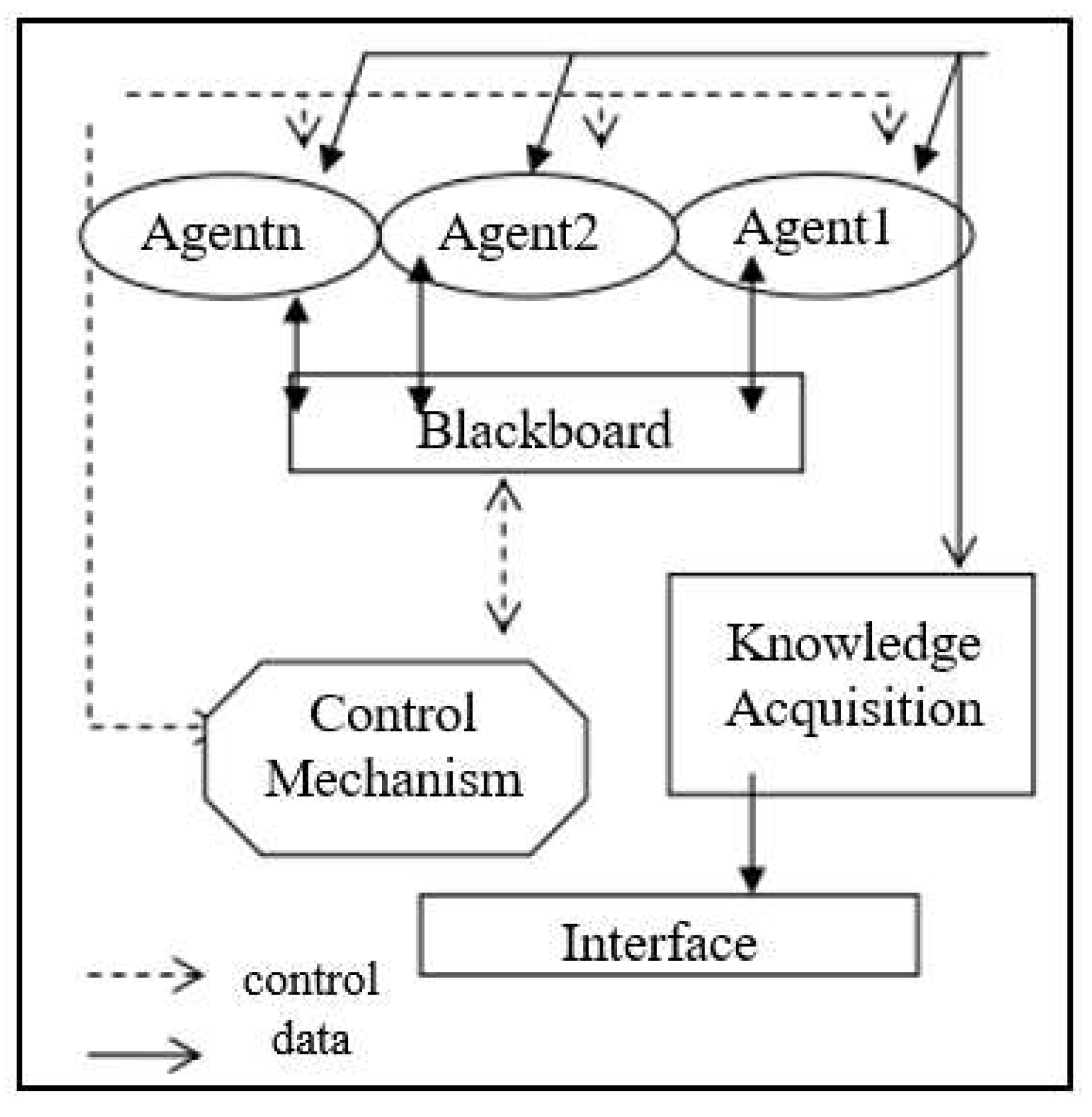
3. Multi-Agent Systems and Palliative Care
4. Clinical Considerations
4.1. Trajectories
4.2. Comparative Studies and Efficacy
4.3. Safety
4.4. Multi-Agent System
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Al-Mahrezi, A.; Al-Mandhari, Z. Palliative Care: Time for Action. Oman Med. J. 2016, 31, 161–163. [Google Scholar] [CrossRef] [PubMed]
- Palliative Care Improves Quality of Life. Available online: https://newsinhealth.nih.gov/2017/01/palliative-care-improves-quality-life (accessed on 6 January 2023).
- Palliative Care and Disease Types|Get Palliative Care. Available online: https://getpalliativecare.org/whatis/disease-types/ (accessed on 6 January 2023).
- Alva, H.; Sequeira, A.H.; Narayana, V.N. Proactive Approach to Palliative Care through Routine Monitoring by Home Caregivers Using Multiagent Systems: A Conceptual Framework. Rochester, NY. 2017. Available online: https://papers.ssrn.com/abstract=3022771 (accessed on 6 January 2023).
- 071204_H4L_FocusonWellness.pdf [Internet]. Available online: https://www.aha.org/system/files/content/00-10/071204_H4L_FocusonWellness.pdf (accessed on 6 January 2023).
- Hoffman, D. Commentary on Chronic Disease Prevention in 2022. National Association of Chronic Disease Directors. Available online: https://chronicdisease.org/wp-content/uploads/2022/04/FS_ChronicDiseaseCommentary2022FINAL.pdf (accessed on 6 January 2023).
- OACT. V. Results. Available online: https://www.ssa.gov/oact/NOTES/as116/as116_V.html (accessed on 6 January 2023).
- FastStats. Available online: https://www.cdc.gov/nchs/fastats/life-expectancy.htm (accessed on 6 January 2023).
- Bloom, D.E.; Cadarette, D. Infectious Disease Threats in the Twenty-First Century: Strengthening the Global Response. Front. Immunol. 2019, 10, 549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollard, A.J.; Bijker, E.M. A guide to vaccinology: From basic principles to new developments. Nat. Rev. Immunol. 2021, 21, 83–100. [Google Scholar] [CrossRef] [PubMed]
- How You Can Prevent Chronic Diseases|CDC. Available online: https://www.cdc.gov/chronicdisease/about/prevent/index.htm (accessed on 6 January 2023).
- CDC Current Cigarette Smoking Among Adults in the United States. Centers for Disease Control and Prevention. 2022. Available online: https://www.cdc.gov/tobacco/data_statistics/fact_sheets/adult_data/cig_smoking/index.htm (accessed on 6 January 2023).
- Data on Excessive Drinking|CDC. Available online: https://www.cdc.gov/alcohol/data-stats.htm (accessed on 6 January 2023).
- CDC Obesity is a Common, Serious, and Costly Disease. Centers for Disease Control and Prevention. 2022. Available online: https://www.cdc.gov/obesity/data/adult.html (accessed on 6 January 2023).
- Wehby, G.L.; Domingue, B.W.; Wolinsky, F.D. Genetic Risks for Chronic Conditions: Implications for Long-term Wellbeing. J. Gerontol. A. Biol. Sci. Med. Sci. 2018, 73, 477–483. [Google Scholar] [CrossRef] [Green Version]
- Palliative Care vs. Hospice: Which to Choose. CaringInfo. Available online: https://www.caringinfo.org/types-of-care/what-is-the-difference-between-palliative-care-and-hospice-care/ (accessed on 6 January 2023).
- Cruz-Oliver, D.M. Palliative Care: An Update. Mo. Med. 2017, 114, 110–115. [Google Scholar]
- Chronic Disease in the United States: A Worsening Health and Economic Crisis. AAF. Available online: https://www.americanactionforum.org/research/chronic-disease-in-the-united-states-a-worsening-health-and-economic-crisis/ (accessed on 6 January 2023).
- A Roadmap of Agent Research and Development. Available online: https://www.researchgate.net/publication/220660843_A_Roadmap_of_Agent_Research_and_Development (accessed on 6 January 2023).
- Ahmed Kamal, M.; Ismail, Z.; Shehata, I.M.; Djirar, S.; Talbot, N.C.; Ahmadzadeh, S.; Shekoohi, S.; Cornett, E.M.; Fox, C.J.; Kaye, A.D. Telemedicine, E-Health, and Multi-Agent Systems for Chronic Pain Management. Clin. Pract. 2023, 13, 470–482. [Google Scholar] [CrossRef]
- Kazar, O. Multi-Agents System for Medical Diagnosis. 2018. Available online: https://www.researchgate.net/publication/324569957_Multi-agents_system_for_medical_diagnosis#fullTextFileContent (accessed on 6 January 2023).
- Bureau, U.C. Older People Projected to Outnumber Children for First Time in U.S. History. Census.gov. Available online: https://www.census.gov/newsroom/press-releases/2018/cb18-41-population-projections.html (accessed on 6 January 2023).
- Anderson, L.A.; Goodman, R.A.; Holtzman, D.; Posner, S.F.; Northridge, M.E. Aging in the United States: Opportunities and Challenges for Public Health. Am. J. Public Health 2012, 102, 393–395. [Google Scholar] [CrossRef]
- Moreno, A. Medical Applications of Multi-Agent Systems. 12 April 2003. Available online: https://www.researchgate.net/publication/2901914_Medical_Applications_of_Multi-Agent_Systems (accessed on 6 January 2023).
- Shakshuki, E.; Reid, M. Multi-Agent System Applications in Healthcare: Current Technology and Future Roadmap. Procedia Comput. Sci. 2015, 52, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Yu, W.; Liu, X.; Zhao, F.; Li, M.; Zhang, L. Control of unreasonable growth of medical expenses in public hospitals in Shanghai, China: A multi-agent system model. BMC Health Serv. Res. 2020, 20, 490. [Google Scholar] [CrossRef]
- Cardoso, L.; Marins, F.; Portela, F.; Santos, M.; Abelha, A.; Machado, J. The Next Generation of Interoperability Agents in Healthcare. Int. J. Environ. Res. Public. Health 2014, 11, 5349–5371. [Google Scholar] [CrossRef] [Green Version]
- Safdari, R.; Shoshtarian Malak, J.; Mohammadzadeh, N.; Danesh Shahraki, A. A Multi Agent Based Approach for Prehospital Emergency Management. Bull. Emerg. Trauma 2017, 5, 171–178. [Google Scholar] [PubMed]
- Mohammadzadeh, N.; Safdari, R.; Rahimi, A. Multi-agent systems: Effective approach for cancer care information management. Asian Pac. J. Cancer Prev. APJCP 2013, 14, 7757–7759. [Google Scholar] [CrossRef] [PubMed]
- Mohammadzadeh, N.; Safdari, R.; Rahimi, A. Multi-Agent System as a New Approach to Effective Chronic Heart Failure Management: Key Considerations. Healthc. Inform. Res. 2013, 19, 162–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murtagh, F.E.M.; Preston, M.; Higginson, I. Patterns of dying: Palliative care for non-malignant disease. Clin. Med. Lond. Engl. 2004, 4, 39–44. [Google Scholar] [CrossRef]
- Levenson, J.W.; McCarthy, E.P.; Lynn, J.; Davis, R.B.; Phillips, R.S. The last six months of life for patients with congestive heart failure. J. Am. Geriatr. Soc. 2000, 48, S101–S109. [Google Scholar] [CrossRef]
- Murray, S.A.; Boyd, K.; Kendall, M.; Worth, A.; Benton, T.F.; Clausen, H. Dying of lung cancer or cardiac failure: Prospective qualitative interview study of patients and their carers in the community. BMJ 2002, 325, 929. [Google Scholar] [CrossRef] [Green Version]
- Murray, S.A.; Kendall, M.; Boyd, K.; Sheikh, A. Illness trajectories and palliative care. BMJ 2005, 330, 1007–1011. [Google Scholar] [CrossRef] [Green Version]
- Siouta, N.; Van Beek, K.; van der Eerden, M.E.; Preston, N.; Hasselaar, J.G.; Hughes, S.; Garralda, E.; Centeno, C.; Csikos, A.; Groot, M.; et al. Integrated palliative care in Europe: A qualitative systematic literature review of empirically-tested models in cancer and chronic disease. BMC Palliat. Care 2016, 15, 56. [Google Scholar] [CrossRef] [Green Version]
- O’Leary, N.; Murphy, N.F.; O’Loughlin, C.; Tiernan, E.; McDonald, K. A comparative study of the palliative care needs of heart failure and cancer patients. Eur. J. Heart Fail. 2009, 11, 406–412. [Google Scholar] [CrossRef]
- Baumann, A.J.; Wheeler, D.S.; James, M.; Turner, R.; Siegel, A.; Navarro, V.J. Benefit of Early Palliative Care Intervention in End-Stage Liver Disease Patients Awaiting Liver Transplantation. J. Pain Symptom Manag. 2015, 50, 882–886.e2. [Google Scholar] [CrossRef]
- Early Palliative Care for Patients with Metastatic Non–Small-Cell Lung Cancer|NEJM. Available online: https://www.nejm.org/doi/full/10.1056/NEJMOa1000678#t=article (accessed on 6 January 2023).
- Muhandiramge, D.; Udeoji, D.U.; Biswas, O.S.; Bharadwaj, P.; Black, L.Z.; Mulholland, K.A.; Moschella, C.; Schwarz, E.R. Palliative care issues in heart transplant candidates. Curr. Opin. Support. Palliat. Care 2015, 9, 5. [Google Scholar] [CrossRef] [PubMed]
- Donald, R.S.; Benjamin, C.; Jodi, A.L.; Linda, G.; Lissi, H.; Patricia, A.C.; Erik, K.F.; Miguel, M.; Sara, E.G.; Kelly, C.V.; et al. Association of Early Palliative Care Use With Survival and Place of Death Among Patients With Advanced Lung Cancer Receiving Care in the Veterans Health Administration|Lung Cancer|JAMA Oncology|JAMA Network. Available online: https://jamanetwork.com/journals/jamaoncology/fullarticle/2751526 (accessed on 6 January 2023).
- Yardley, I.; Yardley, S.; Williams, H.; Carson-Stevens, A.; Donaldson, L.J. Patient safety in palliative care: A mixed-methods study of reports to a national database of serious incidents. Palliat. Med. 2018, 32, 1353–1362. [Google Scholar] [CrossRef] [PubMed]
- Riaño, D.; Moreno, A.; Valls, Ä. PalliaSys: Agent-Based Palliative Care. 2004. Available online: https://www.semanticscholar.org/paper/PalliaSys%3A-Agent-Based-Palliative-Care-Ria%C3%B1o-Moreno/38cef93255fc19dee8453706f82830c1bc51c6c3 (accessed on 6 January 2023).
- McKean, J.; Shorter, H.; Luck, M.; McBurney, P.; Willmott, S. Technology diffusion: Analysing the diffusion of agent technologies. Auton. Agents Multi-Agent Syst. 2008, 17, 372–396. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author (Year) | Groups Studied/Intervention | Results/Findings | Conclusions |
|---|---|---|---|
| Study 1: Baumann AJ et al. The benefit of Early Palliative Care Intervention in End-Stage Liver Disease Patients Awaiting Liver Transplantation [37] | A 2015 improvement report looked at patients with end-stage liver disease (ESLD). The patients were provided an early palliative care intervention and subsequently assessed to see if clinical improvement occurred in addition to positive changes in mood. | Pre-palliative care: 23 of 30 (76.6%) of patients reported moderate-to-severe symptoms of pruritis, well-being, anxiety, appetite, and fatigue. Pre-palliative care: 13 of 30 patients reported depressive symptoms. Post-palliative care: 50% of the moderate-to-severe symptoms significantly improved, with fatigue and well-being having less statistically significant reduction. Post-palliative depressive symptoms were reduced by 27.8%. | Study 1 provides objective data showing symptom improvement in those provided the palliative care intervention. This efficacy is significant for providers to keep in mind for all trajectories of illness. Knowing the efficacy of this palliative care intervention, the healthcare system must deal with the best method to cope with the increase in demand for services if it becomes widely used. |
| Study 2: Yardley I, et al. Patient safety in palliative care: A mixed-methods study of reports to a national database of serious incidents [41] | A 2018 study looked at the national database of the National Health Service in England to find reports of serious incidents requiring investigation. These reports were targeted at patients receiving palliative care. | 475 reports identified. Reports classified as follows: 266 reports of pressure ulcers, 91 reports of medication errors, 18 of disturbed dying, 8 of transfer incidents, 6 of suicides, 5 unspecified. | The study concluded that these incidents could mostly be attributed to lack of coordination, staff and providers without proper palliative care experience, and under-resourcing. |
| Study 3: Sullivan D, et al. Association of Early Palliative Care Use With Survival and Place of Death Among Patients With Advanced Lung Cancer Receiving Care in the Veterans Health Administration [40] | A 2019 study looked at 23,154 patients with Stage IIIb or Stage IV lung cancer from the Veterans Affairs healthcare system. The study assessed enhanced survivability in early palliative care; 57% received palliative care. | Palliative care, after diagnosis, from 0–30 days = decreased survivability. Palliative care from 31–365 days, after diagnosis, =greater survivability. Palliative care received after 365 days = no significance. | Palliative care is associated with greater survivability and reduced risk of death in acute care settings. Palliative care should be considered a complementary approach to disease-modifying therapy in patients with advanced lung cancer. |
| Author (Year) | Groups Studied and Intervention | Results and Findings | Conclusions |
|---|---|---|---|
| Study 1: O’Leary N et al. A comparative study of the palliative care needs of heart failure and cancer patients [36] | A 2009 cross-sectional comparative cohort study looked to assess whether the palliative care needs of those with heart failure were similar to the needs of those with cancer. The study used both quantitative and qualitative measures in the study. | The two groups reported comparable levels of overall need for palliative care. Differences in specific needs did exist between the two groups. For example, the group with heart failure had a completely different symptom burden than the group with cancer. | A tailored approach must be considered with palliative care. It can benefit patients of all illness trajectories. However, each illness requires different needs to increase the comfort of the patient. |
| Study 2: Siouta N. et al., Integrated palliative care in Europe: a qualitative systematic literature review of empirically-tested models in cancer and chronic disease [35] | Fourteen studies including 7 for chronic disease, 4 for oncology, 2 for chronic disease and cancer, and 2 for end-of-life pathways. Evaluation of integrated palliative care in disease treatment throughout Europe. | Better symptom control, less caregiver burden, improvement in continuity and coordination of care, fewer admissions, lower costs, and patients passing in their preferred location. | A generic framework for PC in cancer and chronic disease is needed—one that includes aspects of treatment, consulting, and training. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brondeel, K.C.; Duncan, S.A.; Luther, P.M.; Anderson, A.; Bhargava, P.; Mosieri, C.; Ahmadzadeh, S.; Shekoohi, S.; Cornett, E.M.; Fox, C.J.; et al. Palliative Care and Multi-Agent Systems: A Necessary Paradigm Shift. Clin. Pract. 2023, 13, 505-514. https://doi.org/10.3390/clinpract13020046
Brondeel KC, Duncan SA, Luther PM, Anderson A, Bhargava P, Mosieri C, Ahmadzadeh S, Shekoohi S, Cornett EM, Fox CJ, et al. Palliative Care and Multi-Agent Systems: A Necessary Paradigm Shift. Clinics and Practice. 2023; 13(2):505-514. https://doi.org/10.3390/clinpract13020046
Chicago/Turabian StyleBrondeel, Kimberley C., Sheina A. Duncan, Patrick M. Luther, Alexandra Anderson, Pranav Bhargava, Chizoba Mosieri, Shahab Ahmadzadeh, Sahar Shekoohi, Elyse M. Cornett, Charles J. Fox, and et al. 2023. "Palliative Care and Multi-Agent Systems: A Necessary Paradigm Shift" Clinics and Practice 13, no. 2: 505-514. https://doi.org/10.3390/clinpract13020046
APA StyleBrondeel, K. C., Duncan, S. A., Luther, P. M., Anderson, A., Bhargava, P., Mosieri, C., Ahmadzadeh, S., Shekoohi, S., Cornett, E. M., Fox, C. J., & Kaye, A. D. (2023). Palliative Care and Multi-Agent Systems: A Necessary Paradigm Shift. Clinics and Practice, 13(2), 505-514. https://doi.org/10.3390/clinpract13020046