
Investigation of the Quality of Life of Patients with Gastrointestinal Issues Treated in the Surgical Clinic of a Regional General Hospital in Greece

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Sample and Participants
2.2. Research Tools
2.3. Data Collection
2.4. Ethical Considerations
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
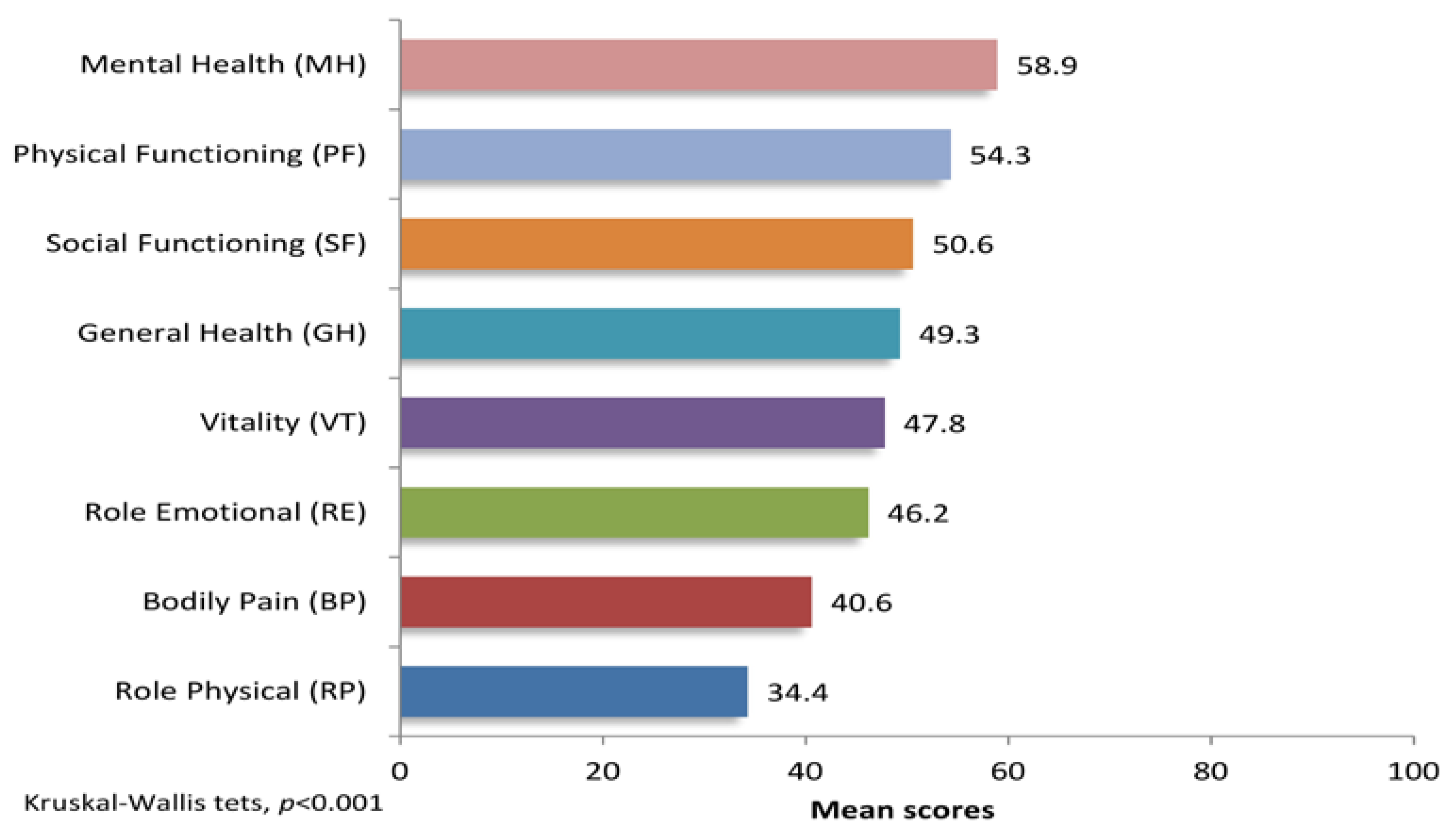
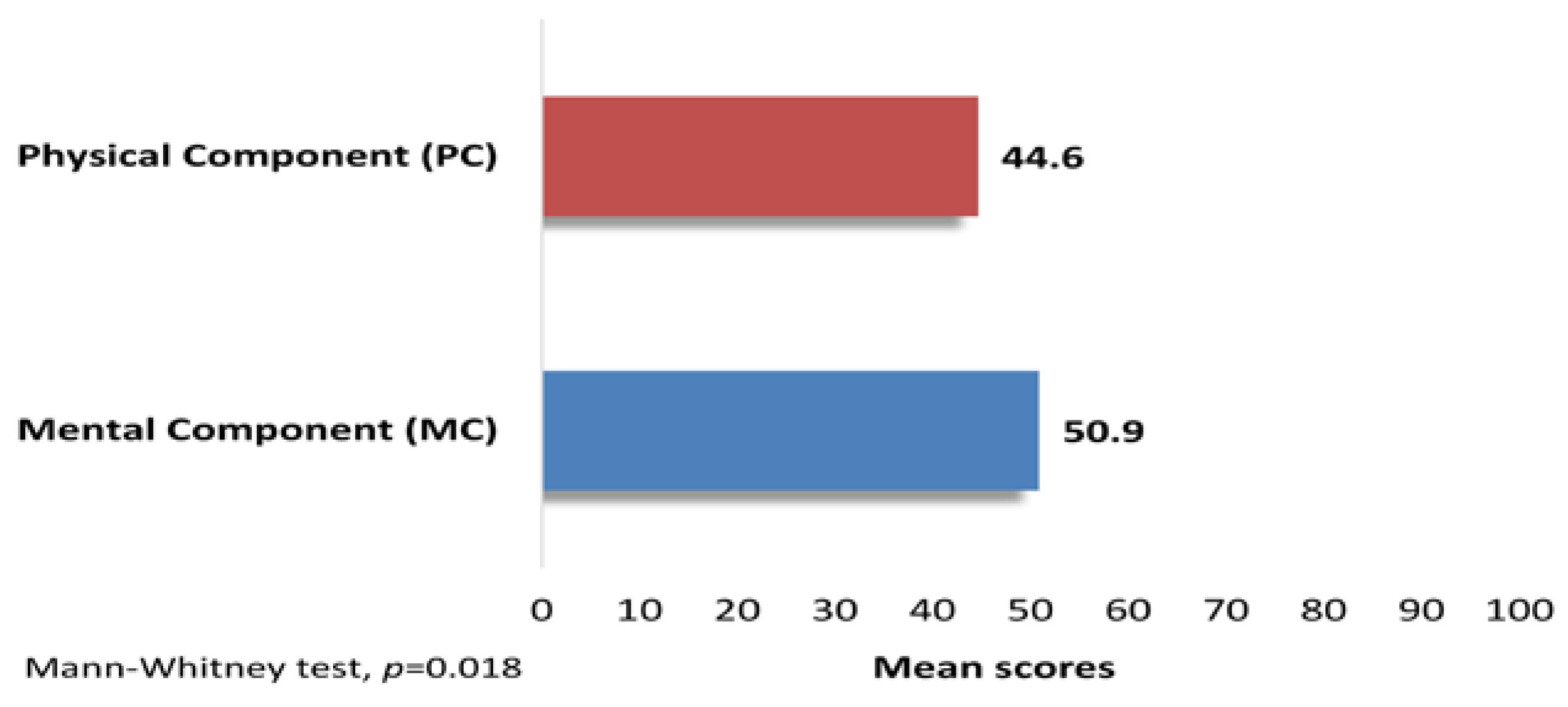
3.2. Quality of Life & Anxiety
3.3. Characteristics, QoL & Anxiety
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Greenwood-Van Meerveld, B.; Johnson, A.C.; Grundy, D. Gastrointestinal Physiology and Function. In Handbook of Experimental Pharmacology; Springer: Berlin/Heidelberg, Germany, 2017; Volume 239, pp. 1–16. [Google Scholar] [CrossRef]
- Black, C.J.; Drossman, D.A.; Talley, N.J.; Ruddy, J.; Ford, A.C. Functional gastrointestinal disorders: Advances in understanding and management. Lancet 2020, 396, 1664–1674. [Google Scholar] [CrossRef]
- Sperber, A.D.; Bangdiwala, S.I.; Drossman, D.A.; Ghoshal, U.C.; Simren, M.; Tack, J.; Whitehead, W.E.; Dumitrascu, D.L.; Fang, X.; Fukudo, S.; et al. Worldwide Prevalence and Burden of Functional Gastrointestinal Disorders, Results of Rome Foundation Global Study. Gastroenterology 2021, 160, 99–114.e113. [Google Scholar] [CrossRef]
- Drossman, D.A. Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features and Rome IV. Gastroenterology 2016, 150, 1262–1279. [Google Scholar] [CrossRef] [Green Version]
- Tack, J.; Stanghellini, V.; Mearin, F.; Yiannakou, Y.; Layer, P.; Coffin, B.; Simren, M.; Mackinnon, J.; Wiseman, G.; Marciniak, A. Economic burden of moderate to severe irritable bowel syndrome with constipation in six European countries. BMC Gastroenterol. 2019, 19, 69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, R.K.; Drossman, D.A. Quality of life measures in irritable bowel syndrome. Expert Rev. Gastroenterol. Hepatol. 2010, 4, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Creed, F.; Ratcliffe, J.; Fernandez, L.; Tomenson, B.; Palmer, S.; Rigby, C.; Guthrie, E.; Read, N.; Thompson, D. Health-related quality of life and health care costs in severe, refractory irritable bowel syndrome. Ann. Intern. Med. 2001, 134, 860–868. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.K.; Shin, C. The Microbiota-Gut-Brain Axis in Neuropsychiatric Disorders: Pathophysiological Mechanisms and Novel Treatments. Curr. Neuropharmacol. 2018, 16, 559–573. [Google Scholar] [CrossRef]
- O’Mahony, S.M.; Clarke, G.; Dinan, T.G.; Cryan, J.F. Irritable Bowel Syndrome and Stress-Related Psychiatric Co-morbidities: Focus on Early Life Stress. In Gastrointestinal Pharmacology; Greenwood-Van Meerveld, B., Ed.; Springer International Publishing: Cham, Switzerland, 2017; pp. 219–246. [Google Scholar]
- Anagnostopoulos, F.; Niakas, D.; Pappa, E. Construct validation of the Greek SF-36 Health Survey. Qual. Life Res. 2005, 14, 1959–1965. [Google Scholar] [CrossRef]
- Rikos, N.; Flouri, M.; Pandermaraki, E.; Spokos, E.; Linardakis, M. Health-related quality of life of patients with rheumatic diseases in the Southern Aegean region, Greece. Arch. Hell. Med. 2022, 39, 344–353. [Google Scholar]
- Fountoulakis, K.N.; Papadopoulou, M.; Kleanthous, S.; Papadopoulou, A.; Bizeli, V.; Nimatoudis, I.; Iacovides, A.; Kaprinis, G.S. Reliability and psychometric properties of the Greek translation of the State-Trait Anxiety Inventory form Y: Preliminary data. Ann. Gen. Psychiatry 2006, 5, 2. [Google Scholar] [CrossRef] [Green Version]
- Emons, W.H.; Habibović, M.; Pedersen, S.S. Prevalence of anxiety in patients with an implantable cardioverter defibrillator: Measurement equivalence of the HADS-A and the STAI-S. Qual. Life Res. 2019, 28, 3107–3116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, M.G.; Jung, H.K. Health related quality of life in functional gastrointestinal disorders in Asia. J. Neurogastroenterol. Motil. 2011, 17, 245–251. [Google Scholar] [CrossRef]
- Ross, E.J.; Vivier, H.; Cassisi, J.E.; Dvorak, R.D. Gastrointestinal health: An investigation of mediating effects on mood and quality of life. Health Psychol. Open 2020, 7, 2055102920974524. [Google Scholar] [CrossRef]
- Van Tilburg, M.A.; Murphy, T.B. Quality of life paradox in gastrointestinal disorders. J. Pediatr. 2015, 166, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.C. Psychological Co-morbidity in Functional Gastrointestinal Disorders: Epidemiology, Mechanisms and Management. J. Neurogastroenterol. Motil. 2012, 18, 13–18. [Google Scholar] [CrossRef] [PubMed]
- Hartono, J.L.; Mahadeva, S.; Goh, K.L. Anxiety and depression in various functional gastrointestinal disorders: Do differences exist? J. Dig. Dis. 2012, 13, 252–257. [Google Scholar] [CrossRef]
- Pletikosić Tončić, S.; Tkalčić, M. A Measure of Suffering in relation to Anxiety and Quality of Life in IBS Patients: Preliminary Results. BioMed Res. Int. 2017, 2017, 2387681. [Google Scholar] [CrossRef] [Green Version]
- Söderquist, F.; Syk, M.; Just, D.; Kurbalija Novicic, Z.; Rasmusson, A.J.; Hellström, P.M.; Ramklint, M.; Cunningham, J.L. A cross-sectional study of gastrointestinal symptoms, depressive symptoms and trait anxiety in young adults. BMC Psychiatry 2020, 20, 535. [Google Scholar] [CrossRef] [PubMed]
- Jerndal, P.; Ringström, G.; Agerforz, P.; Karpefors, M.; Akkermans, L.M.; Bayati, A.; Simrén, M. Gastrointestinal-specific anxiety: An important factor for severity of GI symptoms and quality of life in IBS. Neurogastroenterol. Motil. 2010, 22, 646-e179. [Google Scholar] [CrossRef] [PubMed]
- Kanchibhotla, D.; Sharma, P.; Subramanian, S. Improvement in Gastrointestinal Quality of Life Index (GIQLI) following meditation: An open-trial pilot study in India. J. Ayurveda. Integr. Med. 2021, 12, 107–111. [Google Scholar] [CrossRef]
- Martin, D. Physical activity benefits and risks on the gastrointestinal system. South. Med. J. 2011, 104, 831–837. [Google Scholar] [CrossRef]
- Sadeghian, M.; Sadeghi, O.; Hassanzadeh Keshteli, A.; Daghaghzadeh, H.; Esmaillzadeh, A.; Adibi, P. Physical activity in relation to irritable bowel syndrome among Iranian adults. PLoS ONE 2018, 13, e0205806. [Google Scholar] [CrossRef] [PubMed]
- Axelrod, C.H.; Saps, M. Global Dietary Patterns and Functional Gastrointestinal Disorders. Children 2020, 7, 152. [Google Scholar] [CrossRef] [PubMed]
- Saneei, P.; Esmaillzadeh, A.; Keshteli, A.H.; Roohafza, H.R.; Afshar, H.; Feizi, A.; Adibi, P. Combined Healthy Lifestyle Is Inversely Associated with Upper Gastrointestinal Disorders among Iranian Adults. Dig. Dis. 2021, 39, 77–88. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| n | % | ||
|---|---|---|---|
| Gender | men/women | 42/41 | 50.6/49.4 |
| Age, years | 18–49 | 35 | 42.2 |
| 50–69 | 32 | 38.5 | |
| 70–93 | 16 | 19.3 | |
| Marital status | Unmarried, Divorced, Widowed | 25 | 30.1 |
| Married, Partnered | 58 | 69.9 | |
| Children | yes/no | 69/14 | 83.1/16.9 |
| Nationality | Greek/other | 78/5 | 94.0/6.0 |
| Place of residence | Rural | 18 | 21.7 |
| Urban | 65 | 78.3 | |
| Education | Primary school | 18 | 21.7 |
| Lower Secondary school | 16 | 19.3 | |
| Higher Secondary school | 14 | 16.9 | |
| Higher education (University, Technical College) | 18 | 21.7 | |
| MA, MSc, PhD | 17 | 20.4 | |
| Monthly income, € | <500 | 24 | 28.9 |
| 500–999 | 23 | 27.7 | |
| 1000+ | 36 | 43.4 |
| Mean | SD | Median | Min. | Max. | Cronbach’s α | |
|---|---|---|---|---|---|---|
| SF-36 QoL Components a | ||||||
| Physical Functioning (PF) | 54.3 | 29.7 | 50.0 | 0.0 | 100.0 | 0.900 |
| Role Physical (RP) | 34.3 | 41.6 | 0.0 | 0.0 | 100.0 | 0.897 |
| Bodily Pain (BP) | 40.6 | 24.3 | 40.0 | 0.0 | 80.0 | 0.791 |
| General Health (GH) | 49.3 | 18.0 | 50.0 | 0.0 | 100.0 | 0.697 |
| Vitality (VT) | 47.8 | 20.7 | 50.0 | 0.0 | 95.0 | 0.836 |
| Social Functioning (SF) | 50.6 | 19.7 | 50.0 | 12.5 | 100.0 | 0.680 |
| Role Emotional (RE) | 46.2 | 43.2 | 33.3 | 0.0 | 100.0 | 0.711 |
| Mental Health (MH) | 58.9 | 18.8 | 60.0 | 12.0 | 100.0 | 0.810 |
| Physical Component (PC) | 44.6 | 20.4 | 42.5 | 0.0 | 95.0 | 0.863 |
| moderate/high (>50.0) | n = 29 or 34.9% | |||||
| Mental Component (MC) | 50.9 | 15.6 | 50.2 | 19.3 | 86.3 | 0.787 |
| moderate/high (>50.0) | n = 42 or 50.6% | |||||
| Anxiety | ||||||
| State Anxiety (STAI) b | 45.4 | 8.9 | 47.0 | 26 | 66 | 0.807 |
| low (up to 40) | n = 26 or 31.3% | |||||
| high (>40) | n = 57 or 68.7% | |||||
| QoL: | State Anxiety | Δ-Difference | p-Value | |||
|---|---|---|---|---|---|---|
| Low (up to 40) | High (>40) | |||||
| Mean | SD | Mean | SD | |||
| Physical Component a | 50.4 | 19.8 | 42.0 | 20.3 | 8.4 | 0.083 |
| Mental Component a | 58.7 | 13.8 | 47.3 | 15.1 | 11.4 | 0.002 |
| SF-36 QoL (Moderate/High versus Low) | ||||||
|---|---|---|---|---|---|---|
| Physical Component | Mental Component | |||||
| OR | 95%CI | p-Value | OR | 95%CI | p-Value | |
| Gender (women versus men) | 0.86 | 0.28–2.70 | 0.799 | 0.61 | 0.21, 1.78 | 0.362 |
| Age (for each year of change) | 0.95 | 0.91–0.99 | 0.012 | 0.96 | 0.93, 1.00 | 0.057 |
| Family status (Married or Partnered versus Unmarried, Divorced, Widowed) | 3.97 | 0.91–17.3 | 0.067 | 6.59 | 1.72, 25.3 | 0.006 |
| Children (yes versus no) | 1.48 | 0.27–8.01 | 0.650 | 1.38 | 0.25, 7.46 | 0.711 |
| Education (for each level of change) | 1.02 | 0.67–1.56 | 0.913 | 0.83 | 0.55, 1.27 | 0.394 |
| Place of residence (Urban versus Rural) | 1.53 | 0.36–6.63 | 0.567 | 1.39 | 0.38, 5.08 | 0.619 |
| Monthly income (for each level of change, e.g., <€500, €500–1000 or >€1000) | 1.44 | 0.69–3.00 | 0.336 | 0.99 | 0.48, 2.07 | 0.987 |
| State Anxiety (high versus low) | 0.56 | 0.17–1.85 | 0.341 | 0.16 | 0.05, 0.57 | 0.005 |
| pseudo R2 Negelkerke | 0.265 | 0.268 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rikos, N.; Frantzeskaki, C.; Fragiadaki, M.; Kassotaki, A.; Mpalaskas, A.; Linardakis, M.; Vasilopoulos, G. Investigation of the Quality of Life of Patients with Gastrointestinal Issues Treated in the Surgical Clinic of a Regional General Hospital in Greece. Clin. Pract. 2023, 13, 520-528. https://doi.org/10.3390/clinpract13020048
Rikos N, Frantzeskaki C, Fragiadaki M, Kassotaki A, Mpalaskas A, Linardakis M, Vasilopoulos G. Investigation of the Quality of Life of Patients with Gastrointestinal Issues Treated in the Surgical Clinic of a Regional General Hospital in Greece. Clinics and Practice. 2023; 13(2):520-528. https://doi.org/10.3390/clinpract13020048
Chicago/Turabian StyleRikos, Nikos, Chara Frantzeskaki, Maria Fragiadaki, Anna Kassotaki, Andreas Mpalaskas, Manolis Linardakis, and Georgios Vasilopoulos. 2023. "Investigation of the Quality of Life of Patients with Gastrointestinal Issues Treated in the Surgical Clinic of a Regional General Hospital in Greece" Clinics and Practice 13, no. 2: 520-528. https://doi.org/10.3390/clinpract13020048
APA StyleRikos, N., Frantzeskaki, C., Fragiadaki, M., Kassotaki, A., Mpalaskas, A., Linardakis, M., & Vasilopoulos, G. (2023). Investigation of the Quality of Life of Patients with Gastrointestinal Issues Treated in the Surgical Clinic of a Regional General Hospital in Greece. Clinics and Practice, 13(2), 520-528. https://doi.org/10.3390/clinpract13020048