

The Importance of Periodic Dental Control in the Oral Health Status of Elderly Patients


 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participations
2.3. Statistical Analysis
3. Results
3.1. Epidemiological Profile
3.2. Associated Chronic Diseases
3.3. Dental Hygiene Aspects
3.4. Accessibility to, and Attendance at, the Dentist
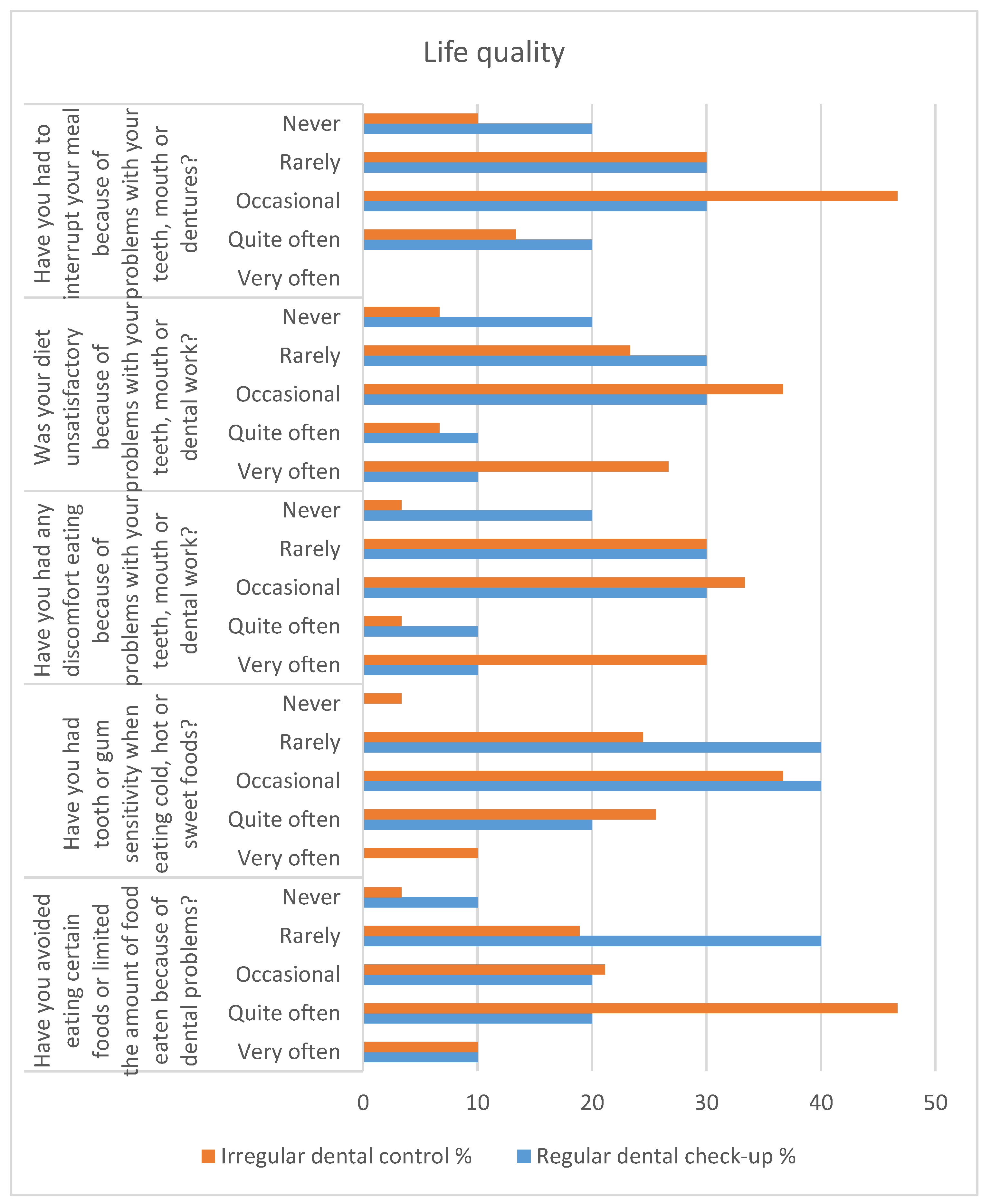
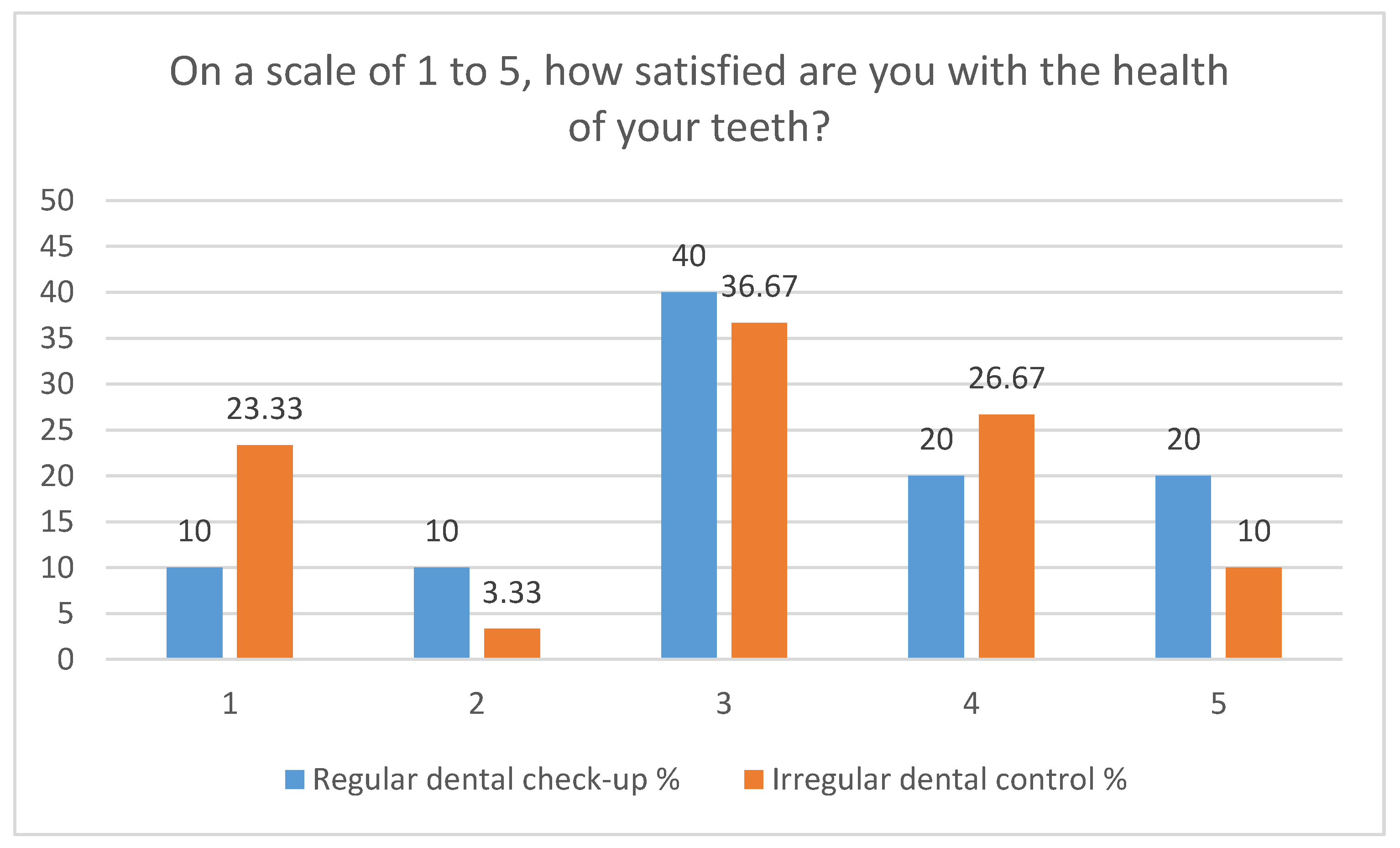
3.5. Quality of Life from a Dental Health Perspective
3.6. Dental and Endodontic Diagnosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Center for Disease Control and Prevention. The 10 Essential Public Health Services. In Public Health Emergencies; Springer Publishing Company: New York, NY, USA, 2021. Available online: https://www.cdc.gov/publichealthgateway/publichealthservices/essentialhealthservices.html (accessed on 11 May 2022).
- Leonardi, F. The Definition of Health: Towards New Perspectives. Int. J. Health Serv. 2018, 48, 735–748. [Google Scholar] [CrossRef] [PubMed]
- Berezovsky, B.; Bencko, V. Oral health in a context of public health: Prevention-related issue. Central Eur. J. Public Health 2021, 29, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Raphael, C. Oral Health and Aging. Am. J. Public Health 2017, 107, S44–S45. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Assembly Resolution Geneva: WHO. 2021. Available online: https://www.who.int/news/item/27-05-2021-world-health-assembly-resolution-paves-the-way-for-better-oral-health-care (accessed on 12 May 2022).
- Fiorillo, L. Oral Health: The First Step to Well-Being. Medicina 2019, 55, 676. [Google Scholar] [CrossRef] [PubMed]
- Dever, G.E.A. An epidemiological model for health policy analysis. Soc. Indic. Res. 1976, 2, 453–466. [Google Scholar] [CrossRef]
- Peres, M.A.; Macpherson, L.M.D.; Weyant, R.J.; Daly, B.; Venturelli, R.; Mathur, M.R.; Listl, S.; Celeste, R.K.; Guarnizo-Herreño, C.C.; Kearns, C.; et al. Oral diseases: A global public health challenge. Lancet 2019, 394, 249–260. [Google Scholar] [CrossRef]
- Lang, N.P.; Suvan, J.E.; Tonetti, M.S. Risk factor assessment tools for the prevention of periodontitis progression a systematic review. J. Clin. Periodontol. 2015, 42, S59–S70. [Google Scholar] [CrossRef]
- Dixon, J.; Manzanares-Céspedes, M.; Davies, J.; Vital, S.; Gerber, G.; Paganelli, C.; Akota, I.; Greiveldinger, A.; Murphy, D.; Quinn, B.F.; et al. O-HEALTH-EDU: A scoping review on the reporting of oral health professional education in Europe. Eur. J. Dent. Educ. 2021, 25, 56–77. [Google Scholar] [CrossRef]
- Cuculescu, M.; Slusanschi, O.; Boscaiu, V.R.; Luis, H.P.S.; Graça, S.M.F.R.; Albuquerque, T.M.B.R.E.G.D.S.; Assunção, V.; Galuscan, A.; Podariu, A.C.; Malmqvist, S.; et al. Self-reported oral health–related habits, attitudes and knowledge in adults from Portugal, Romania and Sweden—A comparative study. Int. J. Dent. Hyg. 2019, 17, 359–368. [Google Scholar] [CrossRef]
- Janto, M.; Iurcov, R.; Daina, C.M.; Neculoiu, D.C.; Venter, A.C.; Badau, D.; Cotovanu, A.; Negrau, M.; Suteu, C.L.; Sabau, M.; et al. Oral Health among Elderly, Impact on Life Quality, Access of Elderly Patients to Oral Health Services and Methods to Improve Oral Health: A Narrative Review. J. Pers. Med. 2022, 12, 372. [Google Scholar] [CrossRef]
- Brian, Z.; Weintraub, J.A. Oral Health and COVID-19: Increasing the Need for Prevention and Access. Prev. Chronic Dis. 2020, 13, E82. [Google Scholar] [CrossRef] [PubMed]
- Reda, R.; Zanza, A.; Di Nardo, D.; Bellanova, V.; Xhajanka, E.; Testarelli, L. Implant Survival Rate and Prosthetic Complications of OT Equator Retained Maxillary Overdenture: A Cohort Study. Prosthesis 2022, 4, 730–738. [Google Scholar] [CrossRef]
- Balaji, T.M.; Varadarajan, S.; Jagannathan, R.; Mahendra, J.; Fageeh, H.I.; Fageeh, H.N.; Mushtaq, S.; Baeshen, H.A.; Bhandi, S.; Gupta, A.A.; et al. Melatonin as a Topical/Systemic Formulation for the Management of Periodontitis: A Systematic Review. Materials 2021, 14, 2417. [Google Scholar] [CrossRef] [PubMed]
- Glasser, M.; Pathman, D. Education for health: What’s in a name? Educ. Health 2010, 23, 520. [Google Scholar]
- Clarkson, J.E.; Pitts, N.B.; Goulao, B.; Boyers, D.; Ramsay, C.R.; Floate, R.; Braid, H.J.; Fee, P.A.; Ord, F.S.; Worthington, H.V.; et al. Risk-based, 6-monthly and 24-monthly dental check-ups for adults: The INTERVAL three-arm RCT. Health Technol. Assess. 2020, 24, 1–138. [Google Scholar] [CrossRef] [PubMed]
- Eguchi, T.; Tada, M.; Shiratori, T.; Imai, M.; Onose, Y.; Suzuki, S.; Satou, R.; Ishizuka, Y.; Sugihara, N. Factors Associated with Undergoing Regular Dental Check-ups in Healthy Elderly Individuals. Bull. Tokyo Dent. Coll. 2018, 59, 229–236. [Google Scholar] [CrossRef]
- Thomson, W.M.; Williams, S.M.; Broadbent, J.M.; Poulton, R.; Locker, D. Long-term Dental Visiting Patterns and Adult Oral Health. J. Dent. Res. 2010, 89, 307–311. [Google Scholar] [CrossRef]
- Bots-VantSpijker, P.C.; van der Maarel-Wierink, C.D.; Schols, J.M.G.A.; Bruers, J.J.M. Provision of Oral Health Care by Dentists to Community-Dwelling Older Patients. Int. Dent. J. 2022, 72, 169–178. [Google Scholar] [CrossRef]
- Bots-VantSpijker, P.C.; van der Maarel-Wierink, C.D.; Schols, J.M.G.A.; Bruers, J.J.M. Assessed and perceived oral health of older people who visit the dental practice, an exploratory cross-sectional study. PLoS ONE 2021, 16, e0257561. [Google Scholar] [CrossRef]
- Crocombe, L.A.; Broadbent, J.M.; Thomson, W.M.; Brennan, D.S.; Poulton, R. Impact of dental visiting trajectory patterns on clinical oral health and oral health-related quality of life. J. Public Health Dent. 2012, 72, 36–44. [Google Scholar] [CrossRef]
- Koistinen, S.; Ståhlnacke, K.; Olai, L.; Ehrenberg, A.; Carlsson, E. Older people’s experiences of oral health and assisted daily oral care in short-term facilities. BMC Geriatr. 2021, 21, 388. [Google Scholar] [CrossRef] [PubMed]
- Gil-Montoya, J.A.; de Mello, A.L.F.; Barrios, R.; Gonzalez-Moles, M.A.; Bravo, M. Oral health in the elderly patient and its impact on general well-being: A nonsystematic review. Clin. Interv. Aging 2015, 10, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.M.; Chu, C.H.; Duangthip, D.; Ettinger, R.L.; Hugo, F.N.; Kettratad-Pruksapong, M.; Liu, J.; Marchini, L.; McKenna, G.; Ono, T.; et al. Global Perspectives of Oral Health Policies and Oral Healthcare Schemes for Older Adult Populations. Front. Oral Health 2021, 2, 703526. [Google Scholar] [CrossRef] [PubMed]
- Duangthip, D.; Chu, C.H. Challenges in Oral Hygiene and Oral Health Policy. Front. Oral Health 2020, 1, 575428. [Google Scholar] [CrossRef] [PubMed]
- Kotronia, E.; Brown, H.; Papacosta, A.O.; Lennon, L.T.; Weyant, R.J.; Whincup, P.H.; Wannamethee, S.G.; Ramsay, S.E. Oral health and all-cause, cardiovascular disease, and respiratory mortality in older people in the UK and USA. Sci. Rep. 2021, 11, 16452. [Google Scholar] [CrossRef]
- Petersen, P.E.; Kandelman, D.; Arpin, S.; Ogawa, H. Global oral health of older people--call for public health action. Community Dent. Health 2010, 27, 257–283. [Google Scholar]
- Müller, F.; Shimazaki, Y.; Kahabuka, F.; Schimmel, M. Oral health for an ageing population: The importance of a natural dentition in older adults. Int. Dent. J. 2017, 67, 7–13. [Google Scholar] [CrossRef]
- Shahrabani, S. Factors affecting oral examinations and dental treatments among older adults in Israel. Isr. J. Health Policy Res. 2019, 8, 43. [Google Scholar] [CrossRef]
- Scannapieco, F.A.; Bush, R.B.; Paju, S. Associations Between Periodontal Disease and Risk for Nosocomial Bacterial Pneumonia and Chronic Obstructive Pulmonary Disease. A Systematic Review. Ann. Periodontol. 2003, 8, 54–69. [Google Scholar] [CrossRef]
- Vozza, I. Oral Prevention and Management of Oral Healthcare. Int. J. Environ. Res. Public Health 2021, 18, 1970. [Google Scholar] [CrossRef]
- Oku, S.; Iyota, K.; Mizutani, S.; Otsuki, S.; Kubo, K.; Yamada, S.; Kobayashi, Y.; Kashiwazaki, H. The Association of Oral Function with Oral Health-Related Quality of Life in University Students: A Cross-Sectional Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 4863. [Google Scholar] [CrossRef] [PubMed]
- Macmahon, S. A Priority for Global Health Research; The Academy of Medical Sciences: London, UK, 2018. [Google Scholar]
- Kanungo, S.; Ghosal, S.; Kerketta, S.; Sinha, A.; Mercer, S.W.; Lee, J.T.; Pati, S. Association of Oral Health with Multimorbidity among Older Adults: Findings from the Longitudinal Ageing Study in India, Wave-1, 2017–2019. Int. J. Environ. Res. Public Health 2021, 18, 12853. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Larrañaga, A.; Vetrano, D.L.; Ferrucci, L.; Mercer, S.W.; Marengoni, A.; Onder, G.; Eriksdotter, M.; Fratiglioni, L. Multimorbidity and functional impairment-bidirectional interplay, synergistic effects and common pathways. J. Intern. Med. 2019, 285, 255–271. [Google Scholar] [CrossRef] [PubMed]
- Islas-Granillo, H.; Borges-Yañez, S.A.; Navarrete-Hernández, J.D.J.; Veras-Hernández, M.A.; Casanova-Rosado, J.F.; Minaya-Sánchez, M.; Casanova-Rosado, A.J.; Fernández-Barrera, M.; Medina-Solís, C.E. Indicators of oral health in older adults with and without the presence of multimorbidity: A cross-sectional study. Clin. Interv. Aging 2019, 14, 219–224. [Google Scholar] [CrossRef] [PubMed]
- Dawoud, B.E.S.; Roberts, A.; Yates, J.M. Drug interactions in general dental practice—Considerations for the dental practitioner. Br. Dent. J. 2014, 216, 15–23. [Google Scholar] [CrossRef]
- Mohan, S. Prime Drug Interplay in Dental Practice. J. Clin. Diagn. Res. 2016, 10, ZE07–ZE11. [Google Scholar] [CrossRef]
- Sicca, C.; Bobbio, E.; Quartuccio, N.; Nicolò, G.; Cistaro, A. Prevention of dental caries: A review of effective treatments. J. Clin. Exp. Dent. 2016, 8, e604–e610. [Google Scholar] [CrossRef]
- Al-Qahtani, S.M.; Razak, P.A.; Khan, S.D. Knowledge and Practice of Preventive Measures for Oral Health Care among Male Intermediate Schoolchildren in Abha, Saudi Arabia. Int. J. Environ. Res. Public Health 2020, 17, 703. [Google Scholar] [CrossRef]
- Wagle, M.; Acharya, G.; Basnet, P.; Trovik, T.A. Knowledge about preventive dentistry versus self-reported competence in providing preventive oral healthcare—A study among Nepalese dentists. BMC Oral Health 2017, 17, 76. [Google Scholar] [CrossRef]
- Winkelmann, J.; Gómez Rossi, J.; van Ginneken, E. Oral Health Care in Europe: Financing, Access and Provision. Health Syst. Transit. 2022, 24, 1–176. [Google Scholar] [CrossRef]
- Bernabé, E.; Masood, M.; Vujicic, M. The impact of out-of-pocket payments for dental care on household finances in low and middle income countries. BMC Public Health 2017, 17, 109. [Google Scholar] [CrossRef] [PubMed]
- Ghanbarzadegan, A.; Balasubramanian, M.; Luzzi, L.; Brennan, D.; Bastani, P. Inequality in dental services: A scoping review on the role of access toward achieving universal health coverage in oral health. BMC Oral Health 2021, 21, 404. [Google Scholar] [CrossRef]
- Institutul Național de Statistică, Activitatea Rețelei Sanitare și de Ocrotirea Sănătății în Anul 2020. Available online: https://insse.ro/cms/ro/content/activitatea-re%C8%9Belei-sanitare-%C8%99i-de-ocrotire-s%C4%83n%C4%83t%C4%83%C8%9Bii-%C3%AEn-anul-2020 (accessed on 22 May 2022).
- Healthcare Activities Statistics—Consultations. Europa.eu. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Healthcare_activities_statistics_-_consultations&oldid=542567 (accessed on 24 May 2022).
- Vinereanu, A.; Munteanu, A.; Stănculescu, A.; Farcașiu, A.T.; Didilescu, A.C. Ecological Study on the Oral Health of Romanian Intellectually Challenged Athletes. Healthcare 2022, 10, 140. [Google Scholar] [CrossRef] [PubMed]
- Bodogai, S.I.; Cutler, S.J. Aging in Romania: Research and Public Policy. Gerontologist 2014, 54, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Bobocea, L.; Gheorghe, I.R.; Spiridon, S.; Gheorghe, C.M.; Purcarea, V.L. The management of health care service quality. A physician perspective. J. Med. Life 2016, 9, 149–152. [Google Scholar] [PubMed]
- Spanemberg, J.C.; Cardoso, J.A.; Slob, E.M.G.B.; López-López, J. Quality of life related to oral health and its impact in adults. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 234–239. [Google Scholar] [CrossRef]
- Zucoloto, M.L.; Maroco, J.; Campos, J.A.D.B. Impact of oral health on health-related quality of life: A cross-sectional study. BMC Oral Health 2016, 16, 216–224. [Google Scholar] [CrossRef]
- Ogunsuji, O.O.; Dosumu, E.B.; Dairo, M.D.; Ogunsuji, A.I. Self assessment of oral health and risk factors affecting oral hygiene status in adolescents attending dental clinic in University College Hospital, Ibadan. Ann. Ib. Postgrad Med. 2021, 19, 70–77. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8935677 (accessed on 26 January 2023).
- Lertpimonchai, A.; Rattanasiri, S.; Arj-Ong Vallibhakara, S.; Attia, J.; Thakkinstian, A. The association between oral hygiene and periodontitis: A systematic review and meta-analysis. Int. Dent. J. 2017, 67, 332–343. [Google Scholar] [CrossRef]
- Goel, P.; Singh, K.; Kaur, A.; Verma, M. Oral healthcare for elderly: Identifying the needs and feasible strategies for service provision. Indian J. Dent. Res. 2006, 17, 11. [Google Scholar] [CrossRef]
- Druică, E.; Mihăilă, V.; Burcea, M.; Cepoi, V. Combining Direct and Indirect Measurements to Assess Patients’ Satisfaction with the Quality of Public Health Services in Romania: Uncovering Structural Mechanisms and Their Implications. Int. J. Environ. Res. Public Health 2019, 17, 152. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Questionnaire. Section 1 | Periodic Dental Control | * p | Chi2 (df) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Periodic | Non-Periodic | Total | |||||||
| No. | % | No. | % | No. | % | ||||
| Age (years) | 65–69 | 15 | 50.00 | 65 | 72.22 | 80 | 66.67 | 0.02 | 18.462 (4) |
| 70–74 | 15 | 50.00 | 9 | 10.00 | 24 | 20.00 | * <0.001 | ||
| 75–79 | 0 | 0 | 9 | 10.00 | 9 | 7.50 | * 0.07 | ||
| 80–84 | 0 | 0 | 6 | 6.67 | 6 | 5.00 | 0.14 | ||
| 85–89 | 0 | 0 | 1 | 1.11 | 1 | 0.83 | 0.56 | ||
| Gender | female | 19 | 63.3 | 50 | 55.5 | 69 | 57.5 | * <0.001 | 1.327 (10) |
| male | 11 | 26.7 | 40 | 44.5 | 51 | 42.5 | * <0.001 | ||
| Environment | urban | 23 | 76.7 | 34 | 37.8 | 57 | 47.5 | * <0.001 | 1.273 (1) |
| rural | 7 | 23.3 | 56 | 62.2 | 63 | 52.5 | * <0.001 | ||
| Education | primary | 0 | 0 | 6 | 6.67 | 6 | 5.00 | 0.14 | 3.528 (2) |
| medium | 15 | 50.00 | 69 | 76.67 | 84 | 70.00 | * 0.006 | ||
| higher | 15 | 50.00 | 15 | 16.67 | 30 | 25.00 | * 0.003 | ||
| Income (EUR) | <100 | 3 | 10.00 | 0 | 0.00 | 3 | 2.50 | * 0.002 | 6.672 (3) |
| 100–300 | 6 | 20.00 | 45 | 50.00 | 51 | 42.50 | * 0.004 | ||
| 300–600 | 18 | 60.00 | 42 | 46.67 | 60 | 50.00 | 0.2 | ||
| 600–1000 | 3 | 10.00 | 3 | 3.33 | 6 | 5.00 | 0.14 | ||
| Questionnaire. Section 2 | Periodic Dental Control | * p | Chi2 (df) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Periodic | Non-Periodic | Total | ||||||||
| No. | % | No. | % | No. | % | |||||
| Chronic diseases | Yes | 12 | 40.00 | 48 | 53.33 | 60 | 50.00 | 0.2 | 1.200 (1) | |
| No | 18 | 60.00 | 42 | 46.67 | 60 | 50.00 | ||||
| Type of chronic diseases | respiratory | 0 | 0 | 3 | 3.33 | 3 | 5.00 | 0.31 | 31.250 (5) | |
| cardiovascular | 9 | 30.00 | 33 | 36.67 | 42 | 70.00 | 0.50 | |||
| oncologic | 0 | 0 | 3 | 3.33 | 3 | 5,00 | 0.31 | |||
| gastrointestinal | 3 | 10.00 | 3 | 3.33 | 6 | 10.00 | 0.14 | |||
| endocrinologic | 0 | 0 | 3 | 3.33 | 3 | 5.00 | 0.31 | |||
| rheumatologic | 0 | 0 | 3 | 3.33 | 3 | 5.00 | 0.31 | |||
| Daily consumption of drugs | Yes | 18 | 60.00 | 54 | 60.00 | 72 | 60.00 | 1 | 1.125 (1) | |
| No | 12 | 40.00 | 36 | 40.00 | 48 | 40.00 | ||||
| Number of drugs administered daily | Between 1 and 3 | 12 | 40.00 | 33 | 36.67 | 45 | 63.61 | 0.74 | 8.909 (3) | |
| Between 4 and 7 | 6 | 20.00 | 12 | 13.33 | 18 | 25.00 | 0.37 | |||
| Between 7 and 10 | 0 | 0 | 3 | 3.33 | 3 | 4.16 | 0.31 | |||
| Over 11 | 0 | 0 | 6 | 6.67 | 6 | 8.33 | 0.14 | |||
| Consumption of drugs for dental pain last month | Yes | 6 | 20.00 | 33 | 36.67 | 39 | 32.50 | 0.09 | 1.845 (1) | |
| No | 24 | 80.00 | 57 | 63.33 | 81 | 67.50 | ||||
| Questionnaire. Section 3 | Periodic Dental Control | * p | Chi2 (df) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Periodic | Non-Periodic | Total | |||||||
| No. | % | No. | % | No. | % | ||||
| Dental hygiene—products | only with water/rinse the mouth | 0 | 0 | 9 | 10.00 | 9 | 7.50 | 0.07 | 18.087 (3) |
| with toothpaste and toothbrush | 30 | 100 | 72 | 80.00 | 102 | 8.50 | * 0.008 | ||
| I use mouthwash | 3 | 10.00 | 3 | 3.33 | 6 | 5.00 | 1 | ||
| I use dental floss | 0 | 0 | 3 | 3.33 | 3 | 2.500 | 0.31 | ||
| I use toothpicks | 0 | 0 | 0 | 0 | 0 | 0 | 1 | ||
| Dental hygiene—frequency | daily | 30 | 100 | 75 | 83.33 | 105 | 87.50 | * 0.01 | 20.957 (3) |
| 1 time a day | 18 | 60.00 | 66 | 73.33 | 84 | 70.00 | 0.16 | ||
| 2 times a day | 12 | 40.00 | 9 | 10.00 | 21 | 17.50 | * 0.000 | ||
| after every meal | 0 | 0 | 0 | 0 | 0 | 0 | 1 | ||
| occasionally | 0 | 0 | 15 | 16.67 | 15 | 12.50 | * 0.01 | ||
| Brushing your teeth in the evening | Never | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 14.609 (3) |
| Very rare | 6 | 20.00 | 30 | 33.33 | 36 | 30.00 | * 0.017 | ||
| Once in a while | 3 | 10.00 | 27 | 30.00 | 30 | 25.00 | * 0.02 | ||
| Almost every night | 6 | 20.00 | 15 | 16.67 | 21 | 17.50 | 0.67 | ||
| Every night | 15 | 50.00 | 18 | 20.00 | 33 | 27.50 | * 0.001 | ||
| The toothbrush used is | Hard/rough | 3 | 10.00 | 3 | 3.33 | 6 | 5.00 | 0.14 | 9.870 (4) |
| Medium | 18 | 60.00 | 51 | 56.67 | 69 | 57.50 | 0.75 | ||
| Soft | 6 | 20.00 | 6 | 6.67 | 12 | 10.00 | * 0.03 | ||
| Electric | 0 | 0 | 0 | 0 | 0 | 0 | 1 | ||
| I do not know | 3 | 10.00 | 21 | 23.33 | 24 | 20.00 | 0.11 | ||
| Non-respondents | 0 | 0 | 9 | 10.00 | 9 | 7.50 | 0.07 | ||
| How often do you change your toothbrush? | At 3 months | 15 | 50.00 | 24 | 26.67 | 39 | 32.50 | * 0.01 | 9.636 (3) |
| Once a year | 0 | 0 | 12 | 13.33 | 12 | 10.00 | * 0.03 | ||
| When needed | 15 | 50.00 | 45 | 50.00 | 60 | 50.00 | 1 | ||
| Non-respondents | 0 | 0 | 9 | 10.00 | 9 | 7.50 | 0.07 | ||
| Used toothpaste | With fluoride | 9 | 30.00 | 18 | 20.00 | 27 | 22.50 | 0.25 | 16.909 (4) |
| Without fluoride | 0 | 0 | 3 | 3.33 | 3 | 2.50 | 0.31 | ||
| Special for gums | 9 | 30.00 | 21 | 23.33 | 30 | 25.00 | 0.46 | ||
| I do not know | 12 | 40.00 | 39 | 43.33 | 41 | 34.16 | 0.75 | ||
| Non-respondents | 0 | 0 | 9 | 10.00 | 9 | 7.50 | 0.07 | ||
| Bleeding occurs when brushing teeth | Yes | 12 | 40.00 | 42 | 46.67 | 54 | 45.00 | 0.52 0.54 | 8.364 (2) |
| No | 18 | 60.00 | 39 | 43.33 | 57 | 47.50 | |||
| Non-respondents | 0 | 0 | 9 | 10.00 | 9 | 7.50 | 0.07 | ||
| Did you have dental problems as a child? | Never | 0 | 0 | 3 | 3.33 | 3 | 2.50 | 0.31 | 14.043 (4) |
| Rarely | 3 | 10.00 | 24 | 26.67 | 27 | 22.50 | * 0.05 | ||
| Sometimes | 15 | 50.00 | 27 | 30.00 | 42 | 35.00 | * 0.04 | ||
| Often | 9 | 30.00 | 33 | 36.67 | 42 | 35.00 | 0.5 | ||
| Very often | 3 | 10.00 | 3 | 3.33 | 6 | 5.00 | 0.14 | ||
| Where you can find out what you need to know about oral health | From the dentist | 24 | 80.00 | 48 | 53.33 | 72 | 60.00 | * 0.01 | 17.783 (4) |
| From the TV | 6 | 20.00 | 24 | 26.67 | 30 | 25.00 | 0.46 | ||
| From the internet | 0 | 0 | 6 | 6.67 | 6 | 5.00 | 0.14 | ||
| Other sources | 0 | 0 | 6 | 6.67 | 6 | 5.00 | 0.14 | ||
| Non-respondents | 0 | 0 | 6 | 6.67 | 6 | 5.00 | 0.14 | ||
| Questionnaire | Periodic Dental Control | * p | Chi2 (df) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Periodic | Non-Periodic | Total | ||||||||
| No. | % | No. | % | No. | % | |||||
| What prevents you from getting to the dentist as often as you would like? | Fear | 3 | 10.00 | 21 | 23.33 | 24 | 20.00 | 0.11 | 12.45 (5) | |
| Unpleasant experiences in the past | 6 | 20.00 | 9 | 10.00 | 15 | 12.50 | 0.15 | |||
| Difficult access | 0 | 0 | 9 | 10.00 | 9 | 7.50 | 0.07 | |||
| Lack of money | 12 | 40.00 | 21 | 23.33 | 24 | 20.00 | 0.07 | |||
| It is not necessary | 9 | 30.00 | 24 | 26.67 | 33 | 27.50 | 0.72 | |||
| Non-respondents | 0 | 0 | 6 | 6.67 | 6 | 5.00 | 0.14 | |||
| Why do you go to the dentist more often? | Toothache | 9 | 30.00 | 42 | 46.67 | 51 | 4,50 | 0.11 | 23.618 (8) | |
| Gum pain | 3 | 10.00 | 6 | 6.67 | 9 | 7.50 | 0.55 | |||
| Bleeding gums | 3 | 10.00 | 0 | 0 | 3 | 2.50 | * 0.002 | |||
| Scaling | 0 | 0 | 0 | 0 | 0 | 0 | 1 | |||
| Caries treatment | 6 | 20.00 | 9 | 10.00 | 15 | 12.50 | 0.15 | |||
| Dental extractions | 3 | 10.00 | 6 | 6.67 | 12 | 10.00 | 0.55 | |||
| Prosthetic works | 6 | 20.00 | 6 | 6.67 | 12 | 10.00 | * 0.03 | |||
| Problems with dentures | 0 | 0 | 15 | 16.67 | 15 | 12.50 | * 0.01 | |||
| Non-respondents | 0 | 0 | 6 | 6.67 | 6 | 5.00 | 0.14 | |||
| Do you usually go to the same dentist? | Yes | 27 | 90.00 | 75 | 83.33 | 103 | 85.83 | 0.37 | 6.358 (2) | |
| No | 3 | 10.00 | 9 | 10.00 | 12 | 10.00 | 1 | |||
| Non-respondents | 0 | 0 | 6 | 6.67 | 6 | 5.00 | 0.14 | |||
| Do you consider regular checkups at the dentist important? | Yes | 30 | 100 | 72 | 80.00 | 102 | 85.00 | * 0.008 | 5.289 (2) | |
| No | 0 | 0 | 9 | 10.00 | 9 | 7.50 | 0.07 | |||
| Non-respondents | 0 | 0 | 9 | 10.00 | 9 | 7.50 | 0.07 | |||
| Questionnaire | Periodic Dental Control | * p | Chi2 (df) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Periodic | Non-Periodic | Total | ||||||||
| Nr. | % | Nr. | % | No. | % | |||||
| Dental diagnosis | Simple caries | Yes | 6 | 20 | 12 | 13.33 | 18 | 15.00 | 0.37 | 1.537 (1) |
| No | 24 | 80 | 78 | 83.33 | 102 | 85.00 | ||||
| Complicated caries | Yes | 15 | 50 | 48 | 53.33 | 63 | 52.50 | 0.75 | 1.397 (1) | |
| No | 15 | 50 | 39 | 43.33 | 54 | 45.00 | ||||
| Endodontic diagnosis | Inflammatory hyperemia | Yes | 6 | 20 | 37 | 41.11 | 43 | 35.83 | * 0.03 | 1.386 (1) |
| No | 24 | 80 | 53 | 58.89 | 77 | 64.17 | ||||
| Pulpitis | Yes | 8 | 26.67 | 31 | 34.44 | 39 | 32.50 | 0.43 | 6.341 (3) | |
| No | 22 | 73.33 | 59 | 65.56 | 81 | 67.50 | ||||
| Serous | 5 | 62.5 | 17 | 54.83 | 22 | 18.33 | 0.46 | |||
| Purulent | 3 | 37.5 | 14 | 45.17 | 17 | 14.17 | 0.46 | |||
| Apical periodontitis | Yes | 21 | 70 | 67 | 74.44 | 88 | 73.33 | 0.63 | 5.498 (3) | |
| No | 9 | 30 | 23 | 25.56 | 32 | 26.67 | ||||
| Acute | 17 | 80.95 | 31 | 46.27 | 48 | 40.00 | * 0.001 | |||
| Chronic | 4 | 19.05 | 36 | 53.73 | 40 | 33.33 | * 0.001 | |||
| Pulp necrosis | Yes | 4 | 13.33 | 24 | 26.67 | 28 | 23.33 | 0.13 | 1.382 (1) | |
| No | 26 | 86.67 | 66 | 73.33 | 92 | 76.67 | ||||
| Pulpal gangrene | Yes | 9 | 30 | 34 | 37.78 | 43 | 35.83 | 0.44 | 1.417 (1) | |
| No | 21 | 70 | 56 | 62.22 | 77 | 64.16 | ||||
| Prosthetic diagnosis | The edentation class | 1 | 3 | 10.00 | 27 | 30.00 | 30 | 25.00 | * 0.02 | 4.387 (3) |
| 2 | 9 | 30.00 | 18 | 20.00 | 27 | 22.50 | 0.25 | |||
| 3 | 18 | 60.00 | 42 | 46.67 | 60 | 50.00 | * 0.04 | |||
| 6 | 0 | 0.00 | 3 | 3.33 | 3 | 2.50 | 0.33 | |||
| Prosthetic works | Yes | 21 | 70.00 | 57 | 63.33 | 78 | 65.00 | 0.5 | 1.265 (1) | |
| No | 9 | 30.00 | 33 | 36.67 | 42 | 35.00 | ||||
| Periodontal diagnosis | Simple chronic gingivitis | Yes | 9 | 30.00 | 30 | 33.33 | 39 | 32.50 | 0.73 | 1.421 (1) |
| No | 21 | 70.00 | 60 | 66.67 | 81 | 67.50 | ||||
| Chronic marginal periodontitis | Yes | 12 | 40.00 | 54 | 60.00 | 66 | 55.00 | 0.05 | 1.257 (1) | |
| No | 18 | 60.00 | 36 | 40.00 | 54 | 45.00 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janto, M.; Iurcov, R.; Daina, C.M.; Venter, A.C.; Suteu, C.L.; Sabau, M.; Badau, D.; Daina, L.G. The Importance of Periodic Dental Control in the Oral Health Status of Elderly Patients. Clin. Pract. 2023, 13, 537-552. https://doi.org/10.3390/clinpract13020050
Janto M, Iurcov R, Daina CM, Venter AC, Suteu CL, Sabau M, Badau D, Daina LG. The Importance of Periodic Dental Control in the Oral Health Status of Elderly Patients. Clinics and Practice. 2023; 13(2):537-552. https://doi.org/10.3390/clinpract13020050
Chicago/Turabian StyleJanto, Michael, Raluca Iurcov, Cristian Marius Daina, Alina Cristiana Venter, Corina Lacramioara Suteu, Monica Sabau, Dana Badau, and Lucia Georgeta Daina. 2023. "The Importance of Periodic Dental Control in the Oral Health Status of Elderly Patients" Clinics and Practice 13, no. 2: 537-552. https://doi.org/10.3390/clinpract13020050
APA StyleJanto, M., Iurcov, R., Daina, C. M., Venter, A. C., Suteu, C. L., Sabau, M., Badau, D., & Daina, L. G. (2023). The Importance of Periodic Dental Control in the Oral Health Status of Elderly Patients. Clinics and Practice, 13(2), 537-552. https://doi.org/10.3390/clinpract13020050