
Can Secondary Adhesive Capsulitis Complicate Calcific Tendinitis of the Rotator Cuff? An Ultrasound Imaging Analysis

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ultrasound Equipment
2.2. Ultrasound Analysis
- -
- The presence of calcific deposit and its location;
- -
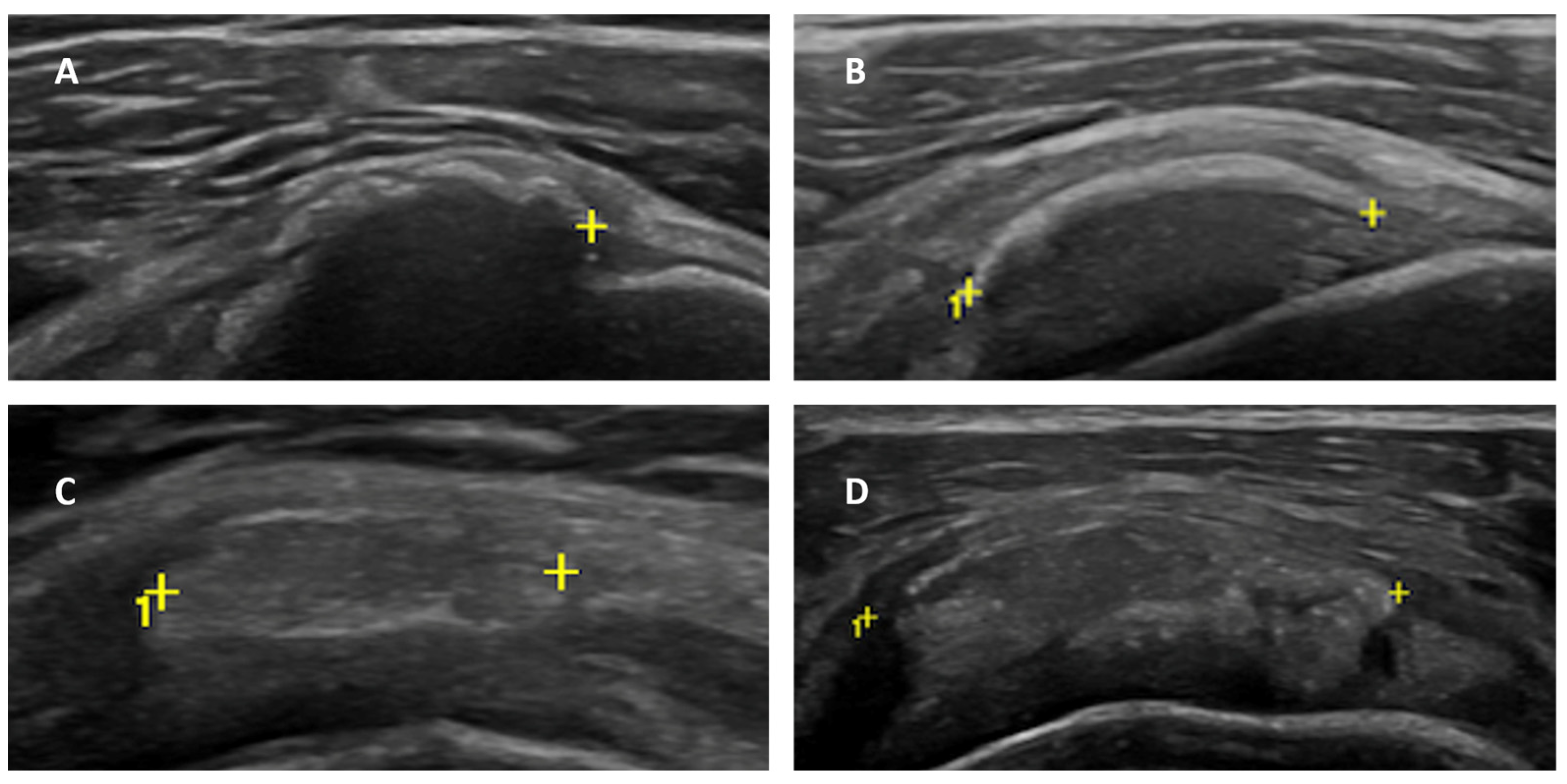
- Calcific deposit maturation stage, according to the classification proposed by Chiou et al. [21]: stage I (arc-shaped with complete posterior acoustic shadowing), stage II (fragmented or punctate with partial posterior acoustic shadowing), stage III (nodular, without posterior shadowing) and stage IV (echogenic with cystic degenerative areas and without posterior shadowing);
- -
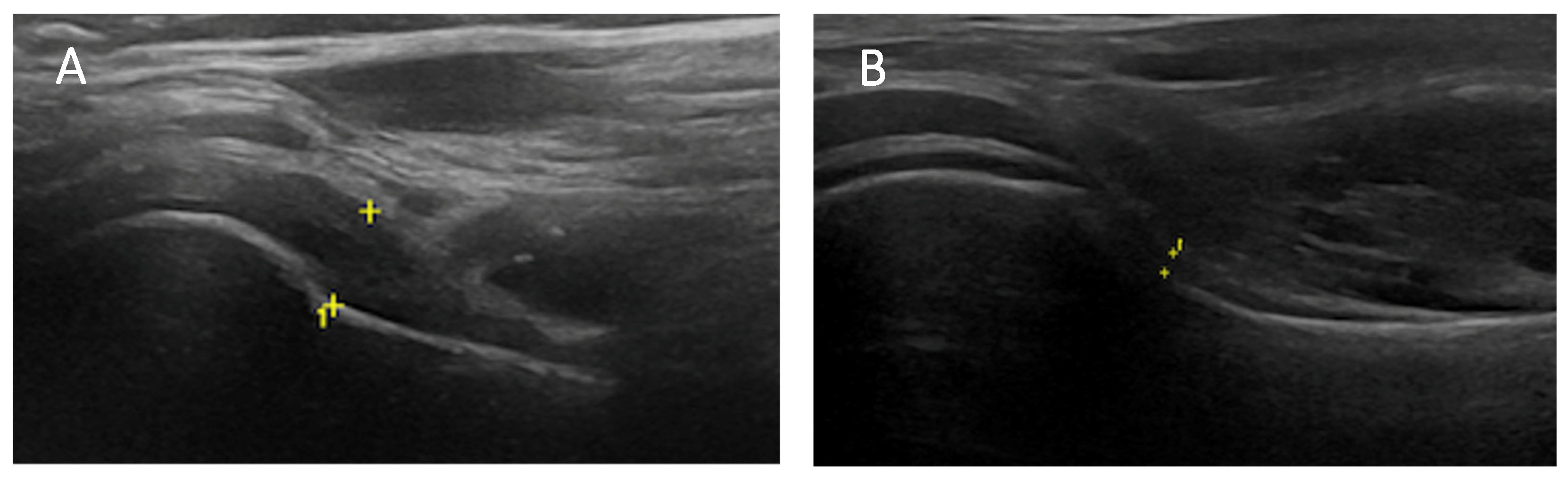
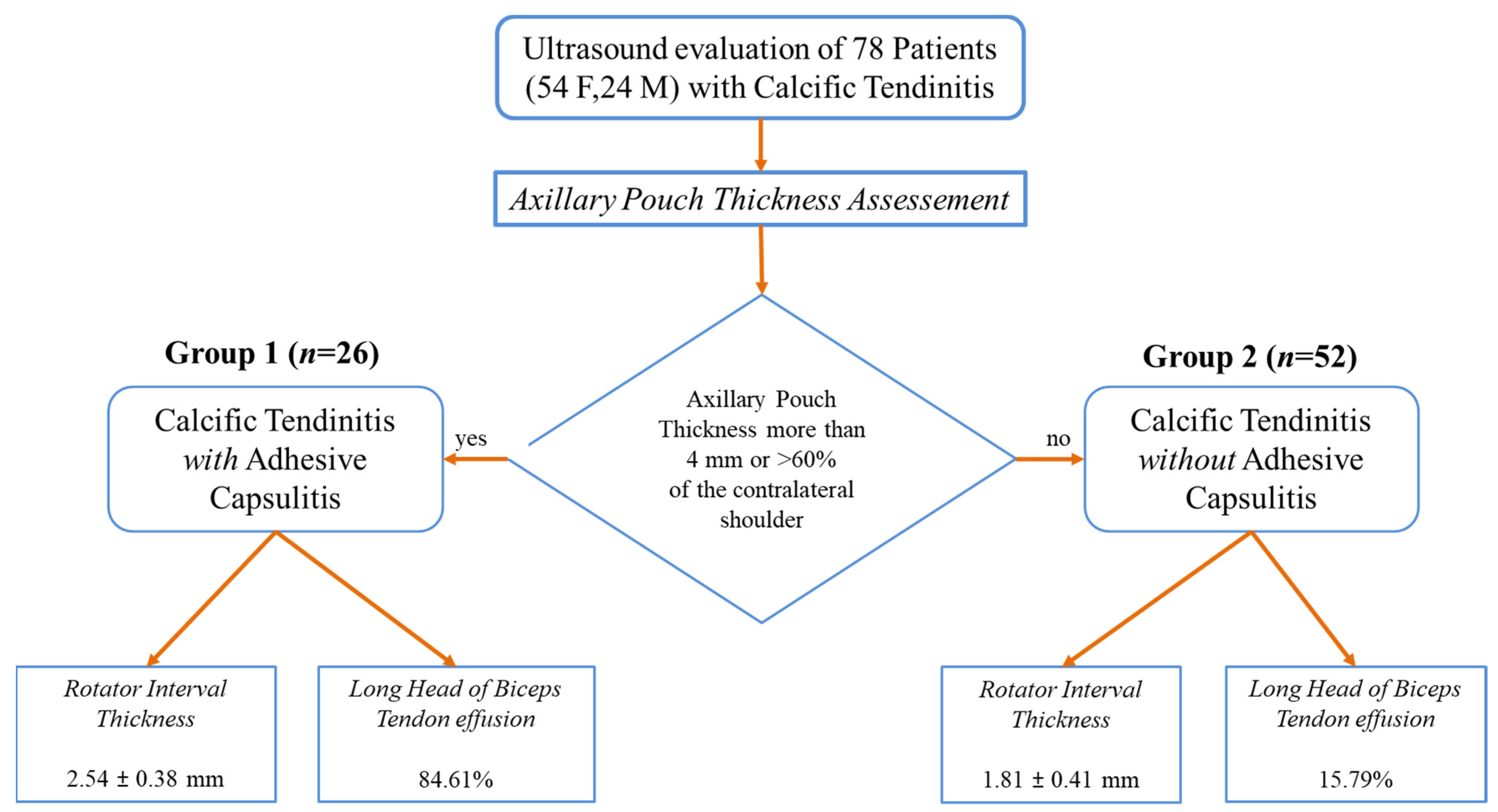
- Axillary pouch (AP) maximum thickness: evaluated in the supine or sitting position with the probe placed longitudinally on the mid-axillary line along the neck of the humerus;
- -
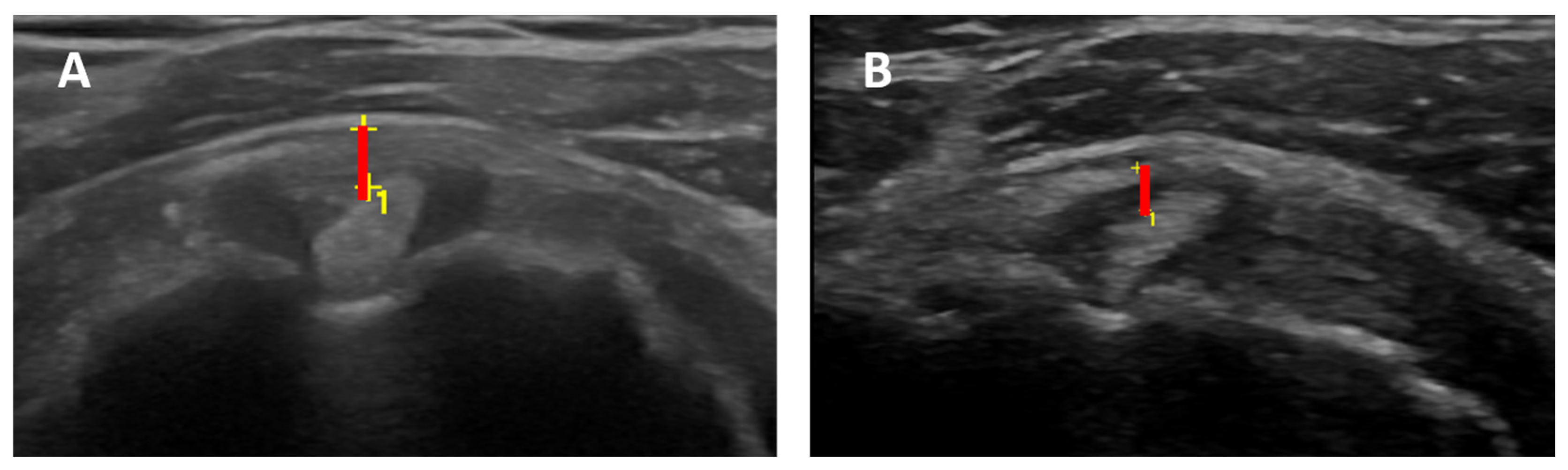
- Rotator interval (RI) maximum thickness: evaluated in the sitting position with the arm in a neutral position, elbow flexed, and hand palm on the knee. RI thickness was evaluated in a scan that included LHBT, supraspinatus, and subscapularis tendons by measuring the distance between LHBT outer contour and peri bursal fat;
- -
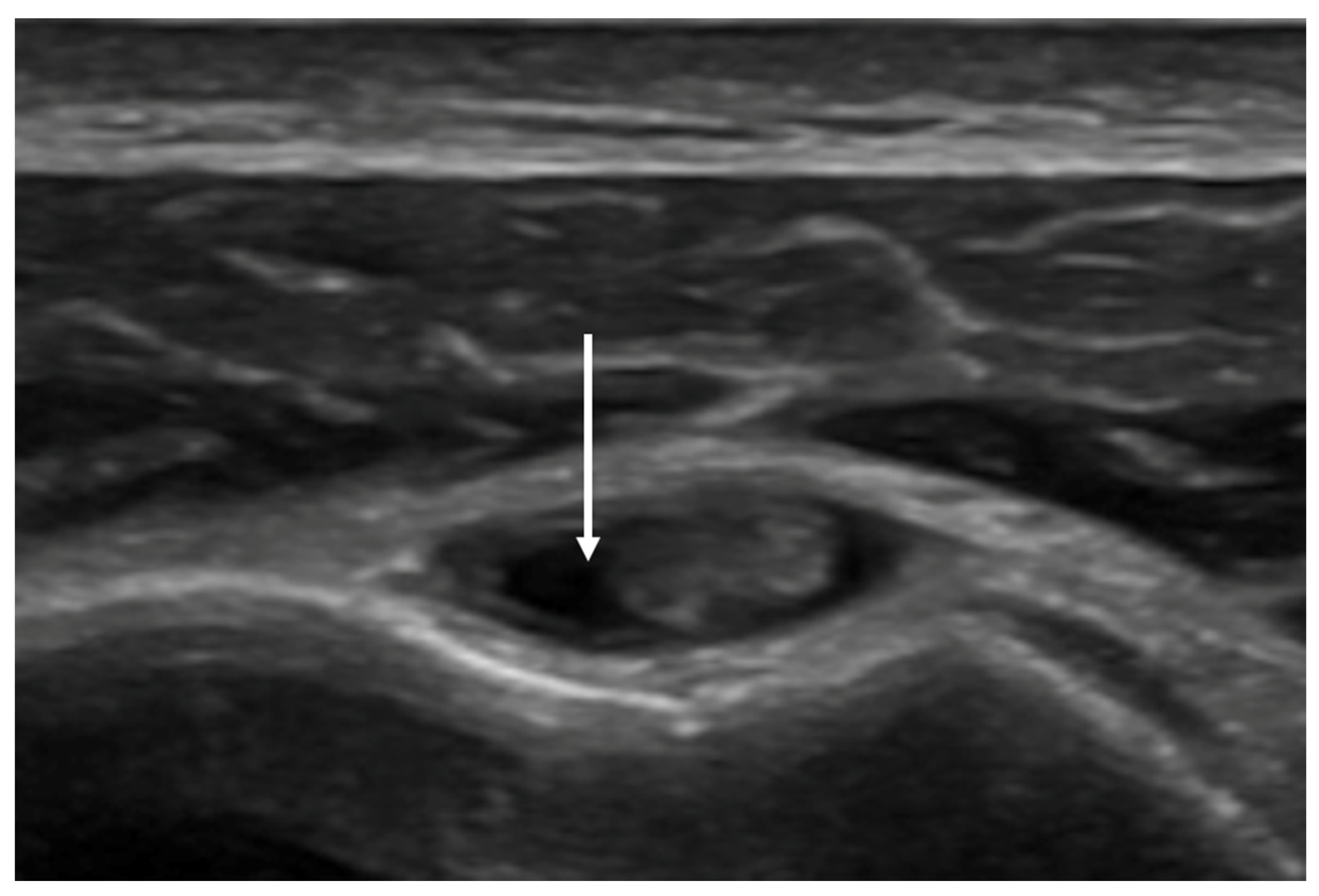
- Effusion within the LHBT sheath: evaluated in the same position of the RI, with the probe placed in the axial plane in the bicipital groove.
2.3. Statistical Analysis
2.4. Clinical Assessment
2.5. Ethics
3. Results
3.1. Patients Demographics
3.2. Calcific Deposit Maturation Stage
3.3. Axillary Pouch (AP) Thickness
3.4. Rotator Interval (RI) Thickness and Effusion within the LHBT Sheath
3.5. Clinical Notes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Darrieutort-Laffite, C.; Blanchard, F.; Le Goff, B. Calcific tendonitis of the rotator cuff: From formation to resorption. Jt. Bone Spine 2018, 85, 687–692. [Google Scholar] [CrossRef]
- Delbello, F.; Spinnato, P.; Gomez, M.P.A. Calcific Tendinopathy Atypically Located Outside the Rotator Cuff: A Systematic Review. Curr. Med. Imaging Former. Curr. Med. Imaging Rev. 2023, 20, e100423215585. [Google Scholar] [CrossRef]
- Chianca, V.; Albano, D.; Messina, C.; Midiri, F.; Mauri, G.; Aliprandi, A.; Catapano, M.; Pescatori, L.C.; Monaco, C.G.; Gitto, S.; et al. Rotator cuff calcific tendinopathy: From diagnosis to treatment. Acta Biomed. 2018, 89, 186–196. [Google Scholar] [CrossRef]
- Saran, S.; Babhulkar, J.A.; Gupta, H.; Chari, B. Imaging of calcific tendinopathy: Natural history, migration patterns, pitfalls and management: A review. Br. J. Radiol. 2024; Online ahead of print. [Google Scholar] [CrossRef]
- Vinanti, G.B.; Pavan, D.; Rossato, A.; Biz, C. Atypical localizations of calcific deposits in the shoulder. Int. J. Surg. Case Rep. 2015, 10, 206–210. [Google Scholar] [CrossRef]
- Ponti, F.; Parmeggiani, A.; Martella, C.; Facchini, G.; Spinnato, P. Imaging of calcific tendinopathy in atypical sites by ultrasound and conventional radiography: A pictorial essay. Med. Ultrason. 2022, 24, 235–241. [Google Scholar] [CrossRef]
- Dukan, R.; Amsallem, L.; Silvera, J.; Masmejean, E.H. Atypical Localization of Calcific Shoulder Tendinopathy: Humeral Insertion of the Pectoralis Major. J. Orthop. Case Rep. 2020, 10, 44–48. [Google Scholar] [CrossRef]
- Albano, D.; Coppola, A.; Gitto, S.; Rapisarda, S.; Messina, C.; Sconfienza, L.M. Imaging of calcific tendinopathy around the shoulder: Usual and unusual presentations and common pitfalls. Radiol. Med. 2021, 126, 608–619. [Google Scholar] [CrossRef]
- Malghem, J.; Omoumi, P.; Lecouvet, F.; Vande Berg, B. Intraosseous migration of tendinous calcifications: Cortical erosions, subcortical migration and extensive intramedullary diffusion, a SIMS series. Skeletal Radiol. 2015, 44, 1403–1412. [Google Scholar] [CrossRef]
- Cho, J.H.; Jung, S.H.; Yang, S.M.; Park, H. Atypical calcific tendinitis involving the long biceps tendon: A rare cause of hemiplegic shoulder pain. J. Back Musculoskelet. Rehabil. 2019, 32, 355–359. [Google Scholar] [CrossRef]
- Al-Khudairi, R.; Maris, A.; Khurram, R.; Tsamados, S.; Farrant, J.; Armstrong, T.M. Gluteus medius calcific tendonitis as a cause of severe anterior hip pain. Radiol. Case Rep. 2023, 19, 1004–1007. [Google Scholar] [CrossRef]
- Dimmick, S.; Hayter, C.; Linklater, J. Acute calcific periarthritis—A commonly misdiagnosed pathology. Skeletal Radiol. 2022, 51, 1553–1561. [Google Scholar] [CrossRef]
- Merolla, G.; Bhat, M.G.; Paladini, P.; Porcellini, G. Complications of calcific tendinitis of the shoulder: A concise review. J. Orthop. Traumatol. 2015, 16, 175–183. [Google Scholar] [CrossRef]
- Fields, B.K.K.; Skalski, M.R.; Patel, D.B.; White, E.A.; Tomasian, A.; Gross, J.S.; Matcuk, G.R. Adhesive capsulitis: Review of imaging findings, pathophysiology, clinical presentation, and treatment options. Skelet. Radiol. 2019, 48, 1171–1184. [Google Scholar] [CrossRef]
- Ricci, M. Adhesive capsulitis: A review for clinicians. JAAPA 2021, 34, 12–14. [Google Scholar] [CrossRef]
- Spinnato, P.; Masuzzo, O.; Tuè, G.; Tucci, F.; Bevere, A.; Vita, F.; Cavallo, M.; Marinelli, A.; Miceli, M. A Novel Ultrasound-Guided Interventional Procedure for the Combined Treatment of Rotator Cuff Calcific Tendinopathy Complicated with Adhesive Capsulitis: The ‘Rizzoli’ Technique. Acad. Radiol. 2023, 30, 2437–2438. [Google Scholar] [CrossRef]
- Chen, S.; Chou, P.; Lue, Y.; Lu, Y. Treatment for frozen shoulder combined with calcific tendinitis of the supraspinatus. Kaohsiung J. Med. Sci. 2008, 24, 78–84. [Google Scholar] [CrossRef]
- Papalexis, N.; Parmeggiani, A.; Facchini, G.; Miceli, M.; Carbone, G.; Cavallo, M.; Spinnato, P. Current concepts in the diagnosis and treatment of adhesive capsulitis: Role of diagnostic imaging and ultrasound-guided interventional procedures. Radiol. Med. 2022, 127, 1390–1399. [Google Scholar] [CrossRef]
- Stella, S.M.; Gualtierotti, R.; Ciampi, B.; Trentanni, C.; Sconfienza, L.M.; Del Chiaro, A.; Pacini, P.; Miccoli, M.; Galletti, S. Ultrasound Features of Adhesive Capsulitis. Rheumatol. Ther. 2021, 9, 481–495. [Google Scholar] [CrossRef]
- Lee, B.C.; Yeo, S.M.; Do, J.G.; Hwang, J.H. Sequential Ultrasound Assessment of Peri-Articular Soft Tissue in Adhesive Capsulitis of the Shoulder: Correlations with Clinical Impairments-Sequential Ultrasound in Adhesive Capsulitis. Diagnostics 2022, 12, 2231. [Google Scholar] [CrossRef]
- Chiou, H.J.; Chou, Y.H.; Wu, J.J.; Hsu, C.C.; Huang, D.Y.; Chang, C.Y. Evaluation of calcific tendonitis of the rotator cuff: Role of color Doppler ultrasonography. J. Ultrasound. Med. 2002, 21, 289–297. [Google Scholar] [CrossRef]
- Picasso, R.; Pistoia, F.; Zaottini, F.; Marcenaro, G.; Miguel-Pérez, M.; Tagliafico, A.S.; Martinoli, C. Adhesive Capsulitis of the Shoulder: Current Concepts on the Diagnostic Work-Up and Evidence-Based Protocol for Radiological Evaluation. Diagnostics 2023, 13, 3410. [Google Scholar] [CrossRef]
- Soussahn, S.; Hu, D.; Durieux, J.; Kosmas, C.; Faraji, N. Adhesive capsulitis: Utility of magnetic resonance imaging as a primary diagnostic tool and clinical management support. Curr. Probl. Diagn. Radiol. 2024. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Sconfienza, L.M.; Albano, D.; Allen, G.; Bazzocchi, A.; Bignotti, B.; Chianca, V.; de Castro, F.F.; Drakonaki, E.E.; Gallardo, E.; Gielen, J.; et al. Clinical indications for musculoskeletal ultrasound updated in 2017 by European Society of Musculoskeletal Radiology (ESSR) consensus. Eur. Radiol. 2018, 28, 5338–5351. [Google Scholar] [CrossRef] [PubMed]
- Cucchi, D.; Di Giacomo, G.; Compagnoni, R.; Castricini, R.; Formigoni, C.; Radici, M.; Melis, B.; Brindisino, F.; De Giorgi, S.; De Vita, A.; et al. A high level of scientific evidence is available to guide treatment of primary shoulder stiffness: The SIAGASCOT consensus. Knee Surg. Sports Traumatol. Arthrosc. 2024, 32, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.Y.; Hsu, P.C.; Tsai, Y.Y.; Huang, J.R.; Wang, K.A.; Wang, J.C. Efficacy of combined ultrasound-guided hydrodilatation with hyaluronic acid and physical therapy in patients with adhesive capsulitis: A randomised controlled trial. Clin. Rehabil. 2024, 38, 202–215. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.W.; Tam, K.W.; Liou, T.H.; Rau, C.L.; Huang, S.W.; Hsu, T.H. Efficacy of Platelet-Rich Plasma Injection on Range of Motion, Pain, and Disability in Patients With Adhesive Capsulitis: A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2023, 104, 2109–2122. [Google Scholar] [CrossRef] [PubMed]
- Papalexis, N.; Ponti, F.; Rinaldi, R.; Peta, G.; Bruno, R.; Miceli, M.; Battaglia, M.; Marinelli, A.; Spinnato, P. Ultrasound-guided Treatments for the Painful Shoulder. Curr. Med. Imaging 2022, 18, 693–700. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Green, S.; Kramer, S.; Johnston, R.V.; McBain, B.; Chau, M.; Buchbinder, R. Manual therapy and exercise for adhesive capsulitis (frozen shoulder). Cochrane Database Syst. Rev. 2014, 2014, CD011275. [Google Scholar] [CrossRef]
- Kayaokay, K.; Arslan Yurtlu, D. A Comparison of the Treatment Outcomes With and Without the Use of Intra-articular Corticosteroids for Frozen Shoulder Manipulation. Cureus 2023, 15, e44427. [Google Scholar] [CrossRef] [PubMed]
- Mun, S.W.; Baek, C.H. Clinical efficacy of hydrodistention with joint manipulation under interscalene block compared with intra-articular corticosteroid injection for frozen shoulder: A prospective randomized controlled study. J. Shoulder Elbow. Surg. 2016, 25, 1937–1943. [Google Scholar] [CrossRef] [PubMed]
- Boyles, R.E.; Flynn, T.W.; Whitman, J.M. Manipulation following regional interscalene anesthetic block for shoulder adhesive capsulitis: A case series. Man. Ther. 2005, 10, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Placzek, J.D.; Roubal, P.J.; Kulig, K.; Pagett, B.T.; Wiater, J.M. Theory and technique of translational manipulation for adhesive capsulitis. Am. J. Orthop. (Belle Mead NJ) 2004, 33, 173–179. [Google Scholar] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Calcific Deposition Stage | Group 1 CT + AC (n = 26) | Group 2 CT (n = 52) |
|---|---|---|
| Stage I | 2 (7.69%) | 3 (5.77%) |
| Stage II | 5 (19.23%) | 16 (30.77%) |
| Stage III | 10 (38.46%) | 28 (53.84%) |
| Stage IV | 9 (34.61%) | 5 (9.62%) |
| Total (n = 78) | CT with AC (n = 26) | CT without AC (n = 52) | p-Value |
|---|---|---|---|
| AP thickness, mm | 3.96 ± 1.37 | 2.08 ± 0.40 | |
| RI thickness, mm | 2.54 ± 0.38 | 1.81 ± 0.41 | <0.00001 |
| LHBT effusion, % | 84.61 | 1579 | <0.00001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tuè, G.; Masuzzo, O.; Tucci, F.; Cavallo, M.; Parmeggiani, A.; Vita, F.; Patti, A.; Donati, D.; Marinelli, A.; Miceli, M.; et al. Can Secondary Adhesive Capsulitis Complicate Calcific Tendinitis of the Rotator Cuff? An Ultrasound Imaging Analysis. Clin. Pract. 2024, 14, 579-589. https://doi.org/10.3390/clinpract14020045
Tuè G, Masuzzo O, Tucci F, Cavallo M, Parmeggiani A, Vita F, Patti A, Donati D, Marinelli A, Miceli M, et al. Can Secondary Adhesive Capsulitis Complicate Calcific Tendinitis of the Rotator Cuff? An Ultrasound Imaging Analysis. Clinics and Practice. 2024; 14(2):579-589. https://doi.org/10.3390/clinpract14020045
Chicago/Turabian StyleTuè, Giovanni, Oriana Masuzzo, Francesco Tucci, Marco Cavallo, Anna Parmeggiani, Fabio Vita, Alberto Patti, Danilo Donati, Alessandro Marinelli, Marco Miceli, and et al. 2024. "Can Secondary Adhesive Capsulitis Complicate Calcific Tendinitis of the Rotator Cuff? An Ultrasound Imaging Analysis" Clinics and Practice 14, no. 2: 579-589. https://doi.org/10.3390/clinpract14020045
APA StyleTuè, G., Masuzzo, O., Tucci, F., Cavallo, M., Parmeggiani, A., Vita, F., Patti, A., Donati, D., Marinelli, A., Miceli, M., & Spinnato, P. (2024). Can Secondary Adhesive Capsulitis Complicate Calcific Tendinitis of the Rotator Cuff? An Ultrasound Imaging Analysis. Clinics and Practice, 14(2), 579-589. https://doi.org/10.3390/clinpract14020045