


Successful Interventional Endovascular Management of Ruptured Penetrating Aortic Ulcer with Associated Enormous Right Pleural False Aneurysm


Abstract
:1. Introduction
2. Case Presentation
2.1. Patient Information
2.2. Clinical Findings
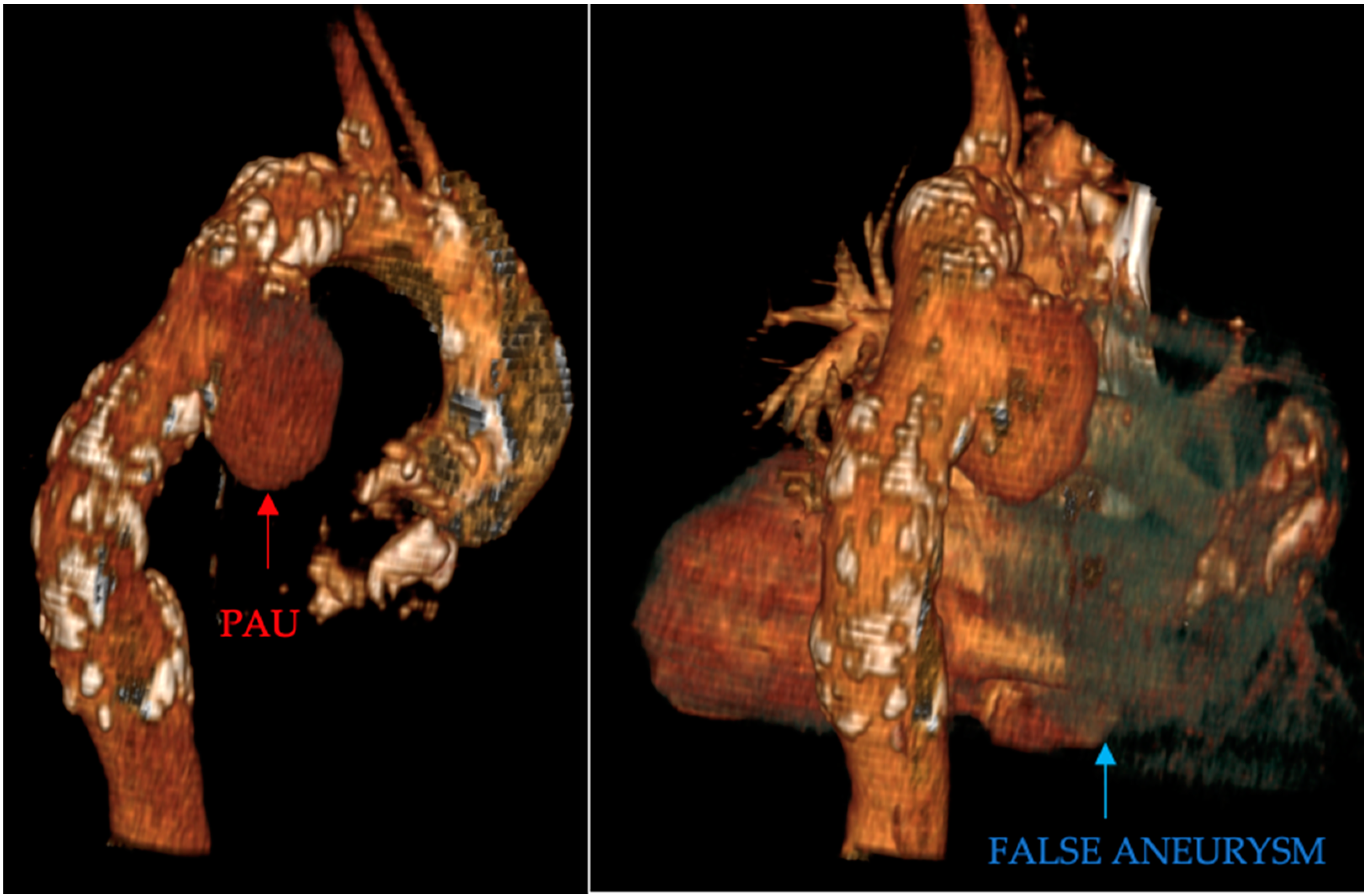
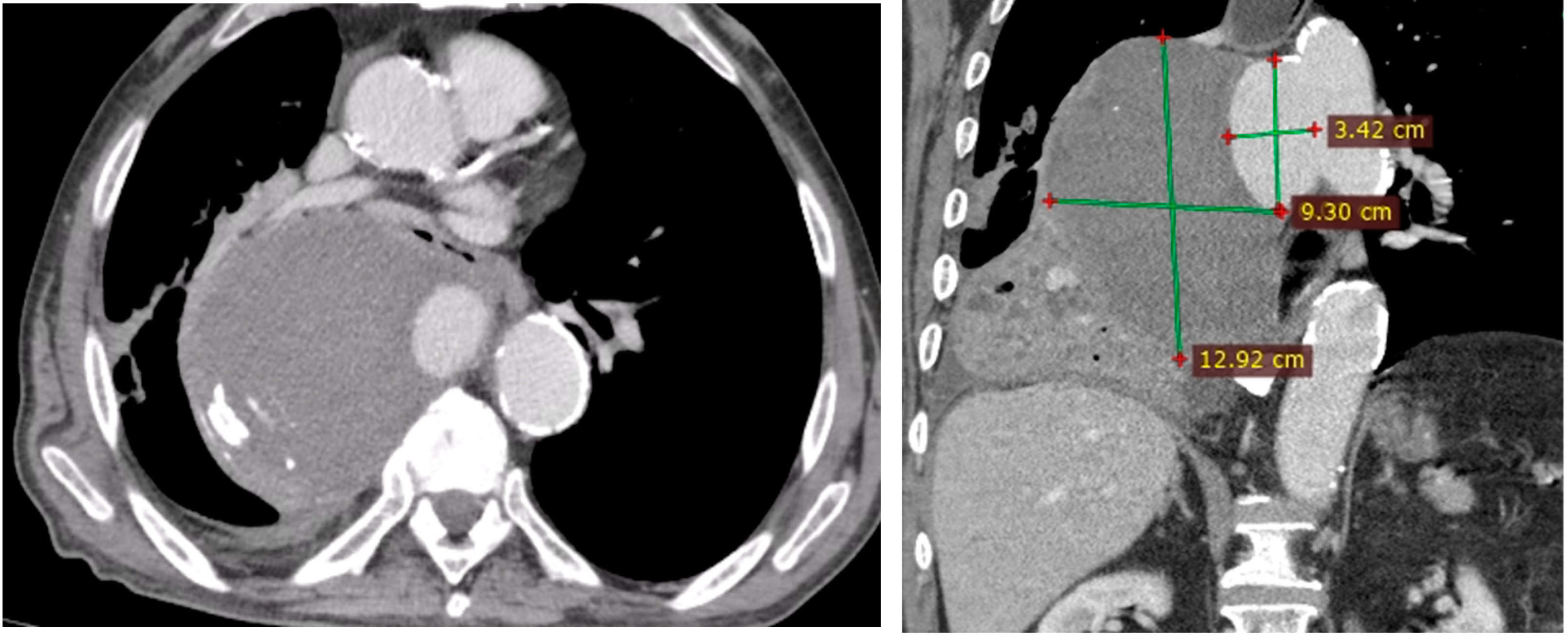
- Penetrating aortic ulcer ruptured: As seen in Figure 2, the thoracic angio-CT scan identified a penetrating ulcer within the aortic wall, particularly located in the isthmic region, measuring approximately 4.2 cm × 3.5 cm. This was a concealed source of significant concern, as it posed an imminent risk of catastrophic hemorrhage.
- Right pleural aortic false aneurysm (Figure 3): The most striking feature was the presence of an expansive false aneurysm within the right pleural cavity, measuring approximately 12.92 cm × 9.3 cm. The size and location of this pseudoaneurysm were unprecedented, introducing a challenge in terms of diagnosis and intervention.
- Megaesophagus: Notably, the imaging findings also uncovered a megaesophagus, a condition characterized by significant dilation of the esophagus. Although not the primary focus of intervention, its presence added another layer of complexity to the clinical scenario. The etiology of the megaesophagus remained to be elucidated.
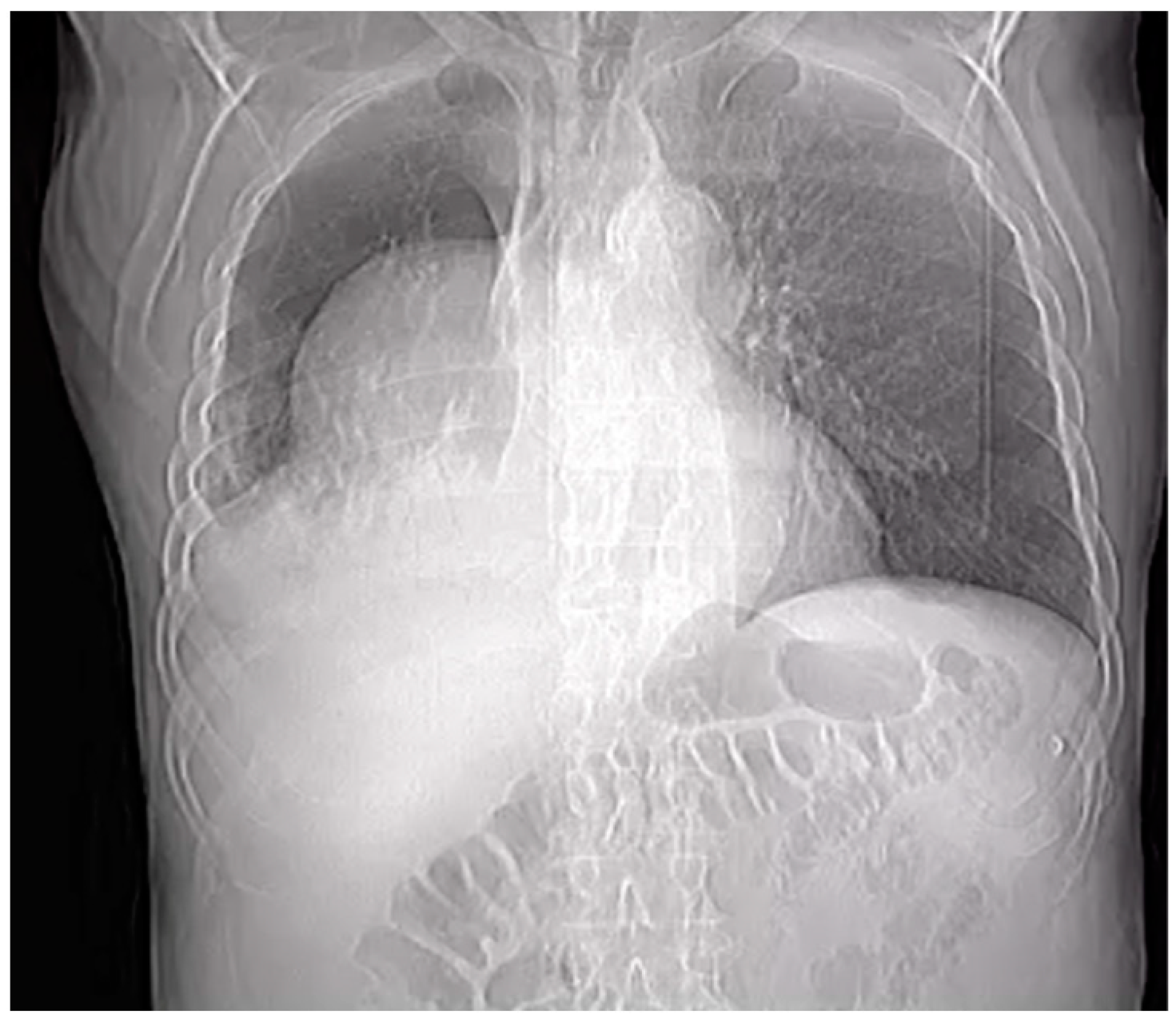
- Compression of the lung: The false aneurysm within the right pleura had exerted a significant mass effect, resulting in the compression of surrounding structures, notably the lung. This compression had led to compromised ventilation of the lung, contributing to a concerning clinical picture.
- Potential lung infection (Empyema): The compromised lung, in part due to the mass effect of the false aneurysm, exhibited signs of infection. Imaging suggested the possible development of empyema. This provided a plausible explanation for the patient’s presenting symptom of hemoptysis.
2.3. Blood Analysis
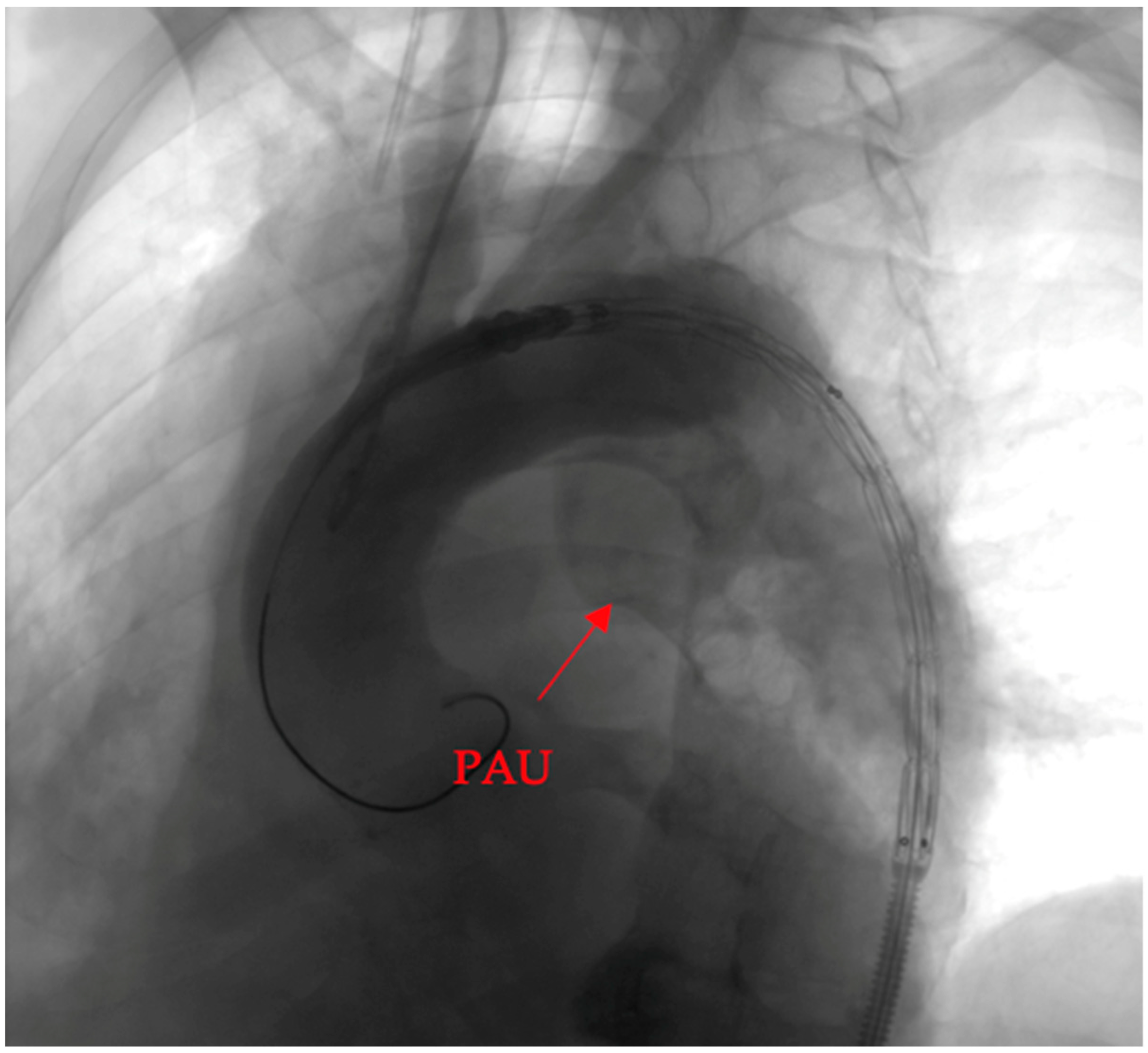
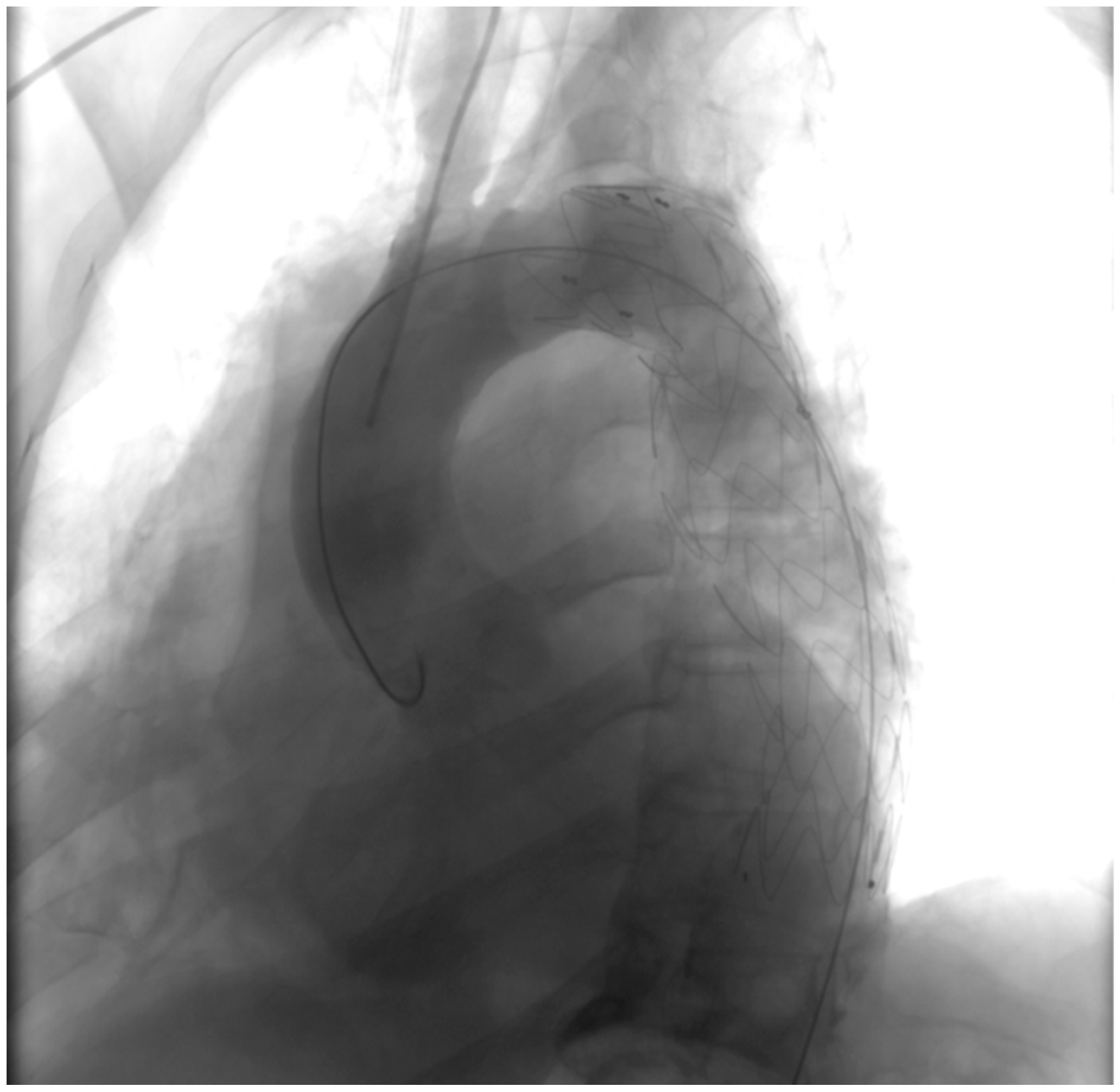
2.4. Endovascular Procedure and Stent Placement
2.5. Outcome
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Erbel, R.; Aboyans, V.; Boileau, C.; Bossone, E.; Di Bartolomeo, R.; Eggebrecht, H.; Evangelista, A.; Falk, V.; Frank, H.; Gaemperli, O.; et al. 2014 ESC Guidelines on the Diagnosis and Treatment of Aortic Diseases: Document Covering Acute and Chronic Aortic Diseases of the Thoracic and Abdominal Aorta of the adultThe Task Force for the Diagnosis and Treatment of Aortic Diseases of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2873–2926. [Google Scholar] [CrossRef] [PubMed]
- Svensson, L.G.; Labib, S.B.; Eisenhauer, A.C.; Butterly, J.R. Intimal Tear Without Hematoma: An Important Variant of Aortic Dissection That Can Elude Current Imaging Techniques. Circulation 1999, 99, 1331–1336. [Google Scholar] [CrossRef] [PubMed]
- O’Gara, P.T.; DeSanctis, R.W. Acute Aortic Dissection and Its Variants: Toward a Common Diagnostic and Therapeutic Approach. Circulation 1995, 92, 1376–1378. [Google Scholar] [CrossRef] [PubMed]
- DeCarlo, C.; Latz, C.A.; Boitano, L.T.; Kim, Y.; Tanious, A.; Schwartz, S.I.; Patell, R.; Mohebali, J.; Dua, A. Prognostication of Asymptomatic Penetrating Aortic Ulcers: A Modern Approach. Circulation 2021, 144, 1091–1101. [Google Scholar] [CrossRef] [PubMed]
- Oderich, G.S.; Kärkkäinen, J.M.; Reed, N.R.; Tenorio, E.R.; Sandri, G.A. Penetrating Aortic Ulcer and Intramural Hematoma. Cardiovasc. Interv. Radiol. 2019, 42, 321–334. [Google Scholar] [CrossRef] [PubMed]
- Murana, G.; Di Marco, L.; Fiorentino, M.; Buia, F.; Brillanti, G.; Lovato, L.; Pacini, D. Endovascular Treatment of Penetrating Atherosclerotic Ulcers of the Arch and Thoracic Aorta: In-Hospital and 5-Year Outcomes. JTCVS Open 2022, 10, 12–21. [Google Scholar] [CrossRef] [PubMed]
- Stanson, A.W.; Kazmier, F.J.; Hollier, L.H.; Edwards, W.D.; Pairolero, P.C.; Sheedy, P.F.; Joyce, J.W.; Johnson, M.C. Penetrating Atherosclerotic Ulcers of the Thoracic Aorta: Natural History and Clinicopathologic Correlations. Ann. Vasc. Surg. 1986, 1, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Movsowitz, H.D.; Lampert, C.; Jacobs, L.E.; Kotler, M.N. Penetrating Atherosclerotic Aortic Ulcers. Am. Heart J. 1994, 128, 1210–1217. [Google Scholar] [CrossRef]
- Evangelista, A.; Moral, S. Penetrating Atherosclerotic Ulcer. Curr. Opin. Cardiol. 2020, 35, 620–626. [Google Scholar] [CrossRef]
- Coady, M.A.; Rizzo, J.A.; Hammond, G.L.; Pierce, J.G.; Kopf, G.S.; Elefteriades, J.A. Penetrating Ulcer of the Thoracic Aorta: What Is It? How Do We Recognize It? How Do We Manage It? J. Vasc. Surg. 1998, 27, 1006–1016. [Google Scholar] [CrossRef]
- Zindovic, I.; Sjögren, J.; Bjursten, H.; Ingemansson, R.; Larsson, M.; Svensson, P.J.; Strandberg, K.; Wierup, P.; Nozohoor, S. The Role of von Willebrand Factor in Acute Type A Aortic Dissection and Aortic Surgery. Thromb. Res. 2019, 178, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Couture, T.; Gaudric, J.; Davaine, J.-M.; Jayet, J.; Chiche, L.; Jarraya, M.; Koskas, F. Results of Cryopreserved Arterial Allograft Replacement for Thoracic and Thoracoabdominal Aortic Infections. J. Vasc. Surg. 2021, 73, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Heinola, I.; Sörelius, K.; Wyss, T.R.; Eldrup, N.; Settembre, N.; Setacci, C.; Mani, K.; Kantonen, I.; Venermo, M. Open Repair of Mycotic Abdominal Aortic Aneurysms With Biological Grafts: An International Multicenter Study. J. Am. Heart Assoc. 2018, 7, e008104. [Google Scholar] [CrossRef] [PubMed]
- Mestres, C.A.; Quintana, E.; Kopjar, T.; Ambrosioni, J.; Almela, M.; Fuster, D.; Ninot, S.; Miró, J.M.; The Hospital Clinic Infective Endocarditis Investigators. Twenty-Year Experience with Cryopreserved Arterial Allografts for Vascular Infections. Eur. J. Cardio-Thorac. Surg. 2019, 55, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Petrunić, M.; Biočina, B.; Uzun, S.; Meštrović, T.; Šafradin, I. Cryopreserved Aortic Homograft for In Situ Replacement of Infected Thoracic Stent Graft Associated With Distal Aortic Arch Rupture and Hematemesis. Ann. Thorac. Surg. 2014, 98, 2219–2221. [Google Scholar] [CrossRef] [PubMed]
- Jonker, F.H.W.; Verhagen, H.J.M.; Lin, P.H.; Heijmen, R.H.; Trimarchi, S.; Lee, W.A.; Moll, F.L.; Atamneh, H.; Rampoldi, V.; Muhs, B.E. Open Surgery versus Endovascular Repair of Ruptured Thoracic Aortic Aneurysms. J. Vasc. Surg. 2011, 53, 1210–1216. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Huh, U.; Song, S.; Kim, M.S.; Kim, C.W.; Jeon, C.H.; Kwon, H.; Wang, I.J. Open Repair versus Thoracic Endovascular Aortic Repair for Treating Traumatic Aortic Injury. Asian J. Surg. 2022, 45, 2224–2230. [Google Scholar] [CrossRef] [PubMed]
- Xenos, E.S.; Abedi, N.N.; Davenport, D.L.; Minion, D.J.; Hamdallah, O.; Sorial, E.E.; Endean, E.D. Meta-Analysis of Endovascular vs Open Repair for Traumatic Descending Thoracic Aortic Rupture. J. Vasc. Surg. 2008, 48, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- Marty-Ané, C.-H.; Berthet, J.-P.; Branchereau, P.; Mary, H.; Alric, P. Endovascular Repair for Acute Traumatic Rupture of the Thoracic Aorta. Ann. Thorac. Surg. 2003, 75, 1803–1807. [Google Scholar] [CrossRef]
- Rizza, A.; Negro, F.; Palermi, S.; Palmieri, C.; Murzi, M.; Credi, G.; Berti, S. Penetrating Aortic Ulceration Treated with Castor Branched Aortic Stent Graft—A Case Series. Int. J. Environ. Res. Public Health 2022, 19, 4809. [Google Scholar] [CrossRef]
- Patel, H.J.; Sood, V.; Williams, D.M.; Dasika, N.L.; Diener, A.C.; Deeb, G.M. Late Outcomes With Repair of Penetrating Thoracic Aortic Ulcers: The Merits of an Endovascular Approach. Ann. Thorac. Surg. 2012, 94, 516–523. [Google Scholar] [CrossRef] [PubMed]
- Writing Group Members; Hiratzka, L.F.; Bakris, G.L.; Beckman, J.A.; Bersin, R.M.; Carr, V.F.; Casey, D.E.; Eagle, K.A.; Hermann, L.K.; Isselbacher, E.M.; et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients With Thoracic Aortic Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation 2010, 121, e266–e369. [Google Scholar] [CrossRef] [PubMed]
- Salim, S.; Locci, R.; Martin, G.; Gibbs, R.; Jenkins, M.; Hamady, M.; Riga, C.; Bicknell, C.; Davies, A.; Jaffer, U.; et al. Short- and Long-Term Outcomes in Isolated Penetrating Aortic Ulcer Disease. J. Vasc. Surg. 2020, 72, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Kreibich, M.; Kremer, J.; Vötsch, A.; Berger, T.; Farag, M.; Winkler, A.; Siepe, M.; Karck, M.; Beyersdorf, F.; Rylski, B.; et al. Multicentre Experience with the Frozen Elephant Trunk Technique to Treat Penetrating Aortic Ulcers Involving the Aortic Arch. Eur. J. Cardio-Thorac. Surg. 2021, 59, 1238–1244. [Google Scholar] [CrossRef]
- Canaud, L.; Hireche, K.; D’annoville, T.; Alric, P. Hybrid Aortic Arch Repair for a Ruptured and Infected Penetrating Atherosclerotic Ulcer of the Aortic Arch. Ann. Vasc. Surg. 2011, 25, 266.e5–266.e7. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Blood Test | Results |
|---|---|
| Hemoglobin (g/dL) | 7.9 |
| Red cell count (106/µL) | 3.00 |
| Platelets (103/µL) | 361 |
| White blood cells (103/µL) | 8.19 |
| ESR (mm/h) | 120 |
| PT (s) | 19.8 |
| INR | 1.23 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grigorescu, A.E.; Anghel, A.; Feier, H. Successful Interventional Endovascular Management of Ruptured Penetrating Aortic Ulcer with Associated Enormous Right Pleural False Aneurysm. Clin. Pract. 2024, 14, 619-628. https://doi.org/10.3390/clinpract14020049
Grigorescu AE, Anghel A, Feier H. Successful Interventional Endovascular Management of Ruptured Penetrating Aortic Ulcer with Associated Enormous Right Pleural False Aneurysm. Clinics and Practice. 2024; 14(2):619-628. https://doi.org/10.3390/clinpract14020049
Chicago/Turabian StyleGrigorescu, Andrei Emanuel, Andrei Anghel, and Horea Feier. 2024. "Successful Interventional Endovascular Management of Ruptured Penetrating Aortic Ulcer with Associated Enormous Right Pleural False Aneurysm" Clinics and Practice 14, no. 2: 619-628. https://doi.org/10.3390/clinpract14020049
APA StyleGrigorescu, A. E., Anghel, A., & Feier, H. (2024). Successful Interventional Endovascular Management of Ruptured Penetrating Aortic Ulcer with Associated Enormous Right Pleural False Aneurysm. Clinics and Practice, 14(2), 619-628. https://doi.org/10.3390/clinpract14020049