Indoor Air Quality and Sustainability Management—Case Study in Three Portuguese Healthcare Units

 ,
,  ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Healthcare Units
2.2. IAQ Characterization Campaigns
- (1)
- Similar rooms in different healthcare units: Consulting, treatment, and waiting rooms at H1, H2 and HC, and hospital wards at H1and H2;
- (2)
- Similar rooms under different weather conditions: Summer and winter campaigns at the general hospitals H1 and H2;
- (3)
- The same healthcare unit under different working conditions: At HC and H2, campaigns were performed both during normal operation and emergency/urgent care assistance.
2.3. Data Analysis
3. Results
3.1. Comparison of Analyzed IAQ Conditions in the Three Healthcare Units
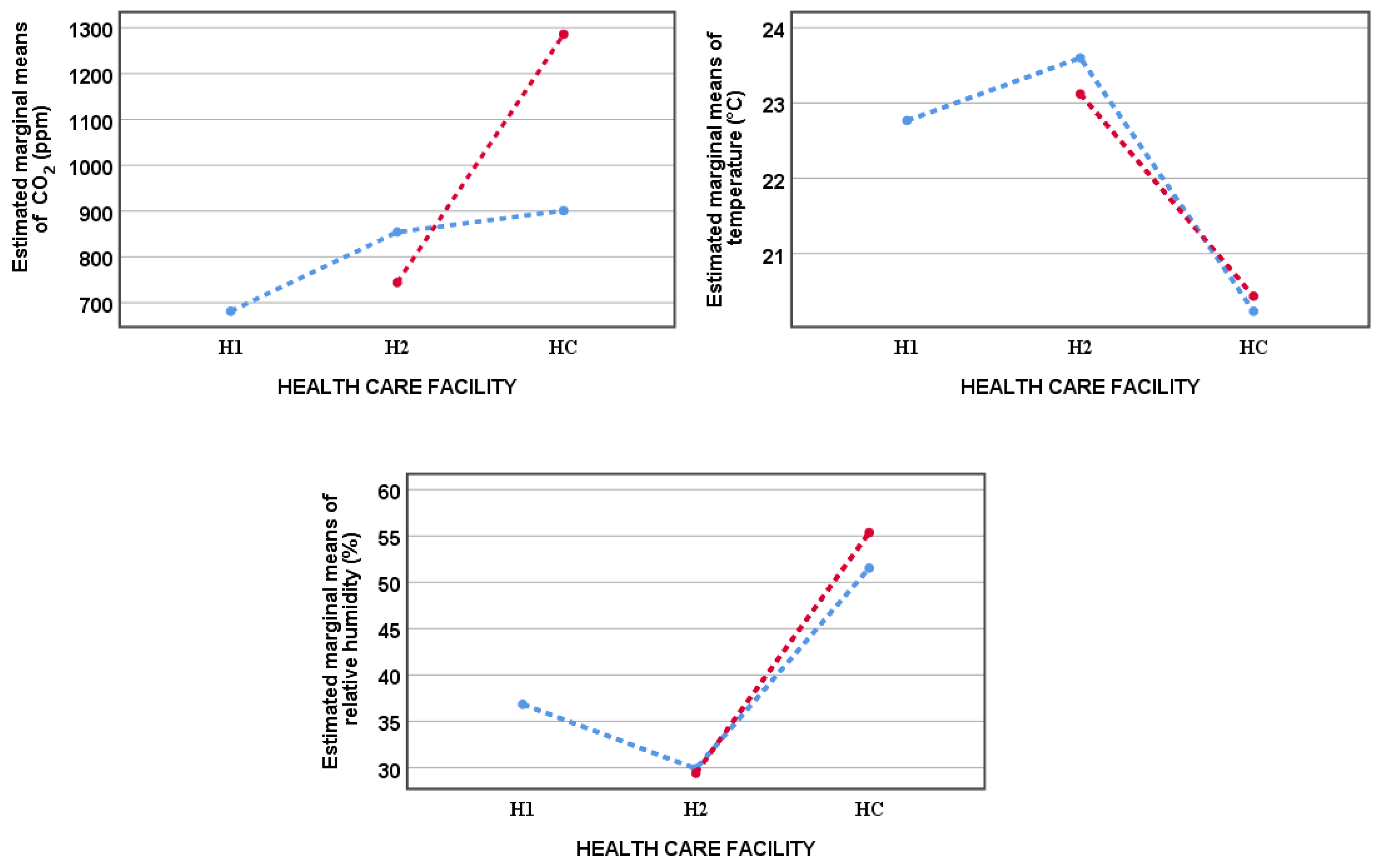
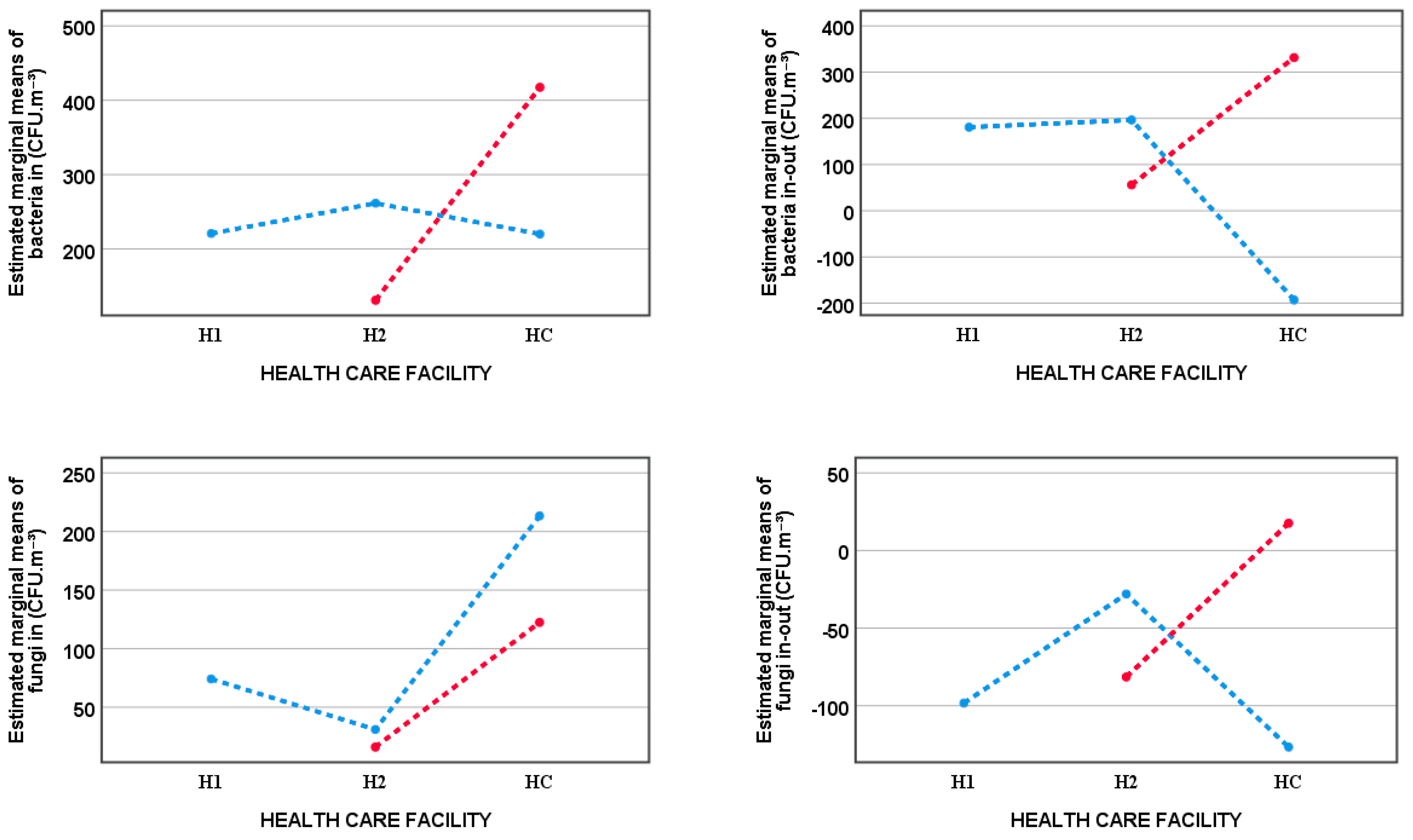
- (1)
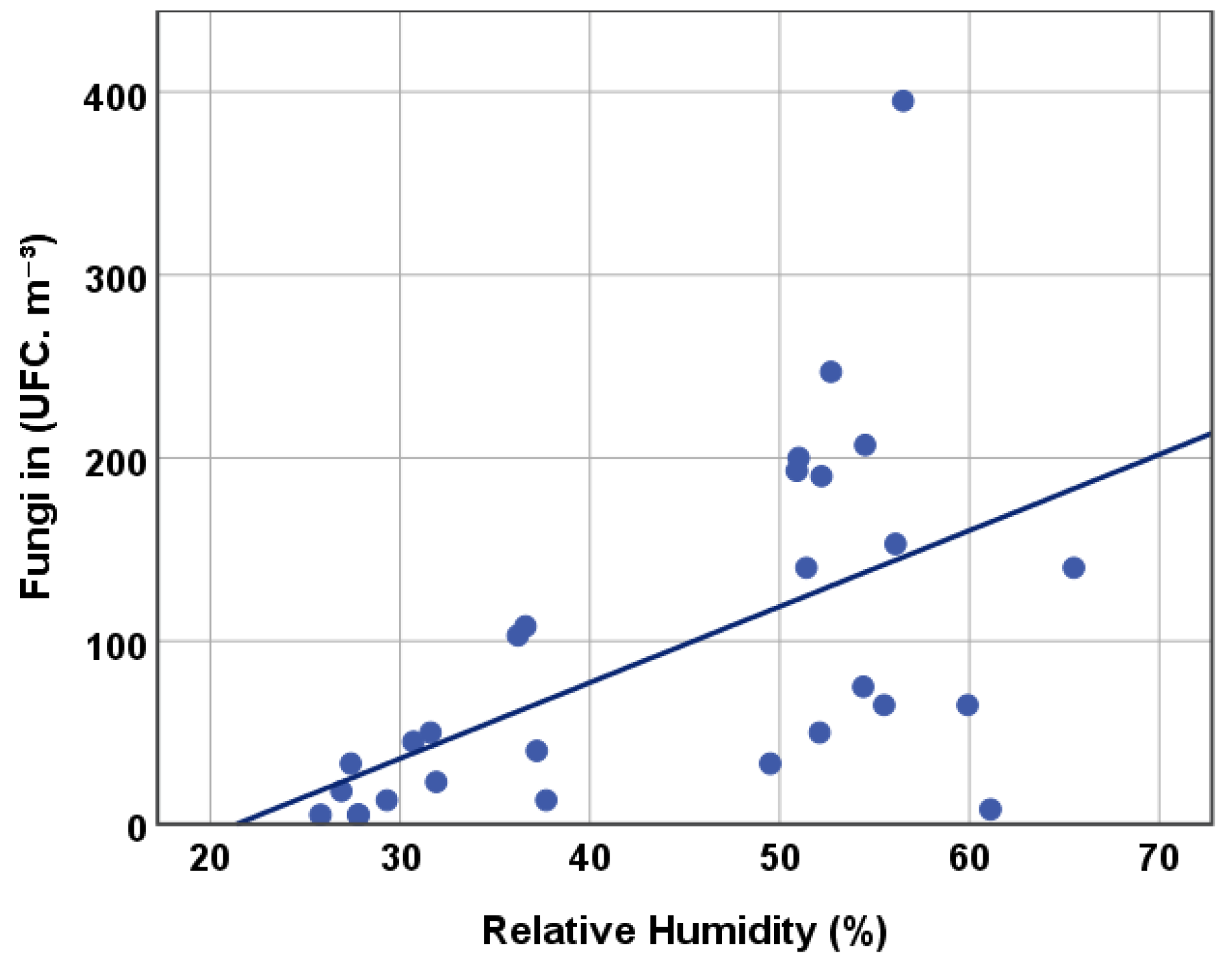
- Under normal working conditions, the two hospitals showed no differences on most analyzed parameters, with the exception of indoor air relative humidity (higher in hospital H1), and the difference fungi in-out (higher in hospital H2).
- (2)
- Under normal working conditions, most of the analyzed parameters in the health center HC were different from those of hospitals H1 and H2: Air temperature and the bacteria in-out difference were lower in HC, whereas relative humidity and fungi concentration were higher in HC. No significant differences were found in indoor air CO2 and bacteria concentrations between HC and hospitals H1 and H2, and in the fungi in-out difference between HC and hospital H1.
- (3)
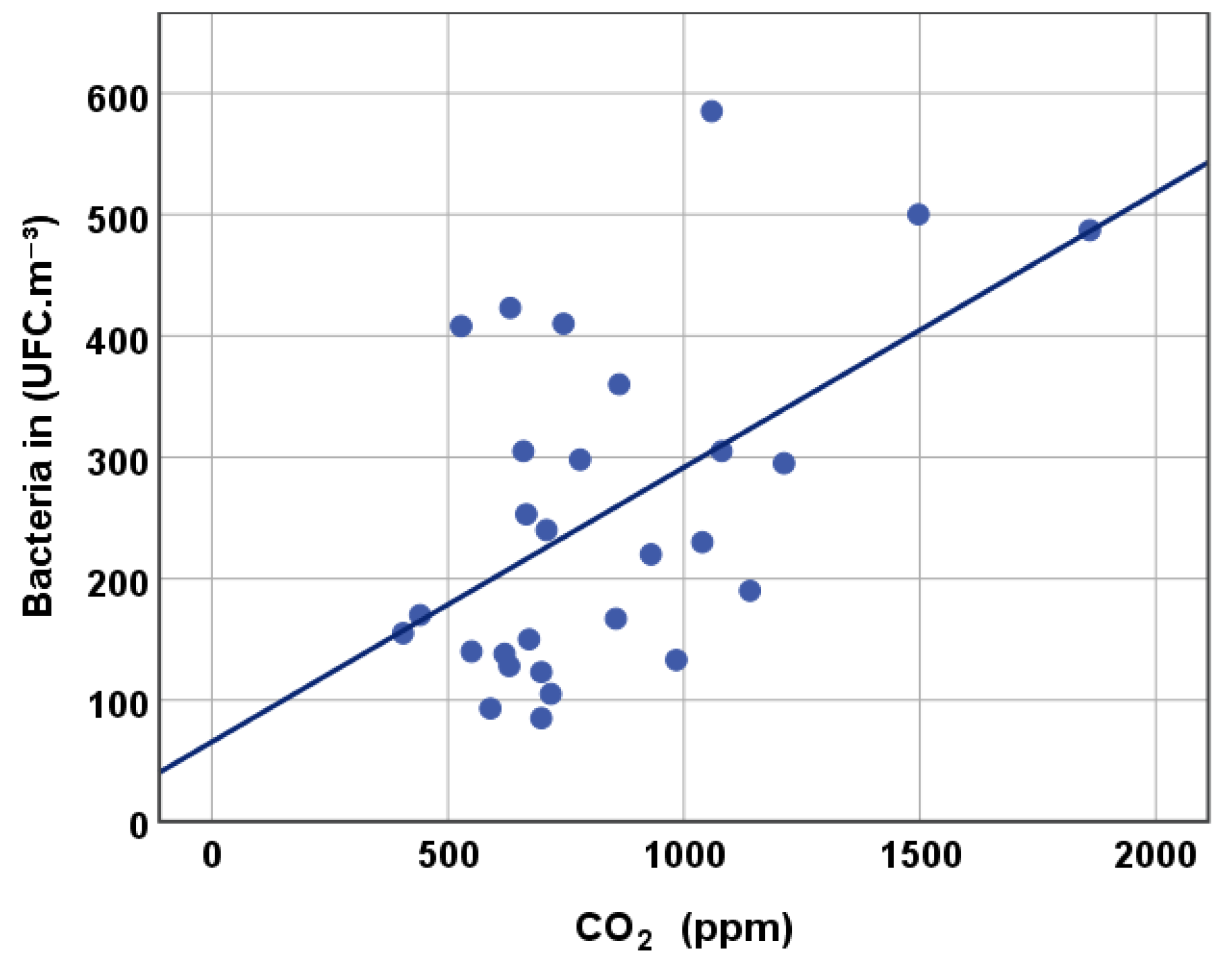
- Under emergency/urgent care conditions, all the analyzed parameters showed significant differences when comparing the health center HC with hospital H2: HC showed higher results for indoor air CO2, bacteria and fungi concentrations, relative humidity, and for the bacteria in-out and fungi in-out differences; indoor air temperature was lower in HC.
- (1)
- In hospital H2 significant differences were found between microbiological parameters under normal and under emergency/urgent care working conditions: Indoor air bacteria concentration, bacteria in-out and fungi in-out differences were higher under normal working conditions.
- (2)
- In the health center HC, the higher values obtained for bacteria in-out and fungi in-out in emergency/urgent care situations are statistically relevant. Although Figure 1 and Figure 2 show higher values for indoor air CO2 and bacteria concentrations in emergency/urgent care conditions, these differences are not significant at a 0.05 significance level.
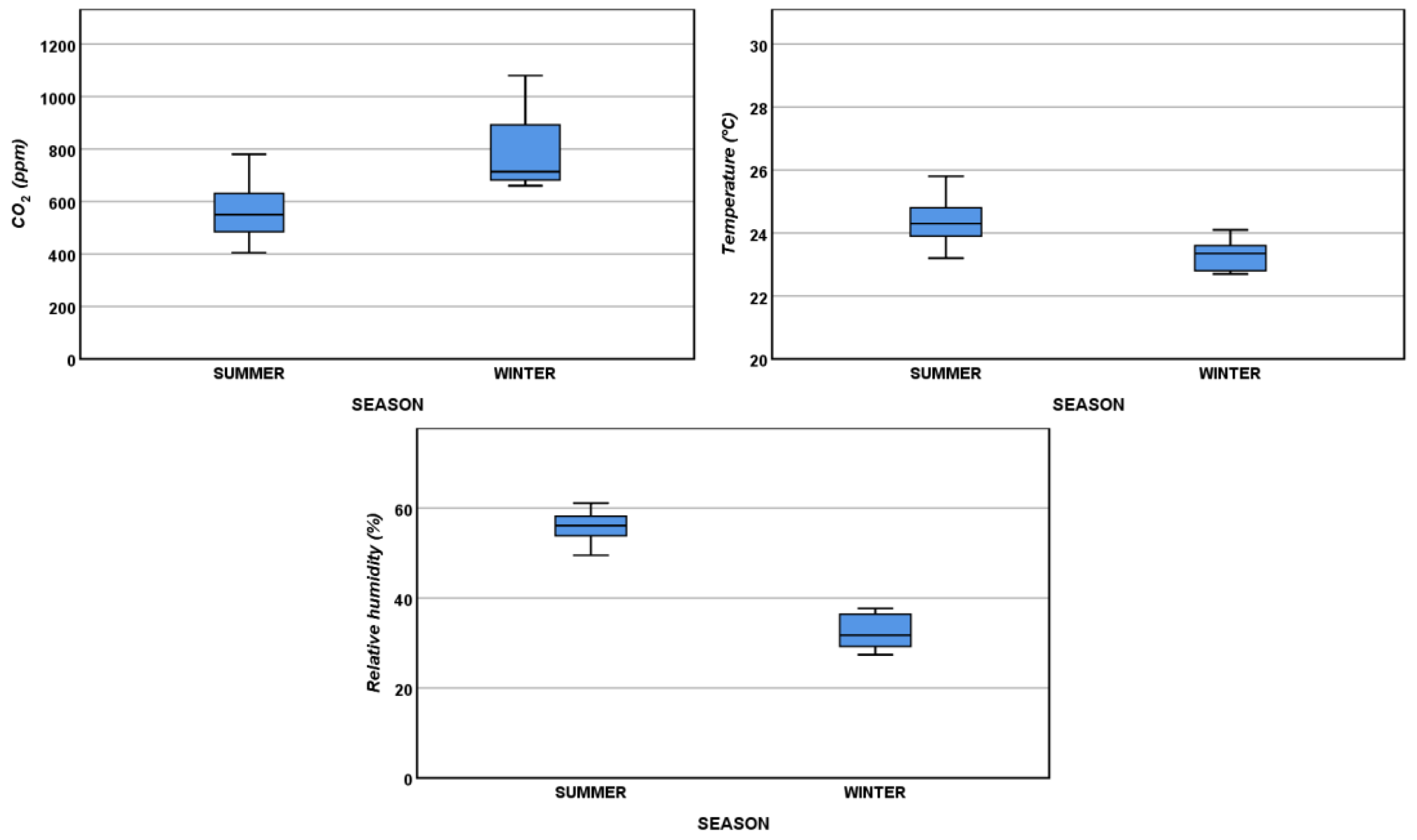
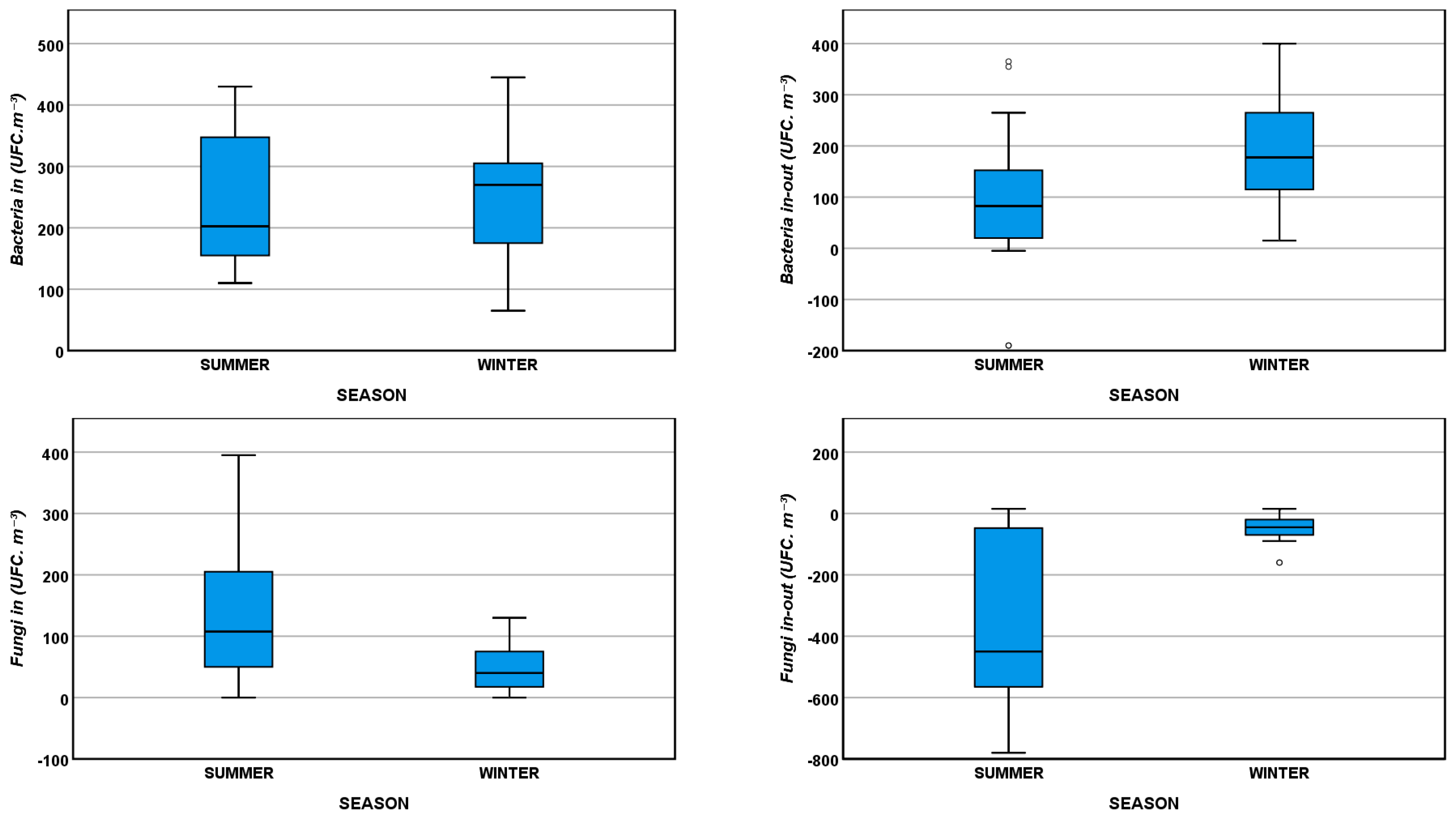
3.2. Seasonal Variation of IAQ
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Fischer, M. Fit for the future? A new approach in the debate about what makes healthcare systems really sustainable. Sustainability 2015, 7, 294–312. [Google Scholar] [CrossRef]
- Carnero, M.C. Assessment of Environmental Sustainability in Health Care Organizations. Sustainability 2015, 7, 8270–8291. [Google Scholar] [CrossRef] [Green Version]
- de Castro, M.F.; Mateus, R.; Serôdio, F.; Bragança, L. Development of benchmarks for operating costs and resources consumption to be used in healthcare building sustainability assessment methods. Sustainability 2015, 7, 13222–13248. [Google Scholar] [CrossRef]
- Naranjo-Gil, D. The role of management control systems and top teams in implementing environmental sustainability policies. Sustainability 2016, 8, 359. [Google Scholar] [CrossRef]
- García-Sanz-Calcedo, J.; Al-Kassir, A.; Yusaf, T. Economic and Environmental Impact of Energy Saving in Healthcare Buildings. Appl. Sci. 2018, 8, 440. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, Z.; Zhang, Z.; Hong, J.; Lin, B. Investigation on the Indoor Environment Quality of health care facilities in China. Build. Environ. 2018, 141, 273–287. [Google Scholar] [CrossRef]
- Kim, J.-R.; Jeon, E.-C.; Cho, S.; Kim, H. The Promotion of Environmental Management in the South Korean Health Sector—Case Study. Sustainability 2018, 10, 2081. [Google Scholar] [CrossRef]
- Qian, H.; Li, Y.; Seto, W.H.; Ching, P.; Ching, W.H.; Sun, H.Q. Natural ventilation for reducing airborne infection in hospitals. Build. Environ. 2010, 45, 559–565. [Google Scholar] [CrossRef]
- Nimlyat, P.S.; Kandar, M.Z. Appraisal of indoor environmental quality (IEQ) in healthcare facilities: A literature review. Sustain. Cities Soc. 2015, 17, 61–68. [Google Scholar] [CrossRef]
- Loupa, G.; Fotopoulou, S.; Tsagarakis, K.P. A tool for analysing the interdependence of indoor environmental quality and reported symptoms of the hospitals’ personnel. J. Risk Res. 2017, 20, 678–691. [Google Scholar] [CrossRef]
- Frontczak, M.; Wargocki, P. Literature survey on how different factors influence human comfort in indoor environments. Build. Environ. 2011, 46, 922–937. [Google Scholar] [CrossRef]
- Jurado, S.R.; Bankoff, A.D.P.; Sanchez, A. Indoor air quality in Brazilian universities. Int. J. Environ. Res. Public Health 2014, 11, 7081–7093. [Google Scholar] [CrossRef] [PubMed]
- Widder, S.H.; Haselbach, L. Relationship among concentrations of indoor air contaminants, their sources, and different mitigation strategies on indoor air quality. Sustainability 2017, 9, 1149. [Google Scholar] [CrossRef]
- EPA-United States Environmental Protection Agency. Fundamentals of Indoor Air Quality in Buildings. Available online: https://www.epa.gov/indoor-air-quality-iaq/fundamentals-indoor-air-quality-buildings (accessed on 23 December 2018).
- World Health Organization. WHO Guidelines for Indoor Air Quality: Selected Pollutants; World Health Organization: Copenhagen, Denmark, 2010; ISBN 978-92-890-0213-4. [Google Scholar]
- World Health Organization. WHO Guidelines for Indoor Air Quality: Dampness and Mould; World Health Organization: Copenhagen, Denmark, 2009; ISBN 978-92-890-4168-3. [Google Scholar]
- El-Sharkawy, M.; Noweir, M.H. Indoor air quality levels in a University Hospital in the Eastern Province of Saudi Arabia. J. Fam. Community Med. 2014, 21, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Wallner, P.; Tappler, P.; Munoz, U.; Damberger, B.; Wanka, A.; Kundi, M.; Hutter, H.P. Health and wellbeing of occupants in highly energy efficient buildings: A field study. Int. J. Environ. Res. Public Health 2017, 14, 314. [Google Scholar] [CrossRef]
- Li, Y.; Leung, G.M.; Tang, J.W.; Yang, X.; Chao, C.Y.H.; Lin, J.Z.; Lu, J.W.; Nielsen, P.V.; Niu, J.; Qian, H.; et al. Role of ventilation in airborne transmission of infectious agents in the built environment—A multidisciplinary systematic review. Indoor Air 2007, 17, 2–18. [Google Scholar] [CrossRef]
- Bekkari, H.; Benchemsi, N.; Touijer, H.; Berrada, S.; Maniar, S.; Ettayebi, M.; El Ouali Lalami, A. Microbial analysis of air in a public hospital in the city of Fez, Morocco. Int. J. Pharm. Clin. Res. 2016, 8, 533–537. [Google Scholar]
- Ikhtiar, M.; Alzad, H.; Paramita, S. Microbiological Assessment of Indoor Air of Takalar County Hospital Wards in South Sulawesi, Indonesia. Sci. J. Public Heal. 2017, 5, 172–177. [Google Scholar] [CrossRef]
- Beggs, C.; Knibbs, L.D.; Johnson, G.R.; Morawska, L. Environmental contamination and hospital-acquired infection: Factors that are easily overlooked. Indoor Air 2015, 25, 462–474. [Google Scholar] [CrossRef]
- Cox-Ganser, J.M.; Rao, C.Y.; Park, J.H.; Schumpert, J.C.; Kreiss, K. Asthma and respiratory symptoms in hospital workers related to dampness and biological contaminants. Indoor Air 2009, 19, 280–290. [Google Scholar] [CrossRef]
- Yang, C.-T.; Liao, C.-J.; Liu, J.-C.; Den, W.; Chou, Y.-C.; Tsai, J.-J. Construction and Application of an Intelligent Air Quality Monitoring System for Healthcare Environment. J. Med. Syst. 2014, 38, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Wallner, P.; Munoz, U.; Tappler, P.; Wanka, A.; Kundi, M.; Shelton, J.F.; Hutter, H.P. Indoor environmental quality in mechanically ventilated, energy-efficient buildings vs. Conventional buildings. Int. J. Environ. Res. Public Health 2015, 12, 14132–14147. [Google Scholar] [CrossRef] [PubMed]
- Hellgren, U.M.; Hyvärinen, M.; Holopainen, R.; Reijula, K. Perceived indoor air quality, air-related symptoms and ventilation in finnish hospitals. Int. J. Occup. Med. Environ. Health 2011, 24, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Gilkeson, C.A.; Camargo-Valero, M.A.; Pickin, L.E.; Noakes, C.J. Measurement of ventilation and airborne infection risk in large naturally ventilated hospital wards. Build. Environ. 2013, 65, 35–48. [Google Scholar] [CrossRef] [Green Version]
- Yau, Y.H.; Chandrasegaran, D.; Badarudin, A. The ventilation of multiple-bed hospital wards in the tropics: A review. Build. Environ. 2011, 46, 1125–1132. [Google Scholar] [CrossRef]
- World Health Organization. WHO Interim Guidelines—Infection Prevention and Control of Epidemic- and Pandemic-Prone Acute Respiratory Diseases in Health Care; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Escombe, A.R.; Oeser, C.C.; Gilman, R.H.; Navincopa, M.; Ticona, E.; Pan, W.; Martínez, C.; Chacaltana, J.; Rodríguez, R.; Moore, D.A.J.; et al. Natural ventilation for the prevention of airborne contagion. PLoS Med. 2007, 4, 0309–0317. [Google Scholar] [CrossRef]
- Jung, C.C.; Wu, P.C.; Tseng, C.H.; Su, H.J. Indoor air quality varies with ventilation types and working areas in hospitals. Build. Environ. 2015, 85, 190–195. [Google Scholar] [CrossRef]
- ISO 16000-17: Indoor Air Part 17: Detection and Enumeration of Moulds–Culture-Based Method; ISO: Geneva, Switzerland, 2008.
- ISO 16000-18: Indoor Air Part 18: Detection and Enumeration of Moulds–Sampling by Impaction; ISO: Geneva, Switzerland, 2011.
- ISO 16000-26: Indoor Air Part 26: Sampling Strategy for Carbon Dioxide; ISO: Geneva, Switzerland, 2012.
- Blanca, M.J.; Alarcón, R.; Arnau, J.; Bono, R.; Bendayan, R. Non-normal data: Is ANOVA still a valid option? Psicothema 2017, 29, 552–557. [Google Scholar] [CrossRef]
- Portuguese Government. Ordinance n.o. 353-A/2013. Diario da Republica. n.o.235, Supplement, 1st Serie of 2013-12-04. Available online: https://dre.pt/application/file/136515. (accessed on 23 December 2018).
- EN 15251-2007: Indoor Environmental Input Parameters for Design and Assessment of Energy Performance of Buildings Addressing Indoor Air Quality, Thermal Environment, Lighting and Acoustics; European Committee for Standardization: Brussels, Belgium, 2007.
- Keppel, G.; Wickens, T.D. Design and Analysis: A Researcher’s Handbook; Pearson Prentice Hall: Upper Saddle River, NJ, USA, 2004. [Google Scholar]
- Reinikainen, L.M.; Jaakkola, J.J.K. Significance of humidity and temperature on skin and upper airway symptoms. Indoor Air 2003, 13, 344–352. [Google Scholar] [CrossRef]
- Park, D.U.; Yeom, J.K.; Lee, W.J.; Lee, K.M. Assessment of the levels of airborne bacteria, gram-negative bacteria, and fungi in hospital lobbies. Int. J. Environ. Res. Public Health 2013, 10, 541–555. [Google Scholar] [CrossRef]
- Cabo Verde, S.; Almeida, S.M.; Matos, J.; Guerreiro, D.; Meneses, M.; Faria, T.; Botelho, D.; Santos, M.; Viegas, C. Microbiological assessment of indoor air quality at different hospital sites. Res. Microbiol. 2015, 166, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Sautour, M.; Sixt, N.; Dalle, F.; L’Ollivier, C.; Fourquenet, V.; Calinon, C.; Paul, K.; Valvin, S.; Maurel, A.; Aho, S.; et al. Profiles and seasonal distribution of airborne fungi in indoor and outdoor environments at a French hospital. Sci. Total Environ. 2009, 407, 3766–3771. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Date | Health Unit | Season | Working Condition | Type of Room | Occupancy Range | CO2 (ppm) | T (°C) | Relative Humidity (%) | Bacteria in (CFU·m−3) Mean ± Std. | Bacteria out (CFU·m−3) Mean ± Std | Fungi in (CFU·m−3) Mean ± Std | Fungi out (CFU·m−3) Mean ± Std |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 20 June 2017 | H1 | Summer | Normal | Consulting | 1–2 | 630 | 23.6 | 61.1 | 128 ± 11 | 73 ± 32 | 8 ± 11 | 515 ± 7 |
| Ward | 1–2 | 550 | 23.2 | 55.5 | 140 ± 42 | 65 ± 7 | ||||||
| 26 June 2017 | H2 | Summer | Normal | Consulting | 1–2 | 632 | 24.2 | 49.5 | 423 ± 11 | 63 ± 18 | 33 ± 11 | 28 ± 4 |
| Ward | 2–4 | 780 | 25.8 | 56.1 | 298 ± 4 | 193 ± 32 | 153 ± 11 | 200 ± 7 | ||||
| 30 June 2017 | H2 | Summer | Normal | Ward | 2–4 | NA | NA | NA | 240 ± 21 | 105 ± 35 | 208 ± 4 | 283 ± 46 |
| 26 July 2017 | H1 | Summer | Normal | Physioth. gym | 2–4 | 528 | 24.8 | 56.5 | 408 ± 18 | 253 ± 138 | 395 ± 0 | 823 ± 39 |
| Ward | 1–2 | 441 | 24.3 | 52.2 | 170 ± 14 | 190 ± 21 | ||||||
| Day-care room | 2–4 | 405 | 24.8 | 59.9 | 155 ± 7 | 65 ± 7 | ||||||
| 29 January 2018 | H1 | Winter | Normal | Consulting | 1–2 | 718 | 22.8 | 36.6 | 105 ± 57 | 40 ± 14 | 108 ± 32 | 173 ± 4 |
| Nebulizer room | 1–2 | 666 | 22.8 | 36.2 | 253 ± 39 | 103 ± 11 | ||||||
| Ward | 1–2 | 660 | 22.7 | 37.7 | 305 ± 0 | 13 ± 4 | ||||||
| 2 February 2018 | H2 | Winter | Normal | Respirat. Physioth. | 10–20 | 1080 | 23.3 | 31.6 | 305 ± 21 | 48 ± 4 | 50 ± 21 | 53 ± 11 |
| Nebulizer room | 1–2 | 698 | 23.4 | 27.4 | 123 ± 46 | 33 ± 18 | ||||||
| Consulting | 1–2 | 745 | 23.8 | 27.8 | 410 ± 49 | 5 ± 7 | ||||||
| Ward | 2–4 | 1039 | 23.4 | 31.9 | 230 ± 42 | 108 ± 32 | 23 ± 4 | 55 ± 35 | ||||
| Treatment room | 1–2 | 709 | 24.1 | 30.7 | 240 ± 63 | 75 ± 42 | 45 ± 0 | 98 ± 11 | ||||
| Emergency | Waiting room | 10–20 | 1140 | 21.7 | 37.2 | 190 ± 7 | 40 ± 7 | |||||
| Nebulizer room | 10–20 | 698 | 23.0 | 29.3 | 85 ± 14 | 13 ± 4 | ||||||
| Treatment room | 1–2 | 672 | 24.0 | 27.8 | 150 ± 42 | 5 ± 0 | ||||||
| Treatment room | 1–2 | 590 | 23.0 | 26.9 | 93 ± 25 | 18 ± 11 | ||||||
| Consulting | 1–2 | 620 | 23.9 | 25.8 | 138 ± 4 | 5 ± 0 | ||||||
| 2 March 2018 | HC | Winter | Normal | Treatment room | 1–2 | 856 | 19.5 | 52.7 | 167 | 413 | 247 | 340 |
| Consulting | 1–2 | 984 | 21.0 | 51.0 | 133 | 200 | ||||||
| Waiting room | 5–10 | 863 | 20.2 | 50.9 | 360 | 193 | ||||||
| 5 March 2018 | HC | Winter | Emergency | Treatment room | 1–2 | 930 | 20.1 | 52.1 | 220 | 50 | 50 | 50 |
| Consulting | 1–2 | 1059 | 20.5 | 51.4 | 585 | 140 | ||||||
| Waiting room | 10–20 | 1212 | 19.3 | 54.4 | 295 | 75 | ||||||
| 17 March 2018 | HC | Winter | Emergency | Treatment room | 1–2 | 1497 | 22.1 | 54.5 | 500 | 140 | 207 | 187 |
| Waiting room | 10–20 | 1860 | 19.3 | 65.5 | 487 | 140 | ||||||
| Consulting | 1–2 | 1157 | 21.3 | 54.3 | NA | NA |
| CO2 | Temperature | Relative Humidity | Bacteria in | Bacteria in-out | Fungi in | Fungi in-out | |||
|---|---|---|---|---|---|---|---|---|---|
| Health Unit * Working Condition | Two-way ANOVA p-value a | 0.040 | 0.390 | 0.239 | 0.001 | 0.000 | 0.016 | 0.000 | |
| Normal | One-way ANOVA p-value a/Partial Eta Squared | 0.179/0.349 | 0.000/0.931 | 0.000/0.976 | 0.705/0.043 | 0.000/0.659 | 0.000/0.812 | 0.001/0.609 | |
| H1–H2 | Post-hoc Tuckey p-value a | 0.078 | 0.001 | 0.959 | 0.057 | 0.004 | |||
| H1–HC | 0.000 | 0.000 | 0.001 | 0.000 | 0.514 | ||||
| H2–HC | 0.000 | 0.000 | 0.000 | 0.000 | 0.002 | ||||
| Emergency | H2–HC | One-way ANOVA p-value a/Partial Eta Squared | 0.014/0.507 | 0.002/0.671 | 0.000/0.896 | 0.000/0.711 | 0.000/0.715 | 0.000/0.688 | 0.000/0.729 |
| H2 | Normal–Emergency | One-way ANOVA p-value a/Partial Eta Squared | 0.426/0.081 | 0.308/0.129 | 0.836/0.006 | 0.002/0.419 | 0.002/0.420 | 0.066/0.176 | 0.000/0.637 |
| HC | Normal–Emergency | 0.102/0.336 | 0.790/0.011 | 0.255/0.180 | 0.109/0.371 | 0.002/0.829 | 0.058/0.477 | 0.004/0.772 | |
| Parameter | t | p-Value (Two-Tail) a |
|---|---|---|
| CO2 (ppm) | −2.84 | 0.014 |
| Temperature (°C) | 3.08 | 0.009 |
| Relative Humidity (%) | 11.3 | 0.000 |
| Bacteria in (CFU·m−3) | −0.0325 | 0.974 |
| Bacteria in-out (CFU·m−3) | −2.20 | 0.036 |
| Fungi in (CFU·m−3) | 2.86 | 0.010 |
| Fungi in-out (CFU·m−3) | −4.34 | 0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fonseca, A.; Abreu, I.; Guerreiro, M.J.; Abreu, C.; Silva, R.; Barros, N. Indoor Air Quality and Sustainability Management—Case Study in Three Portuguese Healthcare Units. Sustainability 2019, 11, 101. https://doi.org/10.3390/su11010101
Fonseca A, Abreu I, Guerreiro MJ, Abreu C, Silva R, Barros N. Indoor Air Quality and Sustainability Management—Case Study in Three Portuguese Healthcare Units. Sustainability. 2019; 11(1):101. https://doi.org/10.3390/su11010101
Chicago/Turabian StyleFonseca, Ana, Isabel Abreu, Maria João Guerreiro, Cristina Abreu, Ricardo Silva, and Nelson Barros. 2019. "Indoor Air Quality and Sustainability Management—Case Study in Three Portuguese Healthcare Units" Sustainability 11, no. 1: 101. https://doi.org/10.3390/su11010101
APA StyleFonseca, A., Abreu, I., Guerreiro, M. J., Abreu, C., Silva, R., & Barros, N. (2019). Indoor Air Quality and Sustainability Management—Case Study in Three Portuguese Healthcare Units. Sustainability, 11(1), 101. https://doi.org/10.3390/su11010101