
Local Response to the COVID-19 Pandemic: The Case of Indonesia



Abstract
:1. Introduction
2. Big Bang Decentralization
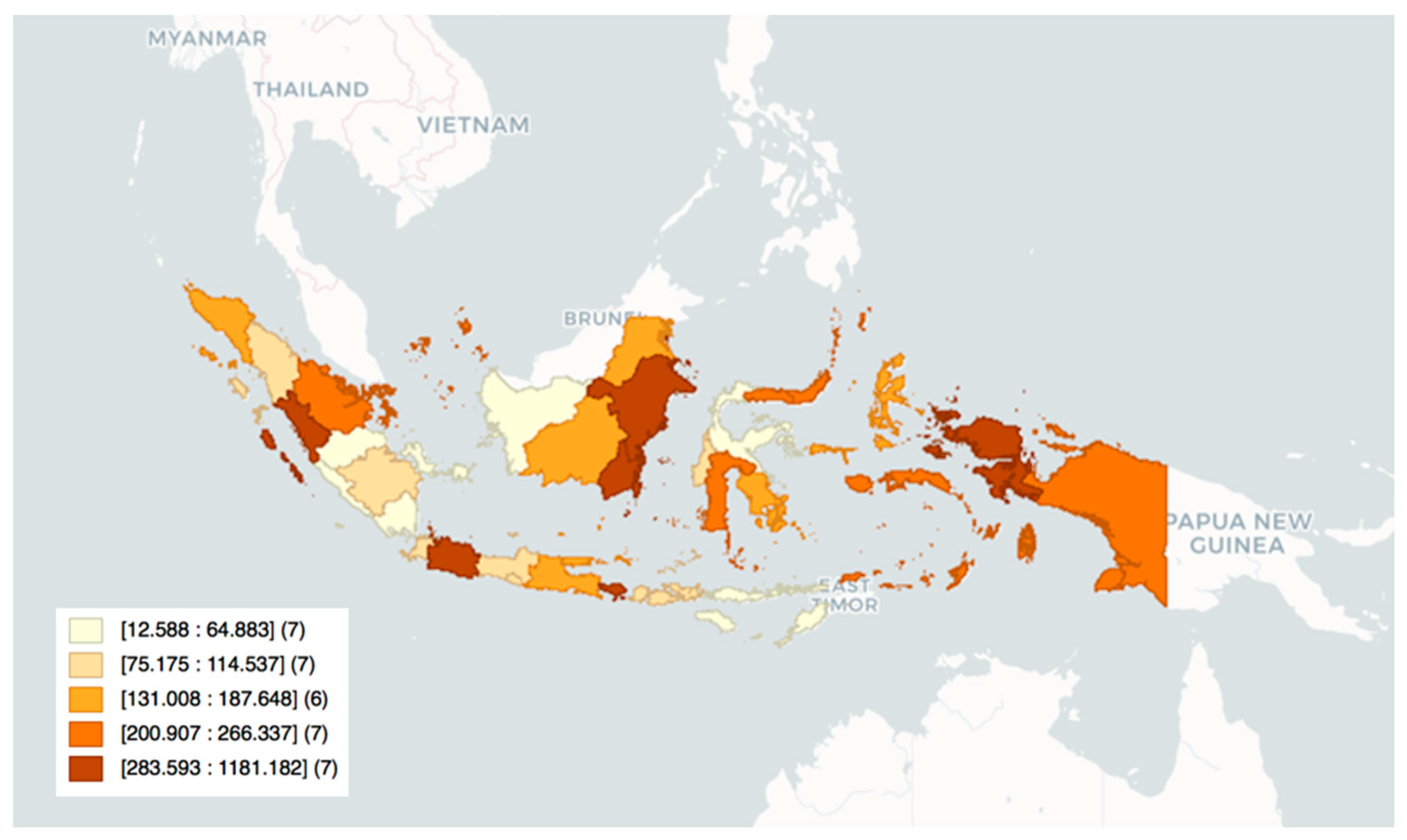
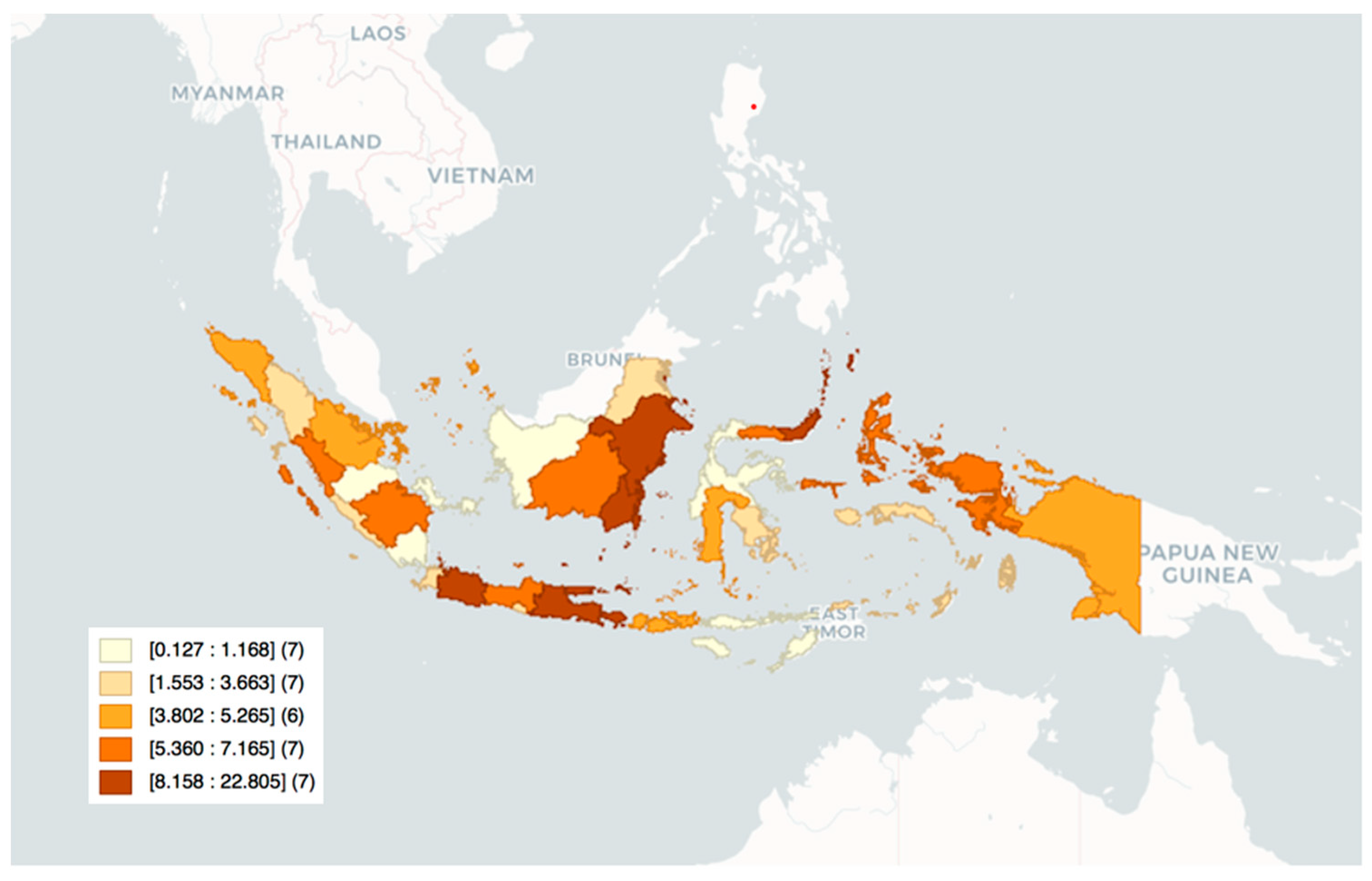
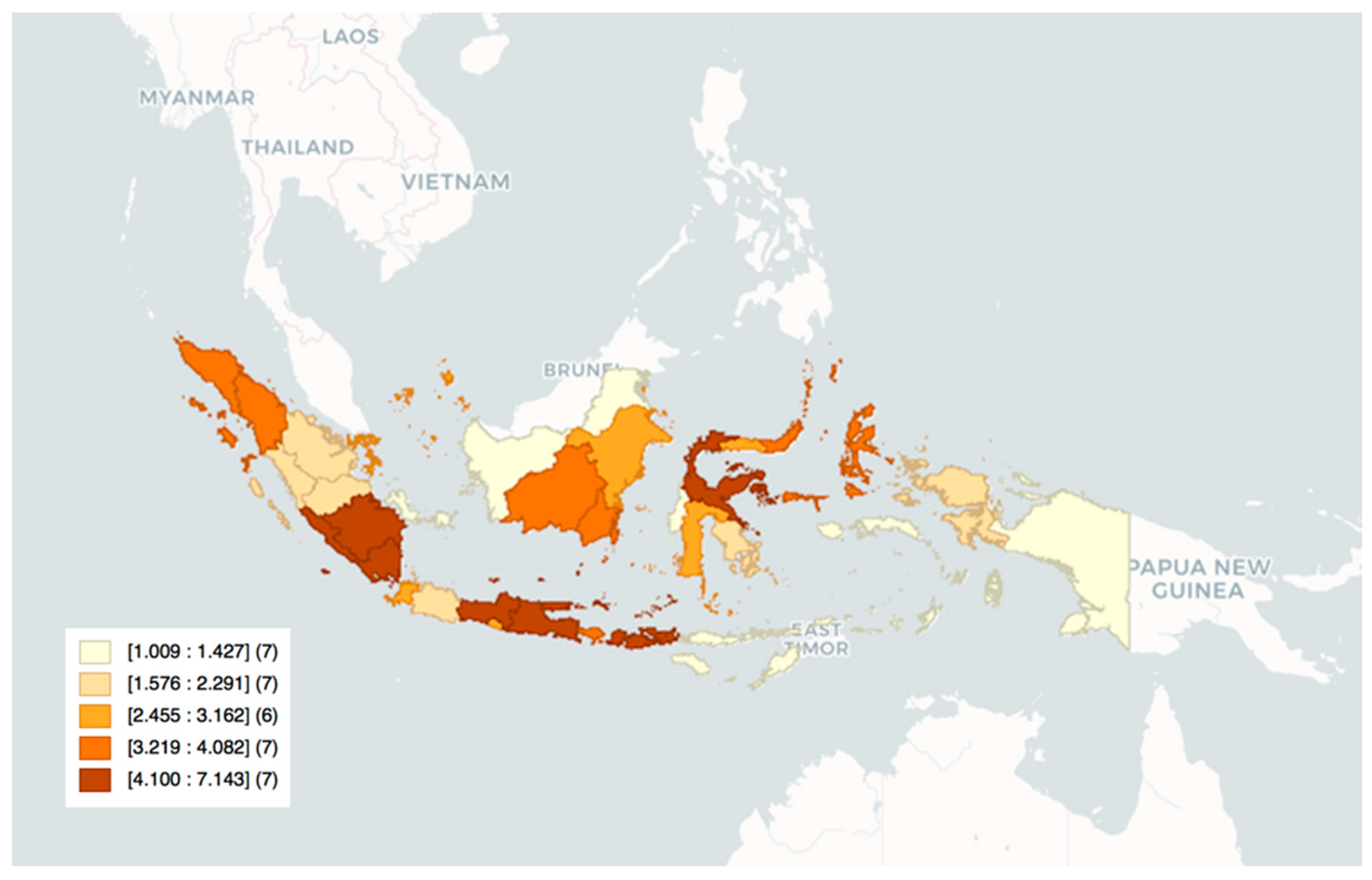
3. COVID-19 Cases and Deaths in Indonesia’s Provinces
4. Pandemic Response
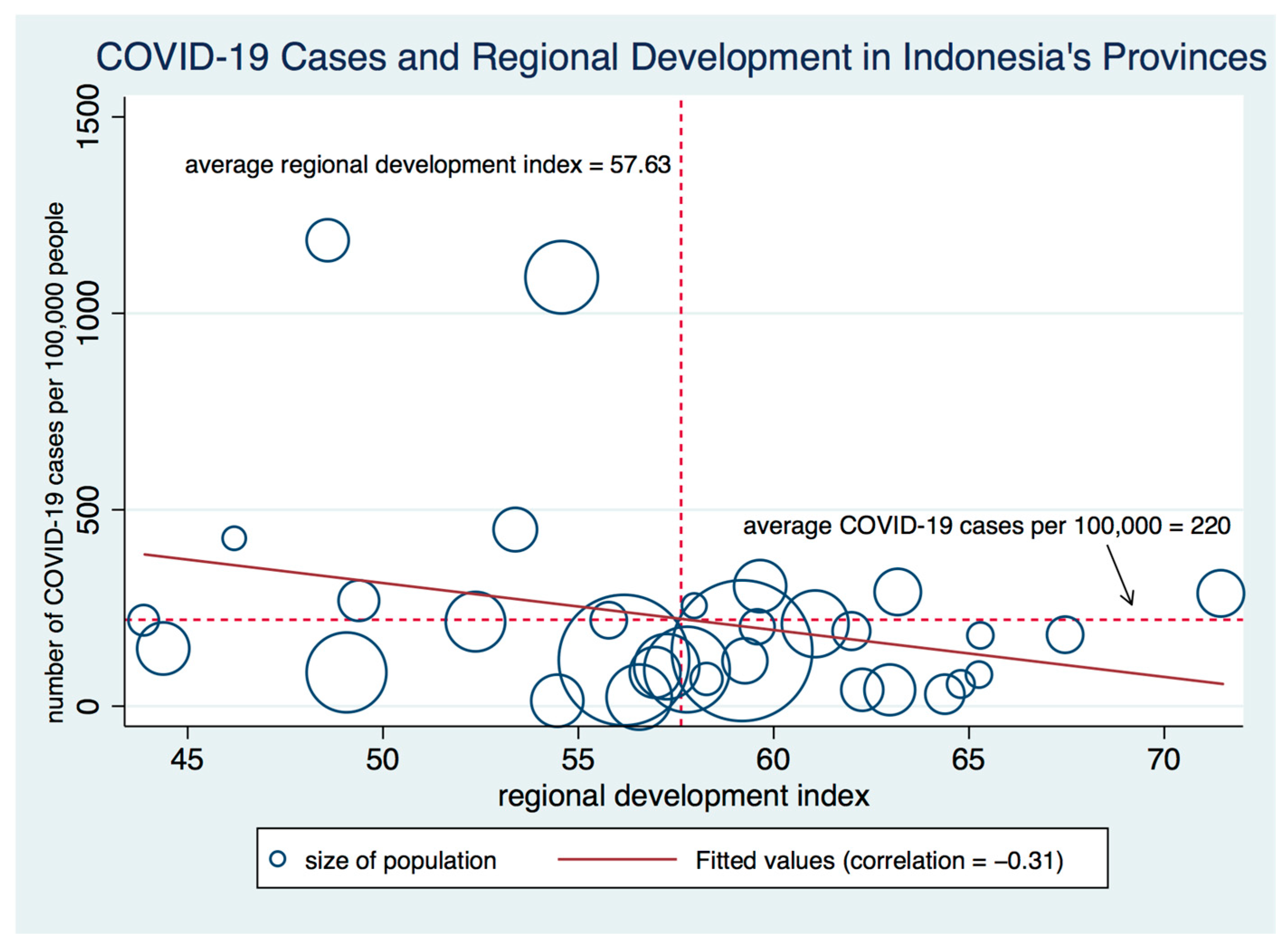
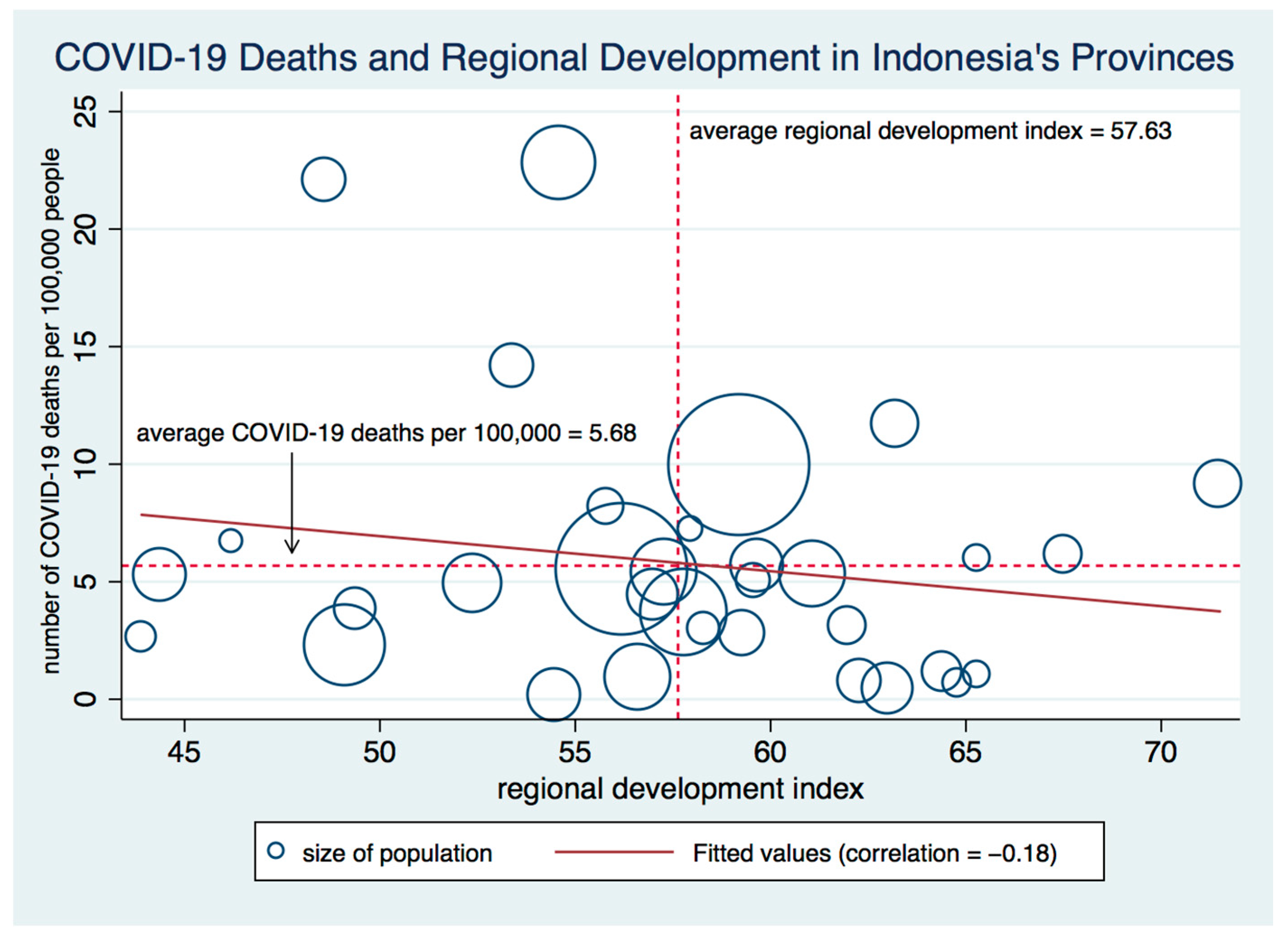
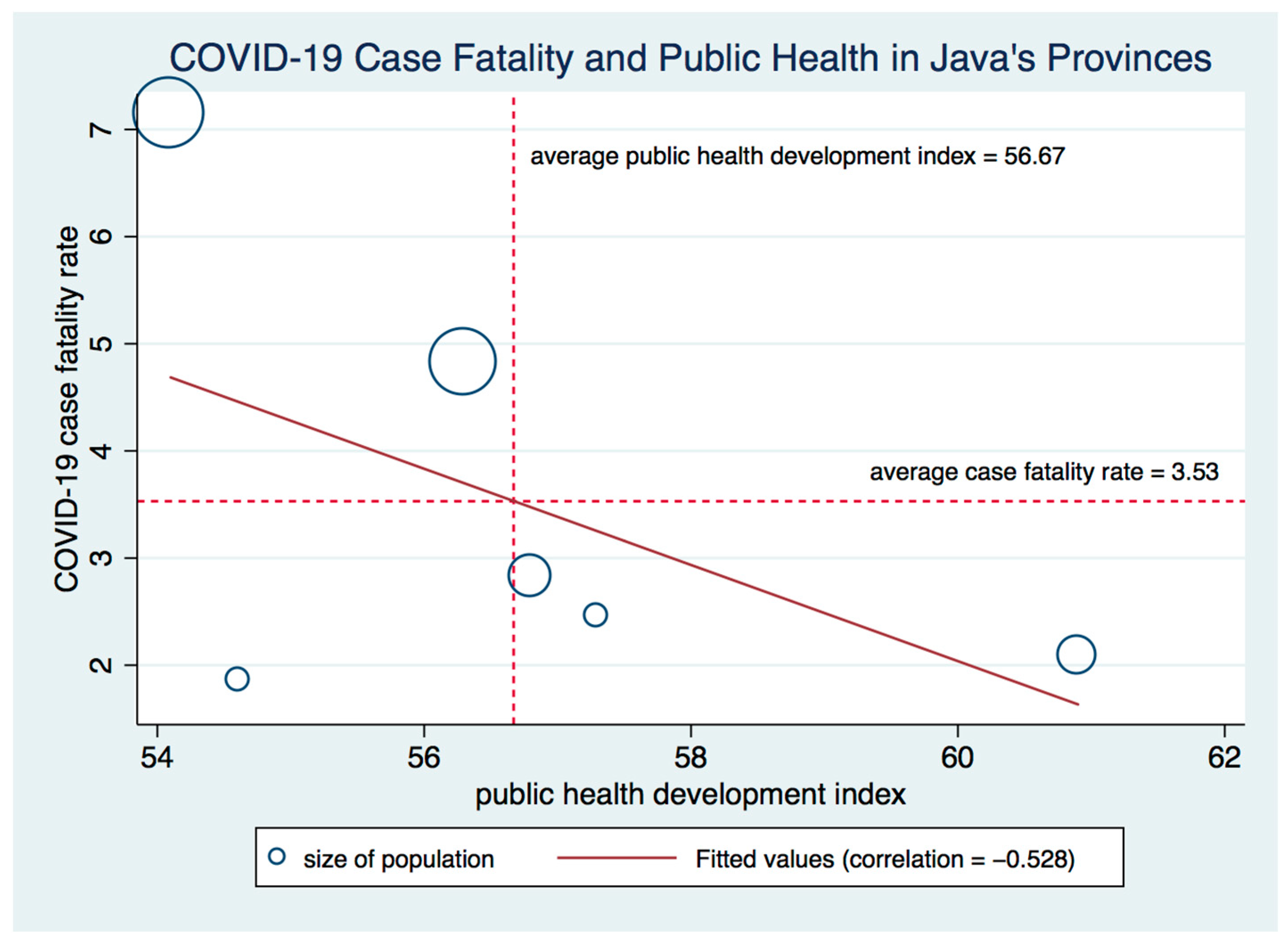
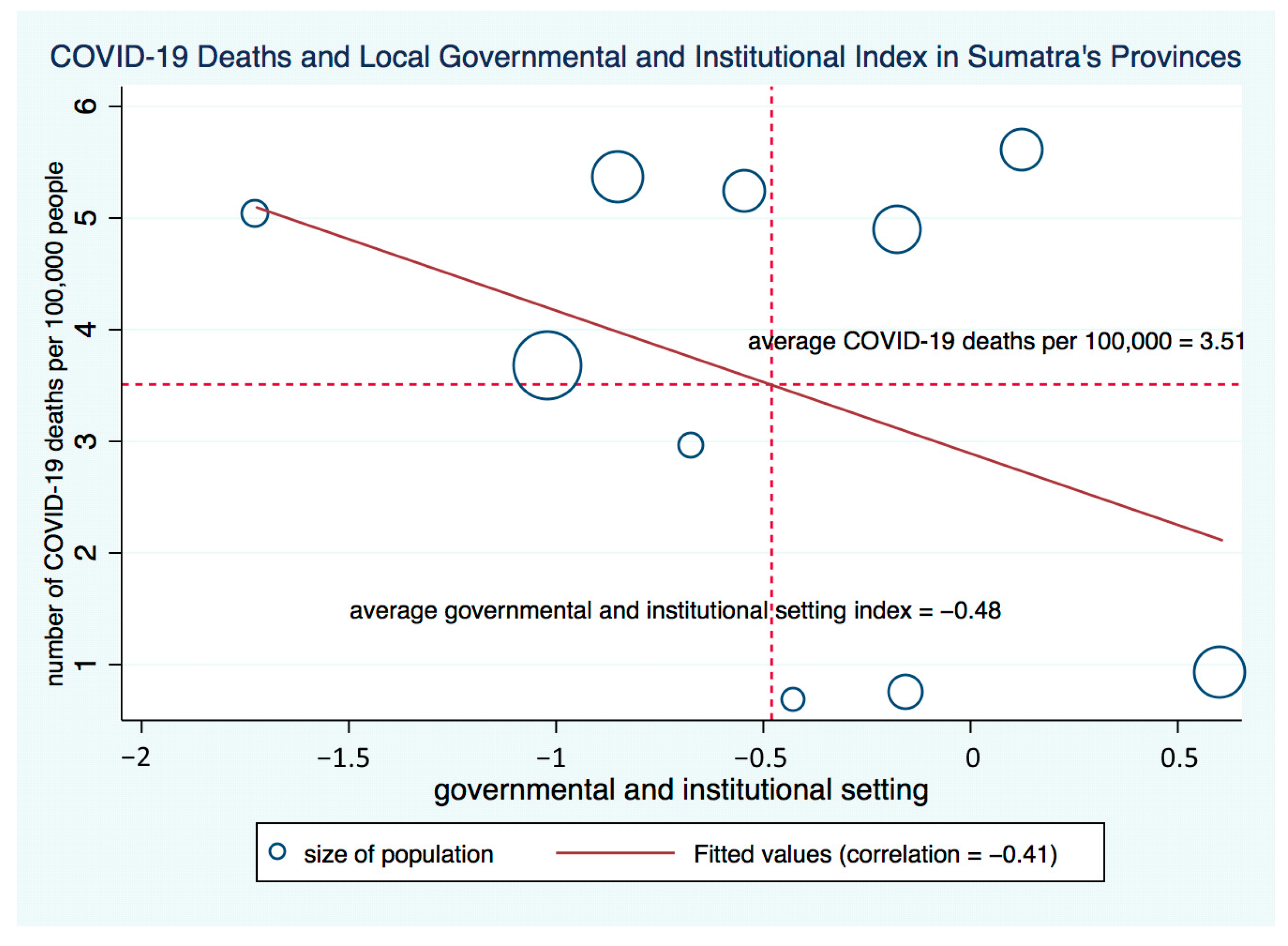
5. The Relationship between COVID-19 Cases and Deaths and Provincial Governments
6. Discussion and Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) Number of COVID-19 cases per 100,000 people | 1.000 | ||||||||||
| (2) Number of COVID-19 deaths per 100,000 people | 0.915 | 1.000 | |||||||||
| (3) COVID-19 case-fatality rate (%) | −0.215 | 0.116 | 1.000 | ||||||||
| (4) Public health development index | 0.286 | 0.379 | 0.167 | 1.000 | |||||||
| (5) Regional sustainable development index | −0.306 | −0.183 | 0.131 | 0.177 | 1.000 | ||||||
| (6) Provincial competitiveness index | 0.500 | 0.642 | 0.269 | 0.679 | 0.104 | 1.000 | |||||
| (7) Macroeconomic stability | 0.642 | 0.733 | 0.223 | 0.484 | −0.129 | 0.864 | 1.000 | ||||
| (8) Government and institutional setting | 0.331 | 0.402 | 0.084 | 0.364 | 0.200 | 0.784 | 0.555 | 1.000 | |||
| (9) Financial, business and manpower conditions | 0.442 | 0.549 | 0.246 | 0.653 | 0.149 | 0.888 | 0.835 | 0.521 | 1.000 | ||
| (10) Quality of life and infrastructure development | 0.241 | 0.442 | 0.337 | 0.749 | 0.126 | 0.777 | 0.470 | 0.520 | 0.583 | 1.000 | |
| (11) Number of hospital units per 100,000 people | 0.743 | 0.604 | −0.216 | 0.131 | −0.274 | 0.190 | 0.270 | 0.109 | 0.180 | 0.069 | 1.000 |
| Variables | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) Number of COVID-19 cases per 100,000 people | 1.000 | ||||||||||
| (2) Number of COVID-19 deaths per 100,000 people | 0.798 | 1.000 | |||||||||
| (3) COVID-19 case-fatality rate (%) | −0.341 | 0.219 | 1.000 | ||||||||
| (4) Public health development index | 0.362 | 0.155 | −0.283 | 1.000 | |||||||
| (5) Regional sustainable development index | −0.233 | −0.523 | −0.365 | 0.364 | 1.000 | ||||||
| (6) Provincial competitiveness index | 0.438 | 0.133 | −0.355 | 0.869 | 0.184 | 1.000 | |||||
| (7) Macroeconomic stability | 0.237 | 0.332 | 0.081 | 0.755 | 0.090 | 0.671 | 1.000 | ||||
| (8) Government and institutional setting | −0.123 | −0.405 | −0.163 | −0.439 | −0.039 | −0.062 | −0.523 | 1.000 | |||
| (9) Financial, business and manpower conditions | 0.185 | 0.017 | −0.246 | 0.933 | 0.440 | 0.819 | 0.685 | −0.493 | 1.000 | ||
| (10) Quality of life and infrastructure development | 0.742 | 0.558 | −0.361 | 0.669 | −0.201 | 0.661 | 0.389 | −0.433 | 0.613 | 1.000 | |
| (11) Number of hospital units per 100,000 people | −0.141 | −0.216 | −0.393 | −0.012 | 0.199 | −0.254 | −0.219 | −0.468 | 0.126 | 0.167 | 1.000 |
| Variables | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) | (11) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| (1) Number of COVID-19 cases per 100,000 people | 1.000 | ||||||||||
| (2) Number of COVID-19 deaths per 100,000 people | 0.962 | 1.000 | |||||||||
| (3) COVID-19 case-fatality rate (%) | −0.562 | −0.325 | 1.000 | ||||||||
| (4) Public health development index | 0.289 | 0.225 | −0.528 | 1.000 | |||||||
| (5) Regional sustainable development index | −0.472 | −0.321 | 0.564 | 0.039 | 1.000 | ||||||
| (6) Provincial competitiveness index | 0.541 | 0.675 | 0.001 | 0.618 | 0.102 | 1.000 | |||||
| (7) Macroeconomic stability | 0.595 | 0.758 | 0.116 | 0.380 | 0.014 | 0.957 | 1.000 | ||||
| (8) Government and institutional setting | 0.638 | 0.670 | −0.348 | 0.805 | −0.160 | 0.918 | 0.817 | 1.000 | |||
| (9) Financial, business and manpower conditions | 0.454 | 0.632 | 0.210 | 0.460 | 0.284 | 0.935 | 0.907 | 0.787 | 1.000 | ||
| (10) Quality of life and infrastructure development | −0.212 | −0.260 | −0.270 | 0.709 | 0.264 | 0.263 | 0.063 | 0.341 | 0.033 | 1.000 | |
| (11) Number of hospital units per 100,000 people | 0.739 | 0.635 | −0.507 | −0.287 | −0.543 | −0.137 | 0.005 | −0.040 | −0.156 | −0.543 | 1.000 |
References
- Pepinsky, T. COVID-19 and Democracy in Indonesia: Short-Term Stability and Long-Term Threats. 26 January. Available online: https://www.brookings.edu/blog/order-from-chaos/2021/01/26/covid-19-and-democracy-in-indonesia-short-term-stability-and-long-term-threats/ (accessed on 24 March 2021).
- Kapucu, N.; van Wart, M. The evolving role of the public sector in managing catastrophic disasters lessons learned. Adm. Soc. 2006, 38, 1–30. [Google Scholar] [CrossRef] [Green Version]
- Baker, D.; Refsgaard, K. Institutional development and scale matching in disaster response management. Ecol. Econ. 2007, 63, 331–343. [Google Scholar] [CrossRef]
- Willoughby, K.; Bathurst, D.; Devereaux, G.; Goss, K.C.; Kellar, E.; Metzenbaum, S.; Hoeve, J.T.; Ucellini, L.W. Emergency and Disaster Management Case Study; National Academy of Public Administration: Washington, DC, USA, 2020. [Google Scholar]
- Ahrens, T.; Ferry, L. Financial resilience of English local government in the aftermath of COVID-19. J. Public Budg. Account. Financ. Manag. 2020, 32, 813–823. [Google Scholar] [CrossRef]
- Huynh, D.; Tosun, M.S.; Yilmaz, S. All-of-government response to the COVID-19 pandemic: The case of Vietnam. Public Adm. Dev. 2020, 40, 236–239. [Google Scholar] [CrossRef]
- World Bank. World Bank, Spending for Development: Making the Most of Indonesia’s New Opportunities; World Bank: Jakarta, Indonesia, 2007. [Google Scholar]
- Hofman, B.; Kaiser, K.; Alm, J.; Martinez-Vazquez, J.; Indrawati, S. The Making of the ‘Big Bang’ and its Aftermath: A Political Economy Perspective. In Reforming Intergovernmental Fiscal Relations and the Rebuilding of Indonesia; Alm, J., Martinez-Vazquez, J., Mulyani Indrawati, S., Eds.; Edward Elgar Publishing: Cheltenham, UK, 2013. [Google Scholar]
- Buehler, M. Decentralisation and Local Democracy in Indonesia: The Marginalisation of the Public Sphere. In Problems of Democratisation in Indonesia: Elections, Institutions and Society; Aspinall, E., Mietzner, M., Eds.; ISEAS–Yusof Ishak Institute: Singapore, 2010; pp. 267–285. [Google Scholar]
- Mahi, B.R. Indonesian Decenteralization: Evaluation, Recent Movement and Future Perspectives. J. Indones. Econ. Bus. 2016, 31, 119–133. [Google Scholar] [CrossRef] [Green Version]
- Fitrani, F.; Hofman, B.; Kaiser, K. Unity in diversity? The creation of new local governments in a decentralizing Indonesia. Bull. Indones. Econ. Stud. 2005, 41, 57–79. [Google Scholar] [CrossRef]
- Smoke, P. Expenditure Assignment under Indonesia’s Emerging Decentralization: A Review of Progress and Issues for the Future. In Reforming Intergovernmental Fiscal Relations and the Rebuilding of Indonesia; Edward Elgar Publishing: Cheltenham, UK, 2013; pp. 02–33. [Google Scholar]
- Lewis, B. Local government spending and service delivery in Indonesia: The perverse effects of subnational fiscal resources. Reg. Stud. 2017, 51, 1695–1707. [Google Scholar] [CrossRef]
- Human Rights Watch. Indonesia: Weak Public Health Response to COVID-19. 13 January. Available online: https://www.hrw.org/news/2021/01/13/indonesia-weak-public-health-response-covid-19# (accessed on 18 February 2021).
- Huhn, N. Indonesia’s COVID-19 Response. Available online: https://www.outbreakobservatory.org/outbreakthursday-1/10/22/2020/indonesias-covid-19-response (accessed on 22 October 2020).
- Daniel, B.J.; Diningrat, A. How to Fix Indonesia’s Covid-19 Governance Problem. 24 September. Available online: https://indonesiaatmelbourne.unimelb.edu.au/how-to-fix-indonesias-covid-19-governance-problem/ (accessed on 24 March 2021).
- Djalante, R.; Lassa, J.; Setiamarga, D.; Sudjatma, A.; Indrawan, M.; Haryanto, B.; Mahfud, C.; Sinapoy, M.S.; Djalante, S.; Rafliana, I.; et al. Review and analysis of current responses to COVID-19 in Indonesia: Period of January to March 2020. Prog. Disaster Sci. 2020, 6, 100091. [Google Scholar] [CrossRef]
- Nyoman, S.I.; Wirawan, A.; Swandewi Astuti, P.A. ‘Nine Months and No Progress’: What Went Wrong in Indonesia’s COVID-19 Responses and What Can Be Done. Edited by Beth Daley. 1 December. Available online: https://theconversation.com/nine-months-and-no-progress-what-went-wrong-in-indonesias-covid-19-responses-and-what-can-be-done-145850 (accessed on 18 February 2021).
- Al Jazeera. Indonesia’s Coronavirus Response Revealed: Too Little, Too Late. 22 April 2020. Available online: https://www.aljazeera.com/news/2020/4/22/indonesias-coronavirus-response-revealed-too-little-too-late (accessed on 18 February 2021).
- World Health Organization. Available online: https://www.who.int/news-room/feature-stories/detail/covid-19-ambassador-assists-disease-control-in-south-sulawesi-indonesia#:~:text=COVID%2D19%20Ambassador%20assists%20disease%20control%20in%20South%20Sulawesi%2C%20Indonesia,-16%20June%202020&text=The%20 (accessed on 16 June 2020).
- Muhammad Beni, S. COVID-19 Is Eroding Indonesian Local Media’s Role as Watchdog. 24 November 2020. Available online: https://www.newmandala.org/covid-19-is-eroding-indonesian-local-medias-role-as-watchdog/ (accessed on 24 March 2021).
- Human Rights Watch. World Report 2021 Events of 2020. 2021. Available online: https://www.hrw.org/sites/default/files/media_2021/01/2021_hrw_world_report.pdf (accessed on 14 February 2021).
- Rahma, H.; Fauzi, A.; Juanda, B.; Widjojanto, B. Development of a Composite Measure of Regional Sustainable Development in Indonesia. Sustainability 2019, 11, 5861. [Google Scholar] [CrossRef] [Green Version]
- Kusumawardani, S.N.; Nambiar, D.; Trihono; Hosseinpoor, A.R. Subnational regional inequality in the public health development index in Indonesia. Glob. Health Action 2018, 11, 41–53. [Google Scholar] [CrossRef] [Green Version]
- Mulya, A.; Ahmad, N.B.; Vania Lavi, D.; Giap, T.K. Competitiveness, Trade, Liveability and Productivity in ASEAN Economies. Govinsider. 28 August 2017. Available online: https://govinsider.asia/wp-content/uploads/docs/ACI_report_Indonesia.pdf (accessed on 28 February 2021).
- Humanitarian Data Exchange. Indonesia: Coronavirus (COVID-19) Subnational Cases. Available online: https://data.humdata.org/dataset/indonesia-covid-19-cases-recoveries-and-deaths-per-province (accessed on 12 November 2020).
- CEIC. Indonesia: Number of Hospitals: CEIC. Global Economic Data, Indicators, Charts & Forecasts. Available online: https://www.ceicdata.com/en/indonesia/number-of-hospitals (accessed on 10 January 2021).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Masyrafah, H.; McKeon, J. Post-Tsunami Aid Effectiveness in Aceh: Proliferation and Coordination in Reconstruction; Wolfensohn Center for Development Working Paper 6, November 2008; Brookings Institution: Washington, DC, USA, 2016. [Google Scholar]









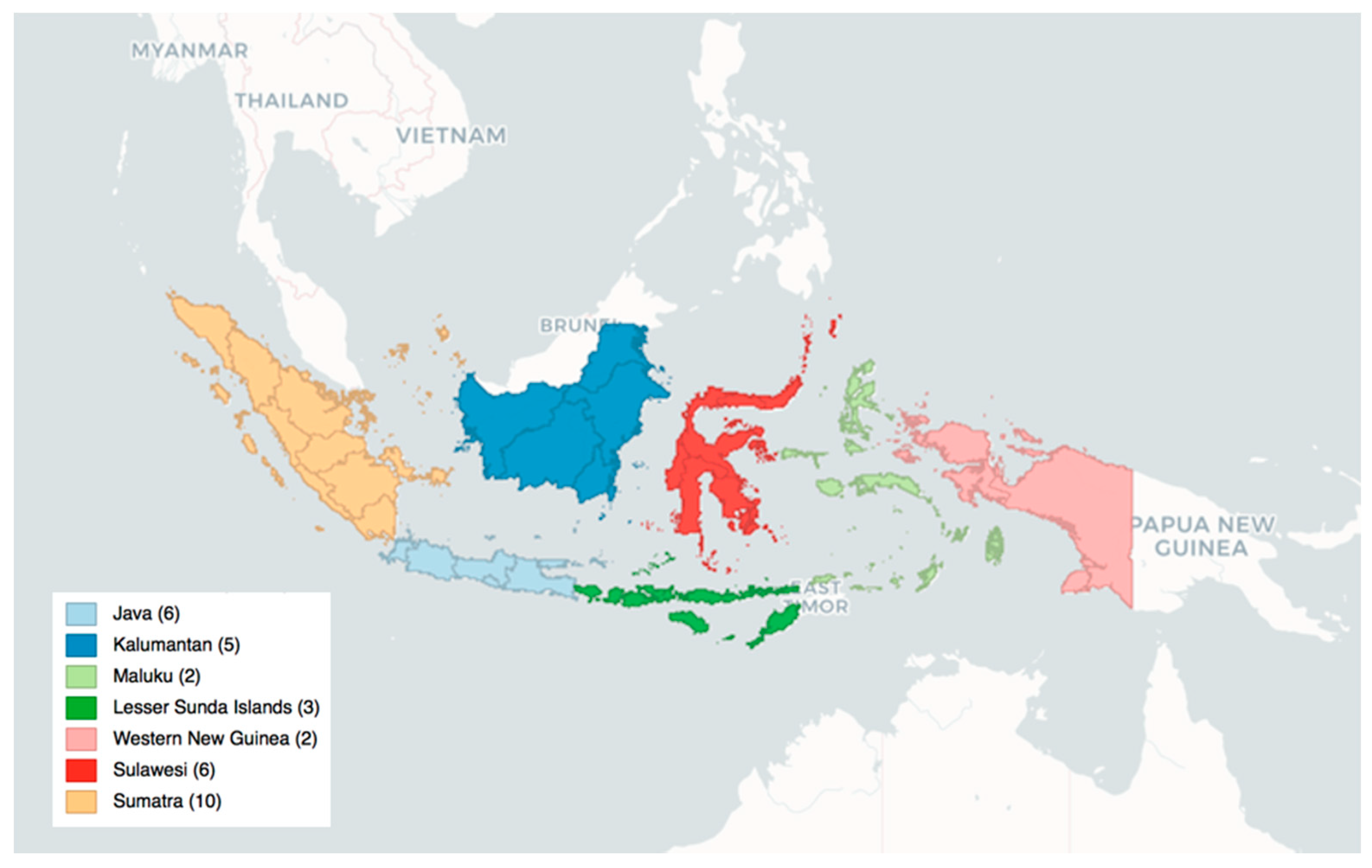
| Region | Provinces |
|---|---|
| Java | Banten, Jakarta, West Java, Central Java, S.R. Yogyakarta, East Java |
| Kalimantan | West Kalimantan, Central Kalimantan, North Kalimantan, East Kalimantan, South Kalimantan |
| Maluku Islands | North Maluku, Province of Maluku |
| Lesser Sunda Islands | Bali, West Nusa Tenggara, East Nusa Tenggara |
| Western New Guinea | West Papua, Province of Papua |
| Sulawesi | North Sulawesi, Gorontalo, Central Sulawesi, West Sulawesi, South Sulawesi, Southeast Sulawesi |
| Sumatra | Aceh, North Sumatra, West Sumatra, Riau, Riau Islands, Jambi, Bengkulu, South Sumatra, Bangka Belitung Islands, Lampung |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sevindik, I.; Tosun, M.S.; Yilmaz, S. Local Response to the COVID-19 Pandemic: The Case of Indonesia. Sustainability 2021, 13, 5620. https://doi.org/10.3390/su13105620
Sevindik I, Tosun MS, Yilmaz S. Local Response to the COVID-19 Pandemic: The Case of Indonesia. Sustainability. 2021; 13(10):5620. https://doi.org/10.3390/su13105620
Chicago/Turabian StyleSevindik, Irem, Mehmet Serkan Tosun, and Serdar Yilmaz. 2021. "Local Response to the COVID-19 Pandemic: The Case of Indonesia" Sustainability 13, no. 10: 5620. https://doi.org/10.3390/su13105620
APA StyleSevindik, I., Tosun, M. S., & Yilmaz, S. (2021). Local Response to the COVID-19 Pandemic: The Case of Indonesia. Sustainability, 13(10), 5620. https://doi.org/10.3390/su13105620