
Application of an Innovative Model for the Risk Management of COVID-19 in a Multinational Manufacturing Company

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Company Description
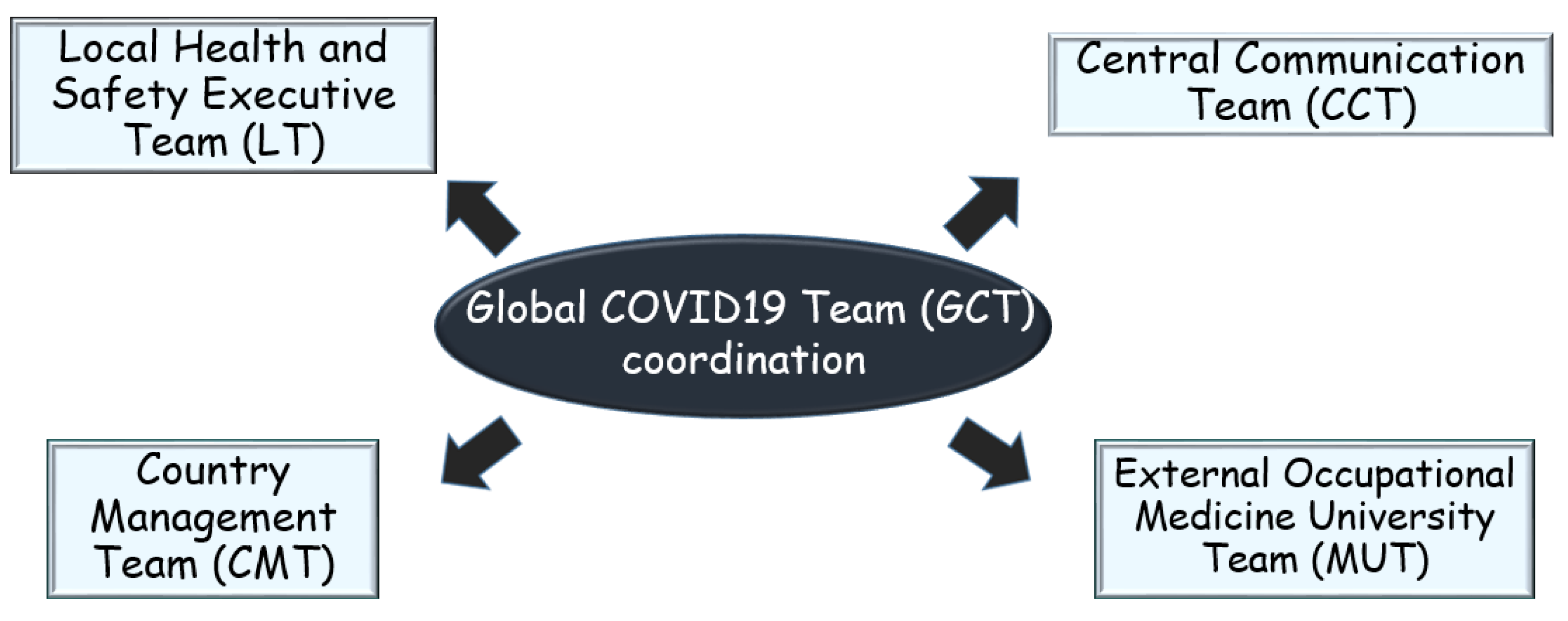
2.2. Risk Management Model: Creation of the Network of Teams
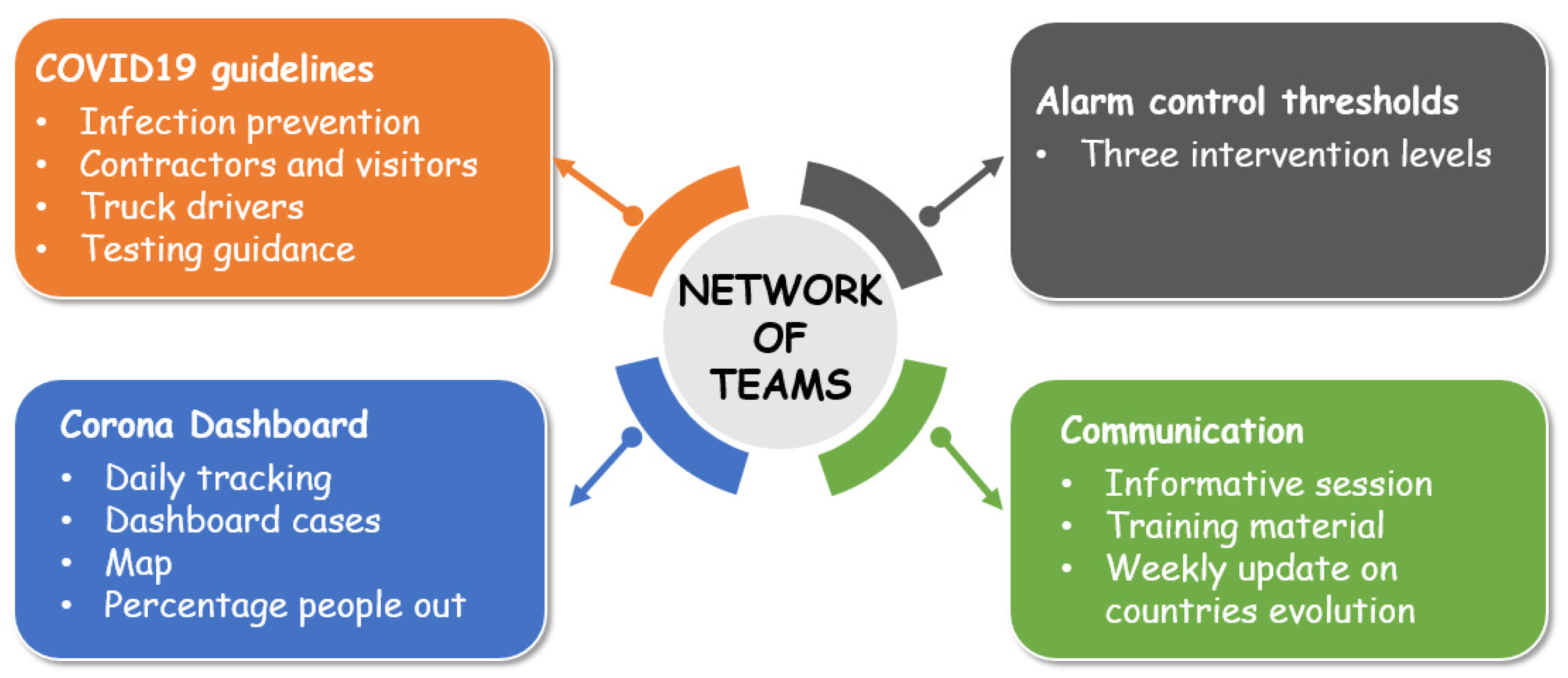
2.3. Risk Management Model: The Operative Tools
- -
- physical distancing (2 m);
- -
- use of certified medical masks and, if a proper distance cannot be maintained, additional PPE, such as a face shield, goggles, close-fitting safety glasses, and in a few specific situations, gloves (for delivering or accepting equipment, spare parts or documents, etc.);
- -
- hand hygiene and proper workplace cleaning and disinfection practices;
- -
- isolation of confirmed cases and quarantine for suspected cases;
- -
- testing strategies, providing recommendations on the usefulness and limitations of molecular, antigenic and serologic tests, to be applied according to the local availability [12].
2.4. Evaluation of the Application of the Model and Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. China Novel Coronavirus Investigating and Research Team. A Novel Coronavirus from Patients with Pneumonia in China. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- ICTV. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Director-General’s Opening Remarks at the Media Briefing on COVID19—March 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Alkahtani, M.; Omair, M.; Khalid, Q.S.; Hussain, G.; Ahmad, I.; Pruncu, C. A COVID-19 supply chain management strategy based on variable production under uncertain environment conditions. Int. J. Environ. Res. Public Health 2021, 18, 1662. [Google Scholar] [CrossRef] [PubMed]
- ECDC. COVID-19 Clusters and Outbreaks in Occupational Setting in the EU/EEA and UK; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2020. [Google Scholar]
- Zisook, R.E.; Monnot, A.; Parker, J.; Gaffney, S.; Dotson, S.; Unice, K. Assessing and managing the risks of COVID-19 in the workplace: Applying industrial hygiene (IH)/occupational and environmental health and safety (OEHS) frameworks. Toxicol. Ind. Health 2020, 36, 607–618. [Google Scholar] [CrossRef] [PubMed]
- Cai, M.; Luo, J. Influence of COVID-19 on Manufacturing Industry and Corresponding Countermeasures from Supply Chain Perspective. J. Shanghai Jiaotong Univ. (Sci.) 2020, 25, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Marinaccio, A.; Boccuni, F.; Rondinone, B.M.; Brusco, A.; D’Amario, S.; Iavicoli, S. Occupational factors in the COVID-19 pandemic in Italy: Compensation claims applications support establishing an occupational surveillance system. Occup. Environ. Med. 2020, 77, 818–821. [Google Scholar] [CrossRef] [PubMed]
- Italian Workers’ Compensation Authority (INAIL). Documento Tecnico Sulla Possibile Rimodulazione Delle Misure di Contenimento del Contagio da SARS-CoV-2 Nei Luoghi di Lavoro e Strategie di Prevenzione. April 2020. Available online: https://www.inail.it/cs/internet/comunicazione/pubblicazioni/catalogogenerale/pubbl-rimodulazione-contenimento-covid19-sicurezza-lavoro.html (accessed on 25 April 2021).
- Iavicoli, S.; Boccuni, F.; Buresti, G.; Gagliardi, D.; Persechino, B.; Valenti, A.; Rondinone, B.M. Risk assessment at work and prevention strategies on COVID-19 in Italy. PLoS ONE 2021, 16, e0248874. [Google Scholar] [CrossRef] [PubMed]
- Koh, D.; Goh, H.P. Occupational health responses to COVID-19: What lessons can we learn from SARS? J. Occup. Health 2020, 62, e12128. [Google Scholar] [CrossRef] [PubMed]
- CDC. Guidance for Expanded Screening Testing to Reduce Silent Spread of SARS-CoV-2; Center for Disease Control: Atlanta, GA, USA, 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/php/opemn-america/expanded-screening-testing.htlm (accessed on 25 April 2021).
- Barnes, M.; Sax, P.E. Challenges of “Return to Work” in an Ongoing Pandemic. N. Engl. J. Med. 2020, 383, 779–786. [Google Scholar] [CrossRef] [PubMed]
- CDC. Interim Guidance for Businesses and Employers Responding to Coronavirus Disease 2019 (COVID-19); Center for Disease Control: Atlanta, GA, USA, 2020; Available online: https://www.cdc.gov/coronavirus/2019-ncov/community/guidance-business-response.html (accessed on 25 April 2021).
- Prem, K.; Liu, Y.; Russell, T.W.; Kucharski, A.J.; Eggo, R.M.; Davies, N.; Centre for the Mathematical Modelling of Infectious Diseases COVID-19 Working Group; Jit, M.; Klepac, P. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: A modelling study. Lancet Public Health 2020, 5, e261–e270. [Google Scholar] [CrossRef] [Green Version]
- EN ISO 10993-1:2010. Biological and Clinical Evaluation of Medical Devices; European Committee for Standardization: Bruxelles, Belgium, 2010. [Google Scholar]
- EN 14683:2019. Medical Face Masks—Requirements and Test Methods; European Committee for Standardization: Bruxelles, Belgium, 2019. [Google Scholar]
- ECDC. Cloth Masks and Mask Sterilisation as Options in Case of Shortage of Surgical Masks and Respirators—26 March 2020; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2020; Available online: https://www.ecdc.europa.eu/sites/default/files/documents/Cloth-face-masks-in-caseshortage-surgical-masks-respirators2020-03-26.pdf (accessed on 25 April 2021).
- WHO. Advice on the Use of Masks in the Context of COVID-19: Interim Guidance; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Davies, A.; Thompson, K.A.; Giri, K.; Kafatos, G.; Walker, J.; Bennett, A. Testing the efficacy of homemade masks: Would they protect in an influenza pandemic? Disaster Med. Public Health Prep. 2013, 7, 413–418. [Google Scholar] [CrossRef] [PubMed]
- MacIntyre, C.R.; Seale, H.; Dung, T.C.; Hien, N.T.; Nga, P.T.; Chughtai, A.A.; Rahman, B.; Dwyer, D.E.; Wang, Q. A cluster randomised trial of cloth masks compared with medical masks in healthcare workers. BMJ Open 2015, 5, e006577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ourworldindata. Coronavirus Pandemic Data Explorer. Available online: https://ourworldindata.org/coronavirus-data-explorer (accessed on 25 April 2021).
- Muller, M. Dynamic Time Warping. In Information Retrieval for Music and Motion; Muller, M., Ed.; Springer: Heidelberg, Germany, 2007; pp. 69–84. [Google Scholar]
- Sakoe, H.; Chiba, S. Dynamic programming algorithm optimization for spoken word recognition. IEEE Trans. Acoust. Speech Signal Proc. 1978, 26, 43–49. [Google Scholar] [CrossRef] [Green Version]
- SAS. The SAS System for Windows; Release 9.4; SAS Institute: Cary, NC, USA, 2011. [Google Scholar]
- Nørgaard, S.K.; Vestergaard, L.S.; Nielsen, J.; Richter, L.; Schmid, D.; Bustos, N.; Braye, T.; Athanasiadou, M.; Lytras, T.; Denissov, G.; et al. Real-time monitoring shows substantial excess all-cause mortality during second wave of COVID-19 in Europe, October to December 2020. Euro Surveill. 2021, 26, 2002023. [Google Scholar]
- Aronsson, G.; Gustafsson, K.; Dallner, M. Sick but yet at work. An empirical study of sickness presenteeism. J. Epidemiol. Community Health 2000, 54, 502–509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, M.G. Non relocatable Occupations at Increased Risk during Pandemics: United States, 2018. Am. J. Public Health 2020, 110, 1126–1132. [Google Scholar] [CrossRef]
- HSE. Making Your Workplace COVID-Secure during the Coronavirus Pandemic; Health and Safety Executive: Bootle, UK, 2021. Available online: https://www.hse.gov.uk/coronavirus/working-safely/index.htm (accessed on 25 April 2021).
- Billock, R.M.; Groenewold, M.R.; Free, H.; Haring Sweeney, M.; Luckhaupt, S.E. Required and Voluntary Occupational Use of hazard controls for COVID-19 prevention in non-health care workplaces—United States, June 2020. MMWR Morb. Mortal Wkly. Rep. 2021, 70, 250–253. [Google Scholar] [CrossRef] [PubMed]
- Dennerlein, J.T.; Burke, L.; Sabbath, E.L.; Williams, J.A.R.; Peters, S.E.; Wallace, L.; Karapanos, M.; Sorensen, G. An integrative Total Worker Health framework for keeping workers safe and healthy during the COVID-19 pandemic. Hum. Factors 2020, 62, 689–696. [Google Scholar] [CrossRef] [PubMed]
- Garcia, P.J.; Alarcón, A.; Bayer, A.; Buss, P.; Guerra, G.; Ribeiro, H.; Rojas, K.; Saenz, R.; Salgado de Snyder, N.; Solimano, G.; et al. COVID-19 Response in Latin America. Am. J. Trop. Med. Hyg. 2020, 103, 1765–1772. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Europe | North America | Latin America | ||||||
|---|---|---|---|---|---|---|---|---|
| Country | N. Sites | N. Workers | Country | N. Sites | N. Workers | Country | N. Sites | N. Workers |
| Germany | 6 | 2716 | US | 9 | 2232 | Mexico | 5 | 3337 |
| France | 6 | 2038 | Canada | 1 | 145 | Brazil | 1 | 343 |
| Netherlands | 5 | 1243 | Chile | 1 | 304 | |||
| UK | 6 | 1190 | Colombia | 1 | 194 | |||
| Spain | 3 | 1122 | ||||||
| Russia | 4 | 1107 | ||||||
| Slovakia | 1 | 1024 | ||||||
| Poland | 1 | 870 | ||||||
| Sweden | 3 | 831 | ||||||
| Italy | 4 | 689 | ||||||
| Austria | 1 | 515 | ||||||
| Belgium | 1 | 426 | ||||||
| Finland | 1 | 223 | ||||||
| Turkey | 1 | 97 | ||||||
| Total | 43 | 14,091 | Total | 10 | 2377 | Total | 8 | 4178 |
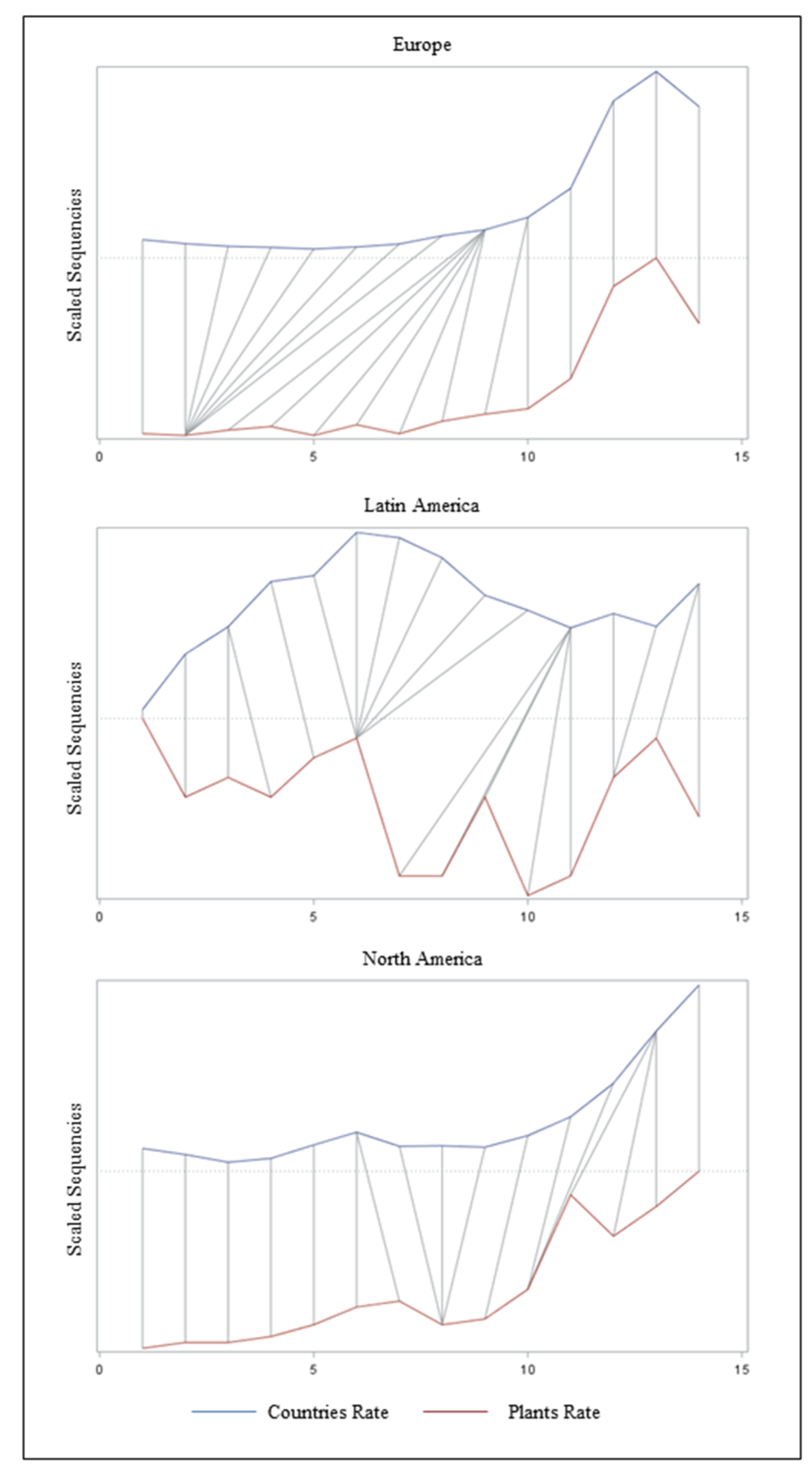
| Geographic Area | Cross-Correlation | Similarity | ||||
|---|---|---|---|---|---|---|
| Lag 0 | Lag 1 | AD | DTW | |||
| r | p | r | p | |||
| Europe | 0.99 | <0.001 | 0.82 | 0.002 | 3.83 | 1.75 |
| North America | 0.88 | 0.001 | 0.07 | 0.008 | 3.36 | 1.45 |
| Latin America | −0.33 | 0.223 | 0.10 | 0.714 | 4.76 | 2.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lovreglio, P.; Stufano, A.; Cagnazzo, F.; Bartolomeo, N.; Iavicoli, I. Application of an Innovative Model for the Risk Management of COVID-19 in a Multinational Manufacturing Company. Sustainability 2021, 13, 5771. https://doi.org/10.3390/su13115771
Lovreglio P, Stufano A, Cagnazzo F, Bartolomeo N, Iavicoli I. Application of an Innovative Model for the Risk Management of COVID-19 in a Multinational Manufacturing Company. Sustainability. 2021; 13(11):5771. https://doi.org/10.3390/su13115771
Chicago/Turabian StyleLovreglio, Piero, Angela Stufano, Francesco Cagnazzo, Nicola Bartolomeo, and Ivo Iavicoli. 2021. "Application of an Innovative Model for the Risk Management of COVID-19 in a Multinational Manufacturing Company" Sustainability 13, no. 11: 5771. https://doi.org/10.3390/su13115771
APA StyleLovreglio, P., Stufano, A., Cagnazzo, F., Bartolomeo, N., & Iavicoli, I. (2021). Application of an Innovative Model for the Risk Management of COVID-19 in a Multinational Manufacturing Company. Sustainability, 13(11), 5771. https://doi.org/10.3390/su13115771