
Measures for Ensuring Sustainability during the Current Spreading of Coronaviruses in the Czech Republic


Abstract
:1. Introduction
- The economic model;
- People and society;
- Resilient ecosystems;
- Municipalities and regions;
- Global development;
- Good governance.
Literature Review
2. Materials and Methods
2.1. Risk Assessment
2.2. Description of Epidemiological Data and Mathematical Models
3. Results and Discussion
- Careful analysis of new risks and heightened existing risks and the proposal of quality countermeasures to mitigate them;
- Construction of mathematical developmental regression models of time series;
- Proposal of a set of measures for individuals to prevent coronavirus infection and stop the further transmission of infection.
3.1. Risk Analysis and Treatment during the Second and Third Waves of Coronavirus
- Failure of the overall population protection system;
- Immediate threat to the life of the affected population;
- Endangering the lives of livestock and domestic animals;
- Production losses of manufacturing and processing companies;
- Reduction in income from tourism;
- Limitations of healthcare for the infected and otherwise disabled population;
- Spreading pandemic outbreaks as a result of their stochastic spread;
- Restrictions on the operation of transport networks;
- Disruption in supplying the population with water, food, medicines and disinfectants;
- Disturbance of public order;
- Restrictions on international trade;
- Intensification of sabotage activities;
- Deliberate spread of the epidemic;
- Increase in migration as a result of the population moving to localities with a lower infection rate, a smaller number of people with newly diagnosed disease and, thereby, a risk of mortality;
- Panic;
- Social impacts on producers, the public administration and families; and
- Social impacts on healthcare staff due to the increased risk of infection and psychological burden.
- The production losses of manufacturing and processing companies which can lead to serious effects at the macroeconomic level in the event of a large-scale pandemic;
- Immediate threat to the life of the affected population;
- Social impacts on healthcare staff due to the increased risk of infection and psychological burden;
- Limitations in healthcare for the infected and otherwise disabled population.
- Strict adherence to the restrictive measures introduced by the government, provided that these measures have been designed on the basis of careful risk analysis and assessment of the current situation in relation to the occurrence and transmission of the pandemic;
- The prompt introduction of nationwide immunization of the population;
- Implementation of rapid orientation detection and identification of outbreaks in regions and companies with a large number of employees by means of periodic testing and consistent tracing;
- Implementation of effective clinical diagnoses and therapies in patients infected with coronavirus;
- Ensuring and performing efficient tracing;
- Clearly identifying outbreaks of infection and clarifying the routes of its transmission;
- Evacuating healthy people from outbreaks of infection;
- Preventing the import of the disease and conducting thorough border-crossing control in both directions and areas with coronavirus outbreaks;
- Restricting travel of the population to foreign countries;
- Applying effective quarantine, isolation and treatment of suspected patients;
- Financially motivating people to adhere strictly to isolation (domestic quarantine), because many identified and potentially infected people often refuse quarantine for economic reasons (the employer mostly pays only 60% of their full salary and this literally means an existential risk for some families);
- Ensuring the decontamination of people, the disinfection of objects and the environment and the minimization of the transmission of infection, especially at workplaces and on public transport;
- Ensuring the availability of medicines, vaccines, means of prophylaxis and vaccination not only for the affected population, but also for the healthy population;
- Strengthening immunity and reducing the population’s perception of infection by means of information campaigns focused on the principles of hygiene, healthy eating, lifestyle, sleep, etc.;
- Minimizing physiological and emotional stressors suppressing the immune system of the population;
- Preventing the misuse of the situation by individuals and social groups with an interest in increasing panic, misinforming the population and spreading fake news;
- Ensure that the general public is informed in a timely and adequate manner of the course and consequences of the pandemic and the corrective measures taken to mitigate the associated risks;
- Rationally implementing restrictions on the production of selected companies and the operation of public services, kindergartens and proximate teaching at primary and secondary schools, vocational schools and tertiary education institutions;
- Specify the timing of walks, zones and the possibility of purchasing selected goods, medicines, etc., for different groups and age categories of the population;
- Reinforcing the level of education and training of specialists in the field of detection, diagnosis and treatment of infectious diseases with an emphasis on the coronavirus;
- Preventing the uncontrolled escape of infection from laboratory, biotechnological and other facilities where coronavirus is handled;
- Intensively developing cooperation with concerned institutions in this country and abroad;
- Implementing appropriate building engineering controls, including sufficient and effective ventilation, possibly enhanced by particle filtration and air disinfection, avoiding air recirculation and avoiding overcrowding. Such measures can easily be implemented without much cost, but only if they are recognized as significant in contributing to infection control goals. The use of engineering controls in public buildings, including hospitals, shops, offices, schools, kindergartens, libraries, restaurants, cruise ships, elevators, conference rooms and public transport, in parallel with effective application of other controls, including isolation and quarantine, social distancing and hand hygiene, is an important measure globally in reducing the likelihood of transmission and thereby in protecting healthcare workers, patients and the general public [41].
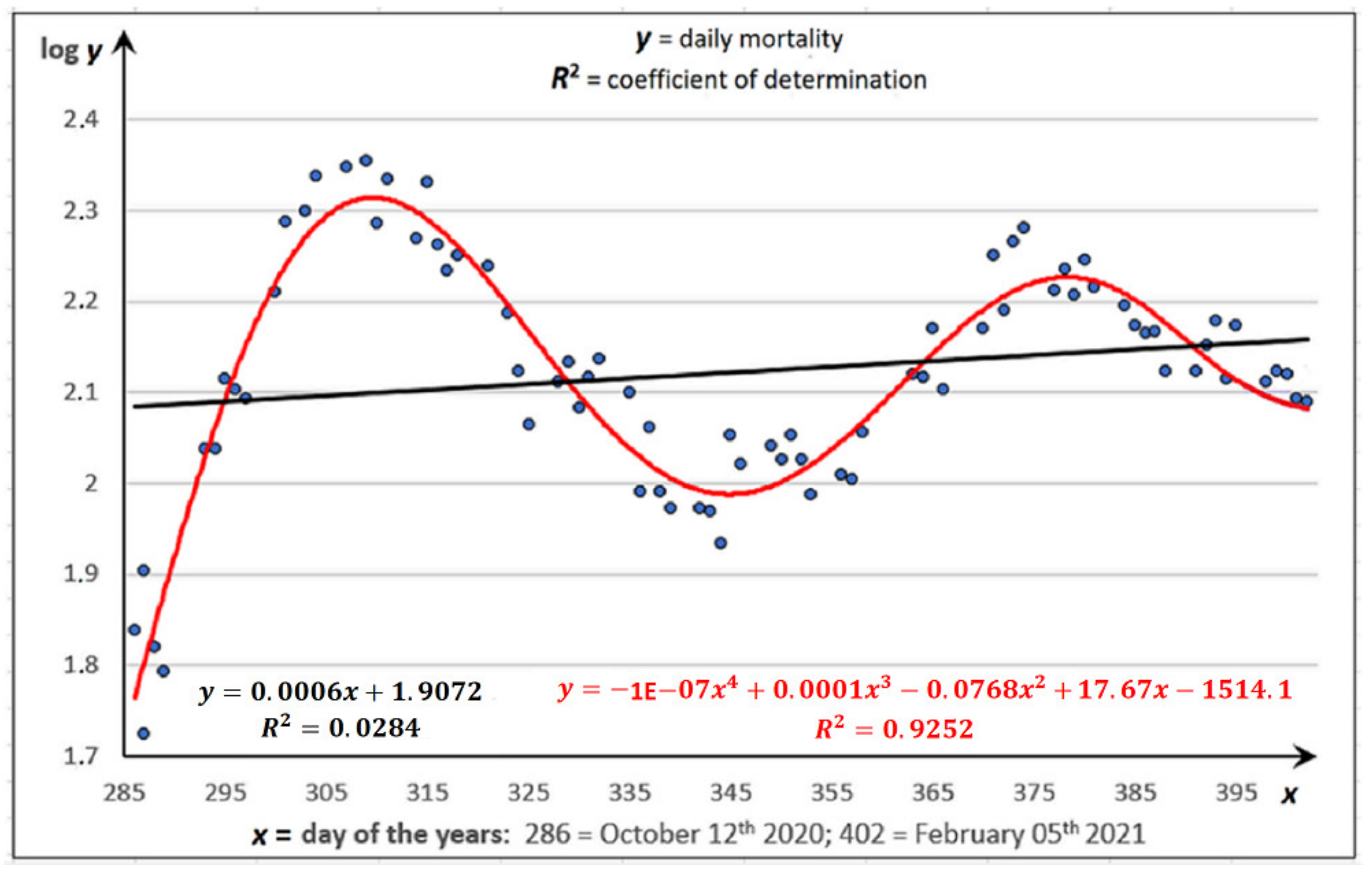
3.2. Developmental Regression Models in the Second and Third Waves of the Coronavirus
- The maxima of occurrence and transmission of coronavirus in the second and third wave occurred at the end of the third decade of October 2020 or the first decade of January 2021;
- The onset of the third wave of coronavirus rate and transmission occurred in the Czech Republic at the turn of October and November last year.
3.3. Prevention of Coronavirus Infection
- It is necessary to avoid becoming stressed, because emotional stress reduces the natural immunity of the organism. There is no need to make your life difficult. Learn to live with the reality of the existence of SARS-CoV-2.
- It is advisable to ensure that the mucous membranes of the oral cavity and throat are always moist and never dry. This can be done by drinking a few sips of water or other fluids every 15 min or so, because once the virus enters the mouth fluids flush it into the stomach where gastric HCl that destroys the coronavirus is present.
- Drinking hot fluids is effective for all viruses of this species. In contrast, consumption of only a minimal amount results in the virus entering the upper respiratory tract and, in the final stage, the alveoli, where it penetrates the semi-permeable membrane to the cell nucleus. This is typical of this type of virus.
- Drinking cold drinks, especially drinks with ice, is inappropriate as the coronavirus survives longer in a cold environment. It is necessary to realize that a decrease in temperature of 1 °C leads to an increase in the basic reproduction number R of about 3% in an environment of around 20 °C and less.
- If the infection occurs in your household, it is advisable to disinfect the surfaces of objects of frequent contact and to wash hands with warm water, sporadically with good quality soap. The frequent treatment of hands with disinfectants is not beneficial, because disinfectants are oxidants decomposing the keratin and collagen proteins that are part of the skin and the layer beneath it.
- It is not necessary to change clothes and to shower as a matter of urgency when returning from the outside environment. Adherence to hygiene and cleanliness is a virtue, but paranoia is not.
- At body temperatures below 38 °C, it is beneficial to avoid the use of medicines to reduce temperature. Fever is a symptom of the coronavirus infection and also of other diseases, though the body’s natural immune response to the presence of any other virus becomes inactive at higher temperatures. Only when the body temperature exceeds 38 °C and difficulty in breathing worsens is it necessary to use medications and physical methods of treatment (cold wraps on the inside of the thighs and arms, the groin or the front of the neck) to reduce the body temperature and to call a doctor immediately.
- It is recommended not to rub your eyes with the hands and not to touch your nose or mouth unintentionally. Although it may seem unbelievable, a person touches his/her face up to 2–3 × 103 times a day.
- Gargling two to three times a day with a warm solution at 45–55 °C prepared from approximately 50 mL of water and one to two grains of KMnO4 or a pinch of table salt provides effective prevention. NaCl solution is, however, less effective.
- From the viewpoint of possible infection, it is not appropriate to touch your mask without hand protection when returning home from the outside environment, as your mask may be contaminated with a virus that has adhered to it. Disposable masks should be discarded immediately.
- Wearing microtone gloves, usually made of high-density polyethylene, to protect the hands is not ideal as they are microporous. The virus accumulates during prolonged use on and inside the glove, especially in an environment with wet sweaty hands, and is easily transmitted by, for example, touching your mouth with your hand.
- When coming into contact with other people, it is optimal to protect the respiratory tract with a respirator made of nanofibers.
- It is recommended that cotton masks are treated with salt by soaking in a solution of NaCl of around 10% by weight and subsequently drying out. This protection works on the basis of osmosis, with freshwater cells, including bacteria, moulds, fungi, viruses and Rickettsiae, trying to dilute the salty environment with their own water and thereby drying themselves out. The salty cotton mask catches and kills the virus. It also works the other way around, when the virus comes from the wearer’s own breath, ensuring the protection of not just the wearer, but also the wearer’s surroundings. The salinity of the mask is so low that it does not cause allergies in users, but is sufficiently effective against the transmission of viruses. If the wearer inhales NaCl microcrystals from the mask, this is only beneficial to his/her respiratory tract, because NaCl effectively cleanses airways. This effect is also used when patients with respiratory problems visit salt caves. Salting is not possible in the case of disposable masks, which are usually made of synthetic fibres whose surface does not capture NaCl due to their hydrophobic nature.
- It is expedient to use masks minimally and exclusively in an environment in which the wearer comes into contact with other people. When a (nano)-mask (respirator) is worn, the exhaled CO2 is inhaled, which reduces the level of O2 in the blood. This causes physiological stress during which the body suffers from hypoxia and is in a sympathomimetic state resulting in increased levels of the hormone cortisol. Cortisol suppresses the immune system as it reduces the number of lymphocytes in the bloodstream and the body becomes more susceptible to any pathogen, e.g., bacteria, viruses or Rickettsiae. Moreover, disposable masks are usually made of synthetic fibres, mostly polypropylene, polyethylene or their copolymers, containing additives that are released, decomposed and cause further weakening of the immunity in a humid breathing environment.
- It would seem expedient for the elderly to use a mask (respirator) in contact with other people and to avoid shaking hands. Young people do not have to worry too much about shaking hands and the possible absence of a mask in a group of their peers, as they increase their own immunity in this way.
- If someone sneezes, the trajectory of the aerosol droplets in the open is less than 3 m before hitting the ground. It is therefore important to maintain an adequate distance, around 2–3 m, from the other people and to remember that the aerosol hovers in the air for a substantially shorter time with increasing humidity. This is why the relative humidity inside enclosed rooms should be higher than 40%. If a humidifier is not available in the household, it is rational to keep the temperature lower and not to overheat the room, so that the relative humidity is as high as possible.
- Vitamins D, E (6000 IU) and ascorbic acid (vitamin C) and zinc tablets may also be used to prevent SARS-CoV-2 infections.
- Although the coronavirus is unlikely to be transmitted by food, it is advisable to process meat and food containing eggs at higher temperatures.
- Consumption of foods and beverages rich in essential elements and vitamins, for example juice from sugar cane, apple cider vinegar and, in particular, ginger in combination with cinnamon and mineral waters, strengthens the immune system. (If you like, approximately 50 mL of hard liquor per day, although this does not directly protect the human body from the coronavirus infection, it strengthens the immune system). On the other hand, the consumption of fried, spicy and sweet foods, sweetened soft drinks, etc., suppresses the immunity of the organism.
- The hormone melatonin, which maintains a strong circadian rhythm and regulates immune processes in the body, is considered an effective immunomodulator. Melatonin is produced by the pineal gland, but only at night and in the dark, so it is necessary to maintain both these conditions at the same time for its synthesis.
- The human immune organism is also stimulated by regular sport, walks in nature, in the park and especially in pine forests, which are an ideal environment for breathing.
4. Conclusions
- The application of the “Fault Tree Analysis” or “Event Tree Analysis” methods to quantify, in particular, the critical risks associated with the occurrence and spread of coronaviruses and to further specify, on this basis, a set of measures to mitigate the associated risks;
- Paying particular attention to the transmission of coronaviruses adsorbed on aluminium silicate and carbon particles less than or equal to 2.5 (μm) in connection with this article;
- The application of the SIR epidemiological model and comparison of the results with our findings using a model of regression analysis of time series; and
- The supplementation of measures for personal prevention of human coronavirus infection through discussions within the work team and contacts with experts at home and abroad.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hatem, F. Le Concept de Développement Durable: Origines Récentes, une Notion Ambiguë Promettant des Applications Paris; Ministère de l’Environnement, Commisariat du Plan: Quebec City, QC, Canada, 1991. [Google Scholar]
- Commission on Environment and Development (CED). Report of the World Commission on Environment and Development: Our Common Future; Oxford University Press: London, UK, 1987. [Google Scholar]
- Zhai, T.T.; Chang, Y.C. Standing of environmental public-interest litigants in China: Evolution, obstacles and solutions. J. Environ. Law 2018, 30, 369–397. [Google Scholar] [CrossRef]
- Ministry of the Environment of the Czech Republic. Strategic Framework for Sustainable Development of the Czech Republic; Ministry of the Environment: Prague, Czech Republic, 2010. Available online: https://www.mzp.cz/en/czech_republic_strategy_sd (accessed on 24 April 2021).
- Basiago, A.D. Economic, social, and environmental sustainability in development theory and urban planning practice. Environmentalist 1998, 19, 145–161. [Google Scholar] [CrossRef]
- United Nations, Department of Economic and Social Affairs. Transforming Our World: The 2030 Agenda for Sustainable Development. 2015. Available online: https://sustainabledevelopment.un.org/post2015/transformingourworld (accessed on 24 April 2021).
- European Commission. Towards a Sustainable Europe by 2030. Available online: https://ec.europa.eu/info/publications/towards-sustainable-europe-2030_en (accessed on 24 April 2021).
- Office of the Government of the Czech Republic, Department for Sustainable Development. Strategic Framework of the Czech Republic 2030; Office of the Government of the Czech Republic: Prague, Czech Republic, 2017. Available online: https://www.vlada.cz/assets/ppov/udrzitelny-rozvoj/projekt-OPZ/Strategic_Framework_CZ2030.pdf (accessed on 29 March 2021).
- Bozek, F. Epidemics, Risk Assessment and Treatment with an Emphasis on Coronavirus; Ambis College: Prague, Czech Republic, 2020; pp. 21–25. [Google Scholar]
- Tušer, I.; Hoskova-Mayerova, Š. Emergency Management in Resolving an Emergency Situation. J. Risk Financ. Manag. 2020, 13, 262. [Google Scholar] [CrossRef]
- Tušer, I.; Hošková-Mayerová, Š. Traffic safety sustainability and population protection in road tunnels. Qual. Quant. 2020. [Google Scholar] [CrossRef]
- Nerini, F.F.; Henrysson, M.; Swain, A.; Swain, B.R. Sustainable Development in the Wake of Covid-19. Res. Square 2021. [Google Scholar] [CrossRef]
- The National Institute of Public Health. Disease by COVID-19 and the New Coronavirus SARS-CoV-2. 2021. Available online: http://www.szu.cz/index.php?lang=2 (accessed on 24 February 2021).
- Trojanek, M.; Grebenyuk, V.; Herrmannová, K.; Nečas, T.; Gregorová, J.; Kucbel, M.; Šín, R.; Roháčová, H.; Stejskal, F. Nový koronavirus (SARS-CoV-2) a onemocnění COVID-19. Časopis Lékařů Českých 2020, 159, 55–66. (In Czech) [Google Scholar] [PubMed]
- Popovic, L. Coronavirus and Its Mutations: What Makes “British” Worse Than the Previous Ones and What Do We Know Next? 2021. Available online: https://www.novinky.cz/koronavirus/clanek/koronavirus-a-jeho-mutace-v-cem-je-britska-horsi-nez-ty-predchozi-a-jake-dalsi-zname-40348273 (accessed on 24 February 2021).
- Conti, P.; Caraffa, A.; Gallenga, C.E.; Kritas, S.K.; Frydas, I.; Younes, A.; Di Emidio, P.; Tetè, G.; Pregliasco, F.; Ronconi, G. The British variant of the new coronavirus-19 (Sars-Cov-2) should not create a vaccine problem. J. Biol. Regul. Homeost. Agents 2021, 35, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Max, R.; Ritchie, H.; Ortiz-Ospina, E.; Hasell, J. Coronavirus Pandemic (COVID-19). 2020. Available online: https://ourworldindata.org/coronavirus (accessed on 24 February 2021).
- WHO Coronavirus Disease (COVID-19). Available online: https://covid19.who.int/ (accessed on 24 February 2021).
- ECDC—European Centre for Disease Prevention and Control. Available online: https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases (accessed on 24 February 2021).
- Anastassopoulou, C.; Russo, L.; Tsakris, A.; Siettos, C. Data-based analysis, modelling and forecasting of the.COVID-19 outbreak. PLoS ONE 2020, 15, e0230405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roosa, K.; Lee, Y.; Luo, R.; Kirpich, A.; Rothenberg, R.; Hyman, J.; Yan, P.; Chowell, G. Real-time forecasts of the COVID-19 epidemic in China from February 5th to February 24th, 2020. Infect. Dis. Model. 2020, 5, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Fanelli, D.; Piazza, F. Analysis and forecast of COVID-19 spreading in China, Italy and France. Chaos Solitons Fractals 2020, 134, 109761. [Google Scholar] [CrossRef] [PubMed]
- Hasan, A.; Putri, E.R.M.; Susanto, H.; Nuraini, N. Data-driven modeling and forecasting of COVID-19 outbreak for public policy making. ISA Trans. 2021. [Google Scholar] [CrossRef] [PubMed]
- Postavaru, O.; Anton, S.R.; Toma, A. COVID-19 pandemic and chaos theory. Math. Comput. Simul. 2021, 181, 38–149. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, I.; Hasan, M.; Akter, R.; Sarkar, B.K.; Rahman, M.; Sarker, M.S.; Samad, M.A. Behavioral preventive measures and the use of medicines and herbal products among the public in response to Covid-19 in Bangladesh: A cross-sectional study. PLoS ONE 2020, 15, e0243706. [Google Scholar] [CrossRef] [PubMed]
- Fikadu, Y.; Yeshaneh, A.; Melis, T.; Mesele, M.; Anmut, W.; Argaw, M. COVID-19 Preventive Measure Practices and Knowledge of Pregnant Women in Guraghe Zone Hospitals. Int. J. Womens Health 2021, 7, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Fong, D.; San Nicolò, K.O.; Alber, M.; Mitterer, M. Evaluating the longitudinal effectiveness of preventive measures against COVID-19 and seroprevalence of IgG antibodies to SARS-CoV-2 in cancer outpatients and healthcare workers. Wiener Klinische Wochenschrift 2021, 27, 1–5. [Google Scholar]
- Sutton, I. Process Risk and Reliability Management: Operational Integrity Management, 1st ed.; Oxford Elsevier Inc.: Amsterdam, The Netherlands, 2010; pp. 143–152. [Google Scholar]
- Dickert, T.G. Methods for Environmental Impact Assessment: Guidelines and Commentary, 1st ed.; University of California: Berkeley, CA, USA, 1974; pp. 79–88. [Google Scholar]
- Krenek, R.; Department of Infectious Diseases, University Hospital Brno-Bohunice, Brno, Czech Republic. Personal communication, 2021.
- Navratil, L.; Faculty of Biomedical Engineering Czech Technical University in Prague, Kladno, Czech Republic. Personal communication, 2021.
- Komar, A.; Faculty of Military Health Sciences, University of Defence, Brno, Czech Republic. Personal communication, 2021.
- Kudlák, A.; Urban, R.; Hoskova-Mayerova, S. Determination of the Financial Minimum in a Municipal Budget to Deal with Crisis Situations. Soft Comput. 2020, 24, 8607–8616. [Google Scholar] [CrossRef]
- Bozek, A.; Stahl und Anlagenbau GmbH, Hinterhermsdorf, Germany. Personal communication, 2021.
- Koudelka, C.; Vrána, V. Rizika a Jejich Analýza, 1st ed.; VSB Technical University of Ostrava: Ostrava, Czech Republic, 2006; pp. 9–11. Available online: http://fei1.vsb.cz/kat420/vyuka/Magisterske%20nav/prednasky/web/RIZIKA.pdf (accessed on 24 February 2021). (In Czech)
- Majumdar, S.N.; Pal, A.; Schehr, G. Extreme value statistics of correlated random variables: A pedagogical review. Phys. Rep. 2020, 840, 1–32. [Google Scholar] [CrossRef] [Green Version]
- Meloun, M.; Militký, J. Statistická analýza experimentálních dat (in Czech), 2nd ed; Academia: Prague, Czech Republic, 2004; p. 953. [Google Scholar]
- Weathington, B.L.; Cunningham, C.J.L.; Pittenger, D.J. Understanding Business Research, 1st ed.; John Wiley & Sons: Hoboken, NJ, USA, 2012; pp. 265–266. [Google Scholar]
- Bakare, E.A.; Hoskova-Mayerova, S. Optimal Control Analysis of Cholera Dynamics in the Presence of Asymptotic Transmission. Axioms 2021, 10, 60. [Google Scholar] [CrossRef]
- Bekesiene, S.; Hošková-Mayerová, Š. Automatic Model Building for Binary Logistic Regression by Using SPSS 20 Software. In Proceedings of the 18th Conference on Applied Mathematics APLIMAT 2019 Proceedings (SPEKTRUM STU), Bratislava, Slovakia, 5–7 February 2019; pp. 31–40, ISBN 978-80-227-4884-1. [Google Scholar]
- Morawska, L.; Tang, W.J.; Bahnfleth, W.; Bluyssen, M.P.; Boerstra, A.; Buonanno, G.; Cao, J.; Dancer, S.; Floto, A.; Franchimon, F.; et al. How can airborne transmission of COVID-19 indoors be minimised? Environ. Int. 2020, 142, 105832. [Google Scholar] [CrossRef] [PubMed]
- Ministry of the Interior of the Czech Republic; NAKIT; National Agency for Communication and Information Technologies. Development in the Czech Republic and in Other Countries. 2021. Available online: https://nakit.cz/koronadata (accessed on 24 February 2021).
- Ministry of Health of the Czech Republic. Covid-19: Overview of the Current Situation in the Czech Republic. 2021. Available online: https://onemocneni-aktualne.mzcr.cz/covid-19 (accessed on 24 February 2021).
- Razali, N.; Wah, Y. Power Comparisons of Shapiro-Wilk, Kolmogorov-Smirnov, Lilliefors and Anderson-Darling tests. J. Stat. Modeling Anal. 2011, 2, 21–33. [Google Scholar]
- Henry, B.; Faculty of Medicine, School of Population and Public Health, The University of British Columbia, Vancouver, BC, Canada. Personal communication, 2020.
- Flegr, J. They Swept Everything under the Rug, Life Stops, It Didn’t Have to Happen at All, Says Flegr; Charles University, The Faculty of Natural Science: Prague, Czech Republic, 2020; Available online: https://video.aktualne.cz/dvtv/vse-zametali-pod-koberec-zivot-se-zastavi-vubec-se-to.nemuse/r~a857cc2e13d711eba7deac1f6b220ee8/ (accessed on 29 March 2021).
- Flegr, J. The Third Wave Will Come before Christmas. The Virus Will Be Much More Aggressive, It’s Too Late for the Veils, Flegr Warns; Charles University, The Faculty of Natural Science: Prague, Czech Republic, 2020; Available online: https://www.televizeseznam.cz/video/face-to-face/treti-vlna-prijde-uz-pred-vanocemi-virus-bude-.mnohem-agresivnejsi-na-rousky-je-pozde-varuje-flegr-64106362 (accessed on 29 March 2021).
- Hardell, L.; University Hospital, Örebro, Sweden. Personal communication, 2020.
- Omelchenko, A.; St. Boniface General Hospital Research Centre, Winnipeg, MB, Canada. Personal communication, 2021.
- Subhas, K.S.; National Risk Management Laboratory, US Environmental Protection Agency, Cincinnati, OH, USA. Personal communication, 2021.
- Ždímal, V. Institute of Chemical Process Fundamentals of the CAS. It’ll Only Survive for Minutes. The Scientist Describes What Happens to the Virus in Warmer Weather. 2020. Available online: https://zpravy.aktualne.cz/domaci/zivot-v-pandemii-vladimir-zdimal-z-ustavu-chemickych-procesu/r~cbc8c13c67a511eb95caac1f6b220ee8/ (accessed on 29 March 2021).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indication of Risk | Name of Hazard | P | N | H | R | Level of Risk | Priority |
|---|---|---|---|---|---|---|---|
| Ra | Failure of the overall system of protection of the population | 1 | 5 | 5 | 25 | marginal | 14 |
| RbE | Endangering the lives of the affected population | 3.5 | 5 | 5 | 89 | tolerable | 2 |
| Rc | Endangering the lives of livestock and domestic animals | 1.5 | 2 | 2 | 6 | acceptable | 17 |
| Rd | Production losses of production and processing companies | 4 | 5 | 4.5 | 90 | tolerable | 1 |
| Re | Reduction of income from tourism | 4 | 3.5 | 3 | 42 | low | 11 |
| Rf | Restrictions on healthcare for the infected and otherwise disabled population | 4 | 4.5 | 4.5 | 81 | acceptable | 3 |
| Rg | Increasing the number of pandemic outbreaks due to its stochastic spread | 3.5 | 4.5 | 3.5 | 55 | medium | 8 |
| Rh | Restrictions on the operation of transport networks | 4 | 3.5 | 3.5 | 49 | medium | 9 |
| Ri | Disruption of the population’s supply of water, food, medicine and disinfectants | 3.5 | 3.5 | 5 | 61 | high | 7 |
| Rj | Disturbance of public order | 2 | 3 | 3.5 | 21 | marginal | 15 |
| Rk | restrictions on international trade | 3 | 3.5 | 4.5 | 47 | medium | 10 |
| Rl | Intensification of sabotage activities | 1.5 | 2.5 | 3 | 11 | acceptable | 16 |
| Rm | Deliberate spread of the epidemic | 2 | 4 | 4.5 | 36 | low | 12 |
| Rn | Increase in migration | 3.5 | 5 | 4 | 70 | high | 6 |
| Ro | Panic | 1.5 | 4 | 5 | 30 | low | 13 |
| Rp | Social impacts on producers, public administrations and families | 4 | 4.5 | 4 | 72 | high | 5 |
| Rq | Social impacts on health workers of increased risk of infection and psychological burden | 4 | 4 | 5 | 80 | acceptable | 4 |
| Degree of Risk | Point Risk Interval | Level of Risk |
|---|---|---|
| I | ≥95 | unacceptable |
| II | 〈85; 95) | tolerable but undesirable (a) |
| III | 〈75; 85) | acceptable (b) |
| IV | 〈60; 75) | high (c) |
| V | 〈45; 60) | medium (d) |
| VI | 〈30; 45) | low (e) |
| VII | 〈15; 30) | marginal |
| VIII | 〈1; 15) | negligible |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Božek, F.; Tušer, I. Measures for Ensuring Sustainability during the Current Spreading of Coronaviruses in the Czech Republic. Sustainability 2021, 13, 6764. https://doi.org/10.3390/su13126764
Božek F, Tušer I. Measures for Ensuring Sustainability during the Current Spreading of Coronaviruses in the Czech Republic. Sustainability. 2021; 13(12):6764. https://doi.org/10.3390/su13126764
Chicago/Turabian StyleBožek, František, and Irena Tušer. 2021. "Measures for Ensuring Sustainability during the Current Spreading of Coronaviruses in the Czech Republic" Sustainability 13, no. 12: 6764. https://doi.org/10.3390/su13126764
APA StyleBožek, F., & Tušer, I. (2021). Measures for Ensuring Sustainability during the Current Spreading of Coronaviruses in the Czech Republic. Sustainability, 13(12), 6764. https://doi.org/10.3390/su13126764