
Dementia and COVID-19 in Chile, New Zealand and Germany: A Research Agenda for Cross-Country Learning for Resilience in Health Care Systems

 , , , , ,
, , , , ,  , ,
, , 
Abstract
:1. Introducing a Hypothesis for Translational Learning of Health Systems in Response to the COVID-19 Pandemic
2. Developing an Agenda for Cross-Country Learning for Resilience in Health Systems in Response to the COVID-19 Pandemic
2.1. Resilience of Health Care Systems
2.2. Sustainability of Learning Health Care Systems
2.3. Inequity in Dementia Care before and during the COVID-19 Pandemic
2.4. Overview of the Three Chosen Countries: Chile, New Zealand and Germany
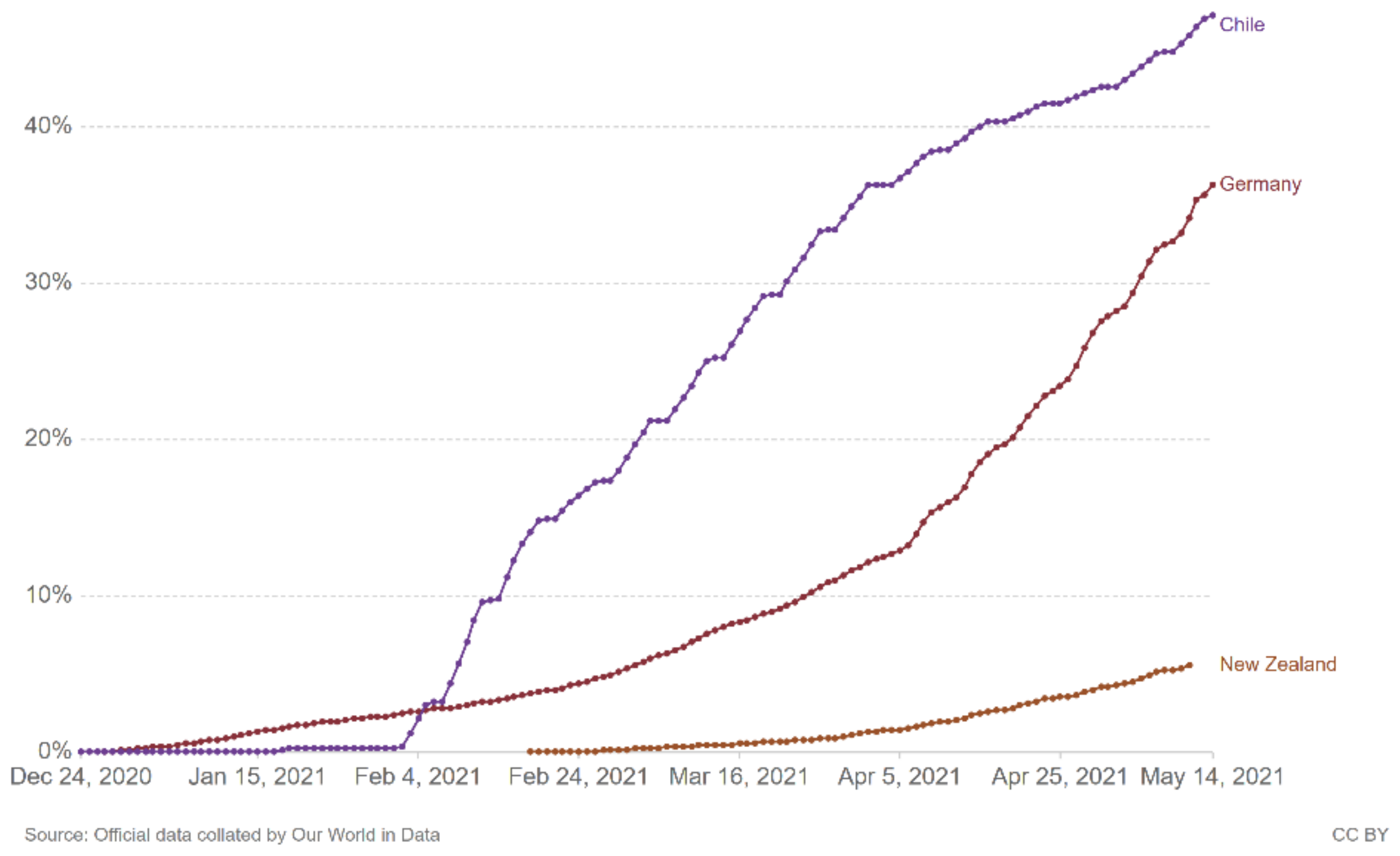
2.5. Contextual Background of the COVID-19 Pandemic in Chile, New Zealand and Germany
2.6. Contextual Background of Dementia in Chile, New Zealand and Germany
2.6.1. Chile
- (a)
- Dementia prevalence and incidence
- (b)
- Dementia strategy
- (c)
- Current developments in research
- (d)
- Reactions to the COVID-19 pandemic
2.6.2. New Zealand
- (a)
- Dementia prevalence and incidence
- (b)
- Dementia strategy
- (c)
- Current developments in research
- (d)
- Reactions to the COVID-19 pandemic
2.6.3. Germany
- (a)
- Dementia prevalence and incidence
- (b)
- Dementia strategy
- (c)
- Current developments in research
- (d)
- Reactions to the COVID-19 pandemic
2.7. Research Objectives and Research Questions
- How have three selected nations (Chile, New Zealand, Germany) responded to the needs of people living with dementia and of their families prior to and during the COVID-19 pandemic?
- How does living in countries with continuous natural hazards and risks impact on building resilience and enabling responses to rapid (respiratory) pandemics such as the COVID-19 pandemic, on the one hand, and to long-term challenges such as dementia, on the other hand? How might this differ in countries with (currently) fewer natural hazards and risks?
- What can we learn from those global experiences to empower health care systems to provide adequate, equitable and sustainable care and support for families living with dementia during times of pandemics and beyond?
3. Methodical and Methodological Considerations
4. Arguments in Support of Our Vision and Agenda
4.1. The Need for a Complex Approach
4.2. Insights and Lessons to Be Learnt from a Trilateral Country Comparison between Chile, New Zealand and Germany
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The Independent Panel for Pandemic Preparedness and Response. COVID-19: Make It the Last Pandemic. Available online: https://theindependentpanel.org/wp-content/uploads/2021/05/COVID-19-Make-it-the-Last-Pandemic_final.pdf (accessed on 25 May 2021).
- World Health Organization. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 8 July 2021).
- World Health Organization. Decade of Healthy Ageing 2020–2030. What Is the Decade of Healthy Ageing? Available online: https://www.who.int/ageing/decade-of-healthy-ageing (accessed on 25 January 2021).
- Alzheimer’s Disease International. From Plan to Impact Report IV. Available online: https://www.alzint.org/resource/from-plan-to-impact-iv/ (accessed on 26 May 2021).
- World Health Organization. COVID-19. In Proceedings of the Virtual Press Conference, Geneva, Switzerland, 21 June 2021. [Google Scholar]
- Greenhalgh, T.; Knight, M.; A’Court, C.; Buxton, M.; Husain, L. Management of post-acute COVID-19 in primary care. BMJ 2020, 370, m3026. [Google Scholar] [CrossRef] [PubMed]
- Meinhardt, J.; Radke, J.; Dittmayer, C.; Franz, J.; Thomas, C.; Mothes, R.; Laue, M.; Schneider, J.; Brünink, S.; Greuel, S.; et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat. Neurosci. 2021, 24, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Heneka, M.T.; Golenbock, D.; Latz, E.; Morgan, D.; Brown, R. Immediate and long-term consequences of COVID-19 infections for the development of neurological disease. Alzheimer’s Res. Ther. 2020, 12, 69. [Google Scholar] [CrossRef]
- Cheung, G.; Rivera-Rodriguez, C.; Martinez-Ruiz, A.; Ma’u, E.; Ryan, B.; Burholt, V.; Bissielo, A.; Meehan, B. Impact of COVID-19 on the health and psychosocial status of vulnerable older adults: Study protocol for an observational study. BMC Public Health 2020, 20, 1814. [Google Scholar] [CrossRef] [PubMed]
- Davies, N.; Frost, R.; Bussey, J.; Hartmann-Boyce, J.; Park, S. Maximising mobility in older people when isolated with COVID-19. Cent. Evid.-Based Med. 2020, in press. [Google Scholar]
- Azevedo, L.; Calandri, I.L.; Slachevsky, A.; Graviotto, H.G.; Vieira, M.C.S.; Andrade, C.B.; Rossetti, A.P.; Generoso, A.B.; Carmona, K.C.; Pinto, L.A.C.; et al. Impact of social isolation on people with dementia and their family caregivers. J. Alzheimer’s Dis. 2021, 81, 607–617. [Google Scholar] [CrossRef]
- Meppiel, E.; Peiffer-Smadja, N.; Maury, A.; Bekri, I.; Delorme, C.; Desestret, V.; Gorza, L.; Hautecloque-Raysz, G.; Landre, S.; Lannuzel, A. Neurologic manifestations associated with COVID-19: A multicentre registry. Clin. Microbiol. Infect. 2021, 27, 458–466. [Google Scholar] [CrossRef]
- Babulal, G.M.; Torres, V.L.; Acosta, D.; Agüero, C.; Aguilar-Navarro, S.; Amariglio, R.; Ussui, J.A.; Baena, A.; Bocanegra, Y.; Brucki, S.M.D.; et al. The impact of COVID-19 on the well-being and cognition of older adults living in the United States and Latin America. EClin. Med. 2021, 35, 100848. [Google Scholar] [CrossRef]
- World Health Organization; Greenblat, C. Factsheet on Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia#:~:text=Rates%20of%20dementia,is%20between%205%2D8%25 (accessed on 9 September 2020).
- Gaugler, J.E.; Bain, L.J.; Mitchell, L.; Finlay, J.; Fazio, S.; Jutkowitz, E.; Banerjee, S.; Butrum, K.; Fazio, S.; Gaugler, J.; et al. Reconsidering frameworks of Alzheimer’s dementia when assessing psychosocial outcomes. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2019, 5, 388–397. [Google Scholar] [CrossRef]
- Gowan, M.E.; Kirk, R.C.; Sloan, J.A. Building resiliency: A cross-sectional study examining relationships among health-related quality of life, well-being, and disaster preparedness. Health Qual. Life Outcomes 2014, 12, 85. [Google Scholar] [CrossRef] [Green Version]
- Huber, M.; Knottnerus, J.A.; Green, L.; van der Horst, H.; Jadad, A.R.; Kromhout, D.; Leonard, B.; Lorig, K.; Loureiro, M.I.; van der Meer, J.W.; et al. How should we define health? BMJ 2011, 343, d4163. [Google Scholar] [CrossRef] [Green Version]
- Vernooij-Dassen, M.; Moniz-Cook, E.; Verhey, F.; Chattat, R.; Woods, B.; Meiland, F.; Franco, M.; Holmerova, I.; Orrell, M.; de Vugt, M. Bridging the divide between biomedical and psychosocial approaches in dementia research: The 2019 INTERDEM manifesto. Aging Ment. Health 2021, 25, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Haldane, V.; Ong, S.-E.; Chuah, F.L.-H.; Legido-Quigley, H. Health systems resilience: Meaningful construct or catchphrase? Lancet 2017, 389, 1513. [Google Scholar] [CrossRef]
- Group of Chief Scientific Advisors to the European Commission; European Group on Ethics in Science and New Technologies (EGE). Special advisor to President Ursula von der Leyen on the response to the coronavirus and COVID-19. In Improving Pandemic Preparedness and Management: Lessons Learnt and Ways Forward: Joint Opinion; European Commission: Brussels, Belgium, 2020. [Google Scholar]
- Chadwiek, C.; Zhang, W.; Huvos, A.; Briand, S.; Moen, A. WHO’s Influenza Strategy: Prevention, Control, and Preparedness. 2020. Available online: https://www.openaccessgovernment.org/whos-influenza-strategy/87166/ (accessed on 3 August 2020).
- European Commission. Draft Proposal for a European Partnership under Horizon Europe: Transforming Health and Care Systems. Version 9. June 2020. Available online: https://ec.europa.eu/info/sites/info/files/research_and_innovation/funding/documents/ec_rtd_he-partnerships-health-system-transform.pdf (accessed on 27 May 2021).
- Intergovernmental Science-Policy Platform on Biodiversity and Ecosystem Services (IPBES). IPBES Workshop on Biodiversity and Pandemics. Executive Summary; IPBES Secretariat: Bonn, Germany; UN Campus: Bonn, Germany, 2020. [Google Scholar]
- Gössling, S.; Scott, D.; Hall, C.M. Pandemics, tourism and global change: A rapid assessment of COVID-19. J. Sustain. Tour. 2021, 29, 1–20. [Google Scholar] [CrossRef]
- Health Environment Research Agenda for Europe (HERA) Consortium. HERA-COVID-19: Research Needs on COVID-19/Environment & Health Nexus; Health Environment Research Agenda for Europe: Montpellier, France, 2020. [Google Scholar]
- World Health Organization. WHO Global Strategic Directions for Nursing and Midwifery 2021–2025. DRAFT 1 April 2021, Inclusive of Comments from Member States Made in the Period 9–29 March 2021. Available online: https://cdn.who.int/media/docs/default-source/health-workforce/who_strategic-directions-for-nursing-and-midwifery-2021-2025.pdf?sfvrsn=a5ffe81f_5&download=true (accessed on 9 June 2021).
- Chan, D.W.-K. A reflection on the anti-epidemic response of COVID-19 from the perspective of disaster management. Int. J. Nurs. Sci. 2020, 7, 382–385. [Google Scholar] [CrossRef] [PubMed]
- Haldane, V.; De Foo, C.; Abdalla, S.M.; Jung, A.-S.; Tan, M.; Wu, S.; Chua, A.; Verma, M.; Shrestha, P.; Singh, S.; et al. Health systems resilience in managing the COVID-19 pandemic: Lessons from 28 countries. Nat. Med. 2021, 27, 964–980. [Google Scholar] [CrossRef]
- Kruk, M.E.; Myers, M.; Varpilah, S.T.; Dahn, B.T. What is a resilient health system? Lessons from Ebola. Lancet 2015, 385, 1910–1912. [Google Scholar] [CrossRef]
- Morton, T.A.; Atkinson, T.; Brooker, D.; Wong, G. The sustainability of community interventions for people affected by dementia: A realist review. Alzheimer’s Dement. 2020, 16, e039708. [Google Scholar] [CrossRef]
- Kuliga, S.; Berwig, M.; Roes, M. Wayfinding in People with Alzheimer’s Disease: Perspective Taking and Architectural Cognition—A Vision Paper on Future Dementia Care Research Opportunities. Sustainability 2021, 13, 1084. [Google Scholar] [CrossRef]
- Shelton, R.C.; Cooper, B.R.; Stirman, S.W. The Sustainability of Evidence-Based Interventions and Practices in Public Health and Health Care. Annu. Rev. Public Health 2018, 39, 55–76. [Google Scholar] [CrossRef] [Green Version]
- Chambers, D.A.; Glasgow, R.E.; Stange, K.C. The dynamic sustainability framework: Addressing the paradox of sustainment amid ongoing change. Implement. Sci. 2013, 8, 117. [Google Scholar] [CrossRef] [Green Version]
- Cacace, M.; Ettelt, S.; Mays, N.; Nolte, E. Assessing quality in cross-country comparisons of health systems and policies: Towards a set of generic quality criteria. Health Policy 2013, 112, 156–162. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Health Emergency and Disaster Risk Management. Available online: https://www.who.int/hac/techguidance/preparedness/risk-management-disabilities-december2017.pdf?ua=1 (accessed on 31 July 2020).
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Public Health England. Disparities in the Risk and Outcomes of COVID-19; Public Health England: London, UK, 2020.
- Wang, Q.; Davis, P.B.; Gurney, M.E.; Xu, R. COVID-19 and dementia: Analyses of risk, disparity, and outcomes from electronic health records in the US. Alzheimer’s Dement. 2021, 17, 1297–1306. [Google Scholar] [CrossRef]
- Lapsley, H.; Kerse, N.; Moyes, S.A.; Keeling, S.; Muru-Lanning, M.L.; Wiles, J.; Jatrana, S. Do household living arrangements explain gender and ethnicity differences in receipt of support services? Findings from LiLACS NZ Māori and non-Māori advanced age cohorts. Ageing Soc. 2020, 40, 1004–1020. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Social Determinants of Health. Available online: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_3 (accessed on 8 July 2021).
- Kerpershoek, L.; de Vugt, M.; Wolfs, C.; Orrell, M.; Woods, B.; Jelley, H.; Meyer, G.; Bieber, A.; Stephan, A.; Selbæk, G.; et al. Is there equity in initial access to formal dementia care in Europe? The Andersen Model applied to the Actifcare cohort. Int. J. Geriatr. Psychiatry 2020, 35, 45–52. [Google Scholar] [CrossRef] [Green Version]
- Bambra, C.; Riordan, R.; Ford, J.; Matthews, F. The COVID-19 pandemic and health inequalities. J. Epidemiol. Commun. Health 2020, 74, 964. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, A.; Pina-Escudero, S.; Possin, K.; Quiroz, Y.; Peres, F.; Slachevsky, A.; Sosa-Ortiz, A.; Brucki, S.; Miller, B. Dementia caregiving across Latin America and the Caribbean and brain health diplomacy. Lancet Healthy Longev. 2021, 2, e222–e231. [Google Scholar] [CrossRef]
- Ibanez, A.; Santamaria-Garcia, H.; Guerrero Barragan, A.; Kornhuber, A.; Ton, A.M.M.; Slachevsky, A.; Teixeira, A.L.; Mar Meza, B.M.; Serrano, C.M.; Cano, C.; et al. The impact of SARS-CoV-2 in dementia across Latin America: A call for an urgent regional plan and coordinated response. Alzheimer’s Dement. 2020, 6, e12092. [Google Scholar] [CrossRef]
- United Nations. Convention on the Rights of Persons with Disabilities and Optional Protocol; United Nations: Geneva, Switzerland, 2006; Available online: https://www.un.org/disabilities/documents/convention/convoptprot-e.pdf (accessed on 19 August 2020).
- The World Bank. The World Bank in Chile. Available online: https://www.worldbank.org/en/country/chile (accessed on 11 August 2020).
- Economic and Development Review Committee (EDRC). OECD Economic Surveys: New Zealand Organization for Economic Co-Operation and Development (OECD); Economic and Development Review Committee: Paris, France, 2019. [Google Scholar]
- Economic and Development Review Committee (EDRC). OECD Economic Surveys: Germany Organization for Economic Co-Operation and Development (OECD); Economic and Development Review Committee (EDRC): Paris, France, 2018. [Google Scholar]
- Organization for Economic Co-Operation and Development (OECD). OECD-Health-Statistics-2019-Frequently-Requested-Data; OECD: Paris, France, 2019. [Google Scholar]
- Lincoln, M. A special self-image is no defence against COVID-19. Nature 2020, 585, 325. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization Regional Office for Europe. Germany. Available online: https://www.euro.who.int/en/countries/germany (accessed on 9 September 2020).
- Ministerio de Salud Gobierno de Chile. Plan Nacional de Demencia 2017; Ministerio de Salud Gobierno de Chile: Santiago, Chile, 2017.
- Ministry of Health. New Zealand Framework for Dementia Care; Ministry of Health: Wellington, New Zealand, 2013.
- New Zealand Dementia Cooperative; Alzheimers New Zealand; Dementia New Zealand. Improving Dementia Services in New Zealand-Dementia Action Plan 2020 to 2025. 2020. Available online: https://carers.net.nz/information/dementia-action-plan-2020-2025/ (accessed on 19 March 2021).
- Bundesministerium für Familie Senioren Frauen und Jugend (BMFSJ); Bundesministerium für Gesundheit (BMG). Nationale Demenzstrategie; Bundesministerium für Familie Senioren Frauen und Jugend: Berlin, Germany; Bundesministerium für Gesundheit (BMG): Berlin, Germany, 2020; p. 149.
- Ritchie, H.; Ortiz-Ospina, E.; Beltekian, D.; Mathieu, E.; Hasell, J.; Macdonald, B.; Giattino, C.; Appel, C.; Rodés-Guirao, L.; Roser, M.; et al. Our World in Data: Coronavirus (COVID-19) Vaccinations. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 15 May 2021).
- Leng, A.; Lemahieu, H. Lowy Institute Covid Performance Index. Deconstructing Pandemic Responses: What Impact Have Geography, Political Systems, Population Size, and Economic Development Had on COVID-19 Outcomes Around the World? Based on Data Available to 13 March 2021. Available online: https://interactives.lowyinstitute.org/features/covid-performance/ (accessed on 15 May 2021).
- World Health Organization. Global Action Plan on the Public Health Response to Dementia 2017–2025; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Dawson, W.D.; Ashcroft, E.C.; Lorenz-Dant, K.; Comas-Herrera, A. Impact of the COVID-19 Outbreak on Community-Based Care Services: A Review of Initial International Policy Reponses; International Long-Term Care Policy Network; CPEC-LSE: London, UK, 2020; Available online: https://ltccovid.org/wp-content/uploads/2020/06/Community-Based-Care-Report-19-May.pdf (accessed on 23 February 2021).
- Slachevsky, A.; Gajardo, J. Chile: Dementia Care: International Perspectives; Oxford University Press: Oxford, UK, 2019; pp. 329–336. [Google Scholar]
- Leon, T.; Castro, L.; Mascayano, F.; Lawlor, B.; Slachevsky, A. Evaluating a Memory Clinic Using the RE-AIM Model. The Experience of the “Memory and Neuropsychiatry Clinic” in Hospital Del Salvador, Chile. Front. Neurol. 2021, 12, 1474. [Google Scholar] [CrossRef]
- Slachevsky, A. Brian Lawlor Presents a Dementia Policy Paper to the Chilean National Congress. Available online: https://archive.gbhi.org/news-1/2019/7/18/brian-lawlor-presents-a-dementia-policy-paper-to-the-chilean-national-congress (accessed on 21 March 2021).
- Superintendencia de Salud. Garantías Explícitas en Salud (GES). Available online: http://www.supersalud.gob.cl/difusion/665/w3-propertyvalue-1962.html (accessed on 19 April 2021).
- World Health Organization; Bramley, D.E. Implementation of the Universal Access with Explicit Guarantees (AUGE). Reform. 2015. Available online: https://www.who.int/health_financing/documents/Efficiency_health_systems_Chile/en/ (accessed on 19 April 2021).
- Custodio, N.; Wheelock, A.; Thumala, D.; Slachevsky, A. Dementia in Latin America: Epidemiological evidence and implications for public policy. Front. Aging Neurosci. 2017, 9, 221. [Google Scholar] [CrossRef]
- Slachevsky, A. Reflexiones e integración. In Cuadernillo Nº1: Serie Envejecimiento: “¿Dónde envejecemos en Chile? Reflexiones Transdisciplinarias en Torno a Movilidad, Urbanismo, Vivienda y Trayectorias Cotidianas de las Personas Mayores—Resultados de la Quinta Escuela Internacional de Verano Sobre Envejecimiento 2018. Vicerrectoría de Investigación y Desarrollo; Universidad de Chile & COPRAD: Santiago, Chile, 2019; pp. 60–76. Available online: https://www.algec.org/wp-content/uploads/2019/04/Donde-envejecemos-en-Chile.pdf (accessed on 18 April 2021).
- Ibanez, A.; Yokoyama, J.S.; Possin, K.L.; Matallana, D.; Lopera, F.; Nitrini, R.; Takada, L.T.; Custodio, N.; Sosa Ortiz, A.L.; Avila-Funes, J.A.; et al. The Multi-Partner Consortium to Expand Dementia Research in Latin America (ReDLat): Driving Multicentric Research and Implementation Science. Front. Neurol. 2021, 12, 103. [Google Scholar] [CrossRef] [PubMed]
- Slachevsky, A.; Budinich, M.; Miranda-Castillo, C.; Núñez-Huasaf, J.; Silva, J.R.; Munoz-Neira, C.; Gloger, S.; Jimenez, O.; Martorell, B.; Delgado, C. The CUIDEME Study: Determinants of burden in Chilean primary caregivers of patients with dementia. J. Alzheimer’s Dis. 2013, 35, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Hojman, D.A.; Duarte, F.; Ruiz-Tagle, J.; Budnich, M.; Delgado, C.; Slachevsky, A. The cost of dementia in an unequal country: The case of Chile. PLoS ONE 2017, 12, e0172204. [Google Scholar] [CrossRef] [PubMed]
- Tapia Muñoz, T.; Slachevsky, A.; León-Campos, M.O.; Madrid, M.; Caqueo-Urízar, A.; Rohde, G.C.; Miranda-Castillo, C. Predictors of unmet needs in Chilean older people with dementia: A cross-sectional study. BMC Geriatr. 2019, 19, 106. [Google Scholar] [CrossRef] [Green Version]
- Gajardo, J.; Aravena, J.; Navarrete, I.; Slachevsky, A.; Gitlin, L.N. Cultural adaptation of the Tailored Activity Program (TAP) in Chile: Implementation challenges and pilot testing: Dementia care research (research projects; nonpharmacological)/Cross-cultural studies and cultural/Linguistic adaptations. Alzheimer’s Dement. 2020, 16, e042222. [Google Scholar] [CrossRef]
- Browne, J.; Fasce, G.; Pineda, I.; Villalobos, P. Policy Response to COVID-19 in Long-Term Care Facilities in Chile. 2020. Available online: https://www.researchgate.net/profile/Gerardo-Fasce/publication/343686741_Policy_response_to_COVID-19_in_Long-Term_Care_Facilities_in_Chile/links/5f39c67792851cd302fe0282/Policy-response-to-COVID-19-in-Long-Term-Care-Facilities-in-Chile.pdf (accessed on 21 March 2021).
- Villalobos Dintrans, P.; Browne, J.; Madero-Cabib, I. It is not just mortality: A call from Chile for comprehensive COVID-19 policy responses among older people. J. Gerontol. B Psychol. Sci. Soc. Sci. 2020, 76, e275–e280. [Google Scholar] [CrossRef]
- Herrera, M.S.; Elgueta, R.; Fernández, M.B.; Giacoman, C.; Leal, D.; Marshall, P.; Rubio, M.; Bustamante, F. A longitudinal study monitoring the quality of life in a national cohort of older adults in Chile before and during the COVID-19 outbreak. BMC Geriatr. 2021, 21, 143. [Google Scholar] [CrossRef]
- Cullum, S.; Varghese, C.; Coomarasamy, C.; Whittington, R.; Hadfield, L.; Rajay, A.; Yeom, B.; Liu, B.; Christie, M.; Appleton, K. Predictors of mortality in Māori, Pacific Island, and European patients diagnosed with dementia at a New Zealand Memory Service. Int. J. Geriatr. Psychiatry 2020, 35, 516–524. [Google Scholar] [CrossRef]
- Casey, J.; Cheung, G. New Zealand. Dementia Care: International Perspectives; Oxford University Press: Oxford, UK, 2019; pp. 115–120. [Google Scholar]
- Kerse, N.; Teh, R.; Moyes, S.A.; Broad, J.; Rolleston, A.; Gott, M.; Kepa, M.; Wham, C.; Hayman, K.; Jatrana, S. Cohort profile: Te puawaitanga o Nga tapuwae Kia Ora tonu, life and living in advanced Age: A cohort study in New Zealand (LiLACS NZ). Int. J. Epidemiol. 2015, 44, 1823–1832. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cullum, S.; Mullin, K.; Zeng, I.; Yates, S.; Payman, V.; Fisher, M.; Cheung, G. Do community-dwelling Māori and Pacific peoples present with dementia at a younger age and at a later stage compared with NZ Europeans? Int. J Geriatr. Psychiatry 2018, 33, 1098–1104. [Google Scholar] [CrossRef]
- Dudley, M.; Menzies, O.; Elder, H.; Nathan, L.; Garrett, N.; Wilson, D. Mate wareware: Understanding ‘dementia’ from a Māori perspective. N. Z. Med. J. (Online) 2019, 132, 66–74. [Google Scholar] [PubMed]
- Battineni, G.; Pallotta, G.; Nittari, G.; Amenta, F. Telemedicine framework to mitigate the impact of the COVID-19 pandemic. J. Taibah. Univ. Med. Sci. 2021, 16, 300–302. [Google Scholar] [CrossRef]
- Cheung, G.; Peri, K. Challenges to dementia care during COVID-19: Innovations in remote delivery of group Cognitive Stimulation Therapy. Aging Ment. Health 2021, 25, 977–979. [Google Scholar] [CrossRef] [PubMed]
- Bickel, H. Incidence and Prevalence of Dementia (Key Aspects 1) [Die Häufigkeit von Demenzerkrankungen (Das Wichtigste 1)]; Deutsche Alzheimer Gesellschaft: Berlin, Germany, 2020. [Google Scholar]
- Schmachtenberg, T.; Monsees, J.; Hoffmann, W.; van den Berg, N.; Stentzel, U.; Thyrian, J.R. Comparing national dementia plans and strategies in Europe—Is there a focus of care for people with dementia from a migration background? BMC Public Health 2020, 20, 784. [Google Scholar] [CrossRef]
- Laporte Uribe, F.; Wolf-Ostermann, K.; Wubbeler, M.; Holle, B. Care Arrangements in Dementia Care Networks: Findings From the DemNet-D Study Baseline and 1-Year Follow-Up. J. Aging Health 2018, 30, 882–903. [Google Scholar] [CrossRef]
- Gove, D.; Diaz-Ponce, A.; Georges, J.; Moniz-Cook, E.; Mountain, G.; Chattat, R.; Oksnebjerg, L.; European Working Group of People with, Dementia. Alzheimer Europe’s position on involving people with dementia in research through PPI (patient and public involvement). Aging Ment. Health 2018, 22, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Hajek, A.; De Bock, F.; Wieler, L.H.; Sprengholz, P.; Kretzler, B.; König, H.-H. Perceptions of Health Care Use in Germany during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health (Online) 2020, 17, 9351. [Google Scholar] [CrossRef]
- Michalowsky, B.; Hoffmann, W.; Bohlken, J.; Kostev, K. Effect of the COVID-19 lockdown on disease recognition and utilisation of healthcare services in the older population in Germany: A cross-sectional study. Age Ageing 2021, 50, 317–325. [Google Scholar] [CrossRef]
- Burns, A.; Lobo, A.; Olde Rikkert, M.; Robert, P.; Sartorius, N.; Semrau, M.; Stoppe, G. COVID 19 and dementia: Experience from six European countries. Int. J. Geriatr. Psychiatry 2021, 36, 943–949. [Google Scholar] [CrossRef]
- Beaglehole, R.; Bonita, R. What is global health? Glob. Health Action 2010, 3. [Google Scholar] [CrossRef]
- World Health Organization. Constitution of the World Health Organization; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Luhmann, N. Differentiation of Society. Can. J. Soc. Cahiers Can. Soc. 1977, 2, 29–53. [Google Scholar] [CrossRef]
- World Health Organization. Everybody Business: Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Frenk, J. The global health system: Strengthening national health systems as the next step for global progress. PLoS Med. 2010, 7, e1000089. [Google Scholar] [CrossRef] [Green Version]
- Adam, T.; Hsu, J.; de Savigny, D.; Lavis, J.N.; Røttingen, J.-A.; Bennett, S. Evaluating health systems strengthening interventions in low-income and middle-income countries: Are we asking the right questions? Health Policy Plan. 2012, 27, iv9–iv19. [Google Scholar] [CrossRef] [PubMed]
- Murray, C.J.; Frenk, J. A framework for assessing the performance of health systems. Bull. World Health Organ. 2000, 78, 717–731. [Google Scholar]
- Alzheimer’s Disease International. World Alzheimer Report 2019: Attitudes to Dementia; Alzheimers’s Disease International: London, UK, 2019. [Google Scholar]
- Roberts, C.; Rochford-Brennan, H.; Goodrick, J.; Gove, D.; Diaz-Ponce, A.; Georges, J. Our reflections of Patient and Public Involvement in research as members of the European Working Group of People with Dementia. Dementia 2019, 19, 10–17. [Google Scholar] [CrossRef]
- Schilling, I.; Gerhardus, A. Methods for involving older people in health research—A review of the literature. Int. J. Environ. Res. Public Health 2017, 14, 1476. [Google Scholar] [CrossRef] [Green Version]
- Batt, A.M.; Delport, S.; Cummins, F.H. Disaster Preparedness and Response in Older Adults: A Review and Discussion. Faculty & Staff Publications—Public Safety. 9. 2018. Available online: https://first.fanshawec.ca/fhcsps_publicsafety_facultystaffpublications/9 (accessed on 12 August 2021).
- Chaudoir, S.R.; Dugan, A.G.; Barr, C.H.I. Measuring factors affecting implementation of health innovations: A systematic review of structural, organizational, provider, patient, and innovation level measures. Implement. Sci. 2013, 8, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.; Milat, A.; Grunseit, A.; Conte, K.; Wolfenden, L.; Bauman, A. The Intervention Scalability Assessment Tool: A pilot study assessing five interventions for scalability. Public Health Res. Pract. 2020, 30, e3022011. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Transmission of SARS-CoV-2: Implications for Infection Prevention Precautions. Scientific Brief; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Van Bavel, J.J.; Baicker, K.; Boggio, P.S.; Capraro, V.; Cichocka, A.; Cikara, M.; Crockett, M.J.; Crum, A.J.; Douglas, K.M.; Druckman, J.N.; et al. Using social and behavioural science to support COVID-19 pandemic response. Nat. Hum. Behav. 2020, 4, 460–471. [Google Scholar] [CrossRef]
- Perrotta, D.; Grow, A.; Rampazzo, F.; Cimentada, J.; Del Fava, E.; Gil-Clavel, S.; Zagheni, E. Behaviors and attitudes in response to the COVID-19 pandemic: Insights from a cross-national Facebook survey. EPJ Data Sci. 2021, 10, 1–13. [Google Scholar] [CrossRef]
- Electoral Commission New Zealand. Mō Te Kaitiaki Take Kōwhiri. 2020 General Election and Referendums—Official Result. Nationwide Party Votes Results. Available online: https://www.electionresults.govt.nz/electionresults_2020/ (accessed on 12 November 2020).
- Watson, K. Jubilation as Chile Votes to Rewrite Constitution. BBC News, 2020. Available online: https://www.bbc.com/news/world-latin-america-54687090(accessed on 12 November 2020).
- Roy, E.A. ‘Go Hard, Go Early’—Now New Zealand Goes Back to the Drawing Board. Guard, 2020. Available online: https://www.theguardian.com/world/2020/aug/16/go-hard-go-early-now-new-zealand-goes-back-to-the-drawing-board(accessed on 17 August 2020).
- Parada, F. Chile lockdown: Anti-Government Protest Broken Up by Police. BBC News. 2020. Available online: https://www.bbc.com/news/world-latin-america-52370165 (accessed on 12 November 2020).
- Lopes, H.; McKay, V. Adult learning and education as a tool to contain pandemics: The COVID-19 experience. Int. Rev. Educ. 2020, 66, 575–602. [Google Scholar] [CrossRef] [PubMed]
- The Lancet. COVID-19: Too little, too late? Lancet 2020, 395, 755. [Google Scholar] [CrossRef]
- World Health Organization. Let’s Flatten the Infodemic Curve. Available online: https://www.who.int/news-room/spotlight/let-s-flatten-the-infodemic-curve (accessed on 26 November 2020).
- Ceron, W.; Sanseverino, G.G.; de-Lima-Santos, M.-F.; Quiles, M.G. COVID-19 fake news diffusion across Latin America. Soc. Netw. Anal. Min. 2021, 11, 47. [Google Scholar] [CrossRef]
- Tuohy, R.; Stephens, C. Older adults’ meanings of preparedness: A New Zealand perspective. Ageing Soc. 2015, 36, 613–630. [Google Scholar] [CrossRef]
- Stichweh, R. Simplifikation des Sozialen. Die Corona-Pandemie und die Funktionssysteme der Weltgesellschaft [Simplification of social life]. In Frankfurter Allgemeine Zeitung (FAZ); Marc Weingart, W.; Virginia Stichweh, Y., Translators; Frankfurter Allgemeine Zeitung GmbH: Frankfurt (Main), Germany, 2020; p. 9. [Google Scholar]
- Schnitker, L.; Fielding, E.; MacAndrew, M.; Beattie, E.; Lie, D.; FitzGerald, G. A national survey of aged care facility managers’ views of preparedness for natural disasters relevant to residents with dementia. Aust. J. Ageing 2019, 38, 182–189. [Google Scholar] [CrossRef]
- Heppenstall, C.P.; Wilkinson, T.J.; Hanger, H.C.; Dhanak, M.R.; Keeling, S. Impacts of the emergency mass evacuation of the elderly from residential care facilities after the 2011 Christchurch earthquake. Disaster Med. Public Health Prep. 2013, 7, 419–423. [Google Scholar] [CrossRef]
- Willoughby, M.; Kipsaina, C.; Ferrah, N.; Blau, S.; Bugeja, L.; Ranson, D.; Ibrahim, J.E. Mortality in nursing homes following emergency evacuation: A systematic review. J. Am. Med. Dir. Assoc. 2017, 18, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Annabell, T.; Nairn, A. Flagging a ‘new’ New Zealand: The discursive construction of national identity in the Flag Consideration Project. Crit. Discourse Stud. 2019, 16, 96–111. [Google Scholar] [CrossRef]
- Immigration New Zealand. Welcoming Communities. Available online: https://www.immigration.govt.nz/about-us/what-we-do/welcoming-communities (accessed on 6 September 2021).
- Shea, B.; Aspin, C.; Ward, J.; Archibald, C.; Dickson, N.; McDonald, A.; Penehira, M.; Halverson, J.; Masching, R.; McAllister, S. HIV diagnoses in indigenous peoples: Comparison of Australia, Canada and New Zealand. Int. Health 2011, 3, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Sternberg, S.A.; Shinan-Altman, S.; Volicer, L.; Casarett, D.J.; van der Steen, J.T. Palliative Care in Advanced Dementia: Comparison of Strategies in Three Countries. Geriatrics 2021, 6, 44. [Google Scholar] [CrossRef] [PubMed]
- Henderson, C.; Rehill, A.; Brooker, D.; Evans, S.C.; Evans, S.B.; Bray, J.; Saibene, F.L.; Scorolli, C.; Szcześniak, D.; d’Arma, A.; et al. Costs and cost-effectiveness of the meeting centres support programme for people living with dementia and carers in Italy, Poland and the UK: The MEETINGDEM study. Health Soc. Care Community 2021. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Chile | New Zealand | Germany |
|---|---|---|---|
| Socio-economic aspects | one of Latin America’s fastest-growing economies in recent decades, enabling the country to significantly reduce poverty; however, more than 30% of the population is economically vulnerable, and income inequality remains high [46] | economic growth is stable and well-being is generally high, but the income distribution is more unequal than the OECD average; “education, health and housing outcomes vary strongly by socio-economic background and ethnicity—Māori and Pasifika tend to fare worse” [47] | highly industrialized, densely populated, high-income country; robust economic growth and high well-being [48] |
| Geophysical, geo-political location | isolated location (Andes as a natural barrier) | isolated geographic location, island | Western European country, having a (land-)border with 9 countries |
| Hazards | frequent and often high-magnitude geophysical (earthquakes, tsunamis, volcanoes, landslides), climatological and meteorological (especially draughts during the last decade in the northern and central parts of the country, ENSO (ENSO: El Niño Southern Oscillation) events) hazards with the potential to create disasters | frequent and often high-magnitude geophysical hazards (earthquakes, tsunamis, landslides, volcanoes) with the potential to create disasters, no frequent meteorological hazards | no frequent geophysical and moderate meteorological hazards, but increasing hazards related to heat stress |
| Political stability | politically rather unstable (ongoing political protests, referendum for a new constitution passed on 25 October 2020) | politically stable (re-election of J. Ardern as prime minister in October 2020) | politically stable |
| Health system | dual health care system, public covers 78% of the population, high out-of-pocket expenditures (35,1%) [49]; recently, the Explicit Guarantees System included Alzheimer disease and other dementias; health care system “robust” but also revealing high “levels of inequity” [50] | health services primarily funded by the central government, 12.9% out-of-pocket expenses [49] | the health care system is administered through several autonomous bodies and associations [51], 12.3% out-of-pocket expenses [49]; universal long-term care insurance also for the older population covering home- and community-based services as well as institutional services |
| National dementia strategy | National Plan for Dementia launched in 2017 [52] | New Zealand Framework for Dementia Care published in 2013 [53]; the National Dementia Plan 2020–25 has not been implemented by government yet [54] | “Alliance for People with Dementia” since 2012 followed by the National Dementia Strategy launched in 2020 [55] |
| COVID-19 | Confirmed Cases | Deaths | Persons Vaccinated with at Least One Dose |
|---|---|---|---|
| per 100,000 1 | per 100,000 1 | per 100 1 | |
| Chile | 4688.33 | 113.89 | 32.09 |
| New Zealand | 43.05 | 0.54 | 0.37 |
| Germany | 3074.39 | 87.63 | 9.2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Laporte Uribe, F.; Arteaga, O.; Bruchhausen, W.; Cheung, G.; Cullum, S.; Fuentes-García, A.; Miranda Castillo, C.; Kerse, N.; Kirk, R.; Muru-Lanning, M.; et al. Dementia and COVID-19 in Chile, New Zealand and Germany: A Research Agenda for Cross-Country Learning for Resilience in Health Care Systems. Sustainability 2021, 13, 10247. https://doi.org/10.3390/su131810247
Laporte Uribe F, Arteaga O, Bruchhausen W, Cheung G, Cullum S, Fuentes-García A, Miranda Castillo C, Kerse N, Kirk R, Muru-Lanning M, et al. Dementia and COVID-19 in Chile, New Zealand and Germany: A Research Agenda for Cross-Country Learning for Resilience in Health Care Systems. Sustainability. 2021; 13(18):10247. https://doi.org/10.3390/su131810247
Chicago/Turabian StyleLaporte Uribe, Franziska, Oscar Arteaga, Walter Bruchhausen, Gary Cheung, Sarah Cullum, Alejandra Fuentes-García, Claudia Miranda Castillo, Ngaire Kerse, Ray Kirk, Marama Muru-Lanning, and et al. 2021. "Dementia and COVID-19 in Chile, New Zealand and Germany: A Research Agenda for Cross-Country Learning for Resilience in Health Care Systems" Sustainability 13, no. 18: 10247. https://doi.org/10.3390/su131810247
APA StyleLaporte Uribe, F., Arteaga, O., Bruchhausen, W., Cheung, G., Cullum, S., Fuentes-García, A., Miranda Castillo, C., Kerse, N., Kirk, R., Muru-Lanning, M., Salinas Ríos, R. A., Schrott, L., Slachevsky, A., & Roes, M. (2021). Dementia and COVID-19 in Chile, New Zealand and Germany: A Research Agenda for Cross-Country Learning for Resilience in Health Care Systems. Sustainability, 13(18), 10247. https://doi.org/10.3390/su131810247