
Enhancing Air Quality for Embedded Hospital Germicidal Lamps

Abstract
:1. Introduction
2. Simulation Approach
2.1. Governing Equations
- (a)
- x-direction momentum equation
- (b)
- y-direction momentum equation
- (c)
- z-direction momentum equationwhere U, V, and W are the mean flow velocities in the x, y, and z directions, respectively; P is the mean flow pressure. And , , and denote the fluid density, dynamic viscosity, and turbulent eddy viscosity, respectively. The turbulent eddy viscosity was obtained from the two-equation k-ε turbulent model by Equation (4).
2.2. Lamp and Fan Geometries
2.3. Material Properties
2.4. Simulation Steps
- (1)
- Model Definition and Simplification
- (2)
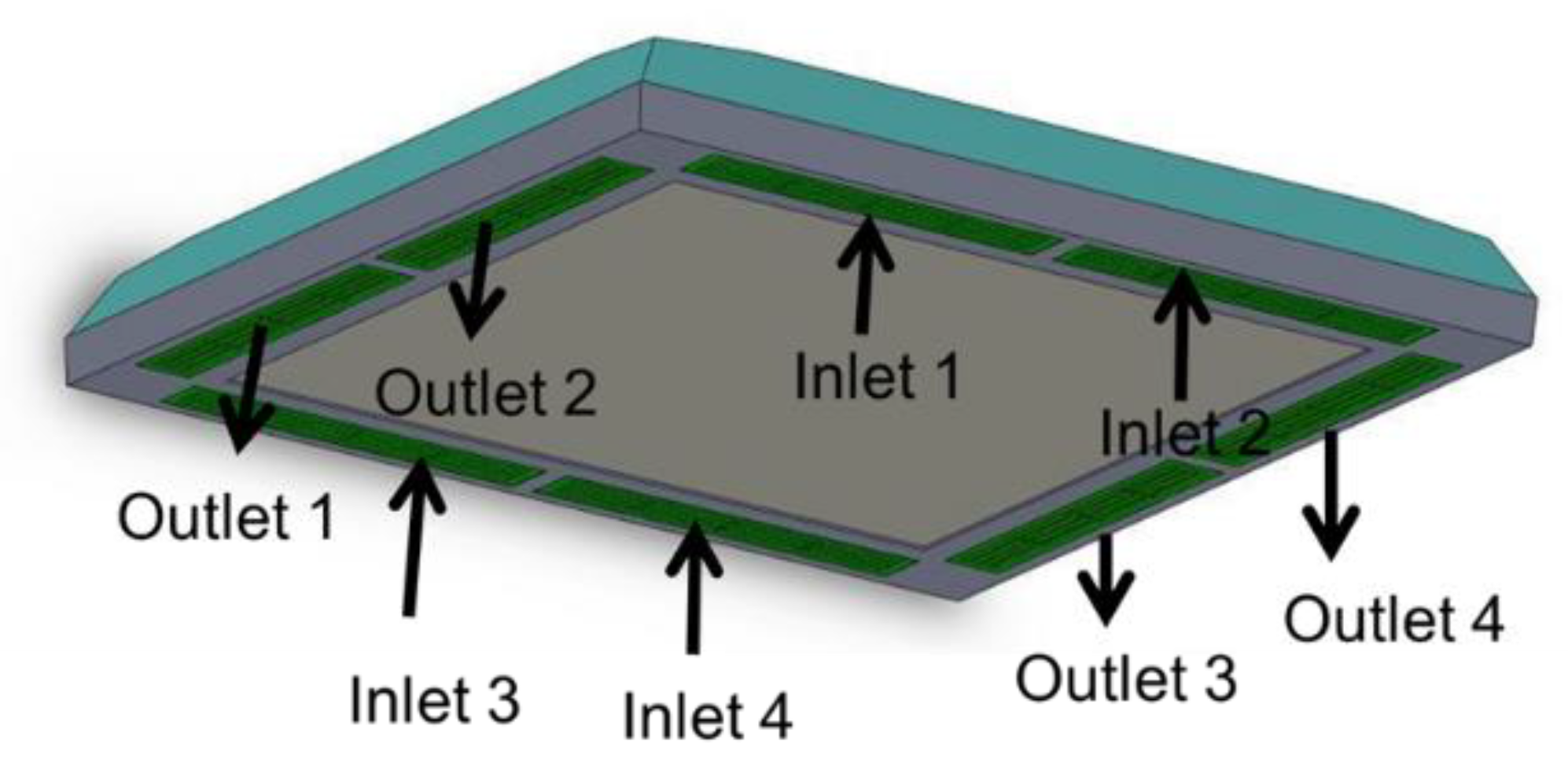
- Boundary Conditions
- (3)
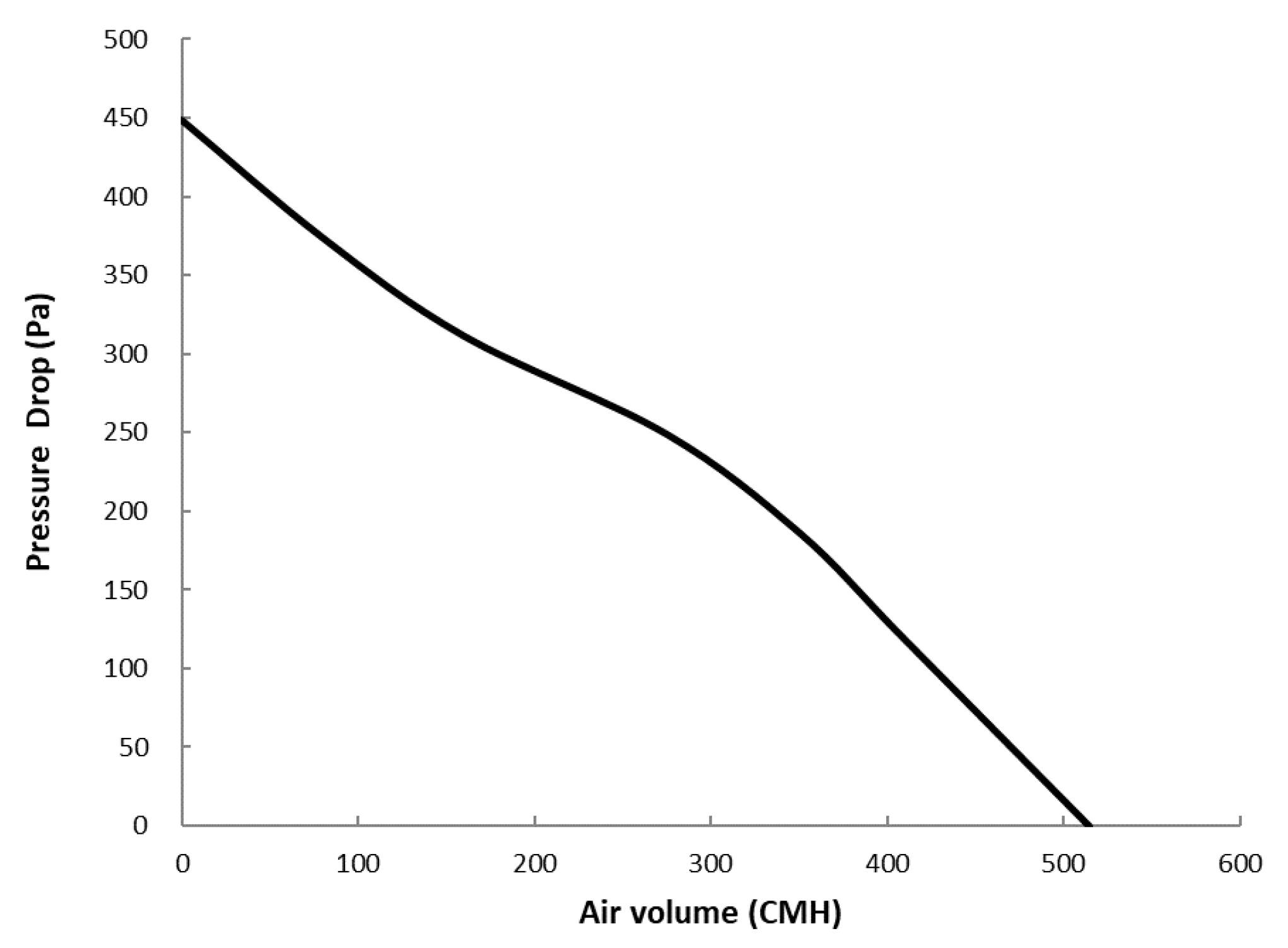
- Fan Performance Curve
- (4)
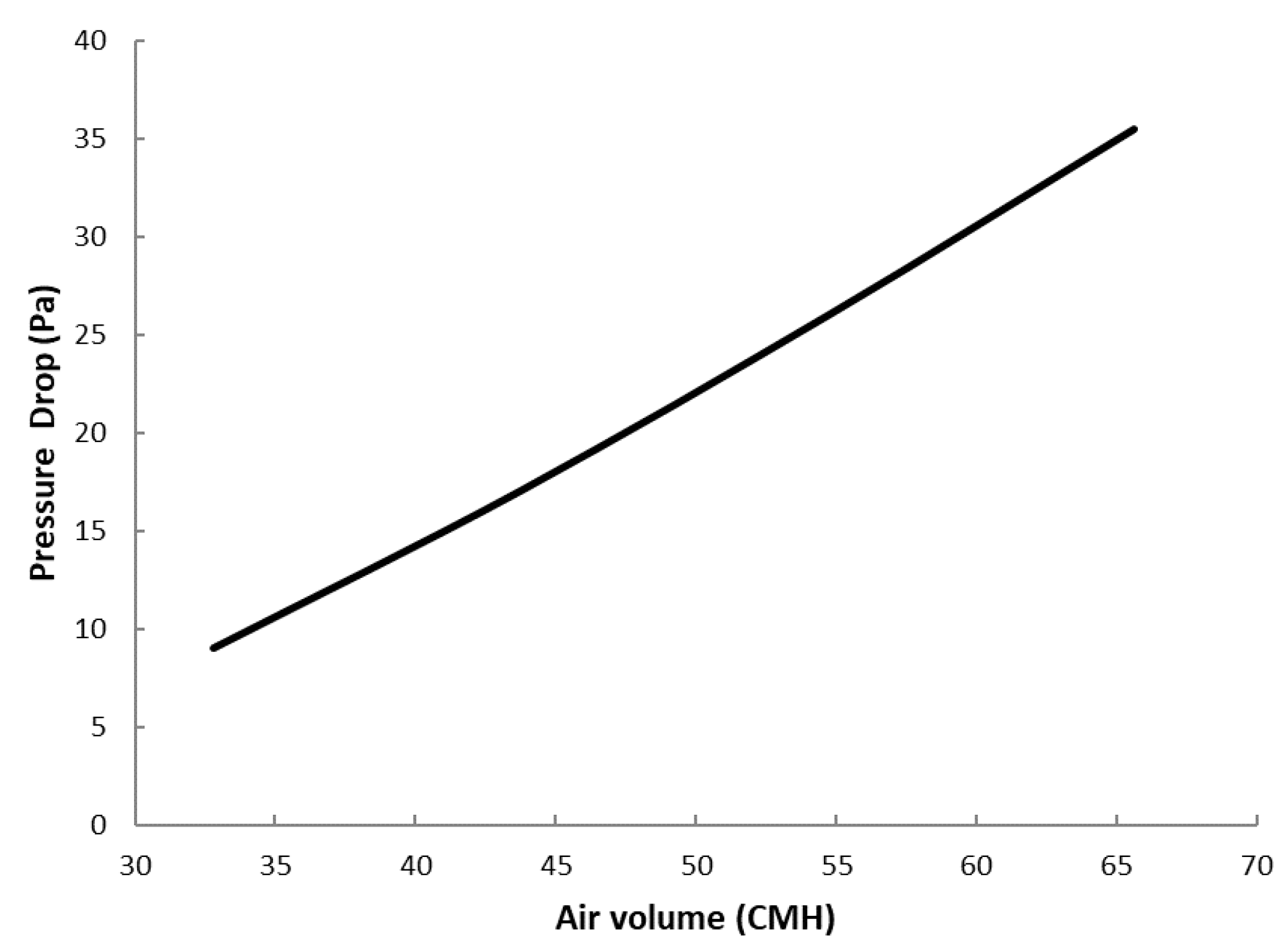
- Filter Resistance Curve
- (5)
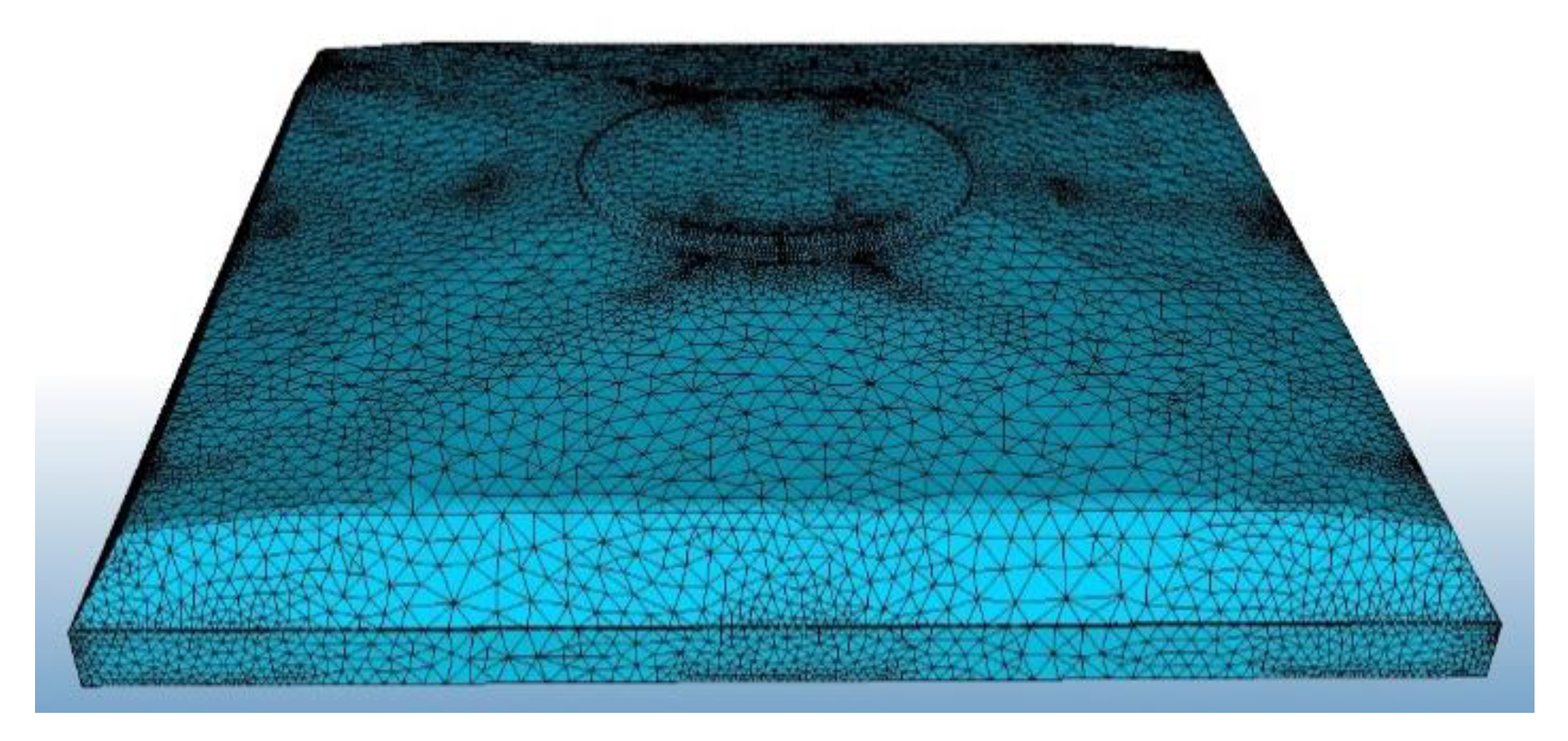
- Mesh and convergence test
3. Results and Discussion
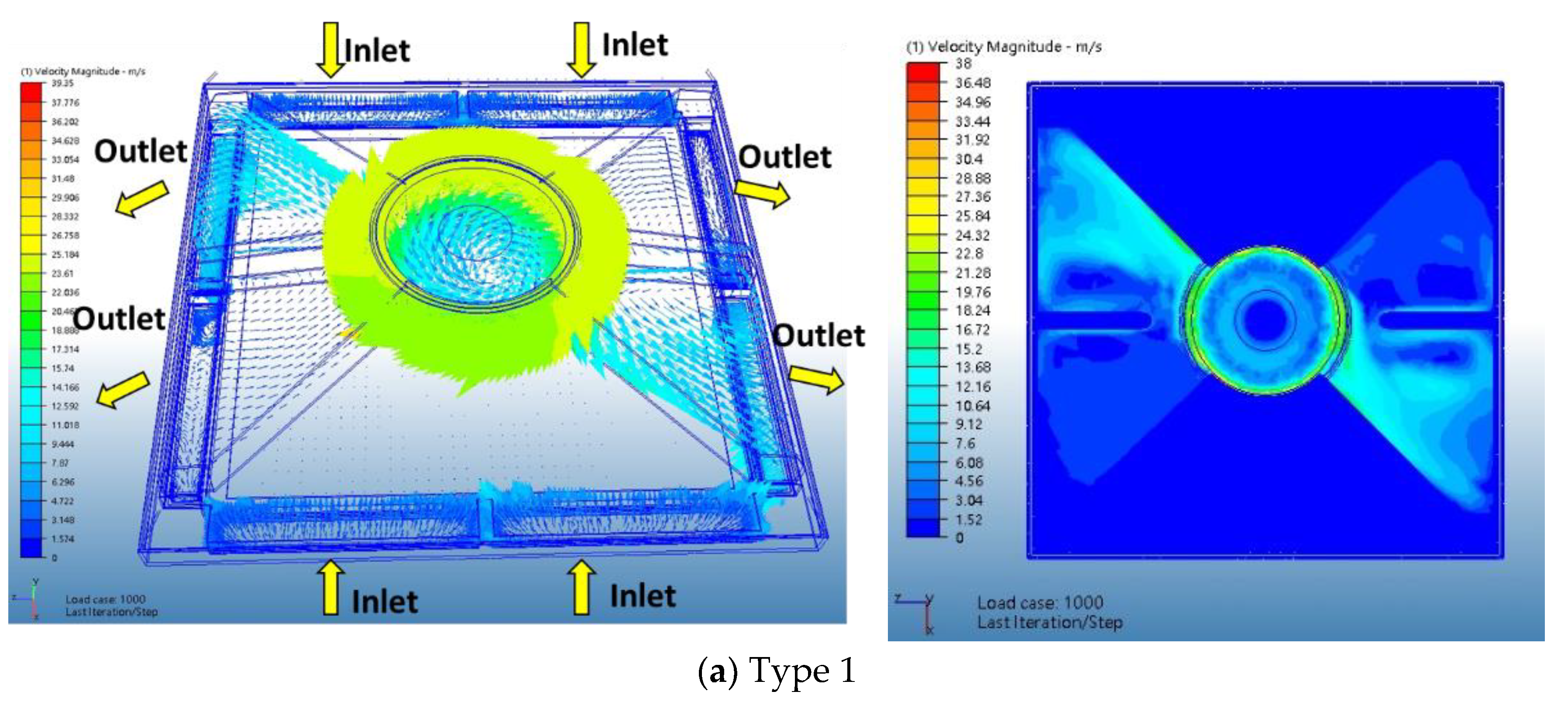
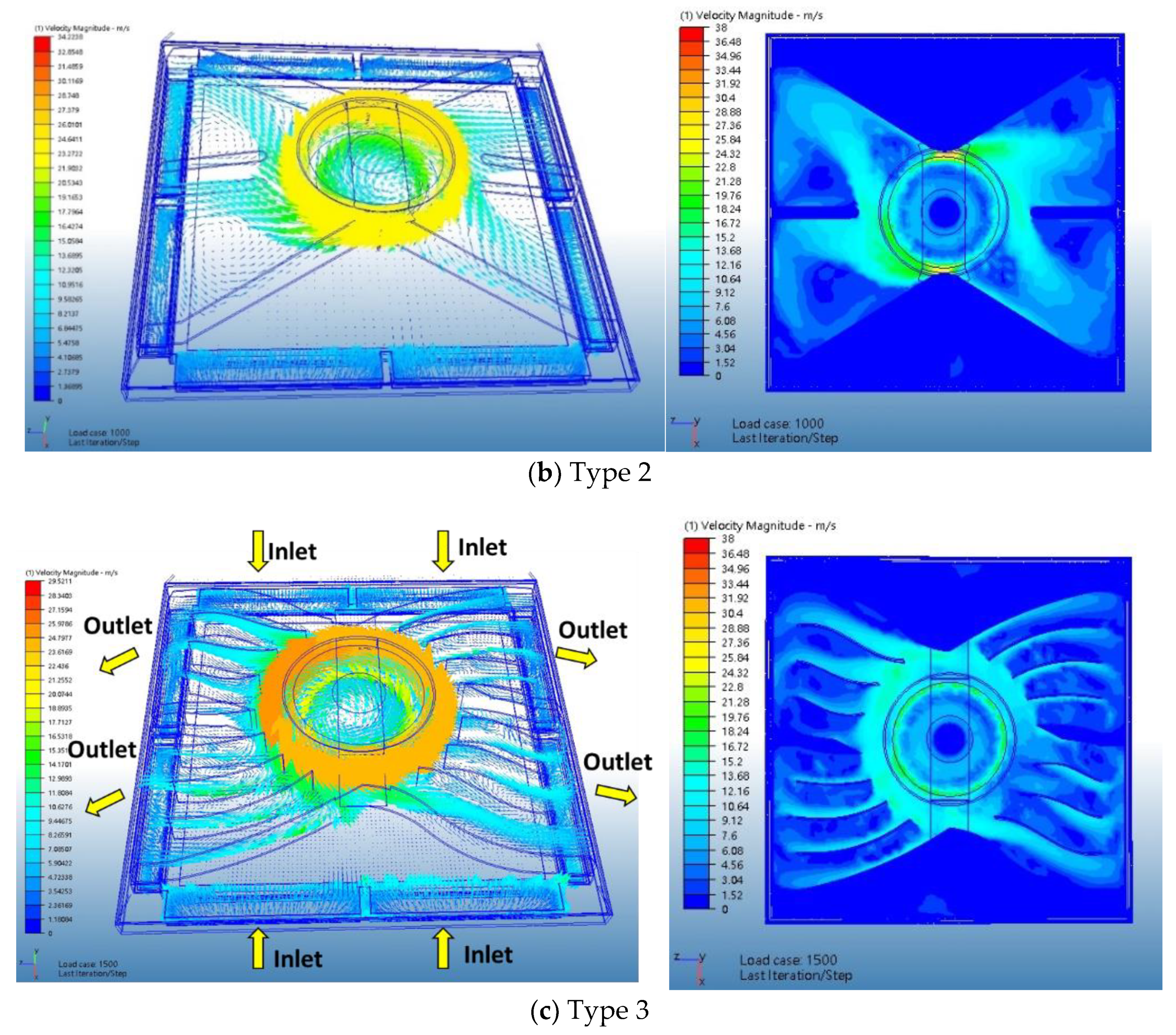
3.1. Velocity Distribution in the Flow Channel (Z-Plane)
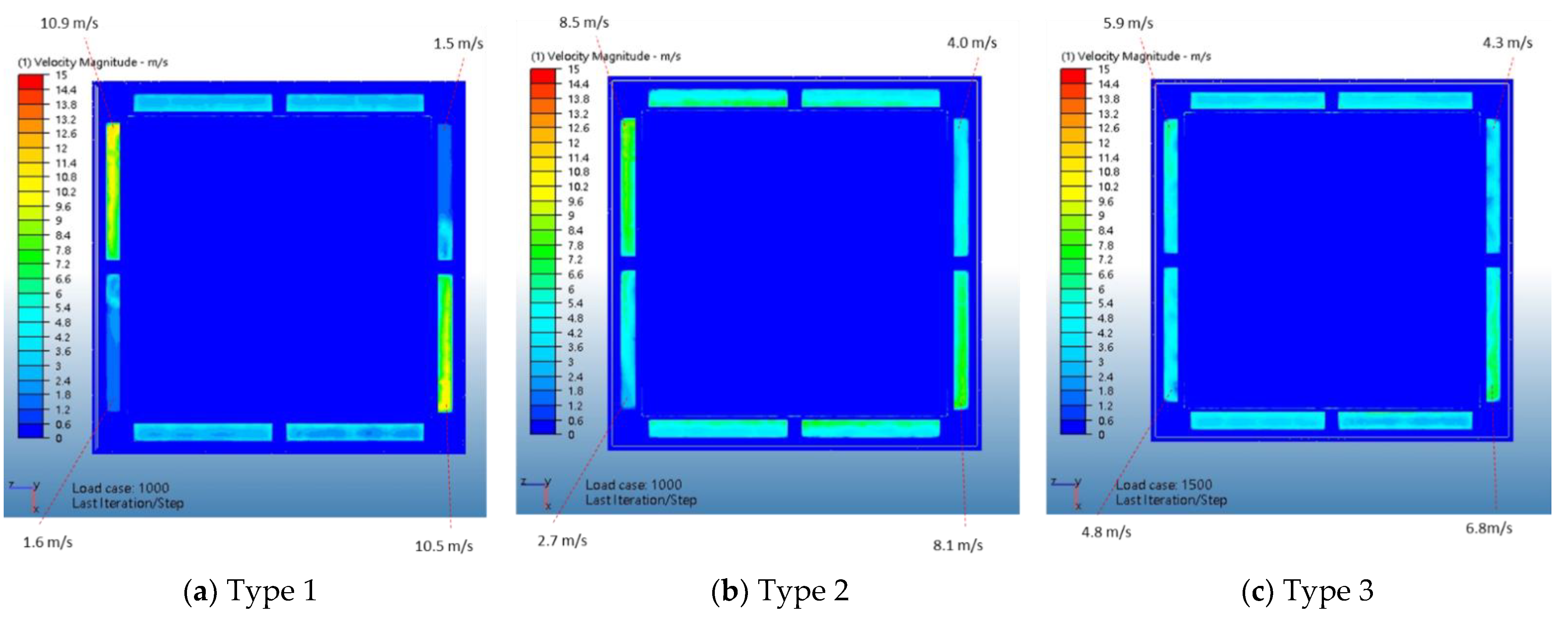
3.2. Inlet/Outlet Velocity Distributions
3.3. Lamp Module Operation Point
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kenarkoohi, A.; Noorimotlagh, Z.; Falahi, S.; Amarloei, A.; Mirzaee, S.A.; Pakzad, I. Hospital indoor air quality monitoring for the detection of SARS-CoV-2 (COVID-19) virus. Sci. Total Environ. 2020, 748, 141324. [Google Scholar] [CrossRef]
- Masoumbeigi, H.; Ghanizadeh, G.; Yousefi Arfaei, R.; Heydari, S.; Goodarzi, H.; Dorostkar Sari, R. Investigation of hospital indoor air quality for the presence of SARS-Cov-2. J. Environ. Health Sci. Eng. 2020, 18, 1259–1263. [Google Scholar] [CrossRef]
- Babaoglu, U.T.; Milletli Sezgin, F.; Yag, F. Sick building symptoms among hospital workers associated with indoor air quality and personal factors. Indoor Built Environ. 2019, 29, 645–655. [Google Scholar] [CrossRef]
- Veysi, R.; Heibati, B.; Jahangiri, M.; Kumar, P.; Latif, M.T.; Karimi, A. Indoor air quality-induced respiratory symptoms of a hospital staff in Iran. Environ. Monit. Assess. 2019, 191, 50. [Google Scholar] [CrossRef] [PubMed]
- Cabo Verde, S.; Almeida, S.M.; Matos, J.; Guerreiro, D.; Meneses, M.; Faria, T. Microbiological assessment of indoor air quality at different hospital sites. Res. Microbiol. 2015, 166, 557–563. [Google Scholar] [CrossRef]
- Jung, C.-C.; Wu, P.-C.; Tseng, C.-H.; Su, H.-J. Indoor air quality varies with ventilation types and working areas in hospitals. Build. Environ. 2015, 85, 190–195. [Google Scholar] [CrossRef]
- Baures, E.; Blanchard, O.; Mercier, F.; Surget, E.; Canna, P.; Rivier, A.; Gangneux, J.-P.; Florentin, A. Indoor air quality in two French hospitals: Measurement of chemical and microbiological contaminants. Sci. Total Environ. 2018, 642, 168–179. [Google Scholar] [CrossRef] [PubMed]
- Chamseddinea, A.; Alameddinea, I.; Hatzopouloub, M.; El-Fadela, M. Seasonal variation of air quality in hospitals with indoor–outdoor correlations. Built Environ. 2019, 148, 689–700. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Wang, H.; Wen, W. Numerical Simulation on a Horizontal Airflow for Airborne Particles Control in Hospital Operating Room. Built Environ. 2009, 44, 2284–2289. [Google Scholar] [CrossRef]
- Vijayan, V.K.; Paramesh, H.; Salvi, S.S.; Dalal, A.A. Enhancing indoor air quality: The air filter advantage. Lung India 2016, 33, 705. [Google Scholar] [CrossRef] [PubMed]
- Bache, S.E.; Maclean, M.; Gettinby, G.; Anderson, J.G.; MacGregor, S.J.; Taggart, I. Universal decontamination of hospital surfaces in an occupied inpatient room with a continuous 405 nm light source. J. Hosp. Infect. 2018, 98, 67–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saini, J.; Dutta, M.; Marques, G. Indoor Air Quality Monitoring Systems Based on Internet of Things: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 4942. [Google Scholar] [CrossRef] [PubMed]
- Karuchit, S.; Warissarangkul, W. Optimum Indoor Air Uv Germicidal Irradiation System for Application in Community Hospitals. Suranaree J. Sci. Technol. 2016, 23, 251–260. [Google Scholar]
- Zhou, Q.; Qian, H.; Liu, L. Numerical Investigation of Airborne Infection in Naturally Ventilated Hospital Wards With Central-Corridor Type. Indoor Built Environ. 2016, 27, 59–69. [Google Scholar] [CrossRef]
- Schiestel, R. Modeling and Simulation of Turbulent Flows; ISTE Ltd and John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2008; pp. 293–327. [Google Scholar]
- San, J. SW175HA2-72 Product Specification Approval Sheet; SAN JU Electric Machinery CO., LTD.: San Ju, China, 2011; pp. 1–4. [Google Scholar]
- AIRREX. AR103 Fiberglass Mat Panel Filter; AIRREX CO., LTD.: Changzhou, China, 2018; pp. 1–2. [Google Scholar]
- Kim, J.; Jang, M.; Choi, K.; Kim, K. Perception of indoor air quality (IAQ) by workers in underground shopping centers in relation to sick-building syndrome (SBS) and store type: A cross-sectional study in Korea. BMC Public Health 2019, 19, 632–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Item | Unit | Air | Plastic |
|---|---|---|---|
| Density | kg/m3 | 1.2047 | 432.54 |
| Viscosity | Pa-s | 1.817 × 10−5 | — |
| Conductivity | W/m-K | 0.02563 | 0.259843 |
| Specific Heat | J/kg-K | 1004 | 837 |
| k-ε Model | Constant | Value | |
| 0.09 | |||
| 1.44 | |||
| 1.92 | |||
| 1.0 | |||
| Boundary conditions | Types 1, 2, and 3 | inlet | Pressure 0 Pa (Gage) |
| outlet | |||
| Mesh conditions (number of nodes and elements) | Type 1 | Fluid | Nodes: 558,526; Elements: 1,618,093 |
| Solid | Nodes: 39,475; Elements: 484,726 | ||
| Type 2 | Fluid | Nodes: 355,004; Elements: 1,060,911 | |
| Solid | Nodes: 28,135; Elements: 304,958 | ||
| Type 3 | Fluid | Nodes: 472,322; Elements: 1,520,467 | |
| Solid | Nodes: 31,239; Elements: 353,267 | ||
| Item | Type 1 | Type 2 | Type 3 | |
|---|---|---|---|---|
| Inlet | Inlet 1 | 64 | 87.3 | 94.8 |
| Inlet 2 | 63.7 | 87.3 | 93.5 | |
| Inlet 3 | 62.1 | 86.9 | 95.5 | |
| Inlet 4 | 62.1 | 86.8 | 92.5 | |
| Sum | 251.9 | 348.3 | 376.3 | |
| Increase rate | 100% | 138.3% | 149.4% | |
| Outlet | Outlet 1 | 135 | 50 | 98.7 |
| Outlet 2 | −10.4 | 116 | 86.4 | |
| Outlet 3 | 135.5 | 68.5 | 97.5 | |
| Outlet 4 | −10.8 | 110.1 | 85.9 | |
| Sum | 249.3 | 344.6 | 368.5 | |
| Increase rate | 100% | 138.2% | 147.8% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.-S. Enhancing Air Quality for Embedded Hospital Germicidal Lamps. Sustainability 2021, 13, 2389. https://doi.org/10.3390/su13042389
Chen J-S. Enhancing Air Quality for Embedded Hospital Germicidal Lamps. Sustainability. 2021; 13(4):2389. https://doi.org/10.3390/su13042389
Chicago/Turabian StyleChen, Jung-Shun. 2021. "Enhancing Air Quality for Embedded Hospital Germicidal Lamps" Sustainability 13, no. 4: 2389. https://doi.org/10.3390/su13042389
APA StyleChen, J. -S. (2021). Enhancing Air Quality for Embedded Hospital Germicidal Lamps. Sustainability, 13(4), 2389. https://doi.org/10.3390/su13042389