
Highlighting the Role of Universally Available and Innate Immune Cell Counts in Acute Ischemic Stroke: A Scoping Review

 ,
, 

Abstract
:1. Introduction
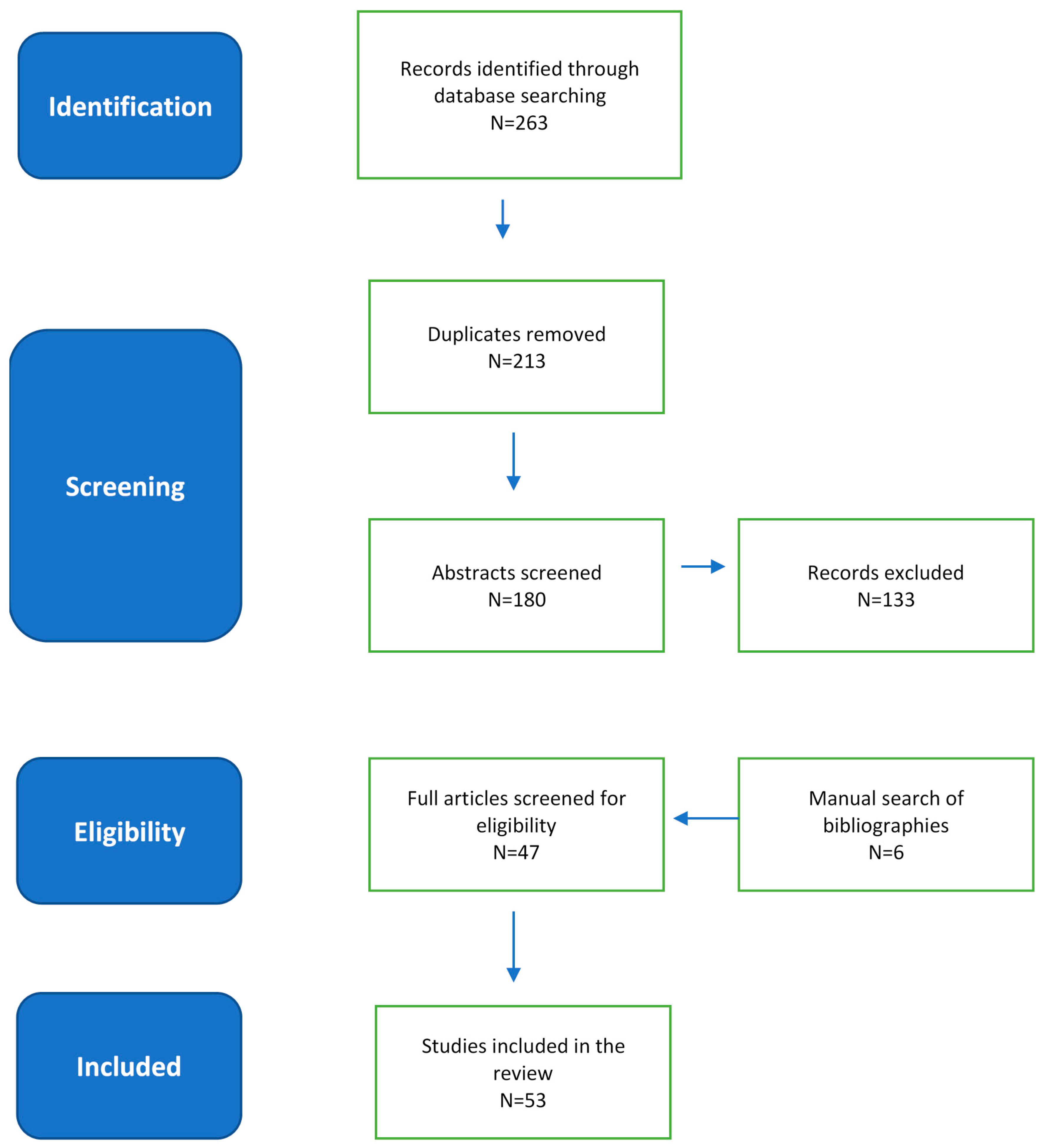
2. Methodology
3. Results
4. Discussion
4.1. The Role of NLR in Acute Ischemic Stroke
4.2. NLR and Its Role in Predisposition to Acute Ischemic Stroke
4.3. NLR and Its Role in Post-Stroke Complications
4.3.1. Stroke Associated Pneumonia
4.3.2. Post-Stroke Delirium
4.3.3. Post-Stroke Depression
5. Future Potential Therapeutic Opportunities
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wijeratne, T. Interview with WFN President on World Health Assembly Endorsement of Resolutions on Epilepsy and Neurological Disorders; World Federation of Neurology: Brussel, Belgium, 2020; Available online: https://wfneurology.org/news/wfn-news/2020-11-15-wfn (accessed on 2 April 2021).
- Jakovljevic, M.; Sugahara, T.; Timofeyev, Y.; Rancic, N. Predictors of (in)efficiencies of Healthcare Expenditure Among the Leading Asian Economies—Comparison of OECD and Non-OECD Nations. Risk Manag. Healthc. 2020, 13, 2261–2280. [Google Scholar] [CrossRef]
- Feigin, V.L.; Abajobir, A.A.; Abate, K.H.; Abd-Allah, F.; Abdulle, A.M.; Abera, S.F.; Abyu, G.Y.; Ahmed, M.B.; Aichour, A.N.; Aichour, I.; et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2017, 388, 1990–2015. [Google Scholar]
- Feigin, V.L.; Nichols, E.; Alam, T.; Bannick, M.S.; Beghi, E.; Blake, N.; Culpepper, W.J.; Dorsey, E.R.; Elbaz, A.; Ellenbogen, R.G.; et al. Global, regional, and national burden of neurological disorders, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459–480. [Google Scholar] [CrossRef] [Green Version]
- Feigin, V.L.; Norrving, B.; Mensah, G.A. Global Burden of Stroke. Circ. Res. 2017, 120, 439–448. [Google Scholar] [CrossRef]
- Jakovljevic, M.; Potapchik, E.; Popovich, L.; Barik, D.; Getzen, T.E. Evolving Health Expenditure Landscape of the BRICS Nations and Projections to 2025. Health Econ. 2016, 26, 844–852. [Google Scholar] [CrossRef]
- Jakovljevj, M. The Key Role of the Leading Emerging Bric Markets in the Future of Global Health Care. Serb. J. Exp. Clin. Res. 2014, 15, 139–143. [Google Scholar] [CrossRef]
- Jakovljevic, M.; Timofeyev, Y.; Ranabhat, C.L.; Fernandes, P.O.; Teixeira, J.P.; Rancic, N.; Reshetnikov, V. Real GDP growth rates and healthcare spending—comparison between the G7 and the EM7 countries. Glob. Health 2020, 16, 1–13. [Google Scholar] [CrossRef]
- Feigin, V.L.; Nguyen, G.; Cercy, K.; Johnson, C.O.; Alam, T.; Parmar, P.G.; Abajobir, A.A.; Abate, K.H.; Abd-Allah, F.; Abejie, A.N.; et al. The GBD 2016 Lifetime Risk of Stroke Collaborators. Global, Regional, and Country-Specific Lifetime Risks of Stroke, 1990 and 2016. N. Engl. J. Med. 2018, 379, 2429–2437. [Google Scholar]
- Gao, M.M.; Wang, J.; Saposnik, G. The Art and Science of Stroke Outcome Prognostication. Stroke 2020, 51, 1358–1360. [Google Scholar] [CrossRef] [PubMed]
- Amruta, N.; Rahman, A.A.; Pinteaux, E.; Bix, G. Neuroinflammation and fibrosis in stroke: The good, the bad and the ugly. J. Neuroimmunol. 2020, 346, 577318. [Google Scholar] [CrossRef]
- Anrather, J.; Iadecola, C. Inflammation and Stroke: An Overview. Neurotherapeutics 2016, 13, 661–670. [Google Scholar] [CrossRef]
- Chamorro, Á. Role of Inflammation in Stroke and Atherothrombosis. Cerebrovasc. Dis. 2004, 17, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Iadecola, C.; Anrather, J. The immunology of stroke: From mechanisms to translation. Nat. Med. 2011, 17, 796–808. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.A.; Crewther, S.G.; Howells, D.W.; Wijeratne, T.; Ma, H.; Hankey, G.J.; Davis, S.; Donnan, G.A.; Carey, L.M. Acute Routine Leukocyte and Neutrophil Counts Are Predictive of Poststroke Recovery at 3 and 12 Months Poststroke: An Exploratory Study. Neurorehabilit. Neural Repair 2020, 34, 844–855. [Google Scholar] [CrossRef]
- Song, S.-Y.; Zhao, X.-X.; Rajah, G.; Hua, C.; Kang, R.-J.; Han, Y.-P.; Ding, Y.-C.; Meng, R. Clinical Significance of Baseline Neutrophil-to-Lymphocyte Ratio in Patients With Ischemic Stroke or Hemorrhagic Stroke: An Updated Meta-Analysis. Front. Neurol. 2019, 10, 1032. [Google Scholar] [CrossRef]
- Wijeratne, T.; Menon, R.; Sales, C.; Karimi, L.; Crewther, S. Carotid artery stenosis and inflammatory biomarkers: The role of inflammation-induced immunological responses affecting the vascular systems. Ann. Transl. Med. 2020, 8, 1276. [Google Scholar] [CrossRef]
- Jakovljevic, M.; Matter-Walstra, K.; Sugahara, T.; Sharma, T.; Reshetnikov, V.; Merrick, J.; Yamada, T.; Youngkong, S.; Rovira, J. Cost-effectiveness and resource allocation (CERA) 18 years of evolution: Maturity of adulthood and promise beyond tomorrow. Cost Eff. Resour. Alloc. 2020, 18, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-C.; Ko, H.-J.; Liu, W.-S.; Hung, C.-L.; Hu, K.-C.; Yu, L.-Y.; Shih, S.-C. Neutrophil-to-lymphocyte ratio as a predictive marker of metabolic syndrome. Medicine 2019, 98, e17537. [Google Scholar] [CrossRef]
- Wang, L.; Song, Q.; Wang, C.; Wu, S.; Deng, L.; Li, Y.; Zheng, L.; Liu, M. Neutrophil to lymphocyte ratio predicts poor outcomes after acute ischemic stroke: A cohort study and systematic review. J. Neurol. Sci. 2019, 406, 116445. [Google Scholar] [CrossRef]
- Fan, L.; Gui, L.; Chai, E.-Q.; Wei, C.-J. Routine hematological parameters are associated with short- and long-term prognosis of patients with ischemic stroke. J. Clin. Lab. Anal. 2018, 32, e22244. [Google Scholar] [CrossRef] [Green Version]
- Świtońska, M.; Piekuś-Słomka, N.; Słomka, A.; Sokal, P.; Żekanowska, E.; Lattanzi, S. Neutrophil-to-Lymphocyte Ratio and Symptomatic Hemorrhagic Transformation in Ischemic Stroke Patients Undergoing Revascularization. Brain Sci. 2020, 10, 771. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.D.; Spears, C.; Cummings, C.; Vangilder, R.L.; Stinehart, K.R.; Gutmann, L.; Domico, J.; Culp, S.; Carpenter, J.; Rai, A.; et al. Admission neutrophil–lymphocyte ratio predicts 90 day outcome after endovascular stroke therapy. J. NeuroInterv. Surg. 2014, 6, 578–583. [Google Scholar] [CrossRef] [PubMed]
- Giede-Jeppe, A.; Madžar, D.; Sembill, J.A.; Sprügel, M.I.; Atay, S.; Hoelter, P.; Lücking, H.; Huttner, H.B.; Bobinger, T. Increased Neutrophil-to-Lymphocyte Ratio is Associated with Unfavorable Functional Outcome in Acute Ischemic Stroke. Neurocrit. Care 2020, 33, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Kocaturk, O.; Besli, F.; Gungoren, F.; Kocaturk, M.; Tanriverdi, Z. The relationship among neutrophil to lymphocyte ratio, stroke territory, and 3-month mortality in patients with acute ischemic stroke. Neurol. Sci. 2018, 40, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.; Jeong, I.; An, G.; Woo, K.; Kim, K.; Kim, J.; Cha, J.; Han, J. Early prediction of severity in acute ischemic stroke and transient ischemic attack using platelet parameters and neutrophil-to-lymphocyte ratio. J. Clin. Lab. Anal. 2018, 33, e22714. [Google Scholar] [CrossRef] [Green Version]
- Guo, Z.; Yu, S.; Xiao, L.; Chen, X.; Ye, R.; Zheng, P.; Dai, Q.; Sun, W.; Zhou, C.; Wang, S.; et al. Dynamic change of neutrophil to lymphocyte ratio and hemorrhagic transformation after thrombolysis in stroke. J. Neuroinflamm. 2016, 13, 199. [Google Scholar] [CrossRef] [Green Version]
- Maestrini, I.; Strbian, D.; Gautier, S.; Haapaniemi, E.; Moulin, S.; Sairanen, T.; Dequatre-Ponchelle, N.; Sibolt, G.; Cordonnier, C.; Melkas, S.; et al. Higher neutrophil counts before thrombolysis for cerebral ischemia predict worse outcomes. Neurology 2015, 85, 1408–1416. [Google Scholar] [CrossRef] [Green Version]
- Pikija, S.; Sztriha, L.K.; Killer-Oberpfalzer, M.; Weymayr, F.; Hecker, C.; Ramesmayer, C.; Hauer, L.; Sellner, J. Neutrophil to lymphocyte ratio predicts intracranial hemorrhage after endovascular thrombectomy in acute ischemic stroke. J. Neuroinflamm. 2018, 15, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Zhang, R.; Wu, X.; Hu, W.; Zhao, L.; Zhao, S.; Zhang, J.; Chu, Z.; Xu, Y. Neutrophil-to-lymphocyte ratio predicts hemorrhagic transformation in ischemic stroke: A meta-analysis. Brain Behav. 2019, 9, e01382. [Google Scholar] [CrossRef]
- Xue, J.; Huang, W.; Chen, X.; Li, Q.; Cai, Z.; Yu, T.; Shao, B. Neutrophil-to-Lymphocyte Ratio Is a Prognostic Marker in Acute Ischemic Stroke. J. Stroke Cerebrovasc. Dis. 2017, 26, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Suh, B.; Shin, D.W.; Kwon, H.-M.; Yun, J.M.; Yang, H.-K.; Ahn, E.; Lee, H.; Park, J.H.; Cho, B. Elevated neutrophil to lymphocyte ratio and ischemic stroke risk in generally healthy adults. PLoS ONE 2017, 12, e0183706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyun, S.; Kwon, S.; Cho, S.; Park, S.; Jung, W.; Moon, S.; Park, J.; Ko, C.; Cho, K. Can the Neutrophil-to-Lymphocyte Ratio Appropriately Predict Carotid Artery Stenosis in Patients with Ischemic Stroke?—A Retrospective Study. J. Stroke Cerebrovasc. Dis. 2015, 24, 2646–2651. [Google Scholar] [CrossRef]
- Jiang, H.; Zhang, J.; Wu, J.; Wei, G.; He, Y.; Gao, X. Neutrophil-to-Lymphocyte Ratio Correlates with Severity of Extracranial Carotid Stenosis—A Study Using Digital Subtraction Angiography. J. Stroke Cerebrovasc. Dis. 2017, 26, 1182–1190. [Google Scholar] [CrossRef] [PubMed]
- Zhou, S.; Cai, B.; Zhang, Y.; Wang, L.; Liu, X.; Xu, G. The Relationship between Neutrophil-to-Lymphocyte Ratio and Aortic Arch Calcification in Ischemic Stroke Patients. J. Stroke Cerebrovasc. Dis. 2017, 26, 1228–1232. [Google Scholar] [CrossRef]
- Nam, K.-W.; Kim, T.J.; Kim, C.K.; Mo, H.; Jeong, H.-Y.; Kang, M.K.; Han, M.-K.; Ko, S.-B.; Yoon, B.-W. Temporal changes in the neutrophil to lymphocyte ratio and the neurological progression in cryptogenic stroke with active cancer. PLoS ONE 2018, 13, e0194286. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Zhao, Q.; Jiang, Y.; Liu, N.; Liu, Q.; Shi, F.-D.; Hao, J.; Xu, Y.; Lo, E.H.; Wang, X. Augmented Brain Infiltration and Activation of Leukocytes After Cerebral Ischemia in Type 2 Diabetic Mice. Front. Immunol. 2019, 10, 2394. [Google Scholar] [CrossRef]
- Semerano, A.; Laredo, C.; Zhao, Y.; Rudilosso, S.; Renú, A.; Llull, L.; Amaro, S.; Obach, V.; Planas, A.M.; Urra, X.; et al. Leukocytes, Collateral Circulation, and Reperfusion in Ischemic Stroke Patients Treated with Mechanical Thrombectomy. Stroke 2019, 50, 3456–3464. [Google Scholar] [CrossRef]
- Semerano, A.; Strambo, D.; Martino, G.; Comi, G.; Filippi, M.; Roveri, L.; Bacigaluppi, M. Leukocyte Counts and Ratios Are Predictive of Stroke Outcome and Hemorrhagic Complications Independently of Infections. Front. Neurol. 2020, 11, 201. [Google Scholar] [CrossRef] [PubMed]
- Povroznik, J.M.; Engler-Chiurazzi, E.B.; Nanavati, T.; Pergami, P. Absolute lymphocyte and neutrophil counts in neonatal ischemic brain injury. SAGE Open Med. 2018, 6, 2050312117752613. [Google Scholar] [CrossRef] [Green Version]
- Guarner, V.; Rubio-Ruiz, M.E. Low-grade systemic inflammation connects aging, metabolic syndrome and cardiovascular disease. Interdiscip. Top. Gerontol. 2015, 40, 99–106. [Google Scholar]
- Saliba, W.; Barnett-Griness, O.; Elias, M.; Rennert, G. Neutrophil to lymphocyte ratio and risk of a first episode of stroke in patients with atrial fibrillation: A cohort study. J. Thromb. Haemost. 2015, 13, 1971–1979. [Google Scholar] [CrossRef]
- Min, K.; Kwon, S.; Cho, S.-Y.; Choi, W.J.; Park, S.-U.; Jung, W.-S.; Moon, S.-K.; Park, J.-M.; Ko, C.-N.; Cho, K.-H. Atrial Fibrillation is Strongly Associated with the Neutrophil to Lymphocyte Ratio in Acute Ischemic Stroke Patients: A Retrospective Study. J. Clin. Lab. Anal. 2016, 31, e22041. [Google Scholar] [CrossRef] [PubMed]
- Duman, T.T.; Aktas, G.; Atak, B.M.; Kocak, M.Z.; Erkus, E.; Savli, H. Neutrophil to lymphocyte ratio as an indicative of diabetic control level in type 2 diabetes mellitus. Afr. Health Sci. 2019, 19, 1602–1606. [Google Scholar] [CrossRef] [PubMed]
- Yalcin, M.; Aparci, M.; Uz, O.; Isilak, Z.; Balta, S.; Dogan, M.; Kardesoglu, E.; Uzun, M. Neutrophil–Lymphocyte Ratio May Predict Left Atrial Thrombus in Patients With Nonvalvular Atrial Fibrillation. Clin. Appl. Thromb. 2013, 21, 166–171. [Google Scholar] [CrossRef]
- Calvo, D.; Filgueiras-Rama, D.; Jalife, J. Mechanisms and Drug Development in Atrial Fibrillation. Pharmacol. Rev. 2018, 70, 505–525. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Zhang, Y.; Ma, L.; Niu, X.; Chang, J. Risk of stroke-associated pneumonia during hospitalization: Predictive ability of combined A2DS2 score and hyperglycemia. BMC Neurol. 2019, 19, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Nam, K.-W.; Kim, T.J.; Lee, J.S.; Kwon, H.-M.; Lee, Y.-S.; Ko, S.-B.; Yoon, B.-W. High Neutrophil-to-Lymphocyte Ratio Predicts Stroke-Associated Pneumonia. Stroke 2018, 49, 1886–1892. [Google Scholar] [CrossRef]
- Wang, L.; Guo, W.; Wang, C.; Yang, X.; Hao, Z.; Wu, S.; Zhang, S.; Wu, B.; Liu, M. Dynamic change of neutrophil to lymphocyte ratios and infection in patients with acute ischemic stroke. Curr. Neurovascular Res. 2020, 17, 1–17. [Google Scholar] [CrossRef]
- Feng, H.-X.; Cheng, Y.; Zhu, W.; Jiang, L.-L.; Dong, X.-F.; Gui, Q.; Wu, G.-H.; Xu, Q.-R.; Shen, M.-Q.; Cheng, Q.-Z. T-lymphocyte subsets as a predictive biomarker for stroke-associated pneumonia. Am. J. Transl. Res. 2018, 10, 4367–4375. [Google Scholar]
- Ruhnau, J.; Schulze, J.; Dressel, A.; Vogelgesang, A. Thrombosis, Neuroinflammation, and Poststroke Infection: The Multifaceted Role of Neutrophils in Stroke. J. Immunol. Res. 2017, 2017, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Enlimomab Acute Stroke Trial Investigators. Use of anti-ICAM-1 therapy in ischemic stroke: Results of the Enlimomab Acute Stroke Trial. Neurology 2001, 57, 1428–1434. [Google Scholar] [CrossRef]
- Oldenbeuving, A.W.; De Kort, P.L.M.; Jansen, B.P.W.; Roks, G.; Kappelle, L.J. Delirium in Acute Stroke: A Review. Int. J. Stroke 2007, 2, 270–275. [Google Scholar] [CrossRef]
- Shi, Q.; Presutti, R.; Selchen, D.; Saposnik, G. Response to Letter Regarding Article, “Delirium in Acute Stroke: A Systematic Review and Meta-Analysis”. Stroke 2012, 43, e65. [Google Scholar] [CrossRef] [Green Version]
- Egberts, A.; Mattace-Raso, F.U. Increased neutrophil-lymphocyte ratio in delirium: A pilot study. Clin. Interv. Aging 2017, 12, 1115–1121. [Google Scholar] [CrossRef] [Green Version]
- Kotfis, K.; Bott-Olejnik, M.; Szylińska, A.; Rotter, I. Could Neutrophil-to-Lymphocyte Ratio (NLR) Serve as a Potential Marker for Delirium Prediction in Patients with Acute Ischemic Stroke? A Prospective Observational Study. J. Clin. Med. 2019, 8, 1075. [Google Scholar] [CrossRef] [Green Version]
- Kotfis, K.; Bott-Olejnik, M.; Szylińska, A.; Listewnik, M.; Rotter, I. Characteristics, Risk Factors and Outcome Of Early-Onset Delirium In Elderly Patients With First Ever Acute Ischemic Stroke—A Prospective Observational Cohort Study. Clin. Interv. Aging 2019, 14, 1771–1782. [Google Scholar] [CrossRef] [Green Version]
- Das, J.; Rajanikant, G.K. Post stroke depression: The sequelae of cerebral stroke. Neurosci. Biobehav. Rev. 2018, 90, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Bartoli, F.; Di Brita, C.; Crocamo, C.; Clerici, M.; Carrà, G. Early Post-stroke Depression and Mortality: Meta-Analysis and Meta-Regression. Front. Psychiatry 2018, 9, 530. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, F.; Villa, R.F. The Neurobiology of Depression: An Integrated Overview from Biological Theories to Clinical Evidence. Mol. Neurobiol. 2016, 54, 4847–4865. [Google Scholar] [CrossRef] [PubMed]
- Spalletta, G.; Bossù, P.; Ciaramella, A.; Bria, P.; Caltagirone, C.; Robinson, R.G. The etiology of poststroke depression: A review of the literature and a new hypothesis involving inflammatory cytokines. Mol. Psychiatry 2006, 11, 984–991. [Google Scholar] [CrossRef] [Green Version]
- Pascoe, M.C.; Crewther, S.G.; Carey, L.M.; Crewther, D.P. Inflammation and Depression: Why Poststroke Depression may be the Norm and Not the Exception. Int. J. Stroke 2011, 6, 128–135. [Google Scholar] [CrossRef]
- Grundy, R.I.; Rothwell, N.J.; Allan, S.M. Site-specific actions of interleukin-1 on excitotoxic cell death in the rat striatum. Brain Res. 2002, 926, 142–148. [Google Scholar] [CrossRef]
- Chen, H.; Luan, X.; Zhao, K.; Qiu, H.; Liu, Y.; Tu, X.; Tang, W.; He, J. The association between neutrophil-to-lymphocyte ratio and post-stroke depression. Clin. Chim. Acta 2018, 486, 298–302. [Google Scholar] [CrossRef]
- Lucke-Wold, A.N.; Regier, M.D.; Petrone, A.; Tennant, C.; Barr, T. Abstract TMP80: Relationship between Neutrophil/Lymphocyte Ratio and Post-stroke Depression. Stroke 2016, 47, ATMP80. [Google Scholar]
- Hu, J.; Zhou, W.; Zhou, Z.; Han, J.; Dong, W. Elevated neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios predict post-stroke depression with acute ischemic stroke. Exp. Ther. Med. 2020, 19, 2497–2504. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aydin Sunbul, E.; Sunbul, M.; Yanartas, O.; Cengiz, F.; Bozbay, M.; Sari, I.; Gulec, H. Increased Neutrophil/Lymphocyte Ratio in Patients with Depression is Correlated with the Severity of Depression and Cardiovascular Risk Factors. Psychiatry Investig. 2016, 13, 121–126. [Google Scholar] [CrossRef] [Green Version]
- Chamorro, A.; Planas, A.M. Inflammation-mediated damage as a potential therapeutic target in acute ischemic stroke. Ernst Schering Res. Found. Workshop 2004, 47, 185–204. [Google Scholar]
- Planas, A.M. Role of Immune Cells Migrating to the Ischemic Brain. Stroke 2018, 49, 2261–2267. [Google Scholar] [CrossRef]
- De Dios, E.; Rios-Navarro, C.; Perez-Sole, N.; Gavara, J.; Marcos-Garces, V.; Rodríguez, E.; Carratalá, A.; Forner, M.J.; Navarro, J.; Blasco, M.L.; et al. Similar Clinical Course and Significance of Circulating Innate and Adaptive Immune Cell Counts in STEMI and COVID-19. J. Clin. Med. 2020, 9, 3484. [Google Scholar] [CrossRef] [PubMed]
- Jakovljevic, M.; Lazarevic, M.; Milovanovic, O.; Kanjevac, T. The New and Old Europe: East-West Split in Pharmaceutical Spending. Front. Pharmacol. 2016, 7, 18. [Google Scholar] [CrossRef] [Green Version]
- Villa, A.; Vegeto, E.; Poletti, A.; Maggi, A. Estrogens, Neuroinflammation, and Neurodegeneration. Endocr. Rev. 2016, 37, 372–402. [Google Scholar] [CrossRef] [Green Version]
- Villa, R.F.; Ferrari, F.; Moretti, A. Post-stroke depression: Mechanisms and pharmacological treatment. Pharmacol. Ther. 2018, 184, 131–144. [Google Scholar] [CrossRef]
- Villanueva, C.; Kross, R.D.; Pérez-Astudillo, L. Free radicals and neuronal recovery from an ischemic penumbra: A review. In Free Radicals and Diseases; IntechOpen: London, UK, 2016. [Google Scholar]
- Köhler, O.; Benros, M.E.; Nordentoft, M.; Farkouh, M.E.; Iyengar, R.L.; Mors, O.; Krogh, J. Effect of Anti-inflammatory Treatment on Depression, Depressive Symptoms, and Adverse Effects: A Systematic Review and Meta-analysis of Randomized Clinical Trials. JAMA Psychiatry 2014, 71, 1381–1391. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, S.-H.; Hosseini, F.; Modabbernia, A.; Ashrafi, M.; Akhondzadeh, S. Effect of celecoxib add-on treatment on symptoms and serum IL-6 concentrations in patients with major depressive disorder: Randomized double-blind placebo-controlled study. J. Affect. Disord. 2012, 141, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Raison, C.L.; Rutherford, R.E.; Woolwine, B.J.; Shuo, C.; Schettler, P.; Drake, D.F.; Haroon, E.; Miller, A.H. A randomized controlled trial of the tumor necrosis factor antagonist infliximab for treatment-resistant depression: The role of baseline inflammatory biomarkers. JAMA Psychiatry 2013, 70, 31–41. [Google Scholar] [CrossRef]
- Chen, Y.-R.; Hsieh, F.-I.; Chang, C.-C.; Chi, N.-F.; Wu, H.-C.; Chiou, H.-Y. Effect on Risk of Stroke and Acute Myocardial Infarction of Nonselective Nonsteroidal Anti-Inflammatory Drugs in Patients with Rheumatoid Arthritis. Am. J. Cardiol. 2018, 121, 1271–1277. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| • Predicts length of hospitalization, cost, disability, and death among patients with AIS |
| • Correlated with the volume of infarct in anterior circulation |
| • Associated with more severe and disabling ischemic strokes |
| • Increased risk of hemorrhagic complications among patients receiving reperfusion therapy |
| • Higher risk of recurrent strokes |
| • Increases risk of stroke among patients with or without traditional cardiovascular risk factors |
| • Increased odds for post-stroke complications such as stroke-associated pneumonia, delirium, and post-stroke depression |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wijeratne, T.; Sales, C.; Menon, R.; Karimi, L.; Jakovljevic, M. Highlighting the Role of Universally Available and Innate Immune Cell Counts in Acute Ischemic Stroke: A Scoping Review. Sustainability 2021, 13, 4069. https://doi.org/10.3390/su13074069
Wijeratne T, Sales C, Menon R, Karimi L, Jakovljevic M. Highlighting the Role of Universally Available and Innate Immune Cell Counts in Acute Ischemic Stroke: A Scoping Review. Sustainability. 2021; 13(7):4069. https://doi.org/10.3390/su13074069
Chicago/Turabian StyleWijeratne, Tissa, Carmela Sales, Rohit Menon, Leila Karimi, and Mihajlo Jakovljevic. 2021. "Highlighting the Role of Universally Available and Innate Immune Cell Counts in Acute Ischemic Stroke: A Scoping Review" Sustainability 13, no. 7: 4069. https://doi.org/10.3390/su13074069
APA StyleWijeratne, T., Sales, C., Menon, R., Karimi, L., & Jakovljevic, M. (2021). Highlighting the Role of Universally Available and Innate Immune Cell Counts in Acute Ischemic Stroke: A Scoping Review. Sustainability, 13(7), 4069. https://doi.org/10.3390/su13074069