
Commercialization Potential of Six Selected Medicinal Plants Commonly Used for Childhood Diseases in South Africa: A Review

 ,
,  ,
, 

Abstract
:1. Introduction
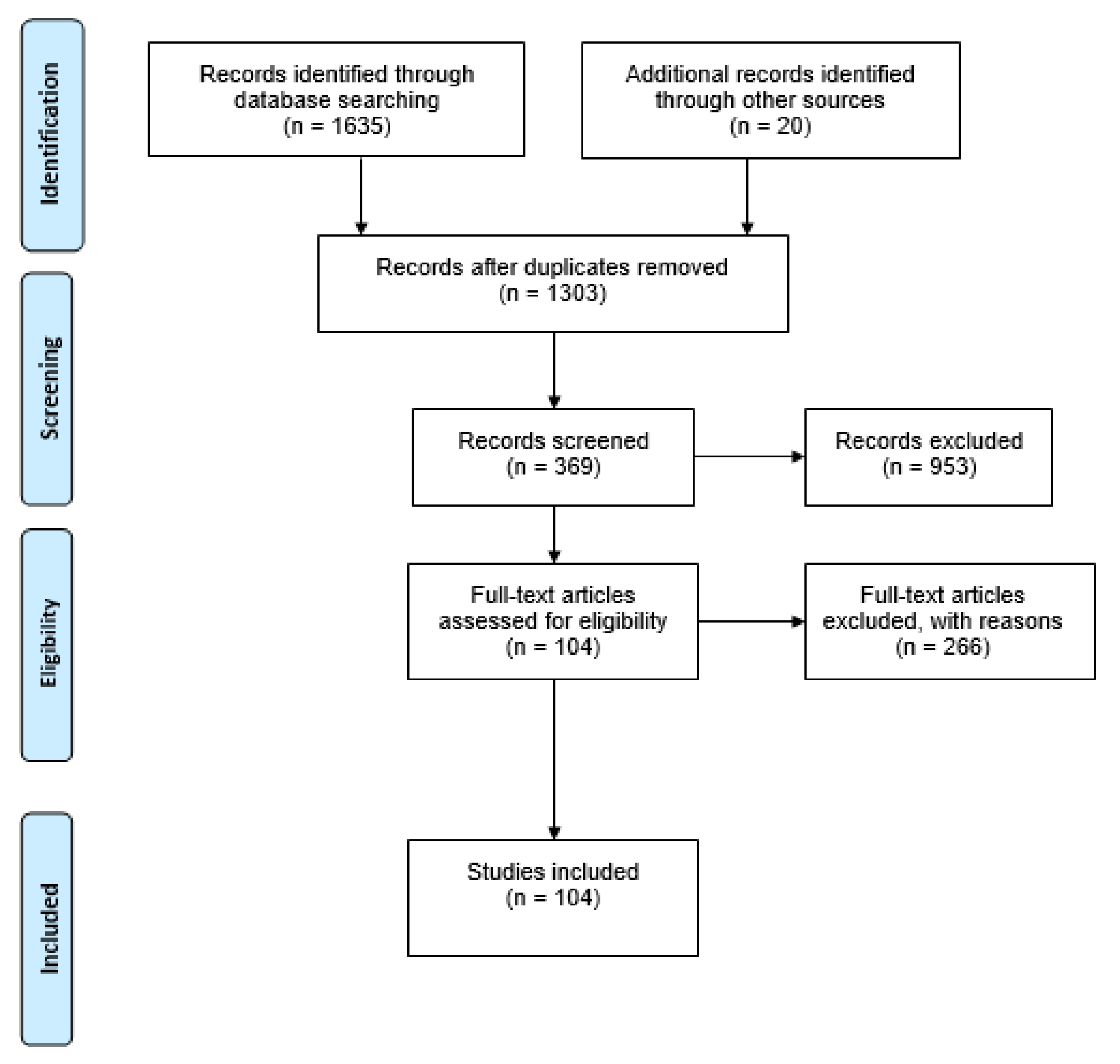
2. Methods
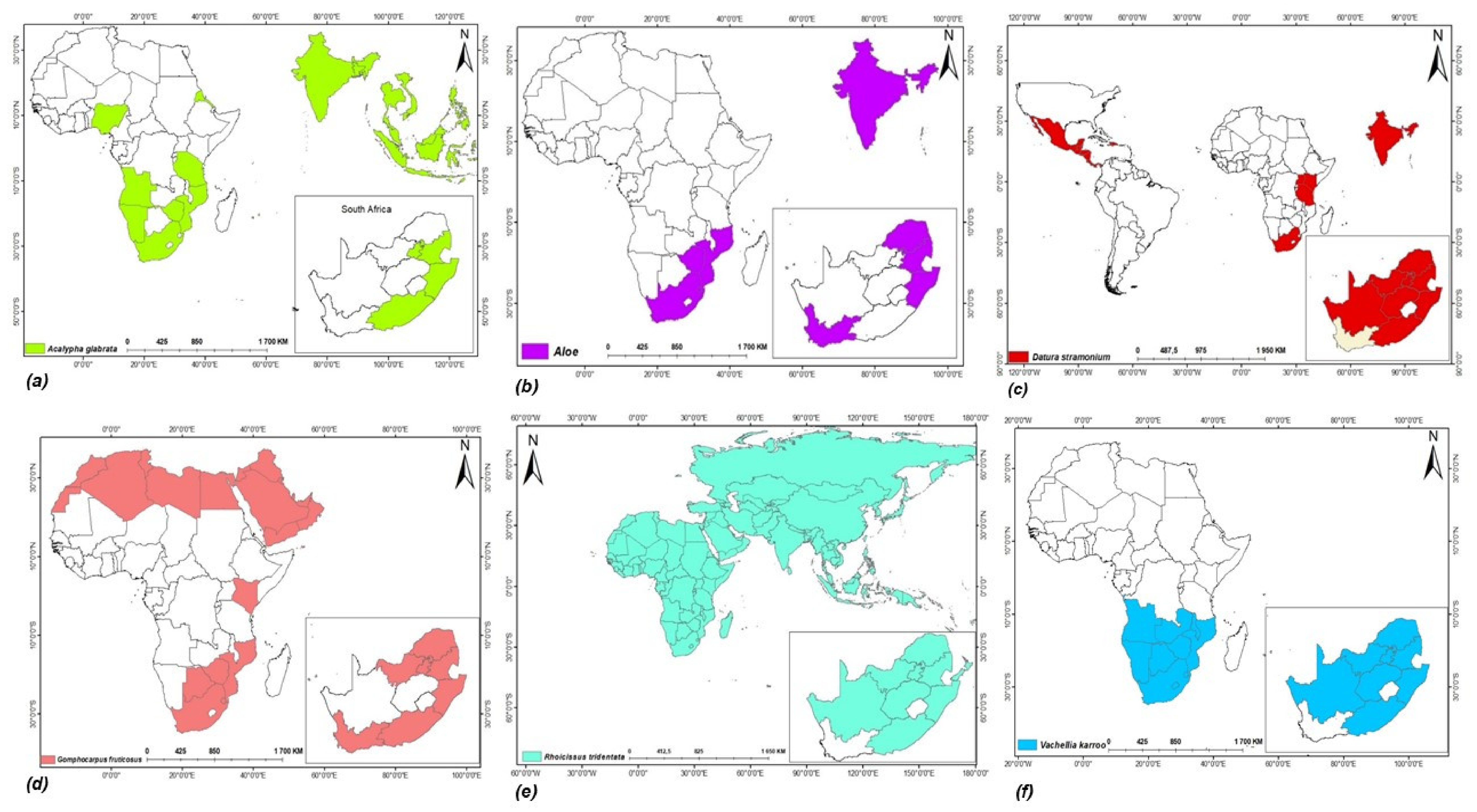
3. Distribution and Occurrence of the Selected Medicinal Plants
4. Ethnobotanical Uses of the Six Medicinal Plants
5. Benefits and Economic Prospects of Selected Medicinal Plants
6. Challenges to Unlocking Potential of Selected Medicinal Plants
6.1. Policy Integration and Medicinal Plants
6.2. Agro-Processing of Medicinal Plants
6.3. Commercialization of Medicinal Plants
7. Prospects of Unlocking the Potential of Selected Medicinal Plants
7.1. Promoting Collaborative Research and Sustainability
7.2. Technology Application and Product Development
7.3. Promoting a Useful Value Chain
7.4. Potential of the Selected Plants for Commercialization
8. Conclusions and Recommendations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- De Villiers, F.P.R.; Ledwaba, M.J.P. Traditional healers and paediatric care. S. Afr. Med. J. 2003, 2003, 664–665. [Google Scholar]
- Sen, S.; Chakraborty, R. Revival, modernization and integration of Indian traditional herbal medicine in clinical practice: Importance, challenges and future. J. Tradit. Complement. Med. 2017, 7, 234–244. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). World Health Organization Traditional Medicine Strategy 2014–2023; WHO: Geneva, Switzerland, 2013; pp. 1–78. [Google Scholar]
- Hutchings, A.; Scott, A.H.; Lewis, G.; Cunningham, A.B. Zulu Medicinal Plants: An Inventory; University of Natal Press: Pietermaritzburg, South Africa, 1996. [Google Scholar]
- Hulley, I.M.; Van Wyk, B.-E. Quantitative medicinal ethnobotany of Kannaland (Western Little Karoo, South Africa): Non-homogeneity amongst villages. S. Afr. J. Bot. 2019, 122, 225–265. [Google Scholar] [CrossRef]
- McGaw, L.J.; Famuyide, I.M.; Khunoana, E.T.; Aremu, A.O. Ethnoveterinary botanical medicine in South Africa: A review of research from the last decade (2009 to 2019). J. Ethnopharmacol. 2020, 257, 112864. [Google Scholar] [CrossRef] [PubMed]
- Semenya, S.; Potgieter, M.; Erasmus, L. Ethnobotanical survey of medicinal plants used by Bapedi healers to treat diabetes mellitus in the Limpopo Province, South Africa. J. Ethnopharmacol. 2012, 141, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Street, R.; Prinsloo, G. Commercially important medicinal plants of South Africa: A review. J. Chem. 2012, 2013, 205048. [Google Scholar] [CrossRef]
- Van Wyk, B.E. A review of commercially important African medicinal plants. J. Ethnopharmacol. 2015, 176, 118–134. [Google Scholar] [CrossRef]
- Omotayo, A.O.; Ndhlovu, P.T.; Tshwene, S.C.; Aremu, A.O. Utilization pattern of indigenous and naturalized plants among some selected rural households of North West Province, South Africa. Plants 2020, 9, 953. [Google Scholar] [CrossRef]
- Ajesh, T.P.; Abdulla Naseef, S.A.; Kumuthakalavalli, R. Ethnobotanical documentation of wild edible fruits used by Muthuvan Tribes of Idukki, Kerala- India. J. Pharm. Biol. Sci. 2012, 3, 479–487. [Google Scholar]
- Omotayo, A.O.; Aremu, O.A. Evaluation of factors influencing the inclusion of indigenous plants for food security among rural households in the North West Province of South Africa. Sustainability 2020, 12, 9562. [Google Scholar] [CrossRef]
- Mander, M.; Ntuli, L.; Diederichs, N.; Mavundla, K. Economics of the traditional medicine trade in South Africa care delivery. S. Afr. Health Rev. 2007, 2007, 189–196. [Google Scholar]
- Williams, V.L.; Witkowski, E.T.F.; Balkwill, K. Volume and financial value of species traded in the medicinal plant markets of Gauteng, South Africa. Int. J. Sustain. Dev. World Ecol. 2007, 14, 584–603. [Google Scholar] [CrossRef]
- Stats, S.A. Living Conditions of Households in South Africa; Statistics South Africa: Pretoria, South Africa, 2015; pp. 1–232. [Google Scholar]
- Masondo, N.A.; Makunga, N.P. Advancement of analytical techniques in some South African commercialized medicinal plants: Current and future perspectives. S. Afr. J. Bot. 2019, 126, 40–57. [Google Scholar] [CrossRef]
- Asong, J.A.; Ndhlovu, P.T.; Khosana, N.S.; Aremu, A.O.; Otang-Mbeng, W. Medicinal plants used for skin-related diseases among the Batswanas in Ngaka Modiri Molema District Municipality, South Africa. S. Afr. J. Bot. 2019, 126, 11–20. [Google Scholar] [CrossRef]
- Magwede, K.; Van Wyk, B.E.; Van Wyk, A.E. An inventory of Vhavenḓa useful plants. S. Afr. J. Bot. 2019, 122, 57–89. [Google Scholar] [CrossRef]
- Moffett, R.O. Basotho Medicinal Plants–Meriana ya Dimela Tsa Basotho; Sun Press: Stellenbosch, South Africa, 2016. [Google Scholar]
- Mhlongo, L.S.; Van Wyk, B.-E. Zulu medicinal ethnobotany: New records from the Amandawe area of KwaZulu-Natal, South Africa. S. Afr. J. Bot. 2019, 122, 266–290. [Google Scholar] [CrossRef]
- Botha, J.; Witkowski, E.T.F.; Shackleton, C.M. Market profiles and trade in medicinal plants in the Lowveld, South Africa. Environ. Conserv. 2004, 31, 38–46. [Google Scholar] [CrossRef] [Green Version]
- Ndhlovu, P.T.; Omotayo, A.O.; Otang-Mbeng, W.; Aremu, A.O. Ethnobotanical review of plants used for the management and treatment of childhood diseases and well-being in South Africa. S. Afr. J. Bot. 2021, 137, 197–215. [Google Scholar] [CrossRef]
- Van Wyk, B.-E. The potential of South African plants in the development of new food and beverage products. S. Afr. J. Bot. 2011, 77, 857–868. [Google Scholar] [CrossRef] [Green Version]
- UNICEF. Levels and Trends in Child Mortality: Report 2019. Estimates Developed by the UN Inter-Agency Group for Child Mortality Estimation; United Nation’s Children Fund: New York, NY, USA, 2019. [Google Scholar]
- Lake, L.; Shung-King, M.; Hendricks, M.; Heywood, M.; Nannan, N.; Laubscher, R.; Bradshaw, D.; Mathews, C.; Goga, A.; Ramraj, T.; et al. Prioritising child and adolescent health: A human rights imperative. S. Afr. Child Gauge 2019, 2, 31–62. [Google Scholar]
- Dold, A.P.; Cocks, M.L. The trade in medicinal plants in the Eastern Cape Province, South Africa. S. Afr. J. Sci. 2002, 98, 589–597. [Google Scholar]
- Moyo, M.; Aremu, A.O.; Van Staden, J. Medicinal plants: An invaluable, dwindling resource in sub-Saharan Africa. J. Ethnopharmacol. 2015, 174, 595–606. [Google Scholar] [CrossRef]
- Shamseer, L.; Moher, D.; Clarke, V.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, K.M.; the PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seebaluck, R.; Gurib-Fakim, A.; Mahomoodally, F. Medicinal plants from the genus Acalypha (Euphorbiaceae)–A review of their ethnopharmacology and phytochemistry. J. Ethnopharmacol. 2015, 159, 137–157. [Google Scholar] [CrossRef] [PubMed]
- Van Wyk, B.-E.; Van Oudtshoorn, B.; Gericke, N. Medicinal Plants of South Africa; Briza: Pretotia, South Africa, 1997. [Google Scholar]
- Grace, O.M.; Simmonds, M.S.J.; Smith, G.F.; Van Wyk, A.E. Documented utility and biocultural value of Aloe L. (Asphodelaceae): A Review. Econ. Bot. 2009, 63, 167–178. [Google Scholar] [CrossRef]
- Corredor-Prado, J.; Conti, D.D.; Sezerino, A.; Guerra, M.; Orth, A. Reproductive biology and absence of fruiting of Aloe saponaria (Aiton) Haw.(Xanthorrhoeaceae) outside its place of origin. Rev. Bras. Plantas Med. 2015, 17, 713–721. [Google Scholar] [CrossRef]
- Smith, G.; Figueiredo, E.; Klopper, R.; Crouch, N. Aloe maculata All. (Asphodelaceae) in the Free State Province, South Africa, and resurrection of ‘var. ficksburgensis’. Bradleya 2012, 30, 13–18. [Google Scholar] [CrossRef]
- Van Wyk, B.; Van Wyk, P. Field Guide to Trees of Southern Africa; Struik: Cape Town, South Africa, 1997. [Google Scholar]
- Gaire, B.P.; Subedi, L. A review on the pharmacological and toxicological aspects of Datura stramonium L. J. Integr. Med. 2013, 11, 73–79. [Google Scholar] [CrossRef] [Green Version]
- Soni, P.; Siddiqui, A.A.; Dwivedi, J.; Soni, V. Pharmacological properties of Datura stramonium L. as a potential medicinal tree: An overview. Asian Pac. J. Trop. Biomed. 2012, 2, 1002–1008. [Google Scholar] [CrossRef] [Green Version]
- Shagal, M.H.; Modibbo, U.U.; Liman, A.B. Pharmacological justification for the ethnomedical use of Datura stramonium stem-bark extract in treatment of diseases caused by some pathogenic bacteria. Int. Res. Pharm. Pharmacol. 2012, 2, 16–19. [Google Scholar]
- Watt, J.M.; Breyer Brandwijk, M. Medicinal and Poisonous Plants of Southern and Eastern Africa; E. & S. Livingstone Ltd.: Edinburgh, UK; London, UK, 1962. [Google Scholar]
- Van Wyk, B.-E.; Gericke, N. People’s Plants: A Guide to the Useful Plants of Southern Africa; Briza Publications: Pretoria, South Africa, 2000. [Google Scholar]
- Marzouk, A.M.; Osman, S.m.; Gohar, A.A. A newpregnane glycoside from Gomphocarpus fruticosus growing in Egypt. Nat. Prod. Res. 2016, 30, 1060–1067. [Google Scholar] [CrossRef]
- Chivandi, E.; Mukonowenzou, N.; Berliner, D. The coastal red-milkwood (Mimusops caffra) seed: Proximate, mineral, amino acid and fatty acid composition. S. Afr. J. Bot. 2016, 102, 137–141. [Google Scholar] [CrossRef]
- Urton, N.R.; Olivier, M.C.; Robertson, B.L. The taxonomy of the Rhoicissus tridentata (Vitaceae) complex in southern Africa. S. Afr. J. Bot. 1986, 52, 389–396. [Google Scholar] [CrossRef]
- Mukundi, M.J.; Mwaniki, N.E.; Ngugi, M.P.; Njagi, J.M.; Agyirifo, S.D.; Gathumbi, K.P.; Muchugi, N.A. In vivo anti-diabetic effects of aqueous leaf extracts of Rhoicissus tridentata in alloxan induced diabetic mice. J. Dev. Drugs 2015, 4. [Google Scholar] [CrossRef]
- Luckow, M.; Miller, J.T.; Murphy, D.J.; Livshultz, T. A phylogenetic analysis of the Mimosoideae (Leguminosae) based on chloroplast DNA sequence data. Adv. Legume Syst. Part 2003, 10, 197–220. [Google Scholar]
- Maroyi, A. Traditional use of medicinal plants in south-central Zimbabwe: Review and perspectives. J. Ethnobiol. Ethnomed. 2013, 9, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, C.L.; Barker, N.P. Species limits in Vachellia (Acacia) karroo (Mimosoideae: Leguminoseae): Evidence from automated ISSR DNA “fingerprinting”. S. Afr. J. Bot. 2012, 83, 36–43. [Google Scholar] [CrossRef] [Green Version]
- Van Wyk, B.-E.; Van Heerden, F.; Van Oudtshoorn, B. Poisonous Plants of South Africa; Briza: Pretoria, South Africa, 2005. [Google Scholar]
- Amoo, S.O.; Aremu, A.O.; Van Staden, J. Unraveling the medicinal potential of South African Aloe species. J. Ethnopharmacol. 2014, 153, 19–41. [Google Scholar] [CrossRef] [PubMed]
- Grace, O. Current perspectives on the economic botany of the genus Aloe L.(Xanthorrhoeaceae). S. Afr. J. Bot. 2011, 77, 980–987. [Google Scholar] [CrossRef] [Green Version]
- Nortje, J.M.; Van Wyk, B.E. Medicinal plants of the Kamiesberg, Namaqualand, South Africa. J. Ethnopharmacol. 2015, 171, 205–222. [Google Scholar] [CrossRef]
- Das, S.; Kumar, P.; Basu, S. Phytoconstituents and therapeutic potentials of Datura stramonium Linn. J. Drug Deliv. Ther. 2012, 2, 4–7. [Google Scholar] [CrossRef]
- Philander, A.L. An ethnobotany of Western Cape Rasta bush medicine. J. Ethnopharmacol. 2011, 138, 578–594. [Google Scholar] [CrossRef] [PubMed]
- Semenya, S.S.; Potgieter, M.J. Ethnobotanical survey of medicinal plants used by Bapedi traditional healers to treat erectile dysfunction in the Limpopo Province, South Africa. J. Med. Plants Res. 2013, 7, 349–357. [Google Scholar]
- Moichwanetse, B.I.; Ndhlovu, P.T.; Sedupane, G.; Aremu, A.O. Ethno-veterinary plants used for the treatment of retained placenta and associated diseases in cattle among Dinokana communities, North West Province, South Africa. S. Afr. J. Bot. 2020, 132, 108–116. [Google Scholar] [CrossRef]
- Omino, E.A.; Kokwaro, J.O. Ethnobotany of Apocynaceae species in Kenya. J. Ethnopharmacol. 1993, 40, 167–180. [Google Scholar] [CrossRef]
- Mabaleha, M.B.; Zietsman, P.C.; Wilhelm, A.; Bonnet, S.L. Ethnobotanical survey of medicinal plants used to treat mental illnesses in the Berea, Leribe, and Maseru Districts of Lesotho. Nat. Prod. Commun. 2019, 14, 1934578X19864215. [Google Scholar] [CrossRef] [Green Version]
- Arnold, H.-J.; Gulumian, M. Pharmacopoeia of traditional medicine in Venda. J. Ethnopharmacol. 1984, 12, 35–74. [Google Scholar] [CrossRef]
- Lin, J.; Opoku, A.; Geheeb-Keller, M.; Hutchings, A.; Terblanche, S.; Jäger, A.K.; Van Staden, J. Preliminary screening of some traditional zulu medicinal plants for anti-inflammatory and anti-microbial activities. J. Ethnopharmacol. 1999, 68, 267–274. [Google Scholar] [CrossRef]
- Van der Merwe, D.; Swan, G.E.; Botha, C.J. Use of ethnoveterinary medicinal plants in cattle by Setswana-speaking people in the Madikwe area of the North West Province of South Africa. J. S. Afr. Vet. Assoc. 2001, 72, 189–196. [Google Scholar] [CrossRef] [Green Version]
- Dold, A.P.; Cocks, M.L. Traditional veterinary medicine in the Alice district of the Eastern Cape Province, South Africa: Research in action. S. Afr. J. Sci. 2001, 97, 375–379. [Google Scholar]
- Corrigan, B.M.; VanWyk, B.-E.; Geldenhuys, C.J.; Jardine, J.M. Ethnobotanical plant uses in the KwaNibela Peninsula, St Lucia, South Africa. S. Afr. J. Bot. 2011, 77, 346–359. [Google Scholar] [CrossRef]
- Maroyi, A. Diversity of use and local knowledge of wild and cultivated plants in the Eastern Cape province, South Africa. J. Ethnobiol. Ethnomed. 2017, 13, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masevhe, N.A.; McGaw, L.J.; Eloff, J.N. The traditional use of plants to manage candidiasis and related infections in Venda, South Africa. J. Ethnopharmacol. 2015, 168, 364–372. [Google Scholar] [CrossRef] [Green Version]
- Mabogo, D.E.N. The Ethnobotany of the Vhavenda; University of Pretoria: Pretoria, South Africa, 1990. [Google Scholar]
- Mulaudzi, R.B.; Ndhlala, A.R.; Kulkarni, M.G.; Finnie, J.F.; Staden, J.V. Anti-inflammatory and mutagenic evaluation of medicinal plants used by Venda people against venereal and related diseases. J. Ethnopharmacol. 2013, 146, 173–179. [Google Scholar] [CrossRef] [PubMed]
- Chinsembu, K.C.; Negumbo, J.; Likando, M.; Mbangu, A. An ethnobotanical study of medicinal plants used to treat livestock diseases in Onayena and Katima Mulilo, Namibia. S. Afr. J. Bot. 2014, 94, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Tripathi, R.; Chung, Y.B.; Deering, K.; Saracini, N.; Willoughby, R.; Wills, O.; Mikhail, M.; Warburton, H.; Jayasinghe, D.; Rafanomezana, J. What Works for Women: Proven approaches for empowering women smallholders and achieving food security. Oxfam Policy Pract. Agric. Food Land 2012, 12, 113–140. [Google Scholar]
- Bhat, R.B. Plants of Xhosa people in the Transkei region of Eastern Cape (South Africa) with major pharmacological and therapeutic properties. J. Med. Plants Res. 2013, 7, 1474–1480. [Google Scholar]
- Dlisani, P.B.; Bhat, R.B. Traditional health practices in Transkei with special emphasis on maternal and child health. Pharm. Biol. 1999, 37, 32–36. [Google Scholar] [CrossRef]
- Zahidin, N.S.; Saidin, S.; Zulkifli, R.M.; Muhamad, I.I.; Ya’akob, H.; Nur, H. A review of Acalypha indica L. (Euphorbiaceae) as traditional medicinal plant and its therapeutic potential. J. Ethnopharmacol. 2017, 207, 146–173. [Google Scholar] [CrossRef] [PubMed]
- Nzue, M.M.; Pierre, A. Use and Conservation Status of Medicinal Plants in the Cape Peninsula, Western Cape Province of South Africa; University of Stellenbosch: Stellenbosch, South Africa, 2009. [Google Scholar]
- Sharma, M.C.; Sharma, S. Phytochemical, preliminary pharmacognostical and antimicrobial evaluation of combined crude aqueous extract. Int. J. Microbiol. 2010, 1, 166–170. [Google Scholar]
- Cock, I. The Genus Aloe: Phytochemistry and Therapeutic Uses Including Treatments for Gastrointestinal Conditions and Chronic Inflammation; Springer: Basel, Switzerland, 2015; Volume 70, pp. 179–235. [Google Scholar]
- Mapiye, C.; Chimonyo, M.; Marufu, M.; Dzama, K. Utility of Acacia karroo for beef production in Southern African smallholder farming systems: A review. Anim. Feed. Sci. Technol. 2011, 164, 135–146. [Google Scholar] [CrossRef]
- Kayombo, E. Traditional methods of protecting the infant and child illness/disease among the Wazigua at Mvomero Ward, Morogoro, Region, Tanzania. J. Altern. Integr. Med. 2013, 2, 1000103. [Google Scholar] [CrossRef]
- Idamokoro, E.M.; Masika, P.J.; Muchenje, V. Vachellia karroo leaf meal: A promising non-conventional feed resource for improving goat production in low-input farming systems of Southern Africa. Afr. J. Range Forage Sci. 2016, 33, 141–153. [Google Scholar] [CrossRef]
- Randrianarivony, T.N.; Ramarosandratana, A.V.; Andriamihajarivo, T.H.; Rakotoarivony, F.; Jeannoda, V.H.; Randrianasolo, A.; Bussmann, R.W. The most used medicinal plants by communities in Mahaboboka, Amboronabo, Mikoboka, Southwestern Madagascar. J. Ethnobiol. Ethnomed. 2017, 13, 19. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, M.; Zafar, M.; Shahzadi, N.; Yaseen, G.; Murphey, T.M.; Sultana, S. Ethnobotanical importance of medicinal plants traded in herbal markets of Rawalpindi- Pakistan. J. Herb. Med. 2018, 11, 78–89. [Google Scholar] [CrossRef]
- Keirungi, J.; Fabricius, C. Selecting medicinal plants for cultivation at Nqabara on the Eastern Cape Wild Coast, South Africa. S. Afr. J. Sci. 2005, 101, 497–501. [Google Scholar]
- Potgieter, L.; Irlich, U.M.; Gaertner, M.; Stafford, L. Recommendations for municipalities to become compliant with national legislation on biological invasions. Bothalia-Afr. Biodivers. Conserv. 2017, 47, 1–11. [Google Scholar]
- Van Wyk, A.S.; Prinsloo, G. Medicinal plant harvesting, sustainability and cultivation in South Africa. Biol. Conserv. 2018, 227, 335–342. [Google Scholar] [CrossRef]
- Constitution of Republic of South Africa. National Environmental Management: Protected Areas Amendment Act (Act No. 21 of 2014). Gov. Gaz. Pretoria S. Afr. 2014, 588, 27274. [Google Scholar]
- Constitution of Republic of South Africa. Republic of South Africa Traditional Health Practitioners Act; Government Gazzatte South Africa: Cape Town, South Africa, 2007. [Google Scholar]
- Constitution of the Republic of South Africa. Notice: Draft Policy on African Traditional Medicine for South Africa; South Africa Department of Communications Pretoria: South Africa, 2008; Volume Notice 906 of 2008; p. 49. [Google Scholar]
- Constitution of the Republic of South Africa. Protection Promotion Development and Management of Indigenous Knowledge Act of 2019; Department of Communications: Cape Town, South Africa, 2019; Volume 42647, pp. 1–28. [Google Scholar]
- NPC. National Development Plan 2030: Our Future-Make It Work; Sherino Printers: Pretoria, South Africa, 2012. [Google Scholar]
- Cotula, L. Land Grab or Development Opportunity?: Agricultural Investment and International Land Deals in Africa; Iied: London, UK, 2009. [Google Scholar]
- Cooksey, B. The Comprehensive Africa Agriculture Development Programme (CAADP) and Agricultural Policies in Tanzania: Going with or against the Grain. In Proceedings of the Future Agricultures. Available online: http://www.future-agricultures.org/pp-conference-papers/the-political-economy-of-caadp-engagement/1646-caadp-and-agricultural-policies-in-tanzania-going-with-or-against-the-grain (accessed on 1 October 2021).
- Van Wyk, B.-E.; Smith, G. Guide to the Aloes of South Africa; Briza Publications: Pretoria, South Africa, 1996. [Google Scholar]
- Herforth, A. Promotion of Traditional African Vegetables in Kenya and Tanzania: A Case Study of an Intervention Representing Emerging Imperatives in Global Nutrition. Ph.D. Thesis, Cornell University, New York, NY, USA, 2010. [Google Scholar]
- Khumalo, N.Z. An Assessment of the Contribution of Peri-Urban Agriculture on Household Food Security in Tongaat, eThekwini Municipality. Master’s Thesis, University of Zululand, KwaDlangezwa, South Africa, 2018. [Google Scholar]
- Mabhaudhi, T.; Chibarabada, T.P.; Chimonyo, V.G.P.; Murugani, V.G.; Pereira, L.M.; Sobratee, N.; Govender, L.; Slotow, R.; Modi, A.T. Mainstreaming underutilized indigenous and traditional crops into food systems: A South African perspective. Sustainability 2019, 11, 172. [Google Scholar] [CrossRef] [Green Version]
- Tesfahuneygn, G.; Gebreegziabher, G. Medicinal plants used in traditional medicine by Ethiopians: A review article. J. Genet. Genet. Eng. 2019, 2, 18–21. [Google Scholar]
- Sofowora, A.; Ogunbodede, E.; Onayade, A. The role and place of medicinal plants in the strategies for disease prevention. Afr. J. Tradit. Complement. Altern. Med. 2013, 10, 210–229. [Google Scholar] [CrossRef]
- Division, N.T.E.P. Economic Transformation, Inclusive Growth, and Competitiveness: A Contribution towards a Growth Agenda for the South African Economy; National Treasury: Pretoria, South Africa, 2019. [Google Scholar]
- Omotayo, O.A.; Ndhlovu, P.T.; Olagunju, K.O.; Tshwane, S.C.; Aremu, A.O. Determinants of household’s income and willingness to pay for indigenous plants in North West Province, South Africa: A Two-stage Heckman Approach. Sustainability 2020, 13, 5458. [Google Scholar] [CrossRef]
- Sharma, K.; Pathania, M.; Lal, H. Value chain analysis and financial viability of agro-processing industries in Himachal Pradesh. Agric. Econ. Res. Rev. 2010, 23, 515–522. [Google Scholar]
- Shaheen, F.A.; Wani, S.A.; Kubrevi, S.S. The landscape of agro-processing industries in Jammu & Kashmir. Agric. Econ. Res. Rev. 2019, 32, 175–182. [Google Scholar]
- Kala, C.P.; Dhyani, P.P.; Sajwan, B.S. Developing the medicinal plants sector in northern India: Challenges and opportunities. J. Ethnobiol. Ethnomed. 2006, 2, 32. [Google Scholar] [CrossRef] [Green Version]
- Paremoer, T. Regional Value Chains: Exploring Linkages and Opportunities in the Agro-Processing Sector across Five SADC Countries; Centre for Competition, Regulation & Economic Development (CCRED): New York, NY, USA, 2018. [Google Scholar]
- Zhang, L.; Zhuang, H.; Zhang, Y.; Wang, L.; Zhang, Y.; Geng, Y.; Gou, Y.; Pei, S.; Wang, Y. Plants for health: An ethnobotanical 25-year repeat survey of traditional medicine sold in a major marketplace in North-west Yunnan, China. J. Ethnopharmacol. 2018, 224, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Suneetha, M.; Chandrakanth, M. Establishing a multi-stakeholder value index in medicinal plants an economic study on selected plants in Kerala and Tamilnadu States of India. Ecol. Econ. 2006, 60, 36–48. [Google Scholar] [CrossRef]
- Awotedu, B.; Akala, A.; Omolola, T.; Owoeye, E.; Olaoti-Laaro, S.; Ogunsiji, A. Some underutilized indigenous timber trees with high medicinal values: Its challenges and prospects. World J. Adv. Res. Rev. 2021, 10, 161–168. [Google Scholar] [CrossRef]
- Kayombo, E.; Mahunnah, R.; Uiso, F. Prospects and challenges of medicinal plants conservation and traditional medicine in Tanzania. Anthropol. Educ. Q. 2013, 1, 108. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scientific Name and Family | Childhood Diseases/Conditions | Plant Parts and Preparation | * Conservation Status in South Africa | Reference | Region(s) of Availability | Signature Phytochemicals |
|---|---|---|---|---|---|---|
| Gomphocarpus fruticosus (L.) W.T. AitonApocynaceae | Convulsions, stomach ailments, chest ailments and milk latex used for the treatment of warts | Whole plant, leaves Infusion/poultice | LC | [4,5,48] | North Africa and the Arabian Peninsula [40]; Southern Africa and East Africa [34,41] | Glycosides [40] |
| Acalypha glabrata Thunb. Euphorbiaceae | Skin-related problems (e.g., skin rashes) | Stem, bark A sufficient amount of fresh stem is cut open and gently heated over an open fire before being applied to the skin. | LC | [67,68] | Indian Ocean islands, Asia and Africa [29,69] | - |
| Vachellia karroo Hayne Banfi and Galosso Syn: Acacia karroo var. transvaalensis (Burtt Davy) Burtt Davy Leguminosae/Fabaceae | Diarrhoea, dysentery, colic and convulsions | Whole plant Infusion and decoction | LC | [4,60,70] | Southern Africa [45,46] | Tannis and flavonoids [30] |
| Datura stramonium L. Solanaceae | Ailments such as mumps, earache (otitis) | Leaves, Maceration | IA | [5,20,51] | Europe and South America [36,37] | Tropane alkaloids [47,71] |
| Rhoicissus tridentata (L.f.) Wild and Drummond. Vitaceae | Pulsating anterior fontanelle, stomach-ache and stop vomiting | Roots, leaves Infusion/Maceration | R | [4,20,56,63] | Africa to Asia and the Pacific Islands [43] | Anthocyanidin [30] |
| Aloe maculata All. Xanthorrhoeaceae | Feverish colds, induce vomiting and weaning | Flower, Infusion | LC | [4,20,38] | Africa, India and other arid areas [31,32] | Acetylated mannans, polymannans, anthroquinones, anthraquinone glycosides, anthrones, lectins [72,73] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ndhlovu, P.T.; Omotayo, A.O.; Otang-Mbeng, W.; Aremu, A.O. Commercialization Potential of Six Selected Medicinal Plants Commonly Used for Childhood Diseases in South Africa: A Review. Sustainability 2022, 14, 177. https://doi.org/10.3390/su14010177
Ndhlovu PT, Omotayo AO, Otang-Mbeng W, Aremu AO. Commercialization Potential of Six Selected Medicinal Plants Commonly Used for Childhood Diseases in South Africa: A Review. Sustainability. 2022; 14(1):177. https://doi.org/10.3390/su14010177
Chicago/Turabian StyleNdhlovu, Peter Tshepiso, Abiodun Olusola Omotayo, Wilfred Otang-Mbeng, and Adeyemi Oladapo Aremu. 2022. "Commercialization Potential of Six Selected Medicinal Plants Commonly Used for Childhood Diseases in South Africa: A Review" Sustainability 14, no. 1: 177. https://doi.org/10.3390/su14010177
APA StyleNdhlovu, P. T., Omotayo, A. O., Otang-Mbeng, W., & Aremu, A. O. (2022). Commercialization Potential of Six Selected Medicinal Plants Commonly Used for Childhood Diseases in South Africa: A Review. Sustainability, 14(1), 177. https://doi.org/10.3390/su14010177