


Study on the Design Strategy of Rehabilitation Space for Patients with Cognitive Disorders Based on the Environmental Adaptation of Disease Symptoms

 , ,
, ,
Abstract
:1. Introduction
2. Research Methodology and Site Overview
2.1. Research Subjects
2.2. Research Method
2.3. Site Overview
3. Feasibility of Spatial Design Intervention in the Rehabilitation of Cognitive Disorders
3.1. Relevance of Disease Recovery to the Environment
3.1.1. Cognitive Impairment and Spatial Layout

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Opinions or Research Findings |
|---|---|
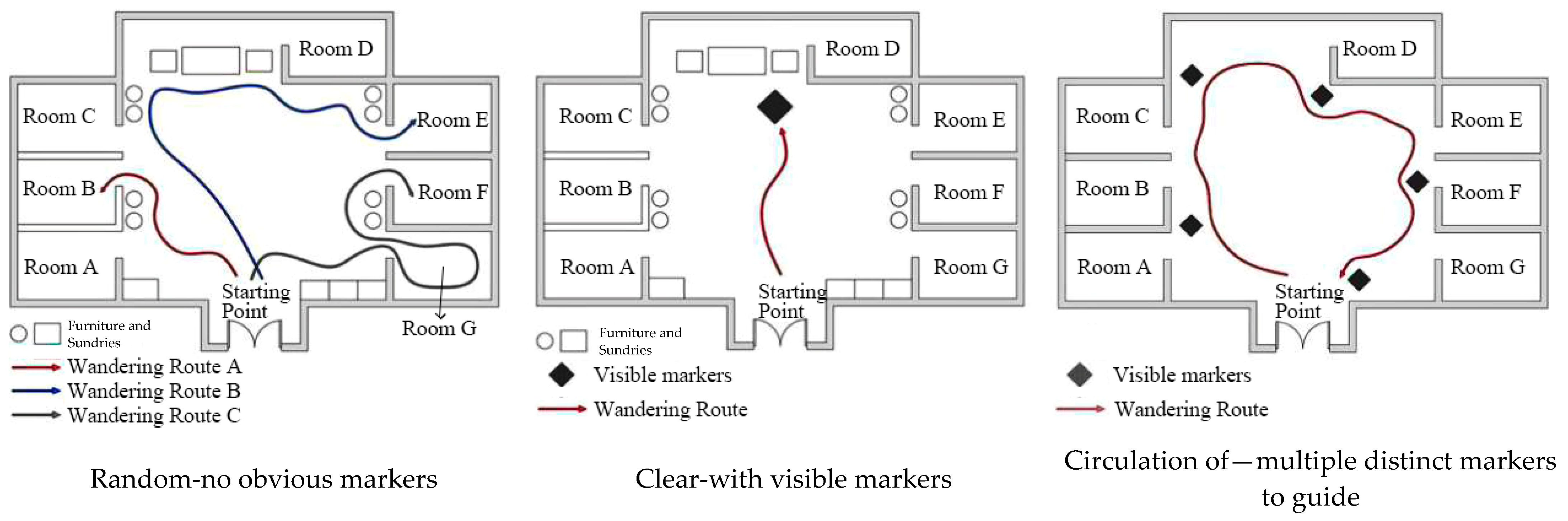
| Yanan, W. [17] | At the Nuremberg Dementia Care Center in Germany, patients’ interaction with their environment is increased by creating pathways that facilitate wandering in circles and rich environmental stimuli, thereby reducing meaningless wandering behavior. |
| Backhouse, T. [41] | Wandering may be more of a problem for patients in home care than in institutional care settings. |
| Algase, D L. [42] | Wandering behavior overlaps with the spatial orientation problem, which is closely related to the spatial context of wandering. |
| Coons, D. [43] | However, the environmental context lacks attraction, engagement, and belonging, and spontaneous activities of restless wandering may occur. A stimulation-rich environment can reduce wandering behavior. |
| Snyder, LH. [44] | Goal orientation, stress, and boredom are the three main causes of wandering behavior. However, when the environment is unattractive, it may increase the wandering behavior of patients. |
| Calkins, M. [45] | As cognitive decline blurs the familiarity of the environment for people with cognitive disorders, unfamiliarity can become frightening and may prompt continuous wandering behavior. |
| Dunkle, R.E. [46] | The stressors associated with moving to a new environment may increase wandering behavior. |
| Dickinson, J. [47] | Wandering behavior of vagrants may be attributed to boredom or stress. |
| Hussain, R.A. [48] | An interesting environment can distract the patient, thus reducing the boredom and restlessness of wandering. |
| Calkins, M.P. [49] | Interactive artwork is used along a corridor in a dementia care unit at the Iowa Veterans Home in Iowa City, and it can interrupt the patient’s wandering behavior. Although simple in design, it adds visual interest to the unit and, more importantly, it may have therapeutic value when wanderers stop and interact. |
3.1.2. Nursing Efficiency and Line of Sight Access
3.2. Feasibility of Spatial Design Interventions for the Rehabilitation of Patients’ Conditions
3.2.1. Adjusting Spatial Layout to Improve Cognitive Function
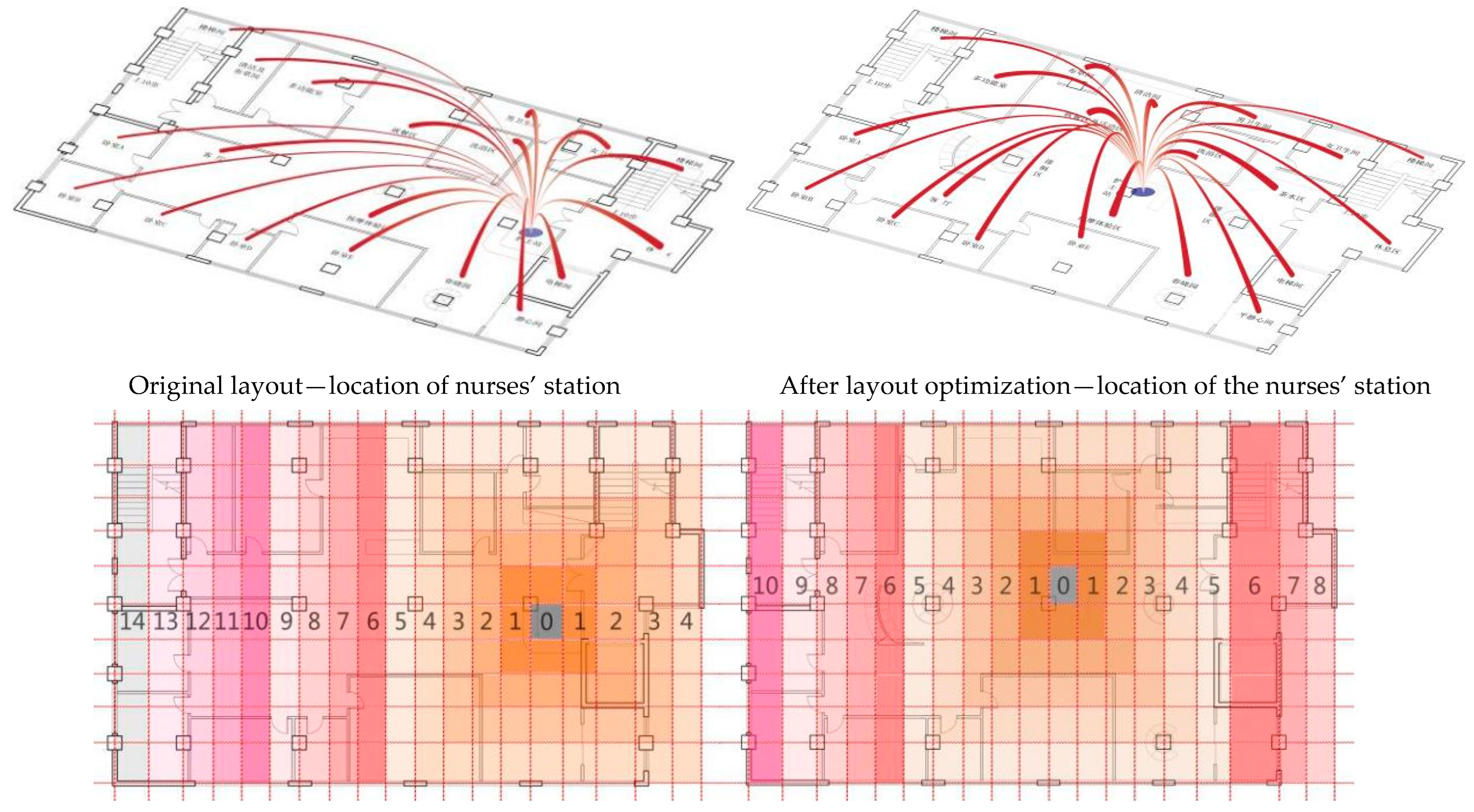
3.2.2. Optimize Visual Access to Improve Care Efficiency
4. Space Transformation Optimization Assessment
4.1. Visual Visibility
4.2. Nursing Efficiency
5. Results and Discussion
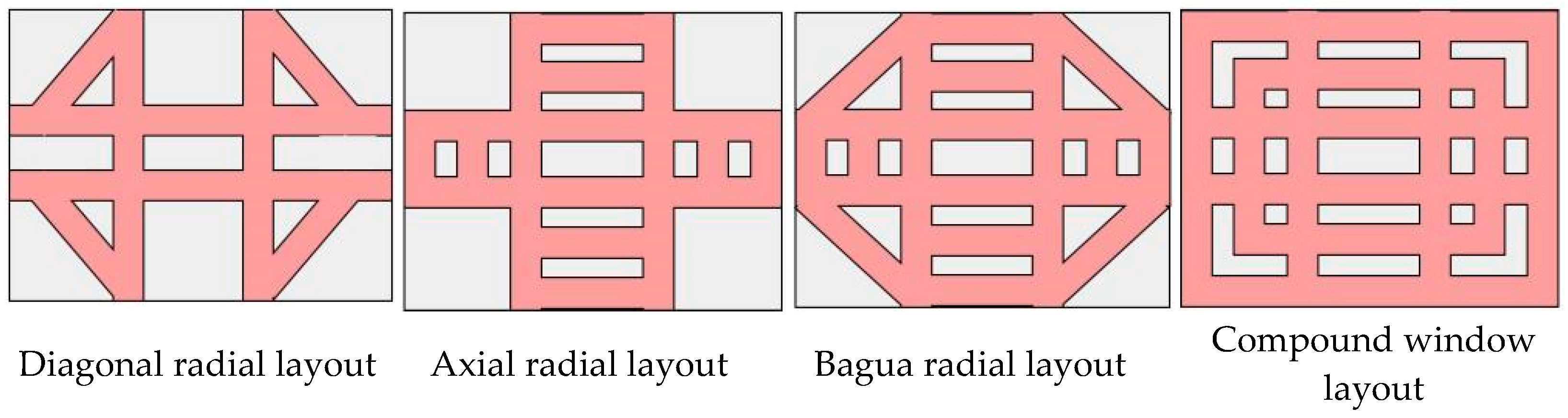
5.1. A Design Approach to Space Layout for the Rehabilitation of Patients with Cognitive Disorders
5.1.1. Guiding Spatial Behavior
5.1.2. Reduced Walking Distance
5.1.3. Deepening Space Exchange
5.2. Discussion of Results
5.3. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guo, T.H.; Dong, L.; Sun, Q.H. Design and Evidence An Exploration of Evidence-Based Design Methods for Rehabilitation Landscapes. Landsc. Archit. 2015, 9, 106–112. [Google Scholar]
- Ulrich, R.S. Aesthetic and affective response to natural environment. In Behavior and the Natural Environment; Springer: New York, NY, USA, 1983; pp. 85–125. [Google Scholar]
- Zeisel, J. Environment-Behavior Studies: A Precursor for Neuroscience in Design. In Brain Landscape: The Coexistence of Neuroscience and Architecture; Eberhard, J.P., Ed.; Oxford University Press: Oxford, UK, 2009. [Google Scholar]
- Zeisel, J. Inquiry by Design: Environment/Behavior/Neuroscience in Architecture, Interiors, Landscape, and Planning; W. W. Norton & Co.: New York, NY, USA, 2006. [Google Scholar]
- Ren, R.J.; Yin, P.; Wang, Z.H. Alzheimer’s disease in China report 2021. Diagn. Theory Pract. 2021, 20, 317–337. [Google Scholar]
- Belger, M.; Haro, J.M.; Reed, C.; Happich, M.; Argimon, J.M.; Bruno, G.; Dodel, R.; Jones, R.W.; Vellas, B.; Wimo, A. Determinants of time to institutionalisation and related healthcare and societal costs in a community-based cohort of patients with Alzheimer’s disease dementia. Eur. J. Health Econ. 2019, 20, 343–355. [Google Scholar] [CrossRef] [Green Version]
- Beeber, A.S.; Zimmerman, S.; Wretman, C.J.; Palmertree, S.; Patel, K.; Sloane, P.D. Potential Side Effects and Adverse Events of Antipsychotic Use for Residents with Dementia in Assisted Living: Implications for Prescribers, Staff, and Families. J. Appl. Gerontol. 2021, 41, 798–805. [Google Scholar] [CrossRef]
- Sandberg, L.; Borell, L.; Rosenberg, L. Risks as dilemmas for home care staff caring for persons with dementia. Aging Ment. Health 2021, 25, 1701–1708. [Google Scholar] [CrossRef] [Green Version]
- China Association of Geriatric Health Care. 2019 China Alzheimer’s Disease Patients’ Family Survival Research Report. Available online: http://weixin.moreedge.cn/bps_2019/index.php (accessed on 14 June 2021).
- Stigsdotter, U.K.; Corazon, S.S.; Sidenius, U.; Kristiansen, J.; Grahn, P. It is not all bad for the grey city—A crossover study on physiological and psychological restoration in a forest and an urban environment. Health Place 2017, 46, 145–154. [Google Scholar] [CrossRef]
- Kaplan, R.; Kaplan, S. Well-being, reasonableness, and the natural environment. Appl. Psychol. Health Well-Being 2011, 3, 304–321. [Google Scholar] [CrossRef] [Green Version]
- Gesler, W.M. Therapeutic landscape: Theory and a case study of Epidauros, Greece. Environ. Plan. 1993, 11, 171–189. [Google Scholar] [CrossRef]
- Marcus, C.C.; Francis, C. (Eds.) Humanity Place: Design Guidelines for Urban Open Space; China Construction Industry Press: Beijing, China, 2001. [Google Scholar]
- Martin, N.; Philip, B.W. Validation therapy for dementia. Cochrane Database Syst. Rev. 2003, 3, CD001394. [Google Scholar]
- Chang, H. (Ed.) Psychology of the Built Environment; China Construction Industry Press: Beijing, China, 1990. [Google Scholar]
- Laurie, S. Reminiscence Therapy: Favorite Things. Libr. J. 2019, 144, 56. [Google Scholar]
- Wang, Y.; Shu, P. Exploring the design of dementia elderly care space based on evidence-based design. Chin. Foreign Archit. 2015, 8, 107–109. [Google Scholar]
- Kemp, D.; Yan, D. The calibration of time: Responding to the progressive disease crisis-two rehabilitation gardens for people with AIDS and dementia. China Gard. 2015, 31, 12–17. [Google Scholar]
- Moore, G.T.; Tuttle, D.P.; Howell, S.C. Environmental Design Research Directions: Process and Prospects; Greenwood: Westport, CT, USA, 1985. [Google Scholar]
- Guo, C. The design practice of large infectious disease hospital. J. Archit. 2007, 10, 80–83. [Google Scholar]
- Studer, R.G. The dynamics of behavior-contingent physical systems. In Environmental Psychology: Man and His Physical Setting; Athens Center of Ekistics: Athens, Greece, 1970; pp. 56–76. [Google Scholar]
- Hamilton, D.K. Hypothesis and measurement: Essential steps for evidence-based design. Healthc. Des. 2004, 3, 43–46. [Google Scholar]
- Yang, W.; Jin, H.; Yan, H.; Liu, X. Study on the creation of plant fragrance in Suzhou Yiyuan Garden. Chin. Gard. 2021, 37, 139–144.9. [Google Scholar]
- Wu, F. The science of place and rehabilitation—A study on the design of Alzheimer’s rehabilitation garden. Archit. Cult. 2018, 1, 125–126. [Google Scholar]
- Su, X. Plant Landscaping; China Forestry Press: Beijing, China, 1994. [Google Scholar]
- Roberts, G.; Morley, C.; Walters, W.; Malta, S.; Doyle, C. Caring for people with dementia in residential aged care: Successes with a composite person-centered care model featuring Montessori-based activities. Geriatr. Nurs. 2015, 36, 106–110. [Google Scholar] [CrossRef]
- Dementia Fact Sheet. 2015. Available online: http://www.who.int/mediacentre/factsheets/fs362/en/ (accessed on 14 June 2021).
- Petersen, R.C.; Smith, G.E.; Waring, S.C.; Ivnik, R.J.; Tangalos, E.G.; Kokmen, E. Mild cognitive impairment: Clinical characterization and outcome. Arch. Neurol. 1999, 56, 303–308. [Google Scholar] [CrossRef]
- Hamilton, D.K.; Watkins, D.H. Evidence-Based Design for Multiple Building Types; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- Wang, H.-H.; Xiao, S.-F. Research progress of neuropathological markers of Alzheimer’s disease. Shanghai Psychiatry 2009, 21, 55–57. [Google Scholar]
- Liu, X.; Wang, Y. Architectural knowledge management based on evidence-based design practice. New Archit. 2019, 1, 82–85. [Google Scholar]
- Mallgrave, H. The Architect’s Brain: Neuroscience, Creativity and Architecture; Electronic Industry Press: Beijing, China, 2011. [Google Scholar]
- Urabe, M.; Fukuda, H.; Noda, Y. Intervention with nostalgic music and reminiscences provide positive emotions for people with dementia and reduces BPSD. In Proceedings of the 2020 Alzheimer’s Association International Conference, Amsterdam, The Netherlands, 27–31 July 2020. [Google Scholar]
- Damuka, N.; Kammari, K.; Potshangbam, A.M.; Rathore, R.S.; Kondapi, A.K.; Vindal, V. Discovery of dual cation-π inhibitors of acetylcholinesterase: Design, synthesis and biological evaluation. Pharmacol. Rep. 2020, 72, 705–718. [Google Scholar] [CrossRef]
- Algase, D.L. Wandering. A dementia-compromised behavior. J. Gerontol. Nurs. 1999, 25, 10. [Google Scholar] [CrossRef]
- Vancampfort, D.; Stubbs, B.; Lara, E.; Vandenbulcke, M.; Swinnen, N.; Smith, L.; Firth, J.; Herring, M.P.; Hallgren, M.; Koyanagi, A. Mild cognitive impairment and sedentary behavior: A multinational study. Exp. Gerontol. 2018, 108, 174–180. [Google Scholar] [CrossRef]
- Sun, X.; Deng, Y.; Dong, B. Advances in the treatment of psycho-behavioral symptoms of dementia and recommendations for caregiving. Mod. Clin. Med. 2021, 47, 223–226. [Google Scholar]
- Zubenko, G.S.; Cohen, B.M.; Lipinski, J.F., Jr. Antidepressant-related akathisia. J. Clin. Psychopharmacol. 1987, 7, 254–257. [Google Scholar] [CrossRef]
- Glenn. Thinking about Hospital Architecture in China: An Interview with Glenn; China Construction Industry Press: Beijing, China, 2015. [Google Scholar]
- Pachilova, R.; Sailer, K. Providing care quality by design: A new measure to assess hospital ward layouts. J. Archit. 2020, 25, 186–202. [Google Scholar] [CrossRef]
- Backhouse, T.; Camino, J.; Mioshi, E. What do we know about behavioral crises in dementia? A systematic review. J. Alzheimer’s Dis. 2018, 62, 99–113. [Google Scholar] [CrossRef] [Green Version]
- Algase, D.L.; Son, G.R.; Beattie, E.; Song, J.; Leitsch, S.; Yao, L. The interrelatedness of wandering and wayfinding in a community sample of persons with dementia. Dement. Geriatr. Cogn. Disord. 2004, 17, 231–239. [Google Scholar] [CrossRef]
- Coons, D. Wandering. Am. J. Alzheimer’s Care Relat. Disord. Res. 1988, 3, 31–36. [Google Scholar] [CrossRef] [Green Version]
- Snyder, L.H.; Rupprecht, P.; Pyrek, J.; Brekhus, S.; Moss, T. Wandering. Gerontologist 1978, 18, 272–280. [Google Scholar] [CrossRef]
- Calkins, M. Designing cues for wanderers. Special needs in nursing homes. Architecture 1989, 78, 117–118. [Google Scholar]
- Dunkle, R.E.; Kart, C.S. Long-term care. In Gerontology Perspectives and Issues; Ferraro, K.F., Ed.; Springer: New York, NY, USA, 1990; pp. 225–243. [Google Scholar]
- Dickinson, J.; McLain-Kark, J. Wandering behavior associated with Alzheimer’s disease and related dementias: Implications for designers. J. Inter. Des. 1996, 22, 32–38. [Google Scholar] [CrossRef]
- Hussain, R.A. Severe behavioral problems. In Geropsychologicol Assessment and Treatment; Terri, I., Lesinsohn, J., Eds.; Springer: New York, NY, USA, 1985; pp. 121–145. [Google Scholar]
- Calkins, M.P. Design for Dementia; National Health: Owings Mills, MD, USA, 1988. [Google Scholar]
- Thompson, D.R.; Hamilton, D.K.; Cadenhead, C.D.; Swoboda, S.M.; Schwindel, S.M.; Anderson, D.C.; Schmitz, E.V.; St Andre, A.C.; Axon, D.C.; Harrell, J.W.; et al. Guidelines for intensive care unit design. Crit. Care Med. 2012, 40, 1586–1600. [Google Scholar] [CrossRef]
- Gharaveis, A.; Hamilton, D.K.; Pati, D.; Shepley, M. The impact of visibility on teamwork, collaborative communication, and security in emergency departments: An exploratory study. HERD Health Environ. Res. Des. J. 2018, 11, 37–49. [Google Scholar] [CrossRef]
- Colley, J.; Zeeman, H.; Kendall, E. “Everything Happens in the Hallways”: Exploring User Activity in the Corridors at Two Rehabilitation Units. HERD Health Environ. Res. Des. J. 2018, 11, 163–176. [Google Scholar] [CrossRef]
- Barsukiewicz, C.K.; Raffel, M.W.; Raffel, N.K. The US Health System: Origins and Functions; Cengage Learning: Boston, MA, USA, 2010. [Google Scholar]
- Hadi, K.; Zimring, C. Design to improve visibility: Impact of corridor width and unit shape. HERD Health Environ. Res. Des. J. 2016, 9, 35–49. [Google Scholar] [CrossRef]
- China Architecture Society. Architectural Design Sourcebook; Construction Industry Press: Beijing, China, 2017. [Google Scholar]
- Liao, X.; Kiyoko, M.; Miyae, Y.; He, X.; Li, Y. Comparison of wandering behavior in Alzheimer’s disease and frontotemporal dementia. Chin. J. Neuropsychiatr. Disord. 2011, 37, 545–549. [Google Scholar]
- Day, K.; Carreon, D.; Stump, C. The therapeutic design of environments for people with dementia: A review of the empirical research. Gerontologist 2000, 40, 397–416. [Google Scholar] [CrossRef] [Green Version]
- US Congress Office of Technology Assessment. Special Care Units for People with Alzheimer’s and Other Dementias: Consumer Education, Research, Regulatory and Reimbursement Issues; US Congress Office of Technology Assessment: Washington, DC, USA, 1992.
- Rocha, I.I.; Narasimhalu, K.; De Silva, D.A. Impact of Air Pollution and Seasonal Haze on Neurological Conditions. Ann. Acad. Med. Singap. 2020, 49, 26–36. [Google Scholar] [CrossRef]
- Special Committee on Neurodegenerative Diseases of the Chinese Society of Microcirculation; Neuropsychological and Behavioral Neurology Group of the Chinese Society of Neurology; Neurorehabilitation Group of the Chinese Society of Neurology; Chinese Society of Neurology. Chinese expert consensus on rehabilitation management of Alzheimer’s disease (2019). Chin. J. Geriatr. 2020, 39, 9–19. [Google Scholar]
- The Architectural Institute of Japan. Architectural Design Data Integration—Human Space; Xu, Y., Ed.; Tianjin University Press: Tianjin, China, 2007; p. 65. [Google Scholar]
- Sallis, J.F.; Glanz, K. Physical activity and food environments: Solutions to the obesity epidemic. Milbank Q. 2009, 87, 123–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Futrell, M.; Melillo, K.D.; Remington, R.; Butcher, H.K. Evidence-based practice guideline: Wandering. J. Gerontol. Nurs. 2014, 40, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and welfare (HIHW) Hospital Dementia Services. Available online: https://www.aihw.gov.au/reports/australias-welfare/aged-care (accessed on 7 September 2022).
- Tong, J. Research on the Internal Space Evaluation of Urban Planning Exhibition Hall Building Based on Spatial Syntax Method; Hunan University of Technology: Zhuzhou, China, 2018. [Google Scholar]
- Trzpuc, S.J.; Martin, C.S. Application of space syntax theory in the study of medical-surgical nursing units in urban hospitals. HERD Health Environ. Res. Des. J. 2010, 4, 34–55. [Google Scholar] [CrossRef] [PubMed]
- Seo, H.B.; Choi, Y.S.; Zimring, C. Impact of hospital unit design for patient-centered care on nurses’ behavior. Environ. Behav. 2011, 43, 443–468. [Google Scholar] [CrossRef]
- Chen, X.; Xuan, X.; Li, Z. The influence of spatial structure of nursing units on nurses’ activity behavior—A comparative study based on evidence-based design theory. Urban Archit. 2018, 32, 49–53. [Google Scholar]
- Gu, J. Doctor-patient harmony and architectural design. Archit. Creat. 2005, 12, 30–35. [Google Scholar]
- Li, H. Research on Public Transportation Space Design Strategy of General Hospital Outpatient Department; Dalian University of Technology: Dalian, China, 2016. [Google Scholar]
- Megahed, N.A.; Ghoneim, E.M. Antivirus-built environment: Lessons learned from COVID-19 pandemic. Sustain. Cities Soc. 2020, 61, 102350. [Google Scholar] [CrossRef]
- Schneider, J.W. USGBC announces partnerships, unveils new climate initiatives. Build. Des. Constr. 2006, 47, 12–13. [Google Scholar]
- Guy, S.; Farmer, G. Reinterpreting sustainable architecture: The place of technology. J. Archit. Educ. 2001, 54, 140–148. [Google Scholar] [CrossRef]





















| Environment-Behavior | Neuroscience | Design | ||
|---|---|---|---|---|
| Variables, Research Methods and Techniques in Various Fields | ||||
| Behavioral outcomes | Performance Results | Neuroscience Factors | Physiological factors | Physical environment elements |
| Observation method, photo documentation, self-reporting, etc. | Clinical records, performances, expert evaluations, etc. | PET scan, MRI, ERP evoked potentials, etc. | Testing physiological responses, such as cortisol testing, blood pressure testing | Describe environment specific Features, such as layout, scale, etc. |
| Medical Effects | Environmental Influences | |||||||
|---|---|---|---|---|---|---|---|---|
| Single Room | Natural Light | Artificial Lighting | Natural Scenery | Flooring Material | Reduce Noise | Rational Layout | Distracting Patients | |
| Reduce getting lost | ● | ● | ●● | |||||
| Reduce medical errors | ● | ● | ● | |||||
| Reduce patient falls | ● | ● | ● | |||||
| Reduce pain feeling | ●● | ● | ●● | ● | ● | ●● | ||
| Improve sleep quality | ●● | ● | ● | ● | ||||
| Reduce patient stress | ● | ● | ● | ●● | ●● | |||
| Reduce negative emotions | ●● | ●● | ● | |||||
| Reduce waiting time | ● | ● | ● | |||||
| Improve privacy and convenience | ●● | ● | ||||||
| Enhance communication | ●● | ● | ||||||
| Add satisfaction | ●● | ● | ● | ● | ● | ● | ||
| Reduce the stress of nursing | ● | ● | ● | ● | ● | |||
| Improve healthcare efficiency | ● | ● | ● | ●● | ||||
| Minimum Walking Distance/m and Gravitational Strength | Increase or Decrease/±m | ||||||
|---|---|---|---|---|---|---|---|
| Functional Area | Before Adjustment | Gravitational Strength | After Adjustment | Gravitational Strength | Changes | Partial | Total |
| Refreshment area | 3.9 | 2 | 8.3 | 4 | + | +4.4 | −83.69 |
| Rest area | 6.7 | 3 | 12.2 | 7 | + | +5.5 | |
| Elevator | 7.5 | 2 | 13.3 | 6 | + | +5.8 | |
| Bathing area | 8.2 | 3 | 11.7 | 2 | − | +3.5 | |
| Massage area | 8.3 | 5 | 1 | 2 | − | −7.3 | |
| Male’s bathroom | 9.6 | 5 | 11.3 | 2 | − | +1.7 | |
| Female’s bathroom | 11 | 4 | 11.1 | 4 | ◯ | +0.1 | |
| Spring dawn garden | 11.4 | 3 | 8 | 3 | ◯ | −3.4 | |
| Dining area | 15.8 | 6 | 8.4 | 2 | − | −7.4 | |
| Calm the mind | 17 | 4 | 14.7 | 6 | + | −2.3 | |
| Living room | 19.8 | 10 | 9.2 | 6 | − | −10.6 | |
| Multifunctional room | 21.2 | 10 | 16.3 | 7 | − | −4.9 | |
| Cleaning room | 23.5 | 12 | 15.2 | 5 | − | −8.3 | |
| Bedroom A | 26.2 | 14 | 17.6 | 9 | − | −8.6 | |
| Bedroom B | 44.1 | 14 | 19.9 | 9 | − | −24.2 | |
| Bedroom C | 23.8 | 11 | 19 | 7 | − | −4.8 | |
| Bedroom D | 22.1 | 8 | 12.4 | 4 | − | −9.7 | |
| Bedroom E | 22.2 | 6 | 13.3 | 3 | − | −8.9 | |
| Stairwell 1 | 10.2 | 5 | 12.27 | 6 | + | +2.07 | |
| Stairwell 2 | 29.3 | 14 | 23.24 | 10 | − | −6.06 | |
| Total Number of Functional Areas/pc | Walking Distance Reduction Number/pc | Proportion/% | Number of Gravitational Enhancements/pc | Proportion/% |
|---|---|---|---|---|
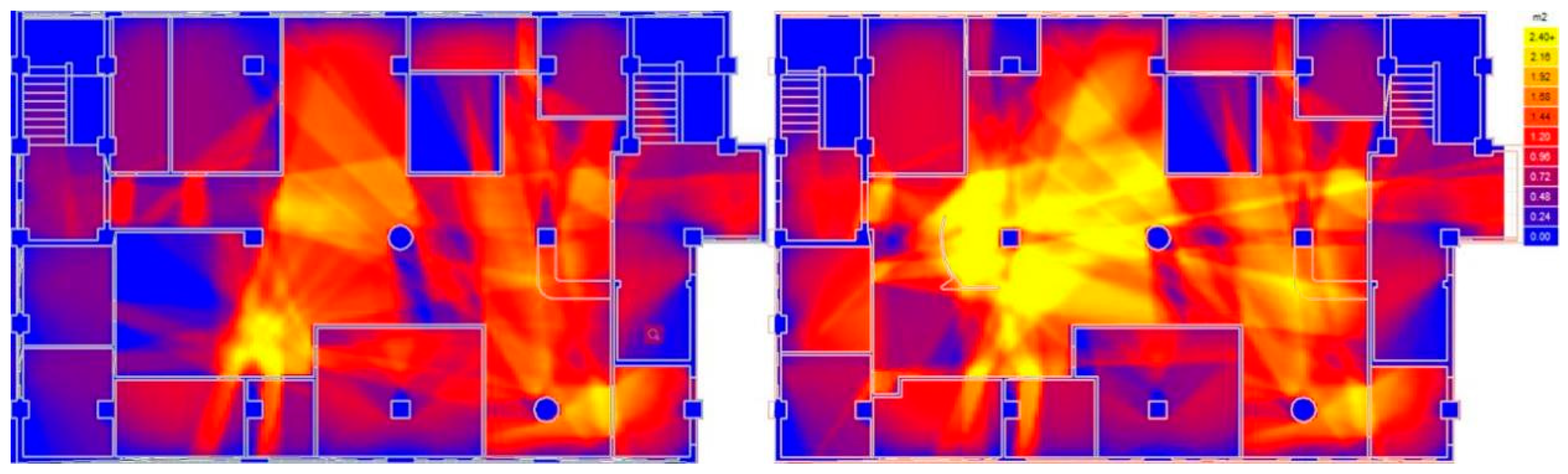
| 20 | 13 | 65% | 13 | 65% |
| High Level | Medium Level | Low Level | Polar Level | |
|---|---|---|---|---|
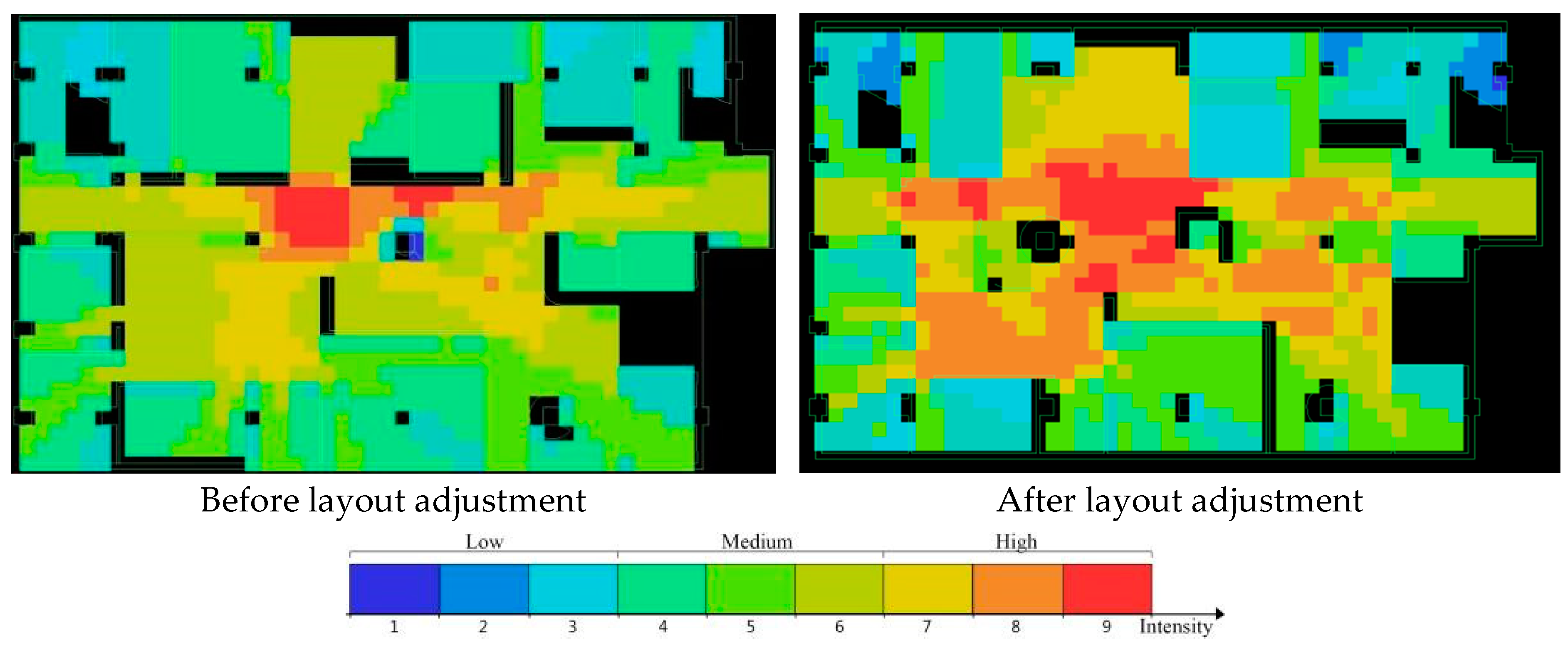
| Before Layout Adjustment | 10 | 3 | 4 | 3 |
| After Layout Adjustment | 10 | 9 | 1 | 0 |
| Domestic and International Nursing Home Layout Models | |||
|---|---|---|---|
 |  |  |  |
 |  |  |  |
| Centripetal | Scattered Cross | Overpass Surround | Multi-core scatter |
| Guangzhou Cihui Building | Protestant Homes in America | Japan Rainbow Hills Rehabilitation Center | Allen Nursing Home, England |
| Layout Movement Model | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, W.; Du, Z.; Toe, D.H.C.; Liu, Y.; Yong, K.W.; Lin, H. Study on the Design Strategy of Rehabilitation Space for Patients with Cognitive Disorders Based on the Environmental Adaptation of Disease Symptoms. Sustainability 2022, 14, 12590. https://doi.org/10.3390/su141912590
Li W, Du Z, Toe DHC, Liu Y, Yong KW, Lin H. Study on the Design Strategy of Rehabilitation Space for Patients with Cognitive Disorders Based on the Environmental Adaptation of Disease Symptoms. Sustainability. 2022; 14(19):12590. https://doi.org/10.3390/su141912590
Chicago/Turabian StyleLi, Weicong, Zhaoming Du, Doris Hooi Chyee Toe, Yueling Liu, Kum Weng Yong, and Haopai Lin. 2022. "Study on the Design Strategy of Rehabilitation Space for Patients with Cognitive Disorders Based on the Environmental Adaptation of Disease Symptoms" Sustainability 14, no. 19: 12590. https://doi.org/10.3390/su141912590
APA StyleLi, W., Du, Z., Toe, D. H. C., Liu, Y., Yong, K. W., & Lin, H. (2022). Study on the Design Strategy of Rehabilitation Space for Patients with Cognitive Disorders Based on the Environmental Adaptation of Disease Symptoms. Sustainability, 14(19), 12590. https://doi.org/10.3390/su141912590