
Spatial Distribution of COVID-19 Infected Cases in Kelantan, Malaysia

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Materials and Methods
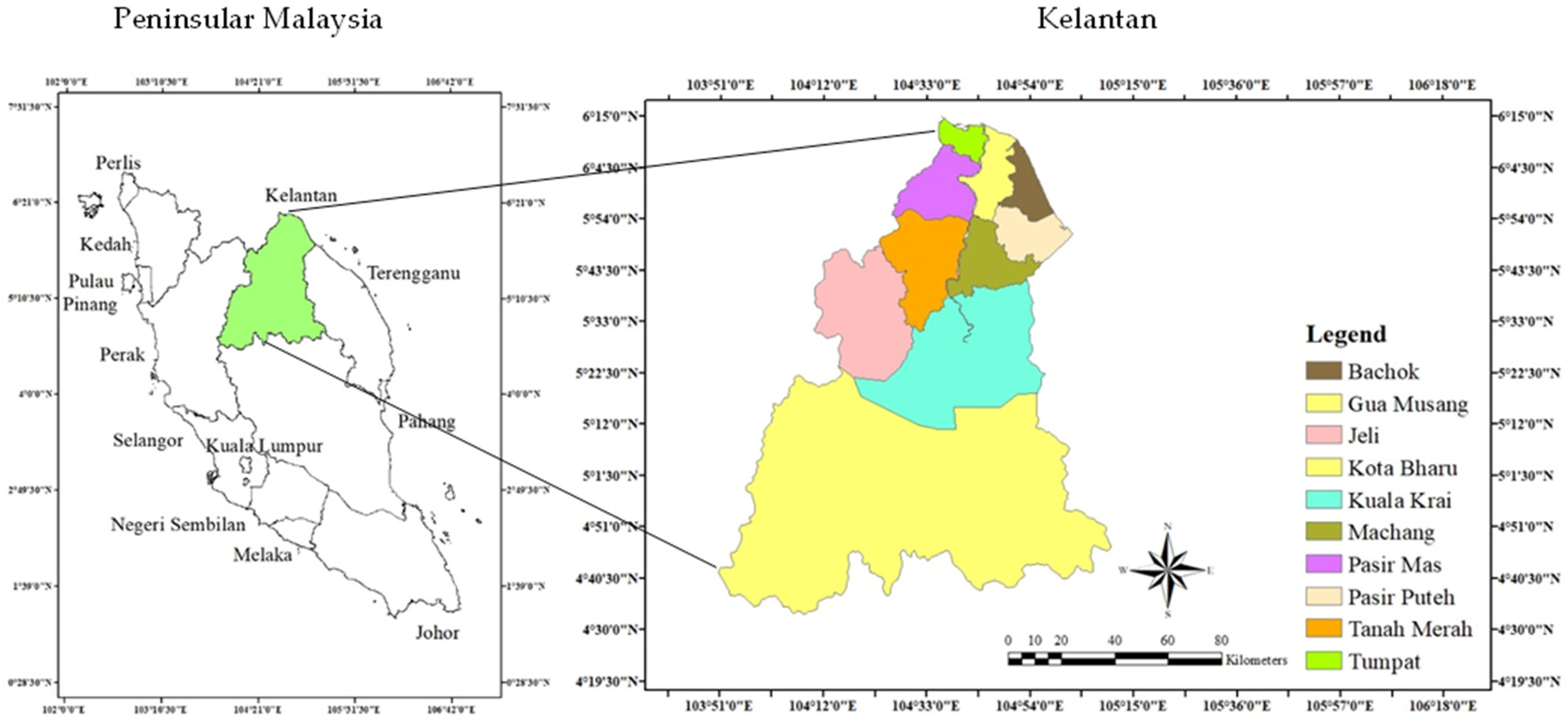
2.1. Study Area
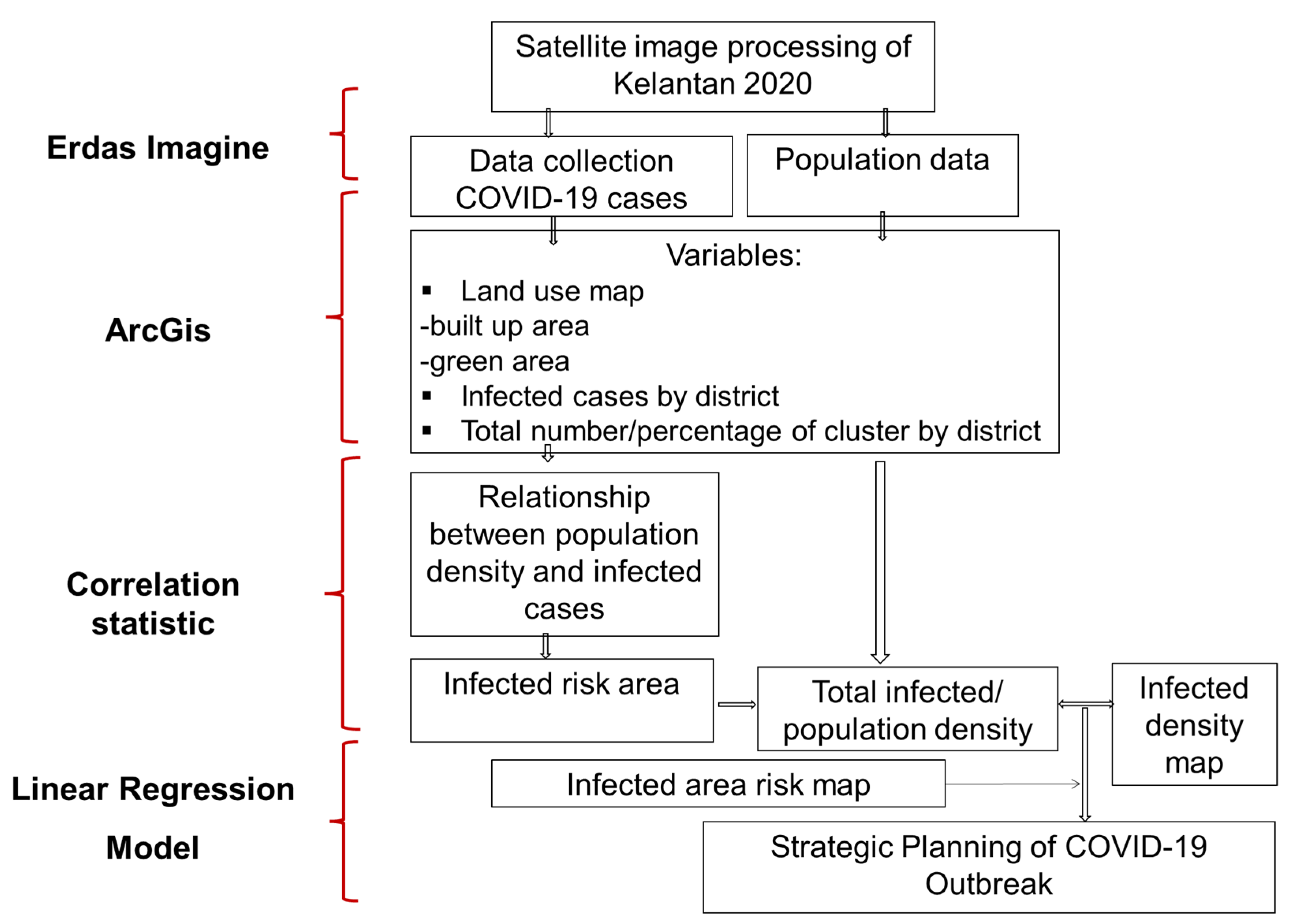
2.2. Methodological Framework
2.3. Data Collection
2.4. Image Processing
2.5. Data Analysis
2.5.1. Linear Regression Model
2.5.2. Spatial COVID-19 Model Map
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bhadra, A.; Mukherjee, A.; Sarkar, K. Impact of population density on COVID-19 infected and mortality rate in India. Model. Earth Syst. Environ. 2021, 7, 623–629. [Google Scholar] [CrossRef] [PubMed]
- WHO. Coronavirus Disease 2019 (COVID-19). 2020. Available online: https://www.who.int/docs/defaultsource/coronaviruse/situationreports/20200226-sitrep-37-covid-19.pdf (accessed on 1 April 2020).
- Ruiz, E.M.A.; Koutronas, E. The Networks Infection Contagious Diseases Positioning System (NICDP-System): The Case of Wuhan-COVID-19 SSRN 3548413. 2020. Available online: https://ssrn.com/abstract=3548413 (accessed on 5 April 2020).
- Ministry of Health. 2020. Available online: http://www.moh.gov.my/index.php (accessed on 10 April 2020).
- Hatta, H.M.; Fuzi, N.M.H.M.; Zin, N.D.M.; Rahim, A.I.A.; Zakria, N.M.; Sulaiman, S.; Muhammad, A.H.; Hussin, Z. An Epidemiological Analysis of COVID-19 cases from Jan to July 2020 in Kelantan, Malaysia. Ulum Islamiyyah. 2021, 33, 149–165. [Google Scholar] [CrossRef]
- Boehmer, T.K.; DeVies, J.; Caruso, E.; van Santen, K.L.; Tang, S.; Black, C.L.; Hartnett, K.P.; Kite-Powell, A.; Dietz, S.; Lozier, M.; et al. Changing age distribution of the COVID-19 pandemic—United States, May–August 2020. Morb. Mortal. Wkly. Rep. 2020, 69, 1404. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Bhagavathula, A.S.; Aldhaleei, W.A.; Rahmani, J.; Mahabadi, M.A.; Bandari, D.K. Novel coronavirus (COVID-19) knowledge and perceptions: A survey of healthcare workers. MedRxiv 2020, 6, e19160. [Google Scholar]
- WHO. Coronavirus Disease (COVID-19) Pandemic. 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 10 September 2022).
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Almeshal, A.M.; Almazrouee, A.I.; Alenizi, M.R.; Alhajeri, S.N. Forecasting the spread of COVID-19 in Kuwait using compartmental and logistic regression models. Appl. Sci. 2020, 10, 3402. [Google Scholar] [CrossRef]
- Nopour, R.; Shanbehzadeh, M.; Kazemi-Arpanahi, H. Using logistic regression to develop a diagnostic model for COVID-19: A single-center study. J. Educ. Health Promot. 2022, 11, 153. [Google Scholar]
- Faizalhakim, A.S.; Nurhidayu, S.; Norizah, K.; Shamsuddin, I.; Hakeem, K.R.; Ismail, A. Climate variability in relation with land use changes over a 30-year period in Kelantan River Basin. Malays. For. 2017, 80, 12–30. [Google Scholar]
- Chapa, F.; Hariharan, S.; Hack, J. A new approach to high-resolution urban land use classification using open access software and true color satellite images. Sustainability 2019, 11, 5266. [Google Scholar] [CrossRef] [Green Version]
- Jensen, J.R. Introductory Digital Image Processing: A Remote Sensing Perspective, 2nd ed.; Prentice-Hall Inc.: Hoboken, NJ, USA, 1996. [Google Scholar]
- Kariyawasam, C.S.; Kumar, L.; Kogo, B.K.; Ratnayake, S.S. Long-term changes of aquatic invasive plants and implications for future distribution: A case study using a tank cascade system in Sri Lanka. Climate 2021, 9, 31. [Google Scholar] [CrossRef]
- Yang, D.; Meng, R.; Morrison, B.D.; McMahon, A.; Hantson, W.; Hayes, D.J.; Serbin, S. A multi-sensor unoccupied aerial system improves characterization of vegetation composition and canopy properties in the Arctic tundra. Remote Sens. 2020, 12, 2638. [Google Scholar] [CrossRef]
- Manandhar, R.; Odeh, I.O.; Ancev, T. Improving the accuracy of land use and land cover classification of Landsat data using post-classification enhancement. Remote Sens. 2009, 1, 330–344. [Google Scholar] [CrossRef]
- Pouncey, R.; Swanson, K.; Hart, K. ERDAS Field Guide; ERDAS Inc.: Reston, CA, USA, 1999. [Google Scholar]
- Rawat, J.S.; Biswas, V.; Kumar, M. Changes in land use/cover using geospatial techniques: A case study of Ramnagar town area, district Nainital, Uttarakhand, India. Egypt. J. Remote Sens. Space Sci. 2013, 16, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Li, C.; Wang, J.; Wang, L.; Hu, L.; Gong, P. Comparison of classification algorithms and training sample sizes in urban land classification with Landsat thematic mapper imagery. Remote Sens. 2014, 6, 964–983. [Google Scholar] [CrossRef] [Green Version]
- Bachri, I.; Hakdaoui, M.; Raji, M.; Teodoro, A.C.; Benbouziane, A. Machine learning algorithms for automatic lithological mapping using remote sensing data: A case study from Souk Arbaa Sahel, Sidi Ifni Inlier, Western Anti-Atlas, Morocco. ISPRS Int. J. Geo-Inf. 2019, 8, 248. [Google Scholar] [CrossRef] [Green Version]
- Rozenstein, O.; Karnieli, A. Comparison of methods for land-use classification incorporating remote sensing and GIS inputs. Appl. Geogr. 2011, 31, 533–544. [Google Scholar] [CrossRef]
- Jensen, K.; McDonald, K.; Podest, E.; Rodriguez-Alvarez, N.; Horna, V.; Steiner, N. Assessing L-band GNSS-reflectometry and imaging radar for detecting sub-canopy inundation dynamics in a tropical wetlands complex. Remote Sens. 2018, 10, 1431. [Google Scholar] [CrossRef] [Green Version]
- Griffith, D.A.; Wong, D.W. Modeling population density across major US cities: A polycentric spatial regression approach. J. Geogr. Syst. 2007, 9, 53–75. [Google Scholar] [CrossRef]
- Dismuke, C.; Lindrooth, R. Ordinary least squares. Methods Des. Outcomes Res. 2006, 93, 93–104. [Google Scholar]
- Ganasegeran, K.; Jamil, M.F.A.; Ch’ng, A.S.H.; Looi, I.; Peariasamy, K.M. Influence of population density for COVID-19 spread in Malaysia: An ecological study. Int. J. Environ. Res. Public Health 2021, 18, 9866. [Google Scholar] [CrossRef]
- Tenerelli, P.; Ehrlich, D. Analysis of built-up spatial pattern at different scales: Can scattering affect map accuracy? Int. J. Digit. Earth 2011, 4, 107–116. [Google Scholar] [CrossRef]
- Sabo, F.; Corbane, C.; Florczyk, A.J.; Ferri, S.; Pesaresi, M.; Kemper, T. Comparison of built-up area maps produced within the global human settlement framework. Trans. GIS 2018, 22, 1406–1436. [Google Scholar] [CrossRef]
- Urban, R.C.; Nakada, L.Y.K. GIS-based spatial modelling of COVID-19 death incidence in São Paulo, Brazil. Environ. Urban. 2021, 33, 229–238. [Google Scholar] [CrossRef]
- Rader, B.; Scarpino, S.V.; Nande, A.; Hill, A.L.; Adlam, B.; Reiner, R.C.; Pigott, D.M.; Gutierrez, B.; Zarebski, A.E.; Shrestha, M.; et al. Crowding and the shape of COVID-19 epidemics. Nat. Med. 2020, 26, 1829–1834. [Google Scholar] [CrossRef]
- Rader, B.; Nande, A.; Adlam, B.; Hill, A.L.; Reiner, R.C.; Pigott, D.M.; Bernardo, G. Crowding and the epidemic intensity of COVID-19 transmission. MedRxiv 2020, 26, 1829–1834. [Google Scholar]
- Şahin, M. Impact of weather on COVID-19 pandemic in Turkey. Sci. Total Environ. 2020, 728, 138810. [Google Scholar] [CrossRef]
- Smith, T.P.; Flaxman, S.; Gallinat, A.S.; Kinosian, S.P.; Stemkovski, M.; Unwin, H.J.T.; Watson, O.J.; Whittaker, C.; Cattarino, L.; Dorigatti, I.; et al. Temperature and population density influence SARS-CoV-2 transmission in the absence of nonpharmaceutical interventions. Proc. Natl. Acad. Sci. USA 2021, 118, e2019284118. [Google Scholar] [CrossRef]
- Souch, J.M.; Cossman, J.S.; Hayward, M.D. Interstates of Infection: Preliminary Investigations of Human Mobility Patterns in the COVID-19 Pandemic. J. Rural. Health 2021, 37, 266–271. [Google Scholar] [CrossRef]
- Garner, M.G.; Hamilton, S.A. Principles of epidemiological modelling. Rev. Sci. Tech.-OIE 2011, 30, 407. [Google Scholar] [CrossRef]
- Ruiqi, L.; Richmond, P.; Roehner, B.M. Effect of population density on epidemics. Phys. A Stat. Mech. Appl. 2018, 510, 713–724. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name | Totals | Totals | Correct | Accuracy | Accuracy |
|---|---|---|---|---|---|
| Class | Reference | Classified | Number | Producers | Users |
| Built-up area | 24 | 23 | 19 | 79.17% | 82.61% |
| Cloud | 9 | 3 | 3 | 33.33% | 100.00% |
| Commercial agriculture | 49 | 50 | 45 | 91.84% | 90.00% |
| Forest | 100 | 118 | 98 | 98.00% | 83.05% |
| Others agriculture | 32 | 33 | 28 | 87.50% | 84.85% |
| Paddy | 16 | 14 | 14 | 87.50% | 100.00% |
| Swamp forest | 15 | 9 | 9 | 60.00% | 100.00% |
| Waterbody | 11 | 6 | 6 | 54.55% | 100.00% |
| Total | 256 | 256 | 222 | ||
| Overall Classification Accuracy = 86.72% | |||||
| Correlations | |||
|---|---|---|---|
| Population_Density | Total_Infected | ||
| Population_Density | Pearson Correlation | 1 | 0.919 ** |
| Sig. (2-tailed) | 0.000 | ||
| N | 10 | 10 | |
| Total_Infected | Pearson Correlation | 0.919 ** | 1 |
| Sig. (2-tailed) | 0.000 | ||
| N | 10 | 10 | |
| Coefficients a | ||||||
|---|---|---|---|---|---|---|
| Model | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | ||
| B | Std. Error | Beta | ||||
| 1 | (Constant) | −43.244 | 19.003 | −2.276 | 0.052 | |
| Population_Density | 0.520 | 0.079 | 0.919 | 6.610 | 0.000 | |
| Model Summary | ||||
|---|---|---|---|---|
| Model | R | R Square | Adjusted R Square | Std. Error of the Estimate |
| 1 | 0.919 a | 0.845 | 0.826 | 36.40054 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nor, A.N.M.; Jamil, R.M.; Aziz, H.A.; Abas, M.A.; Hambali, K.A.; Hassin, N.H.; Abdul Karim, M.F.; Nawawi, S.A.; Amir, A.; Amaludin, N.A.; et al. Spatial Distribution of COVID-19 Infected Cases in Kelantan, Malaysia. Sustainability 2022, 14, 14150. https://doi.org/10.3390/su142114150
Nor ANM, Jamil RM, Aziz HA, Abas MA, Hambali KA, Hassin NH, Abdul Karim MF, Nawawi SA, Amir A, Amaludin NA, et al. Spatial Distribution of COVID-19 Infected Cases in Kelantan, Malaysia. Sustainability. 2022; 14(21):14150. https://doi.org/10.3390/su142114150
Chicago/Turabian StyleNor, Amal Najihah Muhamad, Rohazaini Muhammad Jamil, Hasifah Abdul Aziz, Muhamad Azahar Abas, Kamarul Ariffin Hambali, Nor Hizami Hassin, Muhammad Firdaus Abdul Karim, Siti Aisyah Nawawi, Aainaa Amir, Nazahatul Anis Amaludin, and et al. 2022. "Spatial Distribution of COVID-19 Infected Cases in Kelantan, Malaysia" Sustainability 14, no. 21: 14150. https://doi.org/10.3390/su142114150
APA StyleNor, A. N. M., Jamil, R. M., Aziz, H. A., Abas, M. A., Hambali, K. A., Hassin, N. H., Abdul Karim, M. F., Nawawi, S. A., Amir, A., Amaludin, N. A., Ibrahim, N., Yusoff, A. H., Malek, N. H. A., Rafaai, N. H., Mohd Hatta, S. K., & Grafius, D. (2022). Spatial Distribution of COVID-19 Infected Cases in Kelantan, Malaysia. Sustainability, 14(21), 14150. https://doi.org/10.3390/su142114150