
Healthcare Waste Generation Worldwide and Its Dependence on Socio-Economic and Environmental Factors



Abstract
:1. Introduction
2. Methodology
2.1. Materials
- GDP per capita (US $/capita). This is the gross domestic product (GDP) converted to dollars using purchasing power parity rates. GDP at purchaser’s prices is the sum of gross value added by all resident producers in the economy plus any product taxes and minus any subsidies not included in the value of the products [39]. Data were based on the 2015 calendar year.
- Health expenditure (HE) or healthcare spending per capita (US $/capita). Total health expenditure is the sum of public and private health expenditures. It is a percentage of the GDP and was expressed here in $ per capita [39]. Data were based on the 2014 calendar year.
- Human Development Index (HDI). The HDI was created to emphasize that people and their capabilities should be the ultimate criteria for assessing the development of a country, not economic growth alone. The Human Development Index (HDI) is a summary measure of average achievement in key dimensions of human development, i.e., a long and healthy life, being knowledgeable, and having a decent standard of living. The HDI does not reflect on inequalities, poverty, human security, empowerment, etc. [40]. Data were based on the 2014 calendar year.
- Inequality-adjusted Human Development Index (IHDI). The IHDI combines the country’s average achievements in health, education and income with how those achievements are distributed among the country’s population by “discounting” each dimension’s average value according to its level of inequality. Under perfect equality, the IHDI is equal to the HDI, but falls below the HDI when inequality rises [40]. Data were also based on the 2014 calendar year.
- Multidimensional Poverty Index (MPI). The index identifies the number of people who are multi-dimensionally poor and the number of deprivations with which poor households typically strive [40]. Note that MPI refers to developing countries only, since there are no relevant data for developed countries. Data were based on available values from different calendar years and were available for 21 countries only (European countries had no MPI).
- Life expectancy (LE) at birth (years). This is the number of years that a newborn infant could expect to live if prevailing patterns of age-specific mortality rates at the time of birth stay the same throughout the infant's life [40]. Data were based on the 2014 calendar year.
- Mean years of schooling. Average number of years of education received by people of ages 25 and older, converted from education attainment levels using official durations at each level [39]. Data were based on the 2014 calendar year.
- HIV prevalence, adult (% ages 15–49). Percentage of the population (at ages 15–49) who are living with HIV [40]. Data were based on the 2013 calendar year.
- Deaths due to tuberculosis (per 100,000 people). Number of deaths due to tuberculosis from confirmed and probable cases, expressed per 100,000 people [40]. Data were based on the 2012 calendar year.
- Deaths due to malaria (per 100,000 people). Number of deaths due to malaria from confirmed and probable cases, expressed per 100,000 people [40]. Data were based on the 2012 calendar year.
- Under-five mortality rate (per 1000 live births). Probability of dying between birth and the age of five, expressed per 1000 live births [40]. Data were based on the 2013 calendar year.
- CO2 emissions (annual metric tonnes per capita). Carbon dioxide emissions (CDE) are those stemming from the burning of fossil fuels and the manufacturing of cement. They include carbon dioxide produced during consumption of solid, liquid, and gas fuels and gas flaring [40]. According to Human Development Reports, there are eight indices which indicate the environmental sustainability for each country worldwide. One of them is CO2 emissions per capita, which was chosen as a representative environmental sustainability index. Data were based on the 2011 calendar year.
2.2. Methods
3. Results
3.1. Descriptive Statistics and Test of Normality
3.2. Correlations
3.3. Multiple Linear Regression Modeling
| HCWGR: | the Health-Care Waste Generation Rate in kg/bed/daye |
| Constant: | a constant in kg/bed/day. |
| a, b, c, …, n: | coefficients |
| X1, X2, …., Xn: | independent variables (predictors). Eight of the twelve parameters (health expenditure, HDI, CDE, LE, schooling years, tuberculosis induced deaths, malaria induced deaths, under-five mortality rate) were used during modeling. |
| LE: | Life expectancy (in years), |
| HDI: | Human Development Index, as defined earlier, |
| SCH_Y: | Mean years of schooling (years), and |
| CDE: | CO2 emissions in tonnes per capita per year. |
4. Discussion and Conclusions
- The practical application of the work is that certain socio-economic and environmental indices per country can be used to mathematically predict HCWGR so as to avoid direct and costly HCW weight measurements.
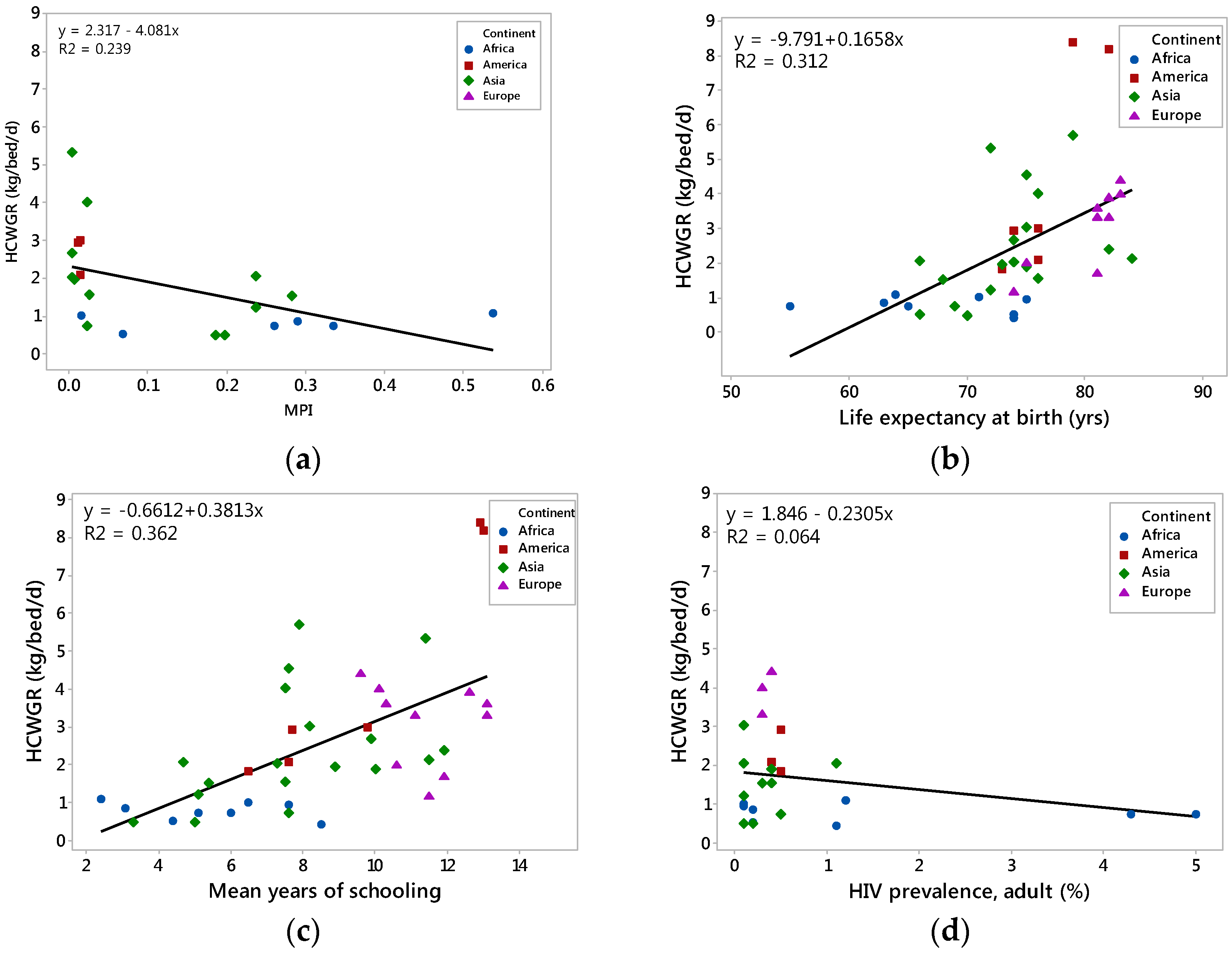
- A positive correlation between HCWGR and seven of the twelve indices (GDP, HE, HDI, IHDI, life expectancy, mean years of schooling, and CDE) was observed.
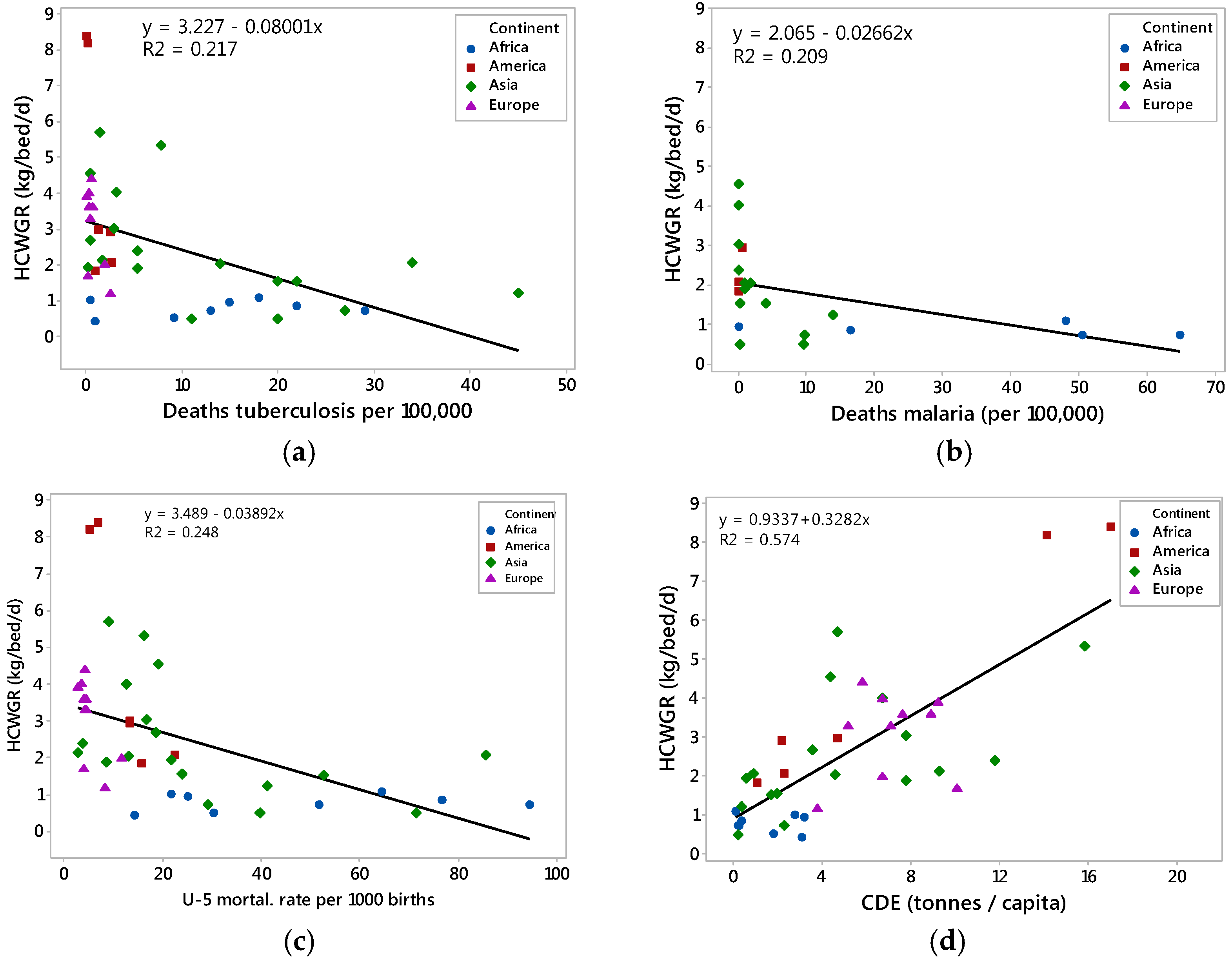
- A negative correlation between HCWGR generation rate and four of the twelve indices (MPI, HIV prevalence, deaths due to tuberculosis, deaths due to malaria, and U-5 mortality rate) was observed.
- Using the Pearson and Spearman correlation coefficients, it was found that the HIV prevalence was not a statistically significant predictor of the HCWGR.
- Based on multiple linear regression modeling, the resulting best reduced model indicated that life expectancy and carbon dioxide emissions positively affect healthcare waste generation and can be used as predictors to adequately describe HCWGR (see Equation (2)). The resulting empirical multiple regression model explained 85% of the variability of the response. Two additional models, Equations (3) and (4), showed that HDI and mean years of schooling can be also used as HCWGR predictors.
- The annual CO2 emissions was the index that affected the HCWGR the most.
- More factors should be investigated in future work to try to augment and validate the proposed regression model and to incorporate principal component analysis to separate and group the significant predictors. In addition, efforts should be made to distinguish the hazardous fraction from the total HCW and to develop similar modeling with the former fraction as well.
Author Contributions
Conflicts of Interest
References
- World Health Organization (WHO). Available online: http://www.who.int/mediacentre/factsheets/fs253/en/ (accessed on 19 November 2016).
- Komilis, D. Issues on medical waste management research. Waste Manag. 2016, 48, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Patwary, M.A.; O’Hare, W.T.; Street, G.; Elahi, K.M.; Hossain, S.S.; Sarker, M.H. Quantitative assessment of medical waste generation in the capital city of Bangladesh. Waste Manag. 2009, 29, 2392–2397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pruss, A.; Giroult, E.; Rushbrook, P. Safe Management of Wastes from Health-Care Activities; World Health Organization: Geneva, Switzerland, 1999. [Google Scholar]
- Mbongwe, B.; Mmereki, B.T.; Magashula, A. Healthcare waste management: Current practices in selected healthcare facilities, Botswana. Waste Manag. 2008, 28, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Canadian Senate Committee. Part VII: Financing Reform. In The Health of Canadians; Parliament of Canada: Ottawa, ON, Canada, 2002. [Google Scholar]
- Windfeld, E.S.; Brooks, M.S. Medical waste management—A review. J. Environ. Manag. 2015, 163, 98–108. [Google Scholar] [CrossRef] [PubMed]
- Karpusenkaite, A.; Ruzgas, T.; Denafas, G. Forecasting medical waste generation using short and extra short datasets: Case study of Lithuania. Waste Manag. Res. 2016, 34, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Bendjoudi, Z.; Taleb, F.; Abdelmalek, F.; Addou, A. Healthcare waste management in Algeria and Mostaganem department. Waste Manag. 2009, 29, 1383–1387. [Google Scholar] [CrossRef] [PubMed]
- Mohee, R. Medical wastes characterization in healthcare institutions of Mauritius. Waste Manag. 2005, 25, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Manga, E.V.; Forton, O.T.; Mofor , A.L.; Woodard, R. Health care waste management in Cameroon: A case study from the Southwestern Region. Resour. Conserv. Recycl. 2011, 57, 108–116. [Google Scholar] [CrossRef]
- Mbarki, A.; Kabbachi, B.; Ezaidi, A.; Benssaou, M. Medical waste management: A case study of the souss-massa-draa region, morocco. J. Environ. Prot. 2013, 4, 914–919. [Google Scholar] [CrossRef]
- Abd El-Salam, M.M. Hospital waste management in El-Beheira Governorate, Egypt. J. Environ. Manag. 2010, 91, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Shouman, E.; Al Bazedi, G.; Sohour, M.H.; Abulnour, A.G. Management of hazardous medical waste treatment in Egypt. World Appl. Sci. J. 2013, 28, 804–808. [Google Scholar]
- Suhair, A.; Gayoum, S. Management of hospital solid waste in Khartoum State. Environ. Monit. Assess. 2013, 185, 8567–8582. [Google Scholar]
- Tesfahun, E.; Kumie, A.; Beyene, A. Developing models for the prediction of hospital healthcare waste generation rate. Waste Manag. Res. 2015, 34, 219–220. [Google Scholar] [CrossRef] [PubMed]
- Eker, H.H.; Bilgili, M.S. Statistical analysis of waste generation in healthcare services: A case study. Waste Manag. Res. 2011, 29, 791–796. [Google Scholar] [CrossRef] [PubMed]
- Kagonji, I.S.; Manyele, S.V. Analysis of the measured medical waste generation rate in Tanzanian district hospitals using statistical methods. Afr. J. Environ. Sci. Technol. 2011, 5, 815–833. [Google Scholar]
- Kaisar Alam Sarkar, M.S.; Haque, M.A.; Khan, T.A. Hospital waste management in Sylhet city. J. Eng. Appl. Sci. 2006, 1, 32–40. [Google Scholar]
- Rabeie, O.L.; Miranzadeh, M.B.; Fallah, S.H.; Dehqan, S.; Moulana, Z.; Amouei, A.; Mohammadi, A.A.; Asgharnia, H.A.; Babaei, M. Determination of Hospital Waste Composition and Management in Amol City, Iran. Health Scope 2012, 1, 127–131. [Google Scholar] [CrossRef]
- Yong, Z.; Gang, X.; Guanxing, W.; Tao, Z.; Dawei, J. Medical waste management in China: A case study of Nanjing. Waste Manag. 2009, 29, 1376–1382. [Google Scholar] [CrossRef] [PubMed]
- Gai, R.; Kuroiwa, C.; Xu, L.; Wang, X.; Zhang, Y.; Li, H.; Zou, C.; He, J.; Tang, W. Hospital medical waste management in Shandong Province, China. Waste Manag. Res. 2009, 27, 336–342. [Google Scholar] [PubMed]
- Patil, A.D.; Shekdar, A.V. Health-care waste management in India. J. Environ. Manag. 2001, 63, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Eleyan, D.; Al-Khatib Issam, A.; Garfield, J. System dynamics model for hospital waste characterization and generation in developing countries. Waste Manag. Res. 2013, 31, 986–995. [Google Scholar] [CrossRef] [PubMed]
- Ananth, A.P.; Prashanthini, V.; Visvanathan, C. Healthcare waste management in Asia. Waste Manag. 2010, 30, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Suwannee, A. Study on waste from hospital and clinics in Phitsanulok. Online J. Health Allied Sci. 2002, 1, 6–14. [Google Scholar]
- Bazrafshan, E.; Mostafapoor, F.K. Survey of medical waste characterization and management in Iran: A case study of Sistan and Baluchestan Province. Waste Manag. Res. 2011, 29, 442–450. [Google Scholar] [CrossRef] [PubMed]
- Phengxay, S.; Okumura, J.; Miyoshi, M.; Sakisaka, K.; Kuroiwa, C. Health-care waste management in Lao PDR: a case study. Waste Manag. Res. 2005, 23, 571–581. [Google Scholar] [CrossRef] [PubMed]
- Maamari, O.; Brandam, C.; Lteif, R.; Salameh, D. Health care waste generation rates and patterns: The case of Lebanon. Waste Mang. 2015, 43, 550–554. [Google Scholar] [CrossRef] [PubMed]
- Jang, Y.C.; Lee, C.; Yoon, O.S.; Kim, H. Medical waste management in Korea. J. Environ. Manag. 2006, 80, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Gusca, J.; Kalnins, S.A.; Blumberga, D.; Bozhko, L.; Khabdullina, Z.; Khabdullin, A. Assessment method of healthcare waste generation in Latvia and Kazakhstan. Energy Procedia 2015, 72, 175–179. [Google Scholar] [CrossRef]
- Nguyen, D.L.; Bui, X.T.; Nguyen, T.H. Estimation of Current and Future Generation of Medical Solid Wastes in Hanoi City, Vietnam. Int. J. Waste Resour. 2014, 4, 139. [Google Scholar] [CrossRef]
- Diaz, L.F.; Eggerth, L.L.; Enkhtsetseg, S. Anejo de Residuos de Establecimientos de Salud en Guayaquil, Ecuador; Pan American Health Organization: Quito, Equador, 2001. [Google Scholar]
- Da Silva, C.E.; Hoppe, A.E.; Ravanello, M.; Mello, N. Medical wastes management in the south of Brazil. Waste Manag. 2005, 25, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Hossain, S.; Santhanam, A.; Nik Norulaini, N.A.; Mohd Omar, M.K. Clinical solid waste management practices and its impact on human health and environment—A review. Waste Manag. 2011, 31, 754–766. [Google Scholar] [CrossRef] [PubMed]
- Johnson, M.K.; Gonzalez, L.M.; Duenas, L.; Gamero, M.; Relyea, G.; Luque, E.L.; Caniza, A.M. Improving waste segregation while reducing costs in a tertiary-care hospital in a lower-middle income country in Central America. Waste Manag. Res. 2013, 31, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Farzadkia, M.; Emamjomeh, M.M.; Golbaz, S.; Sajadi, H.S. An investigation in hospital solid waste management in Iran. Glob. NEST J. 2015, 17, 771–783. [Google Scholar]
- Komilis, D.; Fouki, A.; Papadopoulos, D. Hazardous medical waste generation rates of different categories of health-care facilities. Waste Manag. 2012, 32, 1434–1441. [Google Scholar] [CrossRef] [PubMed]
- World Bank. Available online: http://data.worldbank.org/ (accessed on 23 July 2016).
- Human Development Reports. Available online: http://hdr.undp.org/en/countries (accessed on 15 October 2016).
- Berthouex, P.M.; Brown, L. Statistics for Environmental Engineers, 2nd ed.; Lewis Publishers: New York, NY, USA, 2002. [Google Scholar]
- Chung, J.W.; Meltzer, D.O. Estimate of the carbon footprint of the US health care sector. J. Am. Med. Assoc. 2009, 302, 1967–1972. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
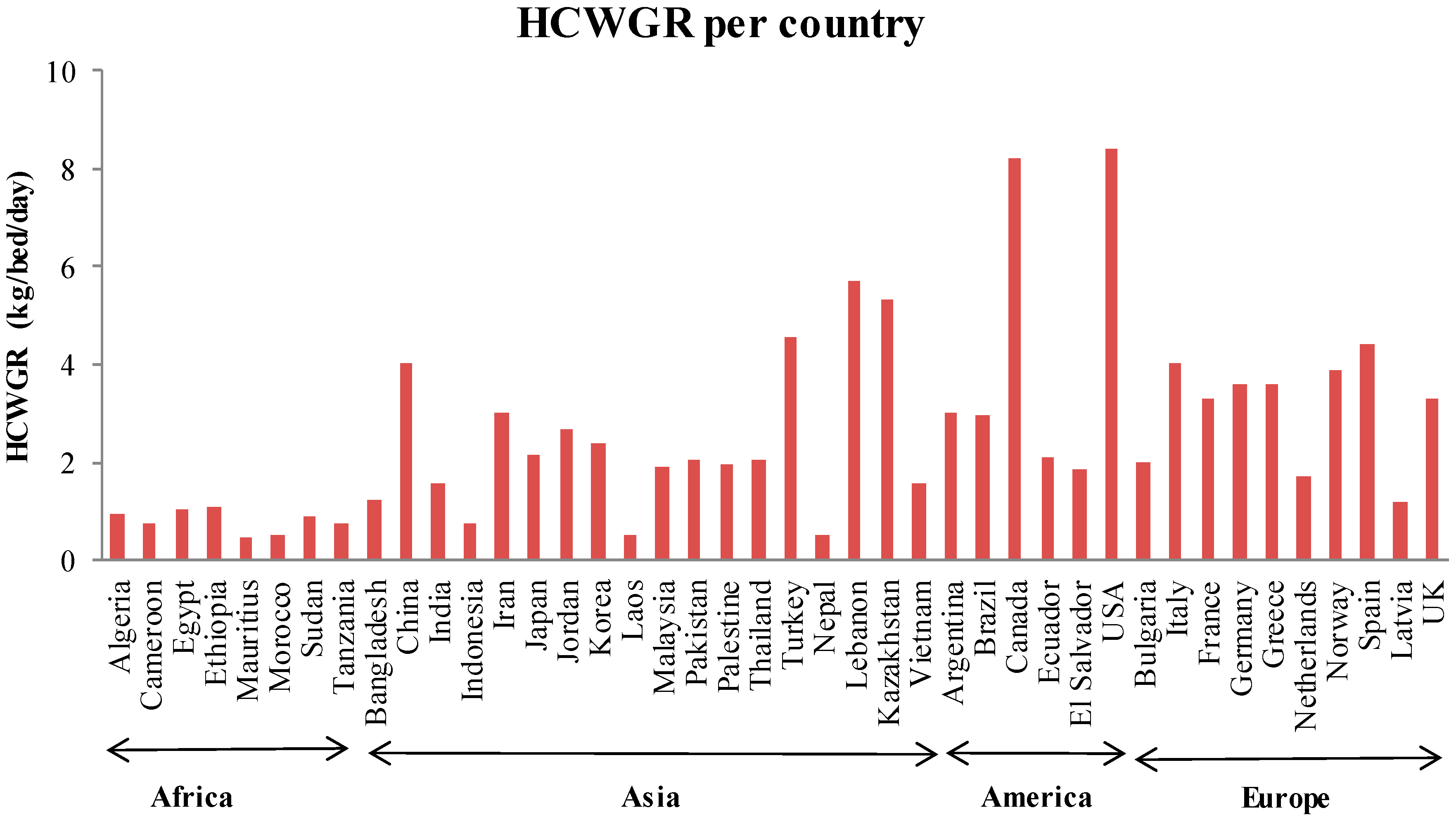
| Country | HCWGR (kg/Bed/Day) | References | Country | HCWGR (kg/Bed/Day) | References | |
|---|---|---|---|---|---|---|
| Africa | Algeria | 0.96 | [9] | Mauritius | 0.44 | [10] |
| Cameroon | 0.55 | [11] | Morocco | 0.53 | [12] | |
| Egypt | 1.03 | [13,14] | Sudan | 0.87 | [15] | |
| Ethiopia | 1.1 | [16] | Tanzania | 0.75 | [17,18] | |
| Asia | Bangladesh | 1.24 | [3,19,20] | Malaysia | 1.9 | [20] |
| China | 4.03 | [21,22] | Pakistan | 2.07 | [7] | |
| India | 1.55 | [20,23] | Palestine | 2.02 | [24] | |
| Indonesia | 0.75 | [25] | Thailand | 2.05 | [26] | |
| Iran | 3.04 | [20,27] | Turkey | 4.55 | [17,28] | |
| Japan | 2.15 | [10,17] | Nepal | 0.5 | [20] | |
| Jordan | 2.69 | [17] | Lebanon | 5.7 | [29] | |
| Korea | 2.4 | [30] | Kazakhstan | 5.34 | [31] | |
| Laos | 0.51 | [28] | Vietnam | 1.57 | [20,32] | |
| America | Argentina | 3 | [4] | Ecuador | 2.09 | [33] |
| Brazil | 2.94 | [34,35] | El Salvador | 1.85 | [36] | |
| Canada | 8.2 | [35] | USA | 8.4 | [7,17,35] | |
| Europe | Bulgaria | 2 | [7] | Netherlands | 1.7 | [37] |
| Italy | 4 | [17] | Norway | 3.9 | [7] | |
| France | 3.3 | [7] | Spain | 4.4 | [7] | |
| Germany | 3.6 | [37] | Latvia | 1.18 | [31] | |
| Greece | 3.6 | [38] | UK | 3.3 | [7] |
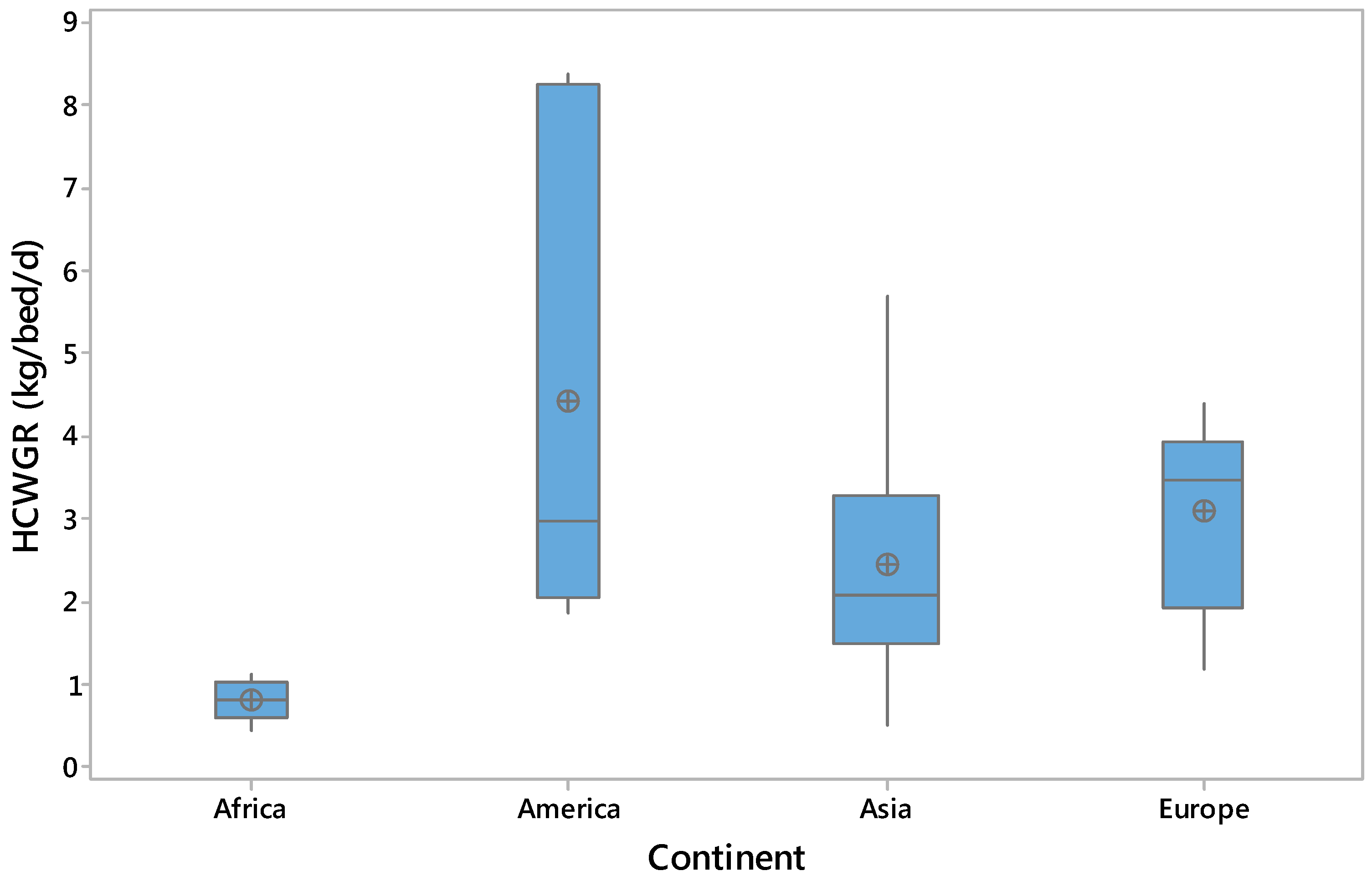
| Continent | Mean ± St. Dev. | Sample Size | Anderson-Darling (AD) Value | p of the AD Normality Test |
|---|---|---|---|---|
| Africa | 0.80 ± 0.23 | 8 | 0.223 | 0.738 |
| America | 4.41 ± 3.0 | 6 | 0.722 | 0.028 |
| Asia | 2.44 ± 1.5 | 18 | 0.664 | 0.069 |
| Europe | 3.10 ± 1.1 | 10 | 0.577 | 0.099 |
| All data | 2.57 ± 1.89 | 42 | 1.338 | <0.005 |
| Index Correlated with HCWGR | Africa | America | Asia | Europe | Overall |
|---|---|---|---|---|---|
| GDP | ns, [ns] n = 8 | 0.985 [1.000] n = 6 | ns, [0.688] n = 18 | ns, [ns] n = 10 | 0.592 [0.699] n = 42 |
| HE | ns, [ns] n = 8 | 0.939 [0.943] n = 6 | ns, [0.725] n = 17 | ns, [ns] n = 10 | 0.599 [0.687] n = 41 |
| HDI | ns, [ns] n = 8 | ns [1.000] n = 6 | ns, [0.678] n = 18 | ns, [ns] n = 10 | 0.612 [0.671] n = 42 |
| IHDI | ns, [ns] n = 6 | ns, [ns] n = 6 | ns, [0.656] n = 16 | ns, [ns] n = 10 | 0.576 [0.652] n = 38 |
| MPI | ns, [ns] n = 6 | ns, [ns] n = 3 | ns, [ns] n = 12 | n = 0 | ns [−0.616] n = 21 |
| LE | ns, [ns] n = 8 | ns, [ns] n = 6 | ns, [ns] n = 18 | 0.824 [0.840] n = 10 | 0.559 [0.687] n = 42 |
| Mean years of schooling | ns, [ns] n = 8 | 0.959 [0.943] n = 6 | ns, [ns] n = 18 | ns, [ns] n = 10 | 0.601 [0.633] n = 42 |
| HIV prevalence | ns, [ns] n = 8 | ns, [ns] n = 3 | ns, [ns] n = 10 | ns, [ns] n = 3 | ns, [ns] n = 24 |
| Deaths tuberculosis | ns, [ns] n = 8 | ns, [ns] n = 6 | ns, [−0.635] n = 18 | ns, [ns] n = 10 | −0.466 [−0.596] n = 42 |
| Deaths malaria | ns, [ns] n = 5 | ns, [ns] n = 3 | ns, [−0.728] n = 13 | n = 0 | ns [−0.656] n = 21 |
| U-5 mortal. rate | ns, [ns] n = 8 | ns, [ns] n = 6 | ns, [-0.604] n = 18 | ns, [ns] n = 10 | −0.498 [−0.650] n = 42 |
| CDE | ns, [ns] n = 8 | 0.987 [0.943] n = 6 | ns, [0.718] n = 18 | ns, [ns] n = 10 | 0.758 [0.727] n = 42 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minoglou, M.; Gerassimidou, S.; Komilis, D. Healthcare Waste Generation Worldwide and Its Dependence on Socio-Economic and Environmental Factors. Sustainability 2017, 9, 220. https://doi.org/10.3390/su9020220
Minoglou M, Gerassimidou S, Komilis D. Healthcare Waste Generation Worldwide and Its Dependence on Socio-Economic and Environmental Factors. Sustainability. 2017; 9(2):220. https://doi.org/10.3390/su9020220
Chicago/Turabian StyleMinoglou, Minas, Spyridoula Gerassimidou, and Dimitrios Komilis. 2017. "Healthcare Waste Generation Worldwide and Its Dependence on Socio-Economic and Environmental Factors" Sustainability 9, no. 2: 220. https://doi.org/10.3390/su9020220
APA StyleMinoglou, M., Gerassimidou, S., & Komilis, D. (2017). Healthcare Waste Generation Worldwide and Its Dependence on Socio-Economic and Environmental Factors. Sustainability, 9(2), 220. https://doi.org/10.3390/su9020220