Incobotulinumtoxin A for Sialorrhea in Neurological Disorders: A Real-Life Experience

 , and
, and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Conclusions
5. Materials and Methods
Author Contributions
Conflicts of Interest
References
- Porta, M.; Gamba, M.; Bertacchi, G.; Vaj, P. Treatment of sialorrhoea with ultrasound guided botulinum toxin type A injection in patients with neurological disorders. J. Neurol. Neurosurg. Psychiatry 2001, 70, 538–540. [Google Scholar] [CrossRef] [PubMed]
- Kalf, J.G.; De Swart, B.J.M.; Borm, G.F.; Bloem, B.R.; Munneke, M. Prevalence and definition of drooling in Parkinson’s disease: A systematic review. J. Neurol. 2009, 256, 1391–1396. [Google Scholar] [CrossRef] [PubMed]
- Politis, M.; Wu, K.; Molloy, S.; Bain, P.G.; Chaudhuri, K.R.; Piccini, P. Parkinson’s disease symptoms: The patient’s perspective. Mov. Disord. 2010, 25, 1646–1651. [Google Scholar] [CrossRef] [PubMed]
- Lakraj, A.A.; Moghimi, N.; Jabbari, B. Sialorrhea: Anatomy, pathophysiology and treatment with emphasis on the role of botulinum toxins. Toxins 2013, 5, 1010–1031. [Google Scholar] [CrossRef] [PubMed]
- Srivanitchapoom, P.; Pandey, S.; Hallett, M. Drooling in Parkinson’s disease: A review. Parkinsonism Relat. Disord. 2014, 20, 1109–1118. [Google Scholar] [CrossRef] [PubMed]
- Proulx, M.; de Courval, F.P.; Wiseman, M.A.; Panisset, M. Salivary production in Parkinson’s disease. Mov. Disord. 2005, 20, 204–207. [Google Scholar] [CrossRef] [PubMed]
- Nóbrega, A.C.; Rodrigues, B.; Torres, A.C.; Scarpel, R.D.; Neves, C.A.; Melo, A. Is drooling secondary to a swallowing disorder in patients with Parkinson’s disease? Parkinsonism Relat. Disord. 2008, 14, 243–245. [Google Scholar] [CrossRef] [PubMed]
- Merelh, M. Sialorrhoea and Drooling in Patients with Parkinson. Drugs Ageing 2008, 25, 1007–1020. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, B.; Nóbrega, A.C.; Sampaio, M.; Argolo, N.; Melo, A. Silent saliva aspiration in Parkinson’s disease. Mov. Disord. 2011, 26, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Nóbrega, A.C.; Rodrigues, B.; Melo, A. Is silent aspiration a risk factor for respiratory infection in Parkinson’s disease patients? Parkinsonism Relat. Disord. 2008, 14, 646–648. [Google Scholar] [CrossRef] [PubMed]
- Kalf, J.G.; Smit, A.M.; Bloem, B.R.; Zwarts, M.J.; Munneke, M. Impact of drooling in Parkinson’s disease. J. Neurol. 2007, 254, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Tan, E.K. Botulinum Toxin Treatment of Sialorrhea: Comparing Different Therapeutic Preparations. Eur. J. Neurol. 2006, 13 (Suppl. 1), 60–64. [Google Scholar] [CrossRef] [PubMed]
- Lagalla, G.; Millevolte, M.; Capecci, M.; Provinciali, L.; Ceravolo, M.G. Botulinum toxin type A for drooling in Parkinson’s disease: A double-blind, randomized, placebo-controlled study. Mov. Disord. 2006, 21, 704–707. [Google Scholar] [CrossRef] [PubMed]
- Sillanpaä, S.; Sipilä, M.; Numminen, J.; Rautiainen, M. The Experience of Treating Drooling with Repeated Botulinum Toxin Injections. ORL J. Otorhinolaryngol. Relat. Spec. 2015, 77, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Mazlan, M.; Rajasegaran, S.; Engkasan, J.P.; Nawawi, O.; Goh, K.J.; Freddy, S.J. A double-blind randomized controlled trial investigating the most efficacious dose of botulinum toxin-A for sialorrhea treatment in asian adults with neurological diseases. Toxins 2015, 7, 3758–3770. [Google Scholar] [CrossRef] [PubMed]
- Weikamp, J.G.; Schinagl, D.A.X.; Verstappen, C.C.P.; Schelhaas, H.J.; de Swart, B.J.M.; Kalf, J.G. Botulinum toxin-A injections vs. radiotherapy for drooling in ALS. Acta Neurol. Scand. 2016, 134, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Chinnapongse, R.; Gullo, K.; Nemeth, P.; Zhang, Y.; Griggs, L. Safety and efficacy of botulinum toxin type B for treatment of sialorrhea in Parkinson’s disease: A prospective double-blind trial. Mov. Disord. 2012, 27, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Ondo, W.G.; Hunter, C.; Moore, W. A double-blind placebo-controlled trial of botulinum toxin B for sialorrhea in Parkinson’s disease. Neurology 2004, 62, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Lagalla, G.; Millevolte, M.; Capecci, M.; Provinciali, L.; Ceravolo, M.G. Long-lasting benefits of botulinum toxin type B in Parkinson’s disease-related drooling. J. Neurol. 2009, 256, 563–567. [Google Scholar] [CrossRef] [PubMed]
- Guidubaldi, A.; Fasano, A.; Ialongo, T.; Piano, C.; Pompili, M.; Mascianà, R.; Siciliani, L.; Sabatelli, M.; Bentivoglio, A.R. Botulinum toxin A versus B in sialorrhea: A prospective, randomized, double-blind, crossover pilot study in patients with amyotrophic lateral sclerosis or Parkinson’s disease. Mov. Disord. 2011, 26, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Sridharan, K.; Sivaramakrishnan, G. Pharmacological interventions for treating sialorrhea associated with neurological disorders: A mixed treatment network meta-analysis of randomized controlled trials. J. Clin. Neurosci. 2018. [Google Scholar] [CrossRef] [PubMed]
- Dressler, D. Five-year experience with incobotulinumtoxinA (Xeomin(®)): The first botulinum toxin drug free of complexing proteins. Eur. J. Neurol. 2012, 19, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Dressler, D.; Bigalke, H. Long-term stability of reconstituted incobotulinumtoxinA: How can we reduce costs of botulinum toxin therapy? J. Neural. Transm. 2017, 124, 1223–1225. [Google Scholar] [CrossRef] [PubMed]
- Dressler, D. Routine use of Xeomin in patients previously treated with Botox: Long term results. Eur. J. Neurol. 2009, 16 (Suppl. 2), 2–5. Available online: http://www.ncbi.nlm.nih.gov/pubmed/20002739 (accessed on 30 April 2018). [CrossRef] [PubMed]
- Jost, W.H.; Benecke, R.; Hauschke, D.; Jankovic, J.; Kaňovský, P.; Roggenkämper, P.; Simpson, D.M.; Comella, C.L. Clinical and pharmacological properties of incobotulinumtoxina and its use in neurological disorders. Drug Des. Dev. Ther. 2015, 9, 1913–1926. [Google Scholar] [CrossRef] [PubMed]
- Dressler, D.; Rychlik, R.; Kreimendahl, F.; Schnur, N.; Lambert-Baumann, J. Long-term efficacy and safety of incobotulinumtoxinA and conventional treatment of poststroke arm spasticity: A prospective, non-interventional, open-label, parallel-group study. BMJ Open 2015, 5, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Restivo, D.A.; Panebianco, M.; Casabona, A.; Lanza, S.; Marchese-Ragona, R.; Patti, F.; Masiero, S.; Biondi, A.; Quartarone, A. Botulinum toxin a for sialorrhoea associated with neurological disorders: Evaluation of the relationship between effect of treatment and the number of glands treated. Toxins 2018, 10, 55. [Google Scholar] [CrossRef] [PubMed]
- Narayanaswami, P.; Geisbush, T.; Tarulli, A.; Raynor, E.; Gautam, S.; Tarsy, D.; Gronseth, G. Drooling in Parkinson’s disease: A randomized controlled trial of incobotulinum toxin A and meta-analysis of Botulinum toxins. Parkinsonism Relat. Disord. 2016, 30, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Benecke, R.; Jost, W.H.; Kanovsky, P.; Ruzicka, E.; Comes, G.; Grafe, S. A new botulinum toxin type A free of complexing proteins for treatment of cervical dystonia. Neurology 2005, 64, 1949–1951. [Google Scholar] [CrossRef] [PubMed]
- Roggenkämper, P.; Jost, W.H.; Bihari, K.; Comes, G.; Grafe, S. Efficacy and safety of a new Botulinum Toxin Type A free of complexing proteins in the treatment of blepharospasm. J. Neural. Transm. 2006, 113, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Akulov, M.A.; Orlova, O.R.; Orlova, A.S.; Usachev, D.J.; Shimansky, V.N.; Tanjashin, S.V.; Khatkova, S.E.; Yunosha-Shanyavskaya, A.V. IncobotulinumtoxinA treatment of facial nerve palsy after neurosurgery. J. Neurol. Sci. 2017, 381, 130–134. [Google Scholar] [CrossRef] [PubMed]
- Proctor, G.B. The physiology of salivary secretion. Periodontology 2016, 70, 11–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mancini, F.; Zangaglia, R.; Cristina, S.; Sommaruga, M.G.; Martignoni, E.; Nappi, G.; Pacchetti, C. Double-blind, placebo-controlled study to evaluate the efficacy and safety of botulinum toxin type A in the treatment of drooling in parkinsonism. Mov. Disord. 2003, 18, 685–688. [Google Scholar] [CrossRef] [PubMed]
- Savarese, R.; Diamond, M.; Elovic, E.; Millis, S.R. Intraparotid Injection of Botulinum Toxin A as a Treatment to Control Sialorrhea in Children with Cerebral Palsy. Am. J. Phys. Med. Rehabil. 2004, 83, 304–311. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic characteristics | Mean ± SD/N (%) |
| Age | 71.1 ± 17.9 years |
| Sex, male | 23 (63.9%) |
| Previous treatment with other BoNT | 5 (13.9%) |
| Botulinum toxin B | 3 (8.3%) |
| Onabotulinumtoxin A | 2 (5.6%) |
| Clinical diagnosis | N (%) |
| Parkinson’s disease | 21 (58.3%) |
| Atypical Parkinsonism | 6 (16.7%) |
| Encephalopathy | 5 (13.9%) |
| Post-traumatic encephalopathy | 2 (5.6%) |
| Connatal encephalopathy | 2 (5.6%) |
| Epileptic encephalopathy | 1 (2.8%) |
| Alzheimer’s disease | 2 (5.6%) |
| Cerebrovascular disease | 1 (2.8%) |
| Huntington’s disease | 1 (2.8%) |
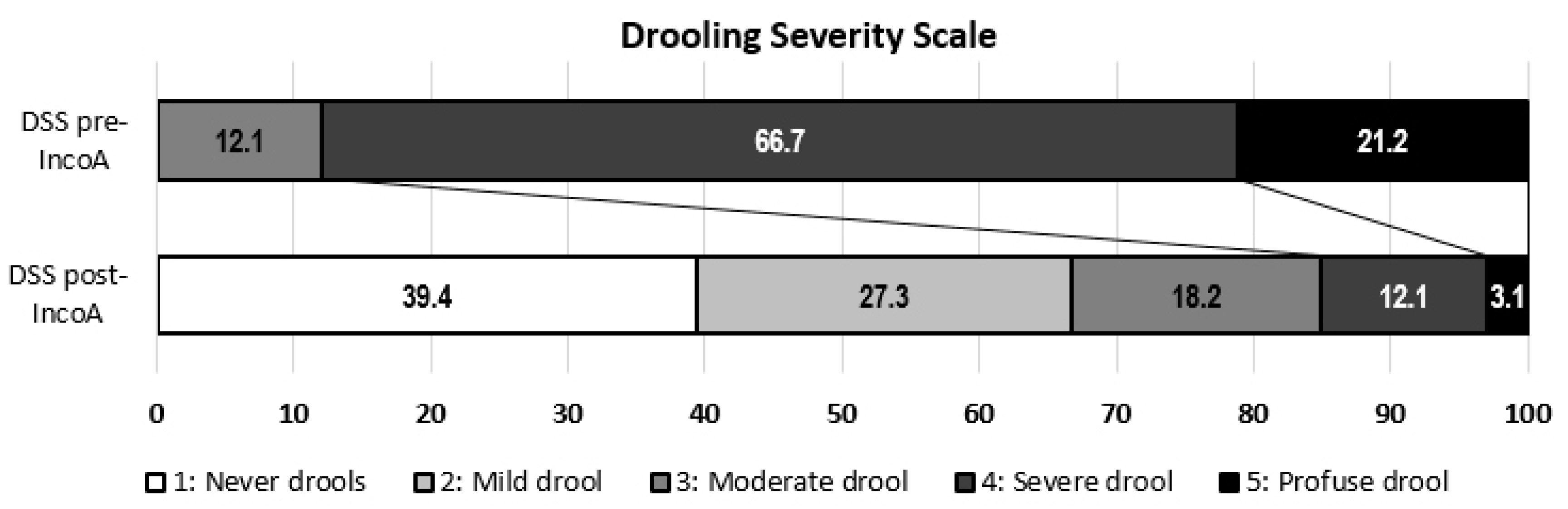
| Severity | |
| 1 | Dry (never drools) |
| 2 | Mild drooling, only lips wet |
| 3 | Moderate drooling, drool reaches the lips and the chin |
| 4 | Severe drooling; drool drips off chin and onto clothing |
| 5 | Profuse drooling, drooling off the body and onto objects |
| Frequency | |
| 1 | No drooling |
| 2 | Occasionally drools |
| 3 | Frequently drools |
| 4 | Constant drooling |
| 1 | Very much improved |
| 2 | Much improved |
| 3 | Minimally improved |
| 4 | No change |
| 5 | Minimally worse |
| 6 | Much worse |
| 7 | Very much worse |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martínez-Poles, J.; Nedkova-Hristova, V.; Escribano-Paredes, J.B.; García-Madrona, S.; Natera-Villalba, E.; Estévez-Fraga, C.; López-Sendón Moreno, J.L.; Avilés-Olmos, I.; Sánchez Díaz, G.; Martínez Castrillo, J.C.; et al. Incobotulinumtoxin A for Sialorrhea in Neurological Disorders: A Real-Life Experience. Toxins 2018, 10, 217. https://doi.org/10.3390/toxins10060217
Martínez-Poles J, Nedkova-Hristova V, Escribano-Paredes JB, García-Madrona S, Natera-Villalba E, Estévez-Fraga C, López-Sendón Moreno JL, Avilés-Olmos I, Sánchez Díaz G, Martínez Castrillo JC, et al. Incobotulinumtoxin A for Sialorrhea in Neurological Disorders: A Real-Life Experience. Toxins. 2018; 10(6):217. https://doi.org/10.3390/toxins10060217
Chicago/Turabian StyleMartínez-Poles, Javier, Velina Nedkova-Hristova, José Bernardo Escribano-Paredes, Sebastián García-Madrona, Elena Natera-Villalba, Carlos Estévez-Fraga, José Luis López-Sendón Moreno, Icíar Avilés-Olmos, Gema Sánchez Díaz, Juan Carlos Martínez Castrillo, and et al. 2018. "Incobotulinumtoxin A for Sialorrhea in Neurological Disorders: A Real-Life Experience" Toxins 10, no. 6: 217. https://doi.org/10.3390/toxins10060217
APA StyleMartínez-Poles, J., Nedkova-Hristova, V., Escribano-Paredes, J. B., García-Madrona, S., Natera-Villalba, E., Estévez-Fraga, C., López-Sendón Moreno, J. L., Avilés-Olmos, I., Sánchez Díaz, G., Martínez Castrillo, J. C., & Alonso-Canovas, A. (2018). Incobotulinumtoxin A for Sialorrhea in Neurological Disorders: A Real-Life Experience. Toxins, 10(6), 217. https://doi.org/10.3390/toxins10060217