Botulinum Toxin Type A Injections Impact Hamstring Muscles and Gait Parameters in Children with Flexed Knee Gait


Abstract
:1. Introduction
2. Results
2.1. Clinical and Functional Evaluations
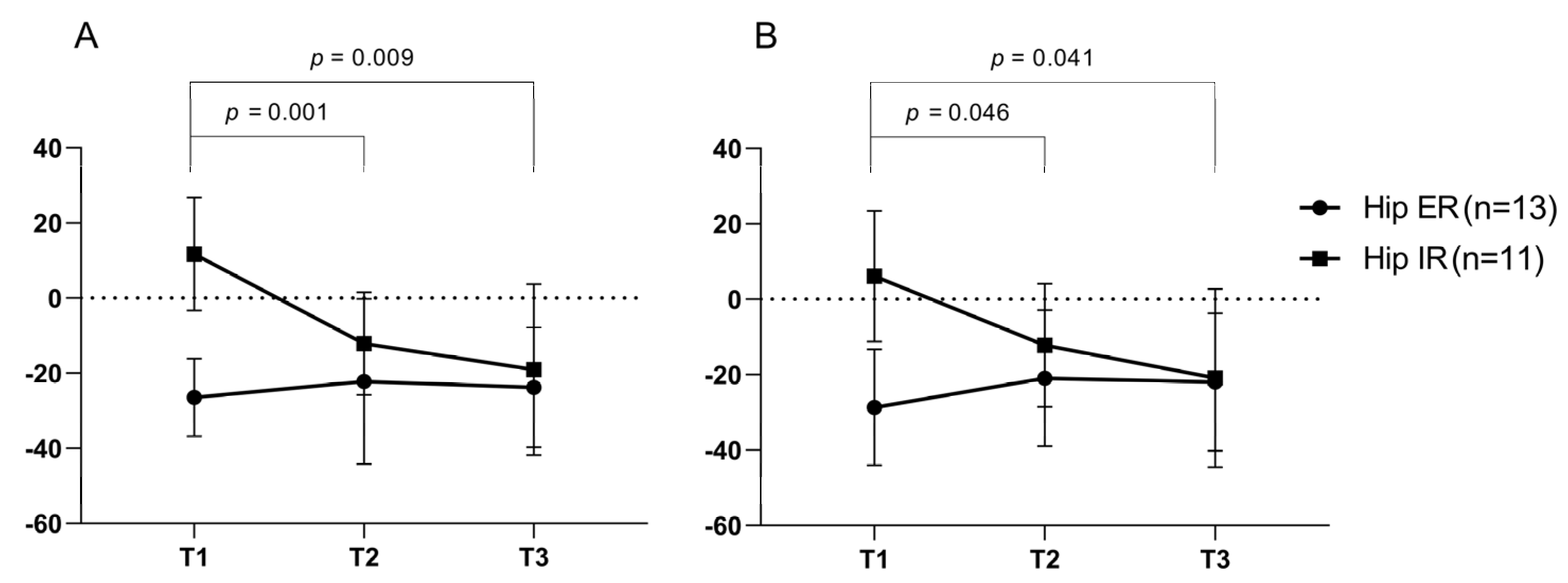
2.2. Gait Analysis Using a Computerized Gait System
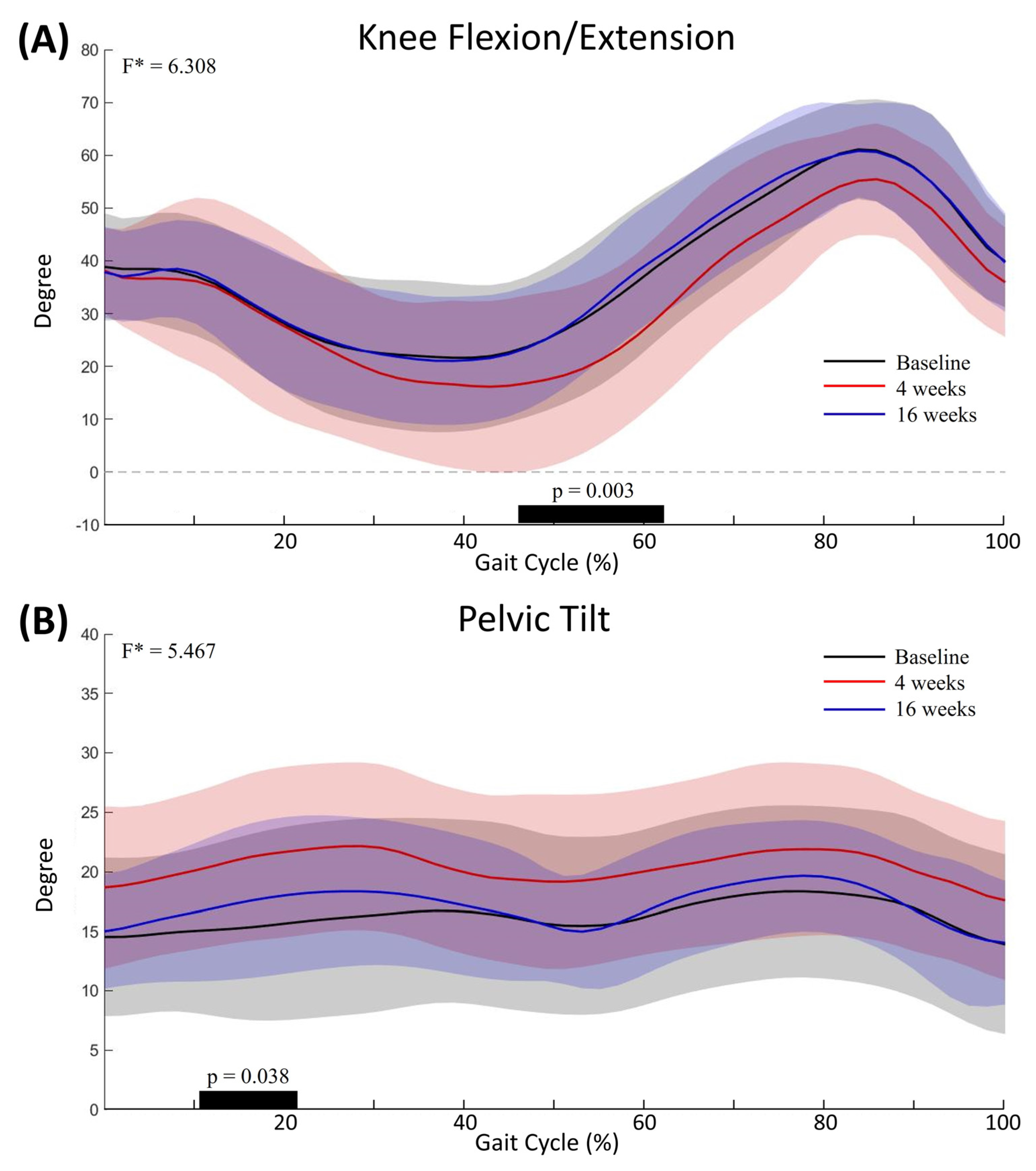
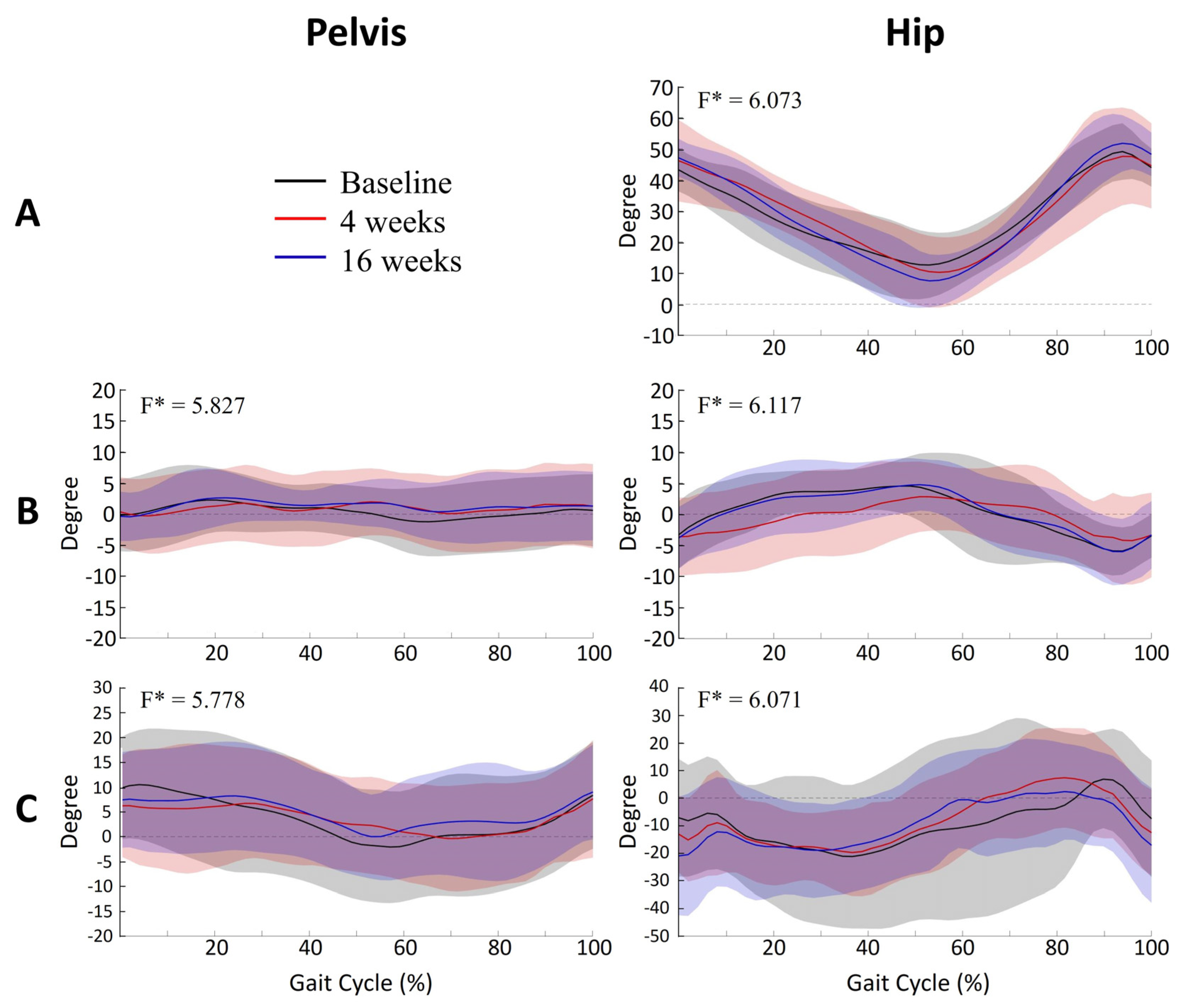
Curve Analysis Using Statistical Parametric Mapping (SPM) Analysis
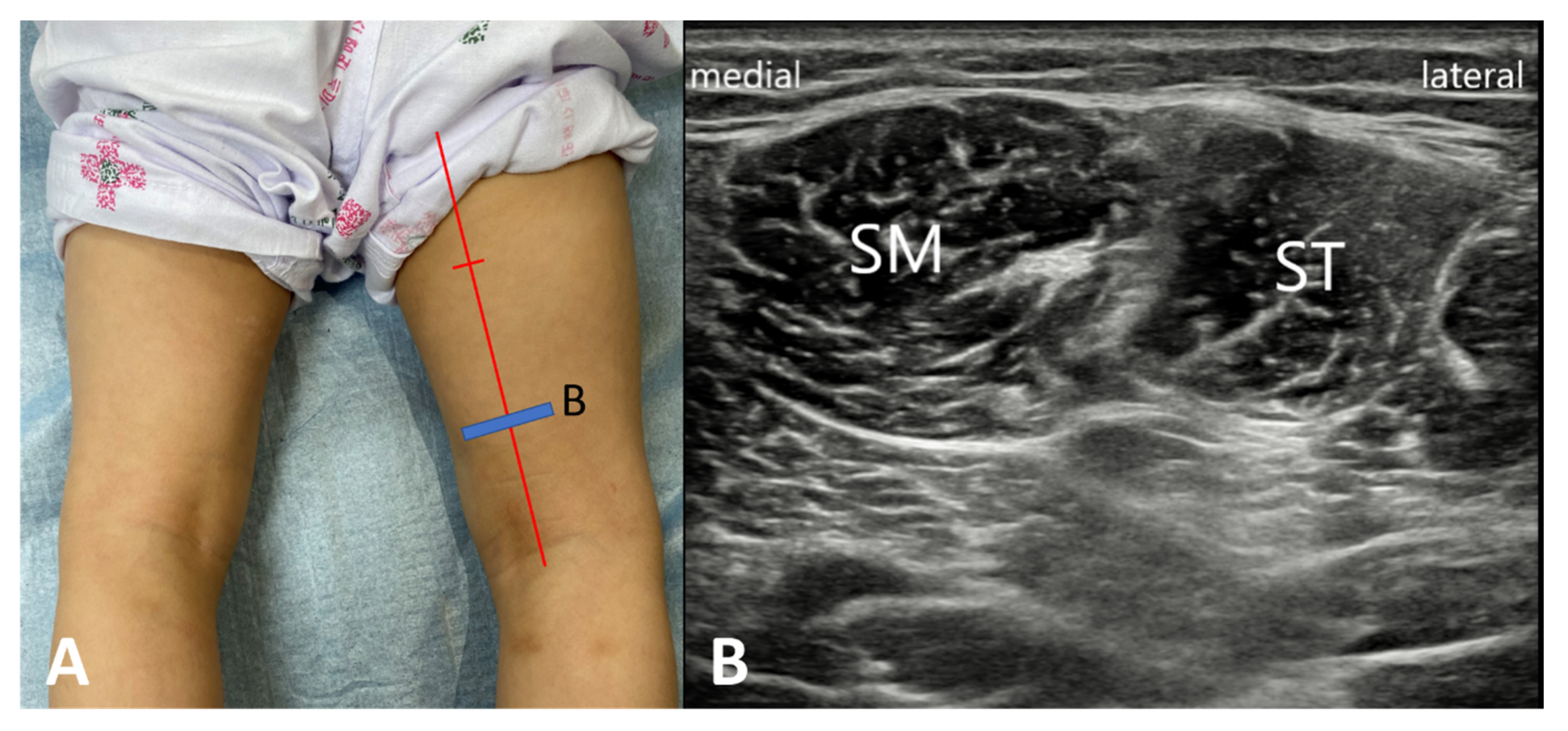
2.3. Muscle-Tendon Length
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Participants
Sample Size
5.2. Intervention
5.2.1. Functional Evaluation
5.2.2. Spasticity Assessment
5.2.3. Gait Analysis Using a Computerized Gait System
5.2.4. Muscle-Tendon Length
5.3. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| FKG | flexed knee gait |
| CP | cerebral palsy |
| BoNT-A | botulinum toxin type A |
| KE | knee extension |
| IC | initial contact |
| SM | semimembranosus |
| ST | semitendinosus |
| GMFCS | Gross Motor Function Classification System |
| GMFM | Gross Motor Function Measure |
| MAS | Modified Ashworth Scale |
| MTS | Modified Tardieu Scale |
| IR | internal rotation |
| ER | external rotation |
| SPM | statistical parametric mapping |
References
- Rose, G.E.; Lightbody, K.A.; Ferguson, R.G.; Walsh, J.C.; Robb, J.E. Natural history of flexed knee gait in diplegic cerebral palsy evaluated by gait analysis in children who have not had surgery. Gait Posture 2010, 31, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Rha, D.W.; Cahill-Rowley, K.; Young, J.; Torburn, L.; Stephenson, K.; Rose, J. Biomechanical and Clinical Correlates of Stance-Phase Knee Flexion in Persons With Spastic Cerebral Palsy. PM R 2016, 8, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Bell, K.J.; Ounpuu, S.; DeLuca, P.A.; Romness, M.J. Natural progression of gait in children with cerebral palsy. J. Pediatr. Orthop. 2002, 22, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Dhawlikar, S.; Root, L.; Mann, R. Distal lengthening of the hamstrings in patients who have cerebral palsy. Long-term retrospective analysis. J. Bone Jt. Surg. Am. Vol. 1992, 74, 1385–1391. [Google Scholar] [CrossRef]
- Arnold, A.S.; Liu, M.Q.; Schwartz, M.H.; Ounpuu, S.; Delp, S.L. The role of estimating muscle-tendon lengths and velocities of the hamstrings in the evaluation and treatment of crouch gait. Gait Posture 2006, 23, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Schutte, L.M.; Hayden, S.W.; Gage, J.R. Lengths of hamstrings and psoas muscles during crouch gait: Effects of femoral anteversion. J. Orthop. Res. 1997, 15, 615–621. [Google Scholar] [CrossRef]
- Hoffinger, S.A.; Rab, G.T.; Abou-Ghaida, H. Hamstrings in cerebral palsy crouch gait. J. Pediatr. Orthop. 1993, 13, 722–726. [Google Scholar] [CrossRef]
- Novak, I.; McIntyre, S.; Morgan, C.; Campbell, L.; Dark, L.; Morton, N.; Stumbles, E.; Wilson, S.A.; Goldsmith, S. A systematic review of interventions for children with cerebral palsy: State of the evidence. Dev. Med. Child Neurol. 2013, 55, 885–910. [Google Scholar] [CrossRef]
- Strobl, W.; Theologis, T.; Brunner, R.; Kocer, S.; Viehweger, E.; Pascual-Pascual, I.; Placzek, R. Best clinical practice in botulinum toxin treatment for children with cerebral palsy. Toxins 2015, 7, 1629–1648. [Google Scholar] [CrossRef] [Green Version]
- Love, S.C.; Novak, I.; Kentish, M.; Desloovere, K.; Heinen, F.; Molenaers, G.; O’Flaherty, S.; Graham, H.K.; Cerebral Palsy, I. Botulinum toxin assessment, intervention and after-care for lower limb spasticity in children with cerebral palsy: International consensus statement. Eur J. Neurol. 2010, 17 (Suppl. S2), 9–37. [Google Scholar] [CrossRef]
- Blumetti, F.C.; Belloti, J.C.; Tamaoki, M.J.; Pinto, J.A. Botulinum toxin type A in the treatment of lower limb spasticity in children with cerebral palsy. Cochrane Database Syst. Rev. 2019, 10, CD001408. [Google Scholar] [CrossRef] [PubMed]
- Thompson, N.S.; Baker, R.J.; Cosgrove, A.P.; Corry, I.S.; Graham, H.K. Musculoskeletal modelling in determining the effect of botulinum toxin on the hamstrings of patients with crouch gait. Dev. Med. Child Neurol. 1998, 40, 622–625. [Google Scholar] [CrossRef] [PubMed]
- Corry, I.S.; Cosgrove, A.P.; Duffy, C.M.; Taylor, T.C.; Graham, H.K. Botulinum toxin A in hamstring spasticity. Gait Posture 1999, 10, 206–210. [Google Scholar] [CrossRef]
- Papadonikolakis, A.S.; Vekris, M.D.; Korompilias, A.V.; Kostas, J.P.; Ristanis, S.E.; Soucacos, P.N. Botulinum A toxin for treatment of lower limb spasticity in cerebral palsy: Gait analysis in 49 patients. Acta Orthop. Scand. 2003, 74, 749–755. [Google Scholar] [CrossRef]
- Unlu, E.; Cevikol, A.; Bal, B.; Gonen, E.; Celik, O.; Kose, G. Multilevel botulinum toxin type a as a treatment for spasticity in children with cerebral palsy: A retrospective study. Clinics (Sao Paulo) 2010, 65, 613–619. [Google Scholar] [CrossRef]
- Scholtes, V.A.; Dallmeijer, A.J.; Knol, D.L.; Speth, L.A.; Maathuis, C.G.; Jongerius, P.H.; Becher, J.G. The combined effect of lower-limb multilevel botulinum toxin type a and comprehensive rehabilitation on mobility in children with cerebral palsy: A randomized clinical trial. Arch. Phys. Med. Rehabil. 2006, 87, 1551–1558. [Google Scholar] [CrossRef]
- Scholtes, V.A.; Dallmeijer, A.J.; Knol, D.L.; Speth, L.A.; Maathuis, C.G.; Jongerius, P.H.; Becher, J.G. Effect of multilevel botulinum toxin a and comprehensive rehabilitation on gait in cerebral palsy. Pediatr. Neurol. 2007, 36, 30–39. [Google Scholar] [CrossRef]
- Fattal-Valevski, A.; Domenievitz, D.; Giladi, N.; Wientroub, S.; Hayek, S. Long-term effect of repeated injections of botulinum toxin in children with cerebral palsy: A prospective study. J. Child. Orthop. 2008, 2, 29–35. [Google Scholar] [CrossRef]
- Nieuwenhuys, A.; Papageorgiou, E.; Desloovere, K.; Molenaers, G.; De Laet, T. Statistical Parametric Mapping to Identify Differences between Consensus-Based Joint Patterns during Gait in Children with Cerebral Palsy. PLoS ONE 2017, 12, e0169834. [Google Scholar] [CrossRef] [Green Version]
- Choi, J.Y.; Park, E.S.; Park, D.; Rha, D.W. Dynamic spasticity determines hamstring length and knee flexion angle during gait in children with spastic cerebral palsy. Gait Posture 2018, 64, 255–259. [Google Scholar] [CrossRef]
- Park, M.S.; Chung, C.Y.; Lee, S.H.; Choi, I.H.; Cho, T.-J.; Yoo, W.J.; Park, B.M.Y.; Lee, K.M. Effects of distal hamstring lengthening on sagittal motion in patients with diplegia: Hamstring length and its clinical use. Gait Posture 2009, 30, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Lovejoy, S.A.; Tylkowski, C.; Oeffinger, D.; Sander, L. The effects of hamstring lengthening on hip rotation. J. Pediatr. Orthop. 2007, 27, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: New York, NY, USA, 1988. [Google Scholar]
- Kang, H. Sample size determination for repeated measures design using G Power software. Anesth. Pain Med. 2015, 10, 6–15. [Google Scholar] [CrossRef]
- Rha, D.W.; Yi, K.H.; Park, E.S.; Park, C.; Kim, H.J. Intramuscular nerve distribution of the hamstring muscles: Application to treating spasticity. Clin. Anat. 2016, 29, 746–751. [Google Scholar] [CrossRef]
- Palisano, R.J.; Copeland, W.P.; Galuppi, B.E. Performance of physical activities by adolescents with cerebral palsy. Phys. Ther. 2007, 87, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russell, D.J.; Rosenbaum, P.L.; Cadman, D.T.; Gowland, C.; Hardy, S.; Jarvis, S. The gross motor function measure: A means to evaluate the effects of physical therapy. Dev. Med. Child Neurol. 1989, 31, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Russell, D.J.; Avery, L.M.; Walter, S.D.; Hanna, S.E.; Bartlett, D.J.; Rosenbaum, P.L.; Palisano, R.J.; Gorter, J.W. Development and validation of item sets to improve efficiency of administration of the 66-item Gross Motor Function Measure in children with cerebral palsy. Dev. Med. Child Neurol. 2010, 52, e48–e54. [Google Scholar] [CrossRef]
- Mutlu, A.; Livanelioglu, A.; Gunel, M.K. Reliability of Ashworth and Modified Ashworth scales in children with spastic cerebral palsy. BMC Musculoskelet. Disord. 2008, 9, 44. [Google Scholar] [CrossRef] [Green Version]
- Haugh, A.B.; Pandyan, A.D.; Johnson, G.R. A systematic review of the Tardieu Scale for the measurement of spasticity. Disabil. Rehabil. 2006, 28, 899–907. [Google Scholar] [CrossRef]
- Yam, W.K.; Leung, M.S. Interrater reliability of Modified Ashworth Scale and Modified Tardieu Scale in children with spastic cerebral palsy. J. Child Neurol. 2006, 21, 1031–1035. [Google Scholar] [CrossRef] [PubMed]
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E. Measurement of lower extremity kinematics during level walking. J. Orthop. Res. 1990, 8, 383–392. [Google Scholar] [CrossRef] [PubMed]
- Arnold, A.S.; Blemker, S.S.; Delp, S.L. Evaluation of a Deformable Musculoskeletal Model for Estimating Muscle–Tendon Lengths During Crouch Gait. Ann. Biomed. Eng. 2001, 29, 263–274. [Google Scholar] [CrossRef] [PubMed]
- Arnold, E.M.; Ward, S.R.; Lieber, R.L.; Delp, S.L. A model of the lower limb for analysis of human movement. Ann. Biomed. Eng. 2010, 38, 269–279. [Google Scholar] [CrossRef] [Green Version]
- Delp, S.L.; Anderson, F.C.; Arnold, A.S.; Loan, P.; Habib, A.; John, C.T.; Guendelman, E.; Thelen, D.G. OpenSim: Open-source software to create and analyze dynamic simulations of movement. IEEE Trans. Biomed. Eng. 2007, 54, 1940–1950. [Google Scholar] [CrossRef] [Green Version]
- Goudriaan, M.; Van den Hauwe, M.; Simon-Martinez, C.; Huenaerts, C.; Molenaers, G.; Goemans, N.; Desloovere, K. Gait deviations in Duchenne muscular dystrophy—Part 2. Statistical non-parametric mapping to analyze gait deviations in children with Duchenne muscular dystrophy. Gait Posture 2018, 63, 159–164. [Google Scholar] [CrossRef]
- Pataky, T.C. Generalized n-dimensional biomechanical field analysis using statistical parametric mapping. J. Biomech. 2010, 43, 1976–1982. [Google Scholar] [CrossRef]
- Adler, R.J.; Taylor, J.E. Random Fields and Geometry, 1st ed.; Springer: New York, NY, USA, 2007; p. 454. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | |
|---|---|
| Age (mean ± SD), year | 7.1 ± 3.0 |
| Sex (Male/Female), n (%) | 19 (65.5%)/10 (34.5%) |
| CP type (Bilateral/Unilateral), n (%) | 23 (79.3%)/6 (20.7%) |
| GMFCS level (I/II/III), n (%) | 6 (20.7%)/12 (41.4%)/11 (37.9%) |
| Exam side (right / left), n (%) | 16 (55.2%)/13 (44.8%) |
| Parameters | T1 (before injection) | T2 (4 weeks after injection) | T3 (16 weeks after injection) | ANOVA p-value | Post hoc analysis | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | T1 vs. T2 | T1 vs. T3 | T2 vs. T3 | ||
| GMFM-88 (%) | ||||||||||
| A. Lying and Rolling | 100 | 0 | 100 | 0 | 100 | 0 | 1.000 | |||
| B. Sitting | 99.48 | 1.35 | 99.6 | 1.06 | 99.71 | 0.64 | 0.228 | |||
| C. Crawling and Kneeling | 91.38 | 8.36 | 92.04 | 6.74 | 93.84 | 6.12 | 0.007 | 1.000 | 0.024 | 0.004 |
| D. Standing | 59.34 | 24.17 | 60.83 | 23.38 | 64.55 | 23.08 | 0.000 | 0.295 | 0.000 | 0.008 |
| E. Walking, Running and Jumping | 42.72 | 25.83 | 43.58 | 26.08 | 46.88 | 27.05 | 0.001 | 0.373 | 0.004 | 0.001 |
| Total score | 78.56 | 11.03 | 79.24 | 10.67 | 81.17 | 10.96 | 0.000 | 0.011 | 0.000 | 0.001 |
| GMFM-66 | 61.62 | 9.47 | 62.12 | 9.59 | 63.43 | 9.81 | 0.000 | 0.016 | 0.000 | 0.001 |
| Knee flexor (degrees) | ||||||||||
| MAS | 2.66 | 0.67 | 1.83 | 0.54 | 1.97 | 0.57 | 0.000 | 0.000 | 0.000 | 0.359 |
| R1 of MTS | 53.79 | 8.83 | 42.07 | 7.14 | 41.9 | 7.61 | 0.000 | 0.000 | 0.000 | 1.000 |
| R2 of MTS | 32.41 | 10.91 | 26.21 | 6.5 | 27.24 | 6.21 | 0.001 | 0.000 | 0.023 | 0.891 |
| R1-R2 of MTS | 21.38 | 11.87 | 15.86 | 7.68 | 14.66 | 6.26 | 0.000 | 0.001 | 0.003 | 1.000 |
| Parameters | T1 (before injection) | T2 (4 weeks after injection) | T3 (16 weeks after injection) | ANOVA p-value | Post hoc analysis | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | T1 vs. T2 | T1 vs. T3 | T2 vs. T3 | ||
| Spatiotemporal | ||||||||||
| Cadence (step/min) | 107.53 | 35.49 | 102.03 | 47.94 | 113.63 | 36.30 | 0.208 | |||
| Walking Speed (cm/s) | 55.50 | 27.01 | 55.46 | 35.97 | 65.29 | 26.82 | 0.123 | |||
| Step Length (cm) | 29.33 | 11.90 | 30.21 | 12.43 | 32.54 | 10.46 | 0.363 | |||
| Step Time (s) | 0.65 | 0.36 | 0.83 | 0.66 | 0.68 | 0.66 | 0.314 | |||
| Step Width (cm) | 12.10 | 4.21 | 14.06 | 5.44 | 12.24 | 5.31 | 0.111 | |||
| Pelvis (degrees) | ||||||||||
| Pelvic tilt at IC | 16.00 | 7.22 | 18.94 | 7.74 | 16.76 | 6.53 | 0.097 | |||
| Max pelvic tilt in ST | 21.15 | 7.96 | 23.74 | 7.62 | 22.65 | 6.31 | 0.170 | |||
| Pelvic tilt at end swing | 15.44 | 8.24 | 17.64 | 7.85 | 15.55 | 6.49 | 0.271 | |||
| Mean pelvic tilt in ST | 17.31 | 7.52 | 20.39 | 7.54 | 18.35 | 5.87 | 0.066 | |||
| Hip (degrees) | ||||||||||
| Hip flexion at IC | 44.29 | 9.26 | 48.16 | 9.47 | 48.39 | 7.76 | 0.036 | 0.078 | 0.106 | 1.000 |
| Max hip extension in terminal ST | 9.33 | 8.87 | 6.15 | 10.48 | 6.78 | 7.84 | 0.190 | |||
| Max hip flexion in SW | 51.14 | 11.37 | 53.72 | 10.25 | 55.21 | 8.70 | 0.085 | |||
| Hip flexion at end swing | 43.50 | 10.18 | 46.97 | 9.61 | 48.31 | 7.64 | 0.034 | 0.239 | 0.064 | 1.000 |
| Knee (degrees) | ||||||||||
| Knee flexion at IC | 37.70 | 10.67 | 34.94 | 9.48 | 36.67 | 8.54 | 0.537 | |||
| Max knee extension in ST | 19.26 | 12.65 | 12.19 | 14.92 | 18.13 | 11.61 | 0.001 | 0.003 | 1.000 | 0.030 |
| Max knee flexion in SW | 64.81 | 9.80 | 61.45 | 7.21 | 65.05 | 10.06 | 0.156 | |||
| Knee flexion at end swing | 36.34 | 10.46 | 33.91 | 9.95 | 36.86 | 10.31 | 0.374 | |||
| Hip (degrees) | ||||||||||
| Hip rotation at IC | −8.96 | 23.07 | −17.56 | 18.96 | −21.62 | 19.08 | 0.042 | 0.290 | 0.084 | 1.000 |
| Max hip internal rotation in ST | 10.47 | 24.39 | 5.87 | 20.64 | 8.71 | 20.37 | 0.694 | |||
| Max hip external rotation in ST | −24.59 | 24.92 | −28.33 | 17.10 | −29.46 | 16.36 | 0.522 | |||
| Mean hip rotation in ST | −11.57 | 23.41 | −13.90 | 17.38 | −11.90 | 18.24 | 0.861 | |||
| Max hip internal rotation in SW | 15.33 | 25.15 | 10.22 | 19.68 | 11.57 | 19.87 | 0.599 | |||
| Max hip external rotation in SW | −19.34 | 25.03 | −19.12 | 16.39 | −23.15 | 20.15 | 0.663 | |||
| Mean hip rotation in SW | −12.72 | 23.82 | −16.94 | 17.48 | −21.47 | 20.41 | 0.249 | |||
| Hip rotation at end swing | 1.61 | 22.67 | −0.81 | 18.09 | −3.07 | 16.43 | 0.616 | |||
| Normalized muscle lengths during gait | ||||||||||
| SM at IC | 1.03 | 0.04 | 1.04 | 0.04 | 1.03 | 0.05 | 0.409 | |||
| Min SM in ST | 0.92 | 0.04 | 0.93 | 0.04 | 0.91 | 0.03 | 0.210 | |||
| Max SM in SW | 1.05 | 0.05 | 1.06 | 0.04 | 1.06 | 0.04 | 0.434 | |||
| SM at end swing | 1.00 | 0.18 | 1.01 | 0.17 | 1.04 | 0.05 | 0.294 | |||
| Mean SM lengthening velocity in SW | 0.31 | 0.15 | 0.37 | 0.18 | 0.41 | 0.17 | 0.017 | 0.256 | 0.025 | 0.737 |
| Max SM lengthening velocity in SW | 0.54 | 0.18 | 0.61 | 0.19 | 0.64 | 0.17 | 0.080 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.K.; Rha, D.W.; Park, E.S. Botulinum Toxin Type A Injections Impact Hamstring Muscles and Gait Parameters in Children with Flexed Knee Gait. Toxins 2020, 12, 145. https://doi.org/10.3390/toxins12030145
Kim SK, Rha DW, Park ES. Botulinum Toxin Type A Injections Impact Hamstring Muscles and Gait Parameters in Children with Flexed Knee Gait. Toxins. 2020; 12(3):145. https://doi.org/10.3390/toxins12030145
Chicago/Turabian StyleKim, Seung Ki, Dong Wook Rha, and Eun Sook Park. 2020. "Botulinum Toxin Type A Injections Impact Hamstring Muscles and Gait Parameters in Children with Flexed Knee Gait" Toxins 12, no. 3: 145. https://doi.org/10.3390/toxins12030145
APA StyleKim, S. K., Rha, D. W., & Park, E. S. (2020). Botulinum Toxin Type A Injections Impact Hamstring Muscles and Gait Parameters in Children with Flexed Knee Gait. Toxins, 12(3), 145. https://doi.org/10.3390/toxins12030145