Intramuscular Neural Distribution of Rhomboid Muscles: Evaluation for Botulinum Toxin Injection Using Modified Sihler’s Method


 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
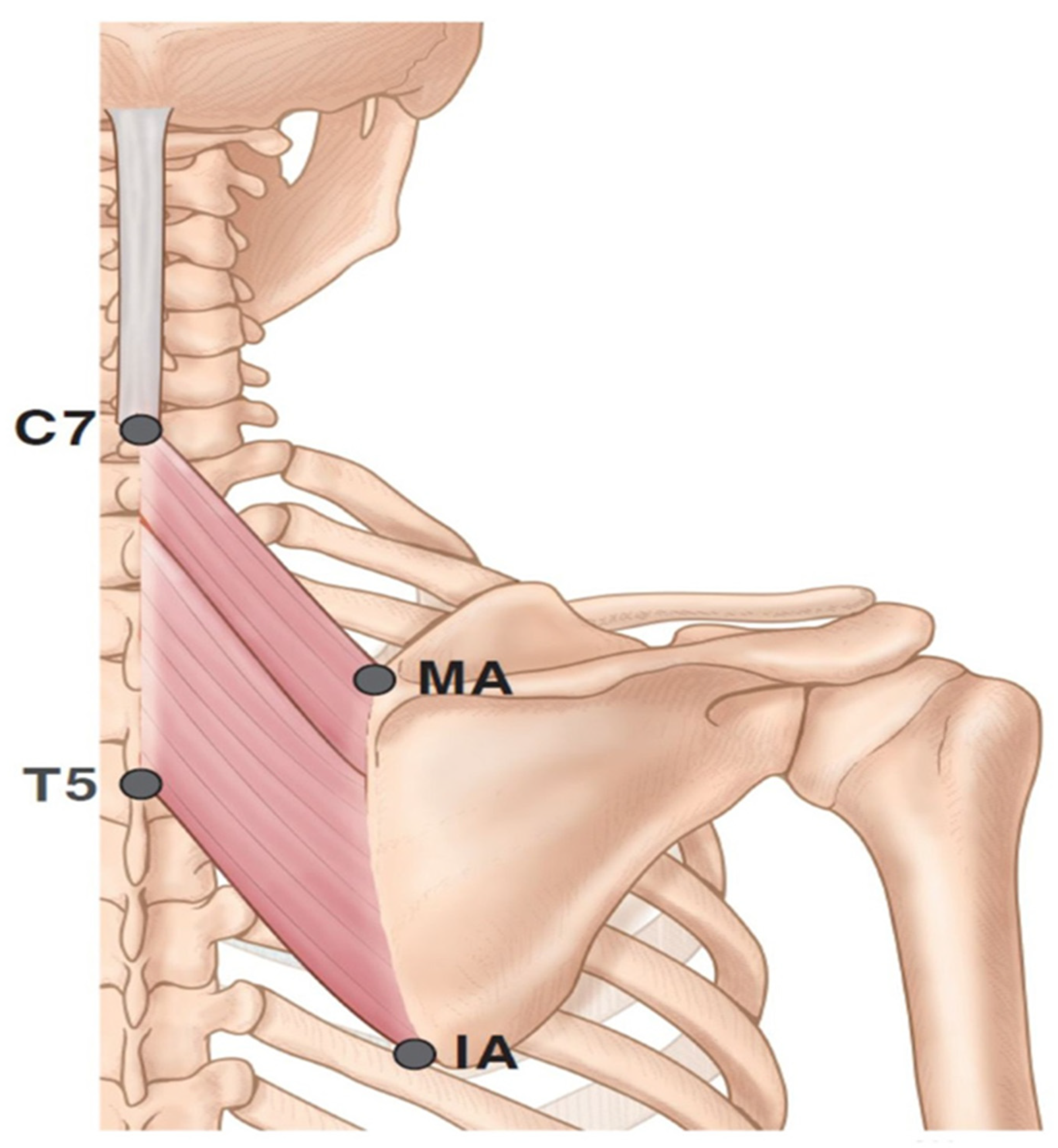
2.1. Locations of the Nerve Entry Points
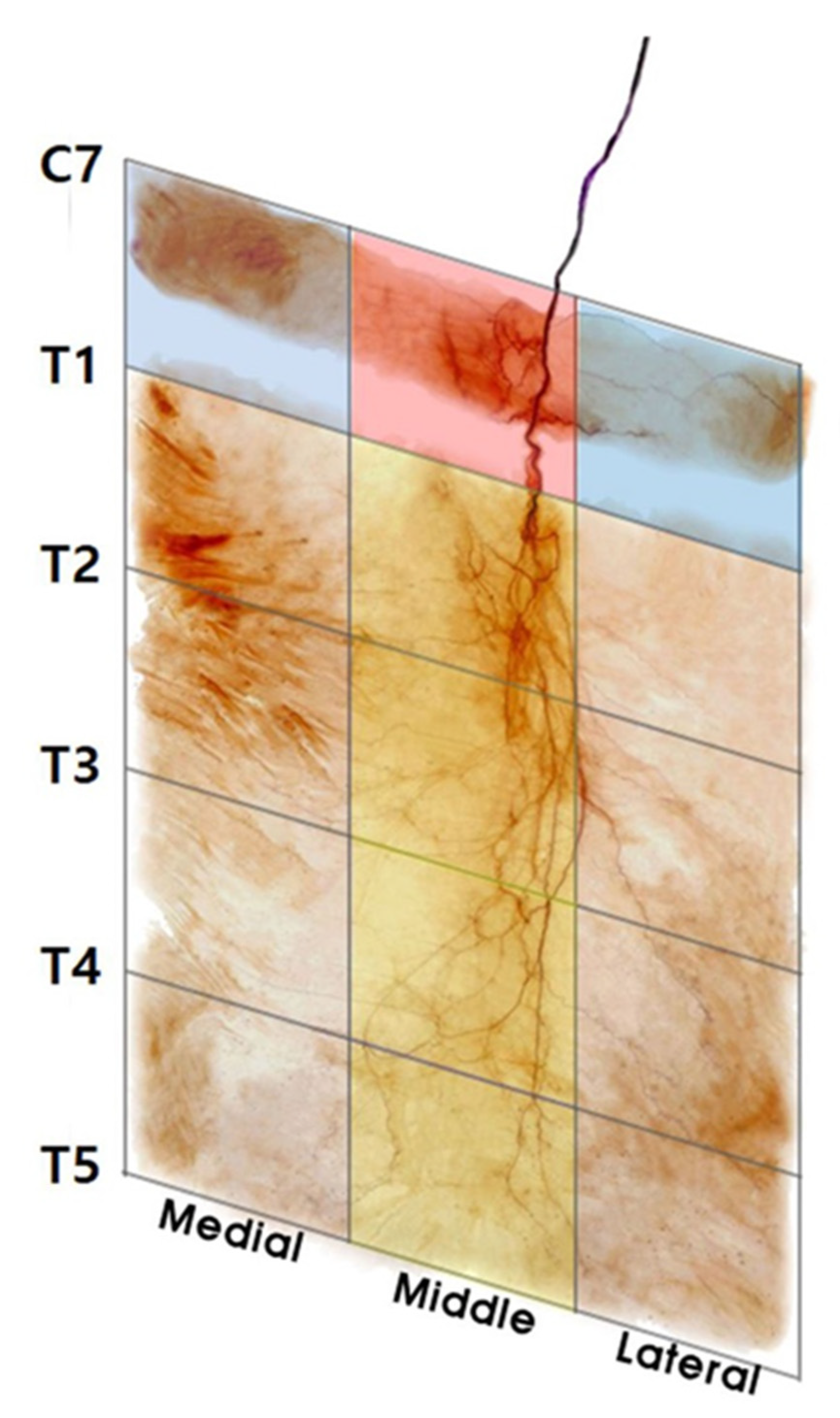
2.2. Intramuscular Arborization Patterns of the Rhomboid Minor
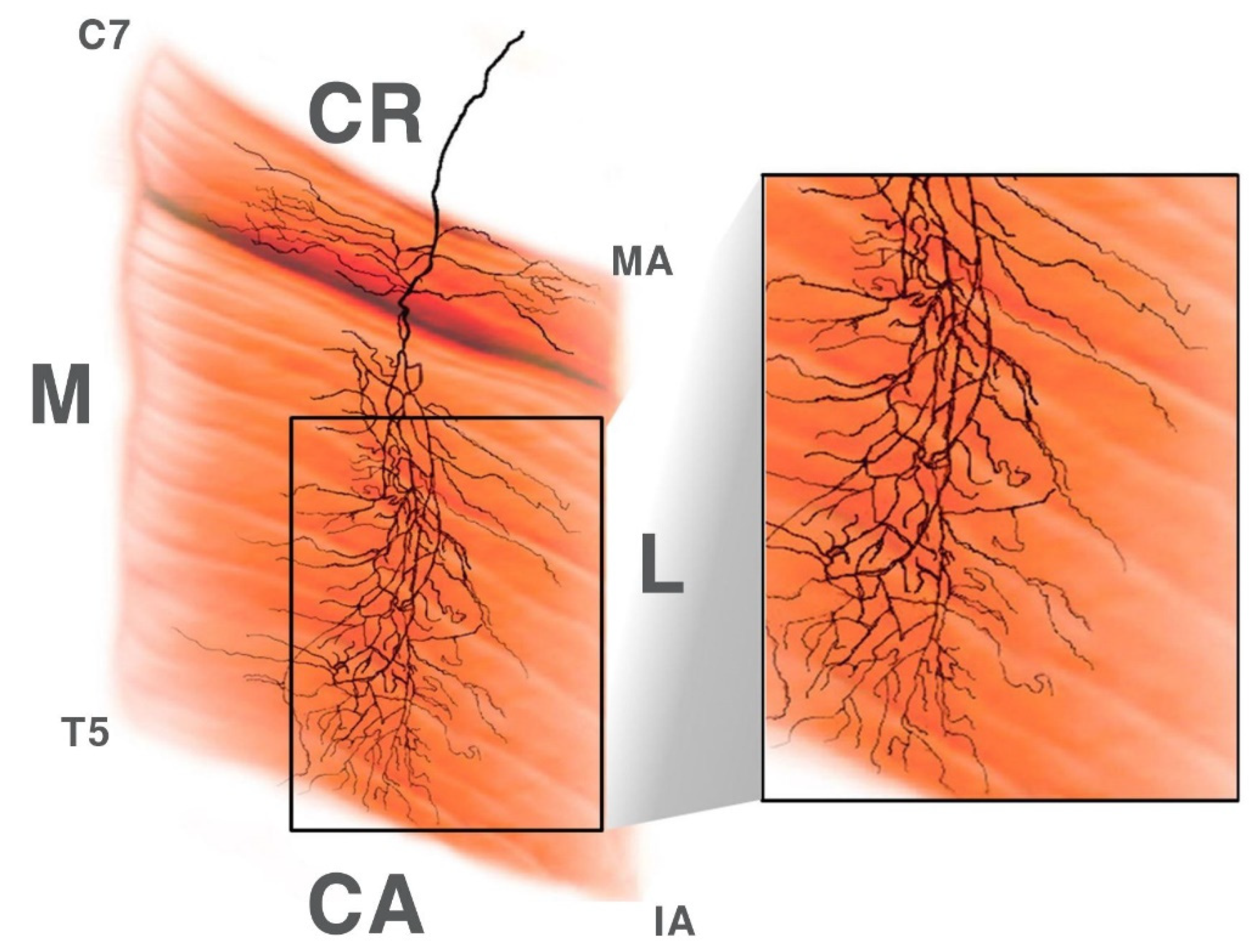
2.3. Intramuscular Arborization Patterns of the Rhomboid Major
3. Discussion
4. Conclusions
5. Materials and Methods
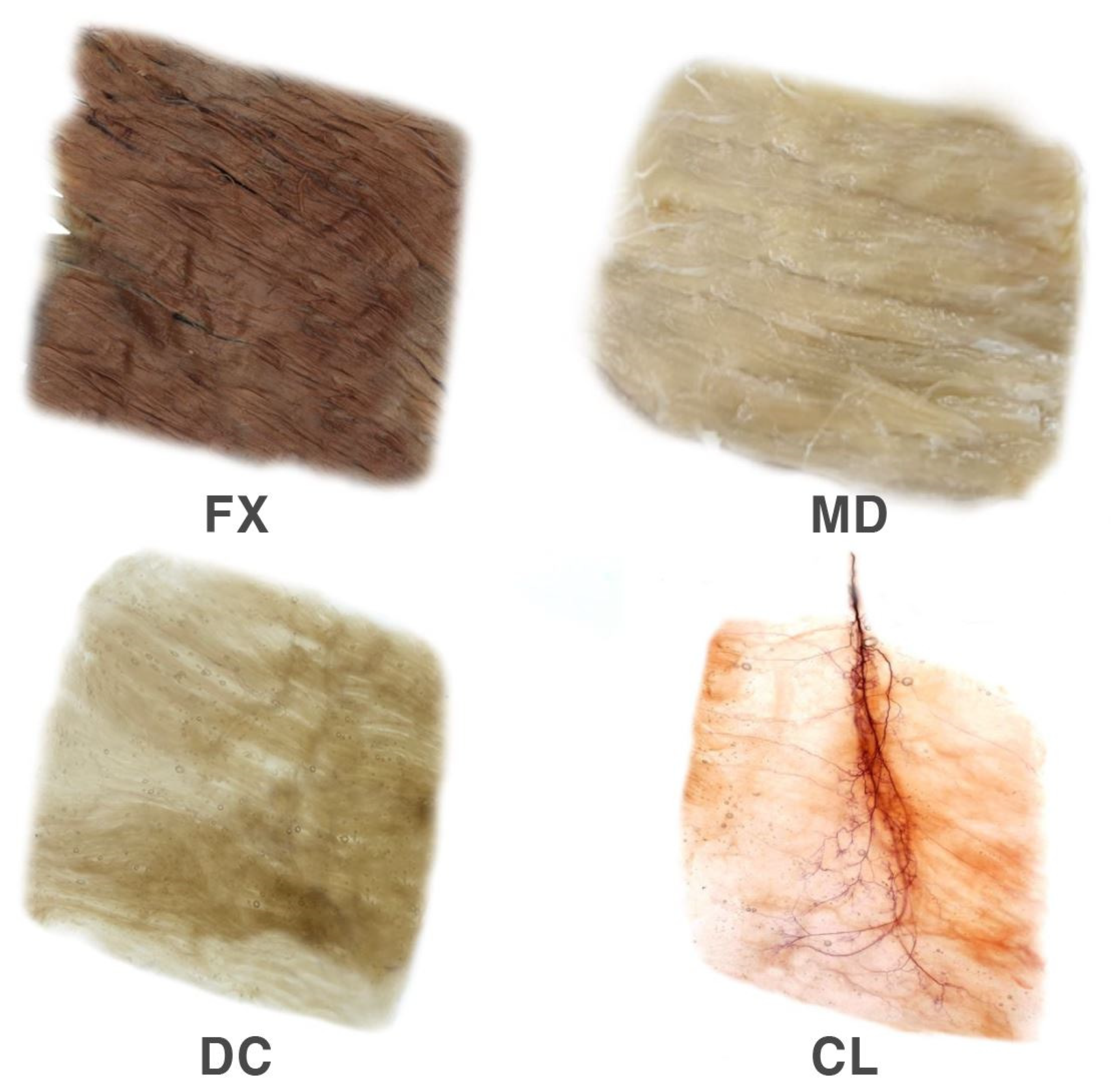
Modified Sihler Staining
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Burgen, A.S.; Dickens, F.; Zatman, L.J. The action of botulinum toxin on the neuro-muscular junction. J. Physiol. 1949, 109, 10–24. [Google Scholar] [CrossRef]
- Lindgren, I.; Jonsson, A.C.; Norrving, B.; Lindgren, A. Shoulder pain after stroke: A prospective population-based study. Stroke 2007, 38, 343–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delpont, B.; Blanc, C.; Osseby, G.V.; Hervieu-Begue, M.; Giroud, M.; Bejot, Y. Pain after stroke: A review. Rev. Neurol. 2018, 174, 671–674. [Google Scholar] [CrossRef] [PubMed]
- Adey-Wakeling, Z.; Liu, E.; Crotty, M.; Leyden, J.; Kleinig, T.; Anderson, C.S.; Newbury, J. Hemiplegic Shoulder Pain Reduces Quality of Life After Acute Stroke: A Prospective Population-Based Study. Am. J. Phys. Med. Rehabil. 2016, 95, 758–763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner-Stokes, L.; Jackson, D. Shoulder pain after stroke: A review of the evidence base to inform the development of an integrated care pathway. Clin. Rehabil. 2002, 16, 276–298. [Google Scholar] [CrossRef] [PubMed]
- Hou, S.; Ivanhoe, C.; Li, S. Botulinum Toxin Injection for Spastic Scapular Dyskinesia After Stroke: Case Series. Medicine 2015, 94, e1300. [Google Scholar] [CrossRef] [PubMed]
- Ashford, S.; Turner-Stokes, L. Management of shoulder and proximal upper limb spasticity using botulinum toxin and concurrent therapy interventions: A preliminary analysis of goals and outcomes. Disabil. Rehabil. 2009, 31, 220–226. [Google Scholar] [CrossRef]
- Van Kuijk, A.A.; Geurts, A.C.; Bevaart, B.J.; van Limbeek, J. Treatment of upper extremity spasticity in stroke patients by focal neuronal or neuromuscular blockade: A systematic review of the literature. J. Rehabil. Med. 2002, 34, 51–61. [Google Scholar] [CrossRef] [Green Version]
- Dressler, D.; Saberi, F.A.; Barbosa, E.R. Botulinum toxin: Mechanisms of action. Arq. Neuropsiquiatr. 2005, 63, 180–185. [Google Scholar] [CrossRef] [Green Version]
- Rosales, R.L.; Kong, K.H.; Goh, K.J.; Kumthornthip, W.; Mok, V.C.; Delgado-De Los Santos, M.M.; Chua, K.S.; Abdullah, S.J.; Zakine, B.; Maisonobe, P.; et al. Botulinum toxin injection for hypertonicity of the upper extremity within 12 weeks after stroke: A randomized controlled trial. Neurorehabil. Neural. Repair. 2012, 26, 812–821. [Google Scholar] [CrossRef]
- Bhakta, B.B.; Cozens, J.A.; Bamford, J.M.; Chamberlain, M.A. Use of botulinum toxin in stroke patients with severe upper limb spasticity. J. Neurol. Neurosurg. Psychiatry. 1996, 61, 30–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brashear, A.; Gordon, M.F.; Elovic, E.; Kassicieh, V.D.; Marciniak, C.; Do, M.; Lee, C.H.; Jenkins, S.; Turkel, C.; Botox Post-Stroke Spasticity Study, G. Intramuscular injection of botulinum toxin for the treatment of wrist and finger spasticity after a stroke. N. Engl. J. Med. 2002, 347, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Hesse, S.; Jahnke, M.T.; Luecke, D.; Mauritz, K.H. Short-term electrical stimulation enhances the effectiveness of Botulinum toxin in the treatment of lower limb spasticity in hemiparetic patients. Neurosci. Lett. 1995, 201, 37–40. [Google Scholar] [CrossRef]
- Childers, M.K.; Brashear, A.; Jozefczyk, P.; Reding, M.; Alexander, D.; Good, D.; Walcott, J.M.; Jenkins, S.W.; Turkel, C.; Molloy, P.T. Dose-dependent response to intramuscular botulinum toxin type A for upper-limb spasticity in patients after a stroke. Arch. Phys. Med. Rehabil. 2004, 85, 1063–1069. [Google Scholar] [CrossRef] [PubMed]
- Childers, M.K. Targeting the neuromuscular junction in skeletal muscles. Am. J. Phys. Med. Rehabil. 2004, 83, S38–S44. [Google Scholar] [CrossRef] [PubMed]
- Ramirez-Castaneda, J.; Jankovic, J.; Comella, C.; Dashtipour, K.; Fernandez, H.H.; Mari, Z. Diffusion, spread, and migration of botulinum toxin. Mov. Disord. 2013, 28, 1775–1783. [Google Scholar] [CrossRef]
- Gracies, J.M.; Lugassy, M.; Weisz, D.J.; Vecchio, M.; Flanagan, S.; Simpson, D.M. Botulinum toxin dilution and endplate targeting in spasticity: A double-blind controlled study. Arch. Phys. Med. Rehabil. 2009, 90, 9–16 e12. [Google Scholar] [CrossRef]
- Van Campenhout, A.; Verhaegen, A.; Pans, S.; Molenaers, G. Botulinum toxin type A injections in the psoas muscle of children with cerebral palsy: Muscle atrophy after motor end plate-targeted injections. Res. Dev. Disabil. 2013, 34, 1052–1058. [Google Scholar] [CrossRef]
- Kinnett, D. Botulinum toxin A injections in children: Technique and dosing issues. Am. J. Phys. Med. Rehabil. 2004, 83, S59–S64. [Google Scholar] [CrossRef]
- Hsu, T.S.; Dover, J.S.; Arndt, K.A. Effect of volume and concentration on the diffusion of botulinum exotoxin A. Arch. Dermatol. 2004, 140, 1351–1354. [Google Scholar] [CrossRef]
- Lepage, D.; Parratte, B.; Tatu, L.; Vuiller, F.; Monnier, G. Extra- and intramuscular nerve supply of the muscles of the anterior antebrachial compartment: Applications for selective neurotomy and for botulinum toxin injection. Surg. Radiol. Anat. 2005, 27, 420–430. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.H.; Choi, Y.J.; Cong, L.; Lee, K.L.; Hu, K.S.; Kim, H.J. Effective botulinum toxin injection guide for treatment of cervical dystonia. Clin. Anat. 2020, 33, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.H.; Rha, D.W.; Lee, S.C.; Cong, L.; Lee, H.J.; Lee, Y.W.; Kim, H.J.; Hu, K.S. Intramuscular nerve distribution pattern of ankle invertor muscles in human cadaver using sihler stain. Muscle Nerve 2016, 53, 742–747. [Google Scholar] [CrossRef] [PubMed]
- Rha, D.W.; Yi, K.H.; Park, E.S.; Park, C.; Kim, H.J. Intramuscular nerve distribution of the hamstring muscles: Application to treating spasticity. Clin. Anat. 2016, 29, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Liem, R.S.; Douwe van Willigen, J. In toto staining and preservation of peripheral nervous tissue. Stain. Technol. 1988, 63, 113–120. [Google Scholar] [CrossRef]
- Lee, D.G.; Chang, M.C. Dorsal scapular nerve injury after trigger point injection into the rhomboid major muscle: A case report. J. Back. Musculoskelet. Rehabil. 2018, 31, 211–214. [Google Scholar] [CrossRef]
- Gray, H.; Carter, H.V. Anatomy: Descriptive and Surgical; Bounty Books: New York, NY, USA, 2014. [Google Scholar]
- Nguyen, V.H.; Liu, H.H.; Rosales, A.; Reeves, R. A Cadaveric Investigation of the Dorsal Scapular Nerve. Anat. Res. Int. 2016, 2016, 4106981. [Google Scholar] [CrossRef] [Green Version]
- Tyvaert, L.; Krystkowiak, P.; Cassim, F.; Houdayer, E.; Kreisler, A.; Destee, A.; Defebvre, L. Myoclonus of peripheral origin: Two case reports. Mov. Disord. 2009, 24, 274–277. [Google Scholar] [CrossRef]
- Hong, C.Z. Lidocaine injection versus dry needling to myofascial trigger point. The importance of the local twitch response. Am. J. Phys. Med. Rehabil. 1994, 73, 256–263. [Google Scholar] [CrossRef]
- Safarpour, D.; Jabbari, B. Botulinum toxin A (Botox) for treatment of proximal myofascial pain in complex regional pain syndrome: Two cases. Pain. Med. 2010, 11, 1415–1418. [Google Scholar] [CrossRef]
- Preston, D.C.; Shapiro, B.E. Electromyography and Neuromuscular Disorders: Clinical–Electrophysiologic Correlations; Elsevier Saunders: New York, NY, USA, 2013; pp. 249–266. [Google Scholar]
- Kim, K.H.; Kim, G.Y.; Lim, S.G.; Park, B.K.; Kim, D.H. A More Precise Electromyographic Needle Approach for Examination of the Rhomboid Major. PMR 2018, 10, 1380–1384. [Google Scholar] [CrossRef] [PubMed]
- Cushman, D.; Henrie, M.; Vernon Scholl, L.; Ludlow, M.; Teramoto, M. Ultrasound Verification of Safe Needle Examination of The Rhomboid Major Muscle. Muscle Nerve 2018, 57, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Abdo, W.F.; Bloem, B.R.; Eijk, J.J.; Geurts, A.C.; van Alfen, N.; van de Warrenburg, B.P. Atypical dystonic shoulder movements following neuralgic amyotrophy. Mov. Disord. 2009, 24, 293–296. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Lim, J.Y. Atypical posttraumatic dystonia treated successfully by botulinum toxin injection. Am. J. Phys. Med. Rehabil. 2015, 94, 246–249. [Google Scholar] [CrossRef]
- Hassan, A.; Pittock, S.J.; Ahlskog, J.E. Steroid-responsive post-traumatic dystonia: A video case report. Parkinsonism. Relat. Disord. 2011, 17, 130–132. [Google Scholar] [CrossRef]
- Gechev, A.; Kane, N.M.; Koltzenburg, M.; Rao, D.G.; van der Star, R. Potential risks of iatrogenic complications of nerve conduction studies (NCS) and electromyography (EMG). Clin. Neurophysiol. Pract. 2016, 1, 62–66. [Google Scholar] [CrossRef] [Green Version]
- Al-Shekhlee, A.; Shapiro, B.E.; Preston, D.C. Iatrogenic complications and risks of nerve conduction studies and needle electromyography. Muscle Nerve 2003, 27, 517–526. [Google Scholar] [CrossRef]
- Lu, L.; Atchabahian, A.; Mackinnon, S.E.; Hunter, D.A. Nerve injection injury with botulinum toxin. Plast. Reconstr. Surg. 1998, 101, 1875–1880. [Google Scholar] [CrossRef]
- Okmen, K. Efficacy of rhomboid intercostal block for analgesia after thoracotomy. Korean. J. Pain. 2019, 32, 129–132. [Google Scholar] [CrossRef]
- Elsharkawy, H.; Maniker, R.; Bolash, R.; Kalasbail, P.; Drake, R.L.; Elkassabany, N. Rhomboid Intercostal and Subserratus Plane Block: A Cadaveric and Clinical Evaluation. Reg. Anesth. Pain. Med. 2018, 43, 745–751. [Google Scholar] [CrossRef]
- Seol, S.J.; Cho, H.; Yoon, D.H.; Jang, S.H. Appropriate depth of needle insertion during rhomboid major trigger point block. Ann. Rehabil. Med. 2014, 38, 72–76. [Google Scholar] [CrossRef] [PubMed]
- Alter, K.E.; Wilson, N.A. Botulinum Neurotoxin Injection Manual; Demos Medical Publishing: New York, NY, USA, 2015. [Google Scholar]




© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, K.-H.; Lee, H.-J.; Choi, Y.-J.; Lee, J.-H.; Hu, K.-S.; Kim, H.-J. Intramuscular Neural Distribution of Rhomboid Muscles: Evaluation for Botulinum Toxin Injection Using Modified Sihler’s Method. Toxins 2020, 12, 289. https://doi.org/10.3390/toxins12050289
Yi K-H, Lee H-J, Choi Y-J, Lee J-H, Hu K-S, Kim H-J. Intramuscular Neural Distribution of Rhomboid Muscles: Evaluation for Botulinum Toxin Injection Using Modified Sihler’s Method. Toxins. 2020; 12(5):289. https://doi.org/10.3390/toxins12050289
Chicago/Turabian StyleYi, Kyu-Ho, Hyung-Jin Lee, You-Jin Choi, Ji-Hyun Lee, Kyung-Seok Hu, and Hee-Jin Kim. 2020. "Intramuscular Neural Distribution of Rhomboid Muscles: Evaluation for Botulinum Toxin Injection Using Modified Sihler’s Method" Toxins 12, no. 5: 289. https://doi.org/10.3390/toxins12050289
APA StyleYi, K. -H., Lee, H. -J., Choi, Y. -J., Lee, J. -H., Hu, K. -S., & Kim, H. -J. (2020). Intramuscular Neural Distribution of Rhomboid Muscles: Evaluation for Botulinum Toxin Injection Using Modified Sihler’s Method. Toxins, 12(5), 289. https://doi.org/10.3390/toxins12050289