Effect of Botulinum Toxin Injection on Asymmetric Lower Face with Chin Deviation

 , and
, and
Abstract
:1. Introduction
2. Results
2.1. Demographic Data
2.2. Summary Statistics
2.3. Assumption Check
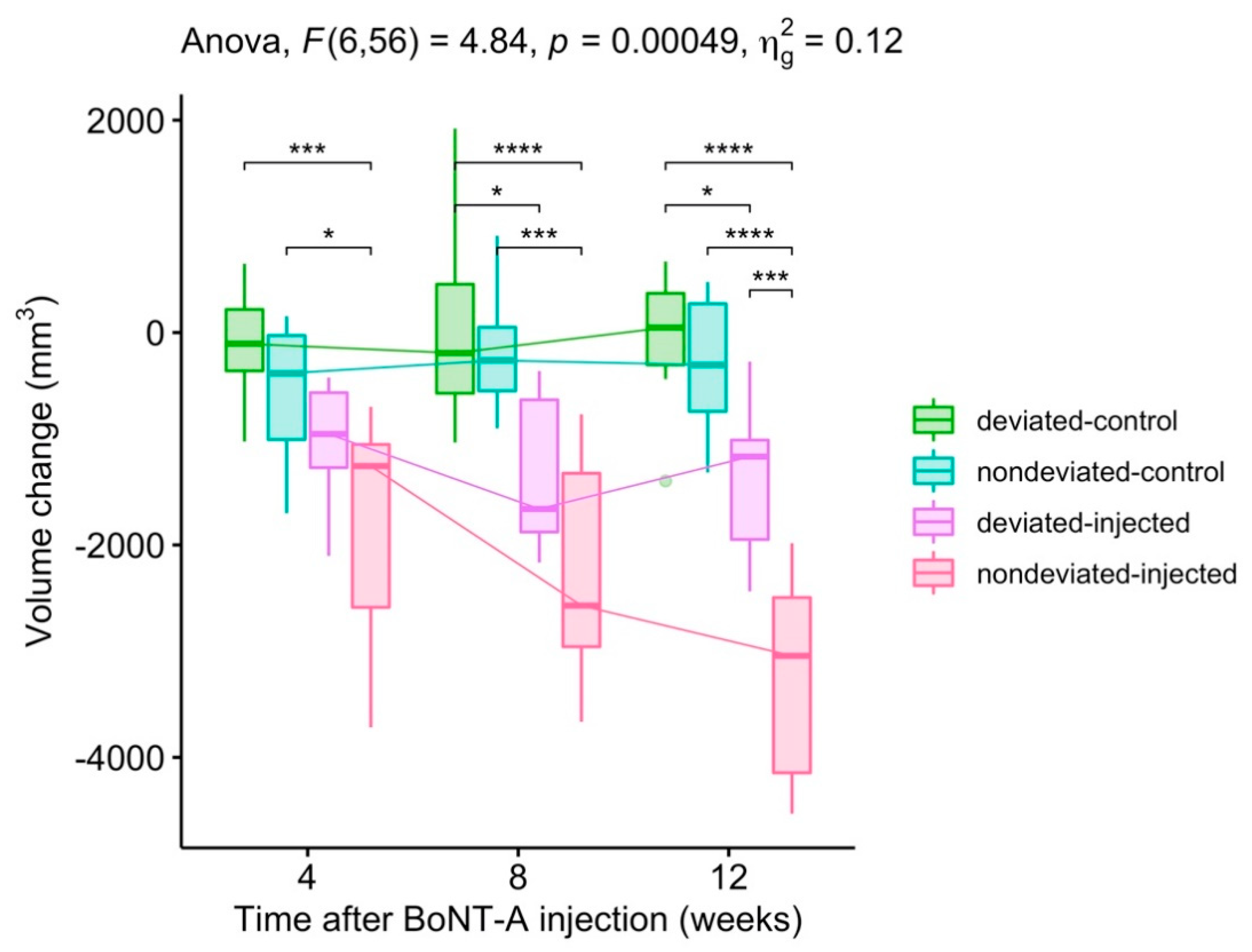
2.4. Report
2.5. Post-Hoc Tests
2.6. Summary
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Patients
5.2. Facial Asymmetry and Group
5.3. BoNT Injection
5.4. Measurement
5.5. Statistical Analyses
Author Contributions
Funding
Conflicts of Interest
References
- Kim, J.Y.; Jung, H.D.; Jung, Y.S.; Hwang, C.J.; Park, H.S. A simple classification of facial asymmetry by TML system. J. Cranio-Maxillofac. Surg. 2014, 42, 313–320. [Google Scholar] [CrossRef] [PubMed]
- You, K.H.; Kim, K.H.; Lee, K.J.; Baik, H.S. Three-dimensional computed tomography analysis of mandibular morphology in patients with facial asymmetry and mandibular retrognathism. Am. J. Orthod. Dentofac. Orthop. 2018, 153, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Shim, W.H.; Yoon, S.H.; Park, J.H.; Choi, Y.C.; Kim, S.T. Effect of botulinum toxin type A injection on lower facial contouring evaluated using a three-dimensional laser scan. Dermatol. Surg. 2010, 36, 2161–2166. [Google Scholar] [CrossRef]
- Blanshan, N.; Krug, H. The use of botulinum toxin for the treatment of chronic joint pain: Clinical and experimental evidence. Toxins 2020, 12, 314. [Google Scholar] [CrossRef] [PubMed]
- Dressler, D.; Adib Saberi, F. Botulinum toxin: Mechanisms of action. Eur. Neurol. 2005, 53, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Fagien, S. Botulinum toxin type A for facial aesthetic enhancement: Role in facial shaping. Plast. Reconstr. Surg. 2003, 112, 6–18. [Google Scholar] [CrossRef]
- Smyth, A.G. Botulinum toxin treatment of bilateral masseteric hypertrophy. Br. J. Oral Maxillofac. Surg. 1994, 32, 29–33. [Google Scholar] [CrossRef]
- Cha, Y.R.; Kim, Y.G.; Kim, J.H.; Kim, S.T. Effect of unilateral injection of botulinum toxin on lower facial asymmetry as evaluated using three-dimensional laser scanning. Dermatol. Surg. 2013, 39, 900–906. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.-W.; Jung, Y.-S.; Baik, H.-S. Three-dimensional analysis of midfacial soft tissue changes after maxillary posterior impaction and intraoral vertical ramus osteotomy for mandibular setback in class III patients. J. Craniofac. Surg. 2017, 28, 1789–1796. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.M.; Baik, H.-S.; Jung, H.-D.; Jang, W.; Choi, Y.J. Diagnosis and surgical outcomes of facial asymmetry according to the occlusal cant and menton deviation. J. Oral Maxillofac. Surg. 2019, 77, 1261–1275. [Google Scholar] [CrossRef]
- Hwang, H.S.; Youn, I.S.; Lee, K.H.; Lim, H.J. Classification of facial asymmetry by cluster analysis. Am. J. Orthod. Dentofac. Orthop. 2007, 132, 279.e1–279.e6. [Google Scholar] [CrossRef]
- Kwon, S.M.; Hwang, J.J.; Jung, Y.H.; Cho, B.H.; Lee, K.J.; Hwang, C.J.; Choi, S.H. Similarity index for intuitive assessment of three-dimensional facial asymmetry. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grummons, D.C. A frontal asymmetry analysis. J. Clin. Orthod. 1987, 21, 448–465. [Google Scholar] [PubMed]
- Lee, E.H.; Yu, H.S.; Lee, K.J.; Han, S.S.; Jung, H.D.; Hwang, C.J. Comparison of three midsagittal planes for three-dimensional cone beam computed tomography head reorientation. Korean J. Orthod. 2020, 50, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Hewitt, A.B. A radiographic study of facial asymmetry. Br. J. Orthod. 1975, 2, 37–40. [Google Scholar] [CrossRef]
- Masuoka, N.; Muramatsu, A.; Ariji, Y.; Nawa, H.; Goto, S.; Ariji, E. Discriminative thresholds of cephalometric indexes in the subjective evaluation of facial asymmetry. Am. J. Orthod. Dentofac. Orthop. 2007, 131, 609–613. [Google Scholar] [CrossRef]
- Kim, N.H.; Chung, J.H.; Park, R.H.; Park, J.B. The use of botulinum toxin type A in aesthetic mandibular contouring. Plast. Reconstr. Surg. 2005, 115, 919–930. [Google Scholar] [CrossRef] [PubMed]
- Baik, H.-S.; Lee, H.J.; Lee, K.-J. A proposal for soft tissue landmarks for craniofacial analysis using 3-dimensional laser scan imaging. World J. Orthod. 2006, 7, 7–14. [Google Scholar]
- Toma, A.M.; Zhurov, A.; Playle, R.; Ong, E.; Richmond, S. Reproducibility of facial soft tissue landmarks on 3D laser-scanned facial images. Orthod. Craniofac. Res. 2009, 12, 33–42. [Google Scholar] [CrossRef]
- Choi, H.-W.; Kim, B.; Kim, J.-Y.; Huh, J.-K.; Park, K.-H. Three-dimensional computed tomography evaluation of craniofacial characteristics according to lateral deviation of chin. Maxillofac. Plast. Reconstr. Surg. 2019, 41, 57. [Google Scholar] [CrossRef]
- Lee, U.L.; Kwon, J.S.; Woo, S.H.; Choi, Y.J. Simultaneous bimaxillary surgery and mandibular reconstruction with a 3-Dimensional printed titanium implant fabricated by electron beam melting: A preliminary mechanical testing of the printed mandible. J. Oral Maxillofac. Surg. 2016, 74, 1501.e11–1501.e15. [Google Scholar] [CrossRef] [PubMed]
- Seo, S.; Baik, H.; Hwang, C.; Yu, H.-S. Analysis of masseter muscle in facial asymmetry before and after orthognathic surgery using 3-dimensional computed tomography. Korean J. Orthod. 2009, 39, 18. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.T.; Mori, Y.; Minami, K.; An, C.H.; Park, J.W.; Kwon, T.G. Does skeletal surgery for asymmetric mandibular prognathism influence the soft tissue contour and thickness? J. Oral Maxillofac. Surg. 2013, 71, 1577–1587. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2020. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | Deviated Chin | Non-Deviated Chin | p | |
|---|---|---|---|---|
| (n = 8) | (n = 8) | |||
| Age [IQR] | 25.0 [22.0; 33.0] | 26.5 [25.0; 34.0] | 0.311 | Mann–Whitney U test |
| Sex | 1.000 | Fisher’s Exact Test | ||
| Female | 5 (62.5%) | 6 (75.0%) | ||
| Male | 3 (37.5%) | 2 (25.0%) | ||
| Menton deviation (mean ± SD) | 5.4 ± 1.2 | 1.5 ± 0.9 | 0.002 | t-test |
| BoNT Injection | Time after BoNT Injection | |||||||
|---|---|---|---|---|---|---|---|---|
| 4 Weeks | 8 Weeks | 12 Weeks | ||||||
| Δ Volume (mm3) mean (SD) | Group I deviated chin | control | −76 | (551) | 112 | (1105) | −59 | (660) |
| injected | −1015 | (561) | −1364 | (715) | −1389 | (735) | ||
| Group II non-deviated chin | control | −572 | (679) | −180 | (566) | −323 | (691) | |
| injected | −1783 | (1126) | −2266 | (1029) | −3242 | (994) | ||
| Δ Bulkiest height (mm) mean (SD) | Group I deviated chin | control | −0.14 | (0.44) | −0.09 | (0.7) | 0.03 | (0.49) |
| injected | −1.22 | (0.55) | −1.62 | (0.74) | −1.66 | (0.48) | ||
| Group II non-deviated chin | control | −0.56 | (0.51) | −0.53 | (0.44) | −0.58 | (0.59) | |
| injected | −2.45 | (1.06) | −3.26 | (1.09) | −3.70 | (0.74) | ||
| Change | Time | Effect | Bonferroni-Adjusted p-Value | |
|---|---|---|---|---|
| Volume change | 4 weeks | Group | 3.00 × 10−3 | ** |
| 8 weeks | Group | 7.20 × 10−5 | **** | |
| 12 weeks | Group | 7.46 × 10−8 | **** | |
| Bulkiest height change | 4 weeks | Group | 4.71 × 10−6 | **** |
| 8 weeks | Group | 7.65 × 10−8 | **** | |
| 12 weeks | Group | 4.32 × 10−12 | **** | |
| Time | Group1 | Group2 | Bonferroni-Adjusted p-Value | ||
|---|---|---|---|---|---|
| 4 weeks | deviated-control | nondeviated-control | 1.00 | ||
| 4 weeks | deviated-control | deviated-injected | 1.24 × 10−1 | ||
| 4 weeks | deviated-control | nondeviated-injected | 7.34 × 10−4 | *** | |
| 4 weeks | nondeviated-control | deviated-injected | 1.00 | ||
| 4 weeks | nondeviated-control | nondeviated-injected | 2.26 × 10−2 | * | |
| 4 weeks | deviated-injected | nondeviated-injected | 3.29 × 10−1 | ||
| 8 weeks | deviated-control | nondeviated-control | 1.00 | ||
| 8 weeks | deviated-control | deviated-injected | 1.40 × 10−2 | * | |
| 8 weeks | deviated-control | nondeviated-injected | 5.67 × 10−5 | **** | |
| 8 weeks | nondeviated-control | deviated-injected | 7.21 × 10−2 | ||
| 8 weeks | nondeviated-control | nondeviated-injected | 3.45 × 10−4 | *** | |
| 8 weeks | deviated-injected | nondeviated-injected | 3.01 × 10−1 | ||
| 12 weeks | deviated-control | nondeviated-control | 1.00 | ||
| 12 weeks | deviated-control | deviated-injected | 1.21 × 10−2 | * | |
| 12 weeks | deviated-control | nondeviated-injected | 4.29 × 10−8 | **** | |
| 12 weeks | nondeviated-control | deviated-injected | 6.51 × 10−2 | ||
| 12 weeks | nondeviated-control | nondeviated-injected | 2.32 × 10−7 | **** | |
| 12 weeks | deviated-injected | nondeviated-injected | 3.35 × 10−4 | *** | |
| Time | Group1 | Group2 | Bonferroni-Adjusted p-Value | |
|---|---|---|---|---|
| 4 weeks | deviated-control | nondeviated-control | 1.00 | |
| 4 weeks | deviated-control | deviated-injected | 2.30 × 10−2 | * |
| 4 weeks | deviated-control | nondeviated-injected | 1.62 × 10−6 | **** |
| 4 weeks | nondeviated-control | deviated-injected | 3.83 × 10−1 | |
| 4 weeks | nondeviated-control | nondeviated-injected | 4.29 × 10−5 | **** |
| 4 weeks | deviated-injected | nondeviated-injected | 7.93 × 10−3 | ** |
| 8 weeks | deviated-control | nondeviated-control | 1.00 | |
| 8 weeks | deviated-control | deviated-injected | 2.99 × 10−3 | ** |
| 8 weeks | deviated-control | nondeviated-injected | 4.23 × 10−8 | **** |
| 8 weeks | nondeviated-control | deviated-injected | 5.16 × 10−2 | |
| 8 weeks | nondeviated-control | nondeviated-injected | 6.94 × 10−7 | **** |
| 8 weeks | deviated-injected | nondeviated-injected | 1.40 × 10−3 | ** |
| 12 weeks | deviated-control | nondeviated-control | 2.83 × 10−1 | |
| 12 weeks | deviated-control | deviated-injected | 1.97 × 10−5 | **** |
| 12 weeks | deviated-control | nondeviated-injected | 2.01 × 10−12 | **** |
| 12 weeks | nondeviated-control | deviated-injected | 5.49 × 10−3 | ** |
| 12 weeks | nondeviated-control | nondeviated-injected | 1.27 × 10−10 | **** |
| 12 weeks | deviated-injected | nondeviated-injected | 7.98 × 10−07 | **** |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.; Park, J.-H.; Favero, V.; Mah, J.; Jung, Y.-S.; Kim, S.T. Effect of Botulinum Toxin Injection on Asymmetric Lower Face with Chin Deviation. Toxins 2020, 12, 456. https://doi.org/10.3390/toxins12070456
Kim D, Park J-H, Favero V, Mah J, Jung Y-S, Kim ST. Effect of Botulinum Toxin Injection on Asymmetric Lower Face with Chin Deviation. Toxins. 2020; 12(7):456. https://doi.org/10.3390/toxins12070456
Chicago/Turabian StyleKim, Dongwook, Ju-Hyun Park, Vittorio Favero, James Mah, Young-Soo Jung, and Seong Taek Kim. 2020. "Effect of Botulinum Toxin Injection on Asymmetric Lower Face with Chin Deviation" Toxins 12, no. 7: 456. https://doi.org/10.3390/toxins12070456
APA StyleKim, D., Park, J. -H., Favero, V., Mah, J., Jung, Y. -S., & Kim, S. T. (2020). Effect of Botulinum Toxin Injection on Asymmetric Lower Face with Chin Deviation. Toxins, 12(7), 456. https://doi.org/10.3390/toxins12070456