A Review of the Efficacy of FDA-Approved B. anthracis Anti-Toxin Agents When Combined with Antibiotic or Hemodynamic Support in Infection- or Toxin-Challenged Preclinical Models

Abstract
:1. Introduction
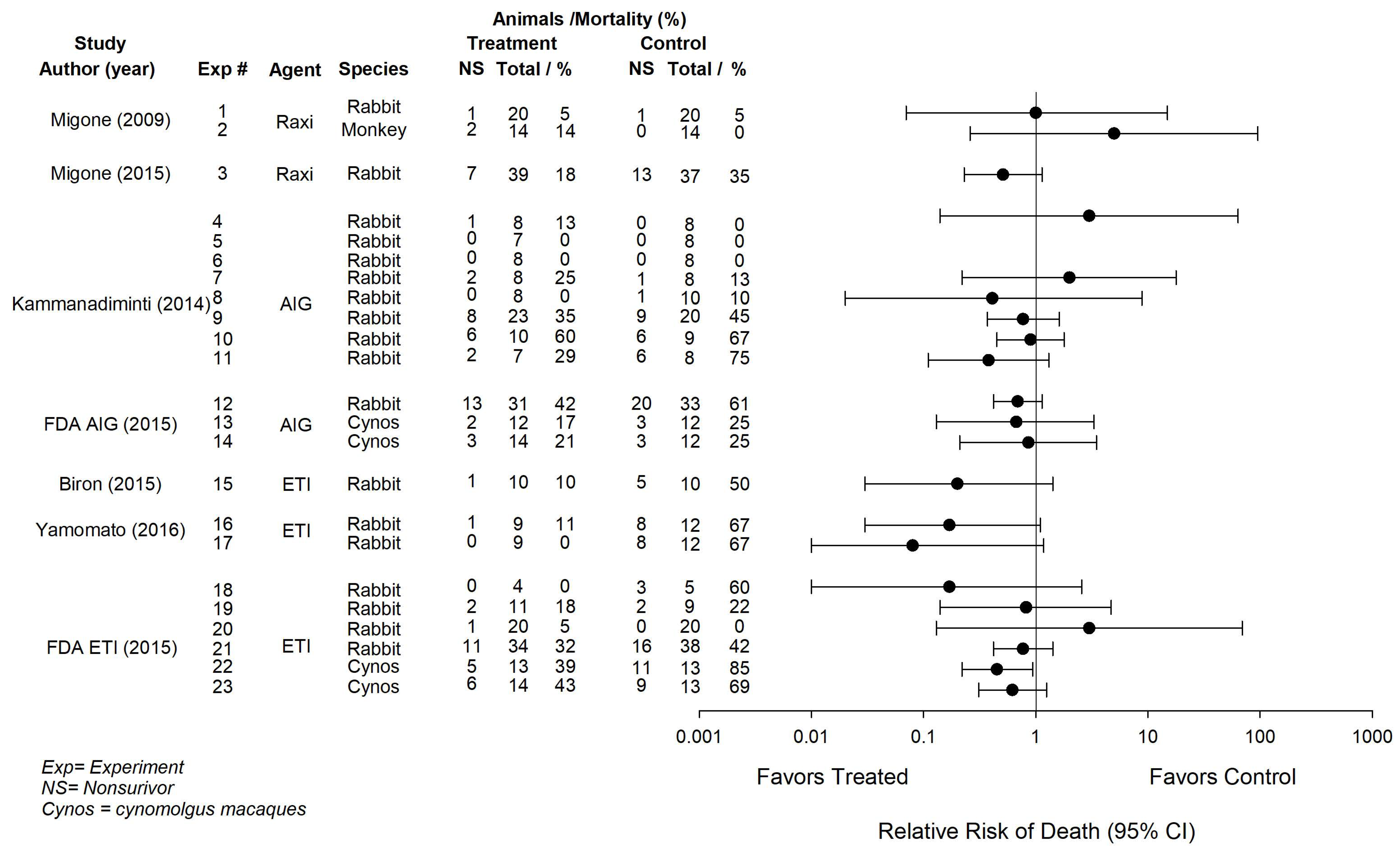
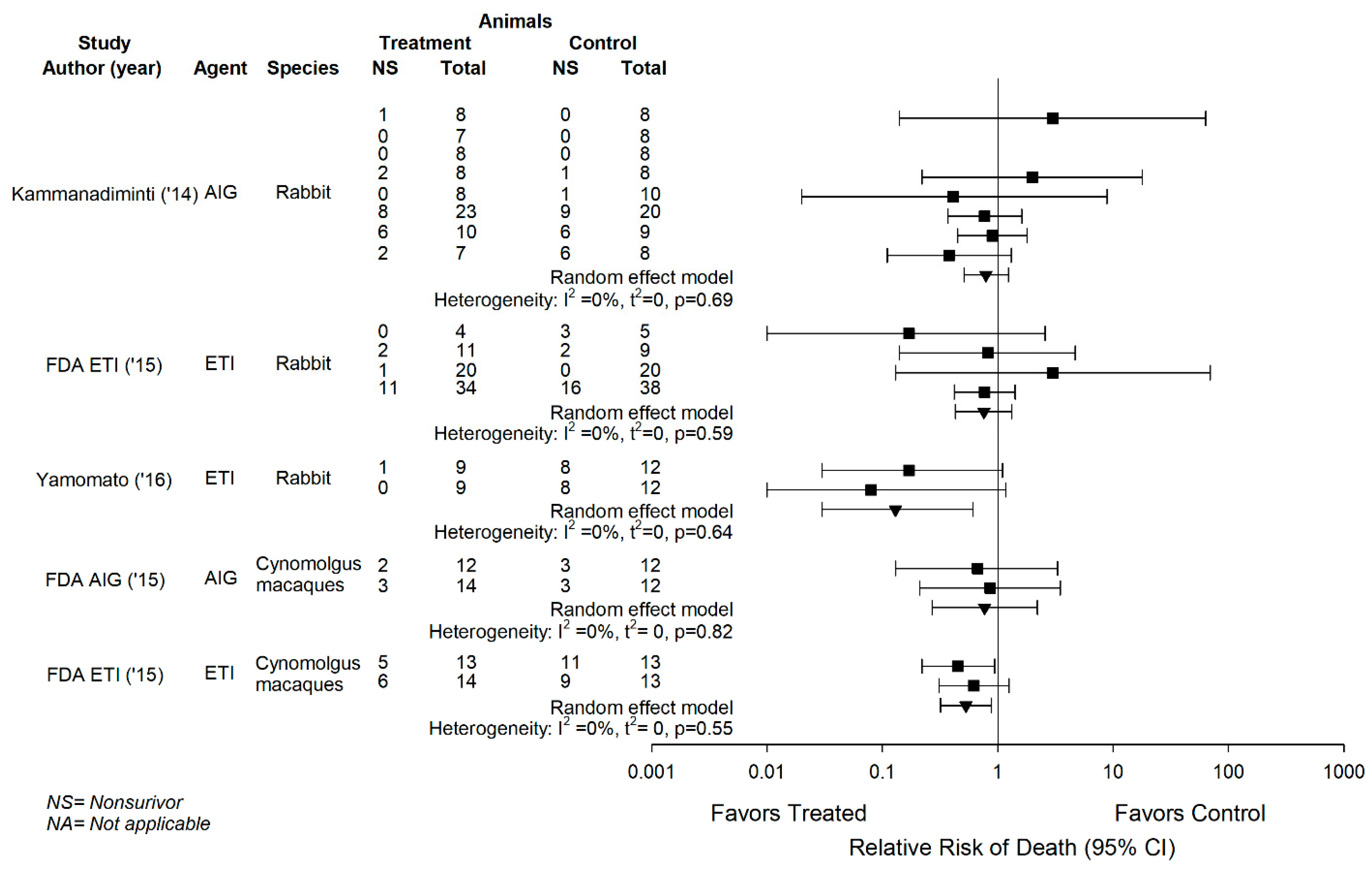
2. Effects of the Three B. anthracis Anti-Toxin Agents when Combined with Antibiotics in Live B. anthracis Challenged Animal Models
2.1. Raxibacumab
2.2. Anthrax Immune Globulin Intravenous
2.3. ETI-204
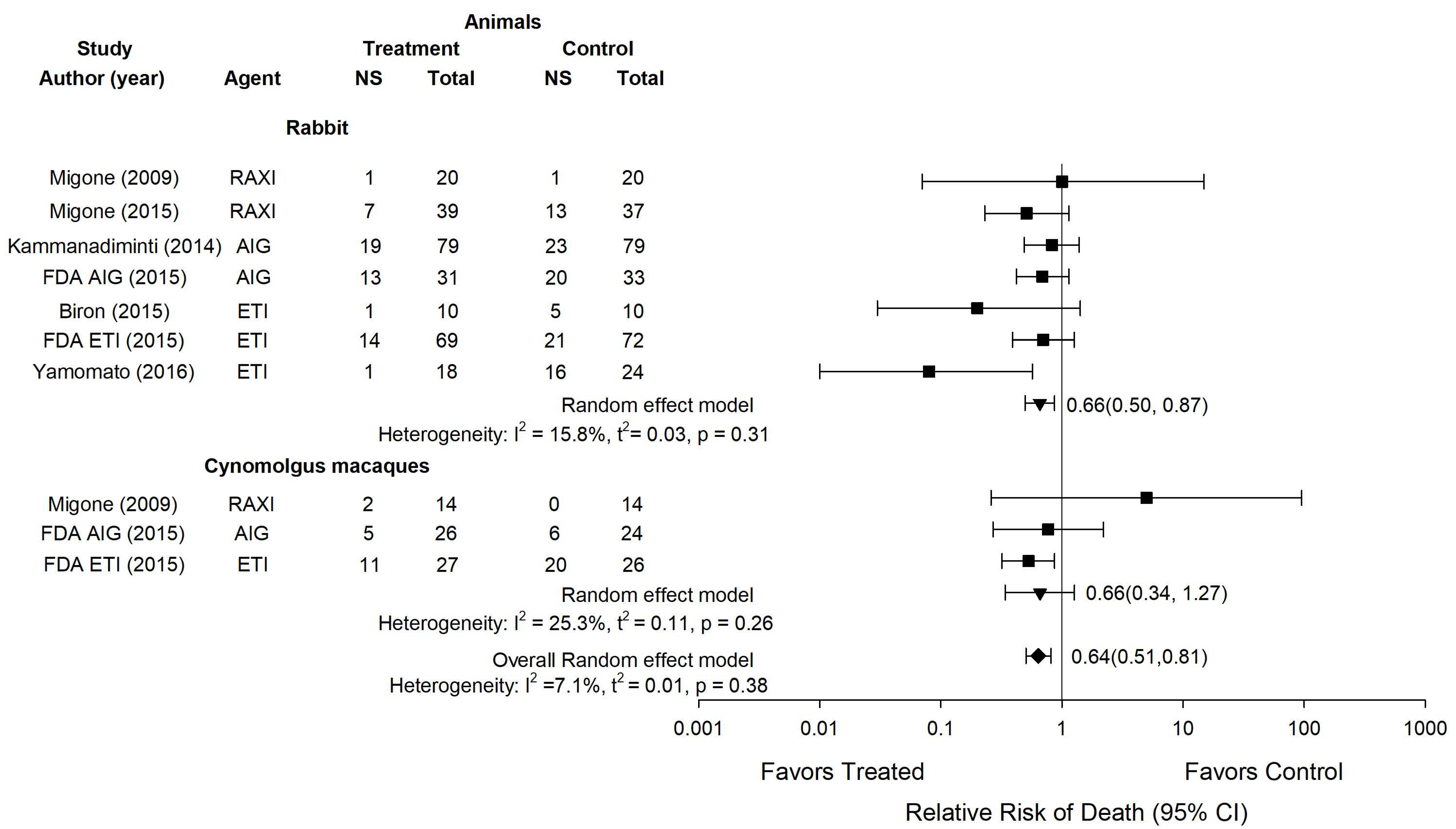
2.4. Overall Experience with Anti-Toxin Agents
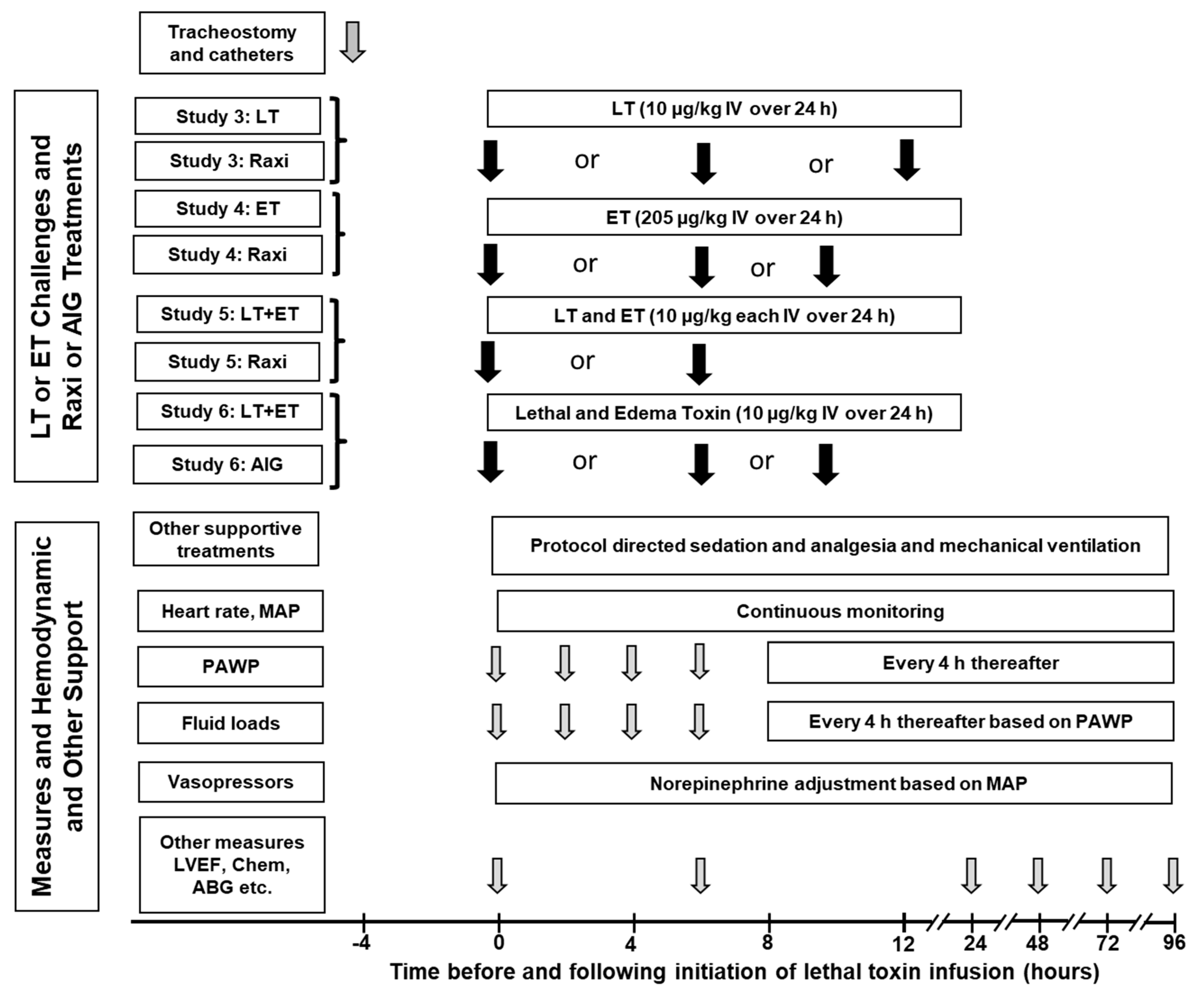
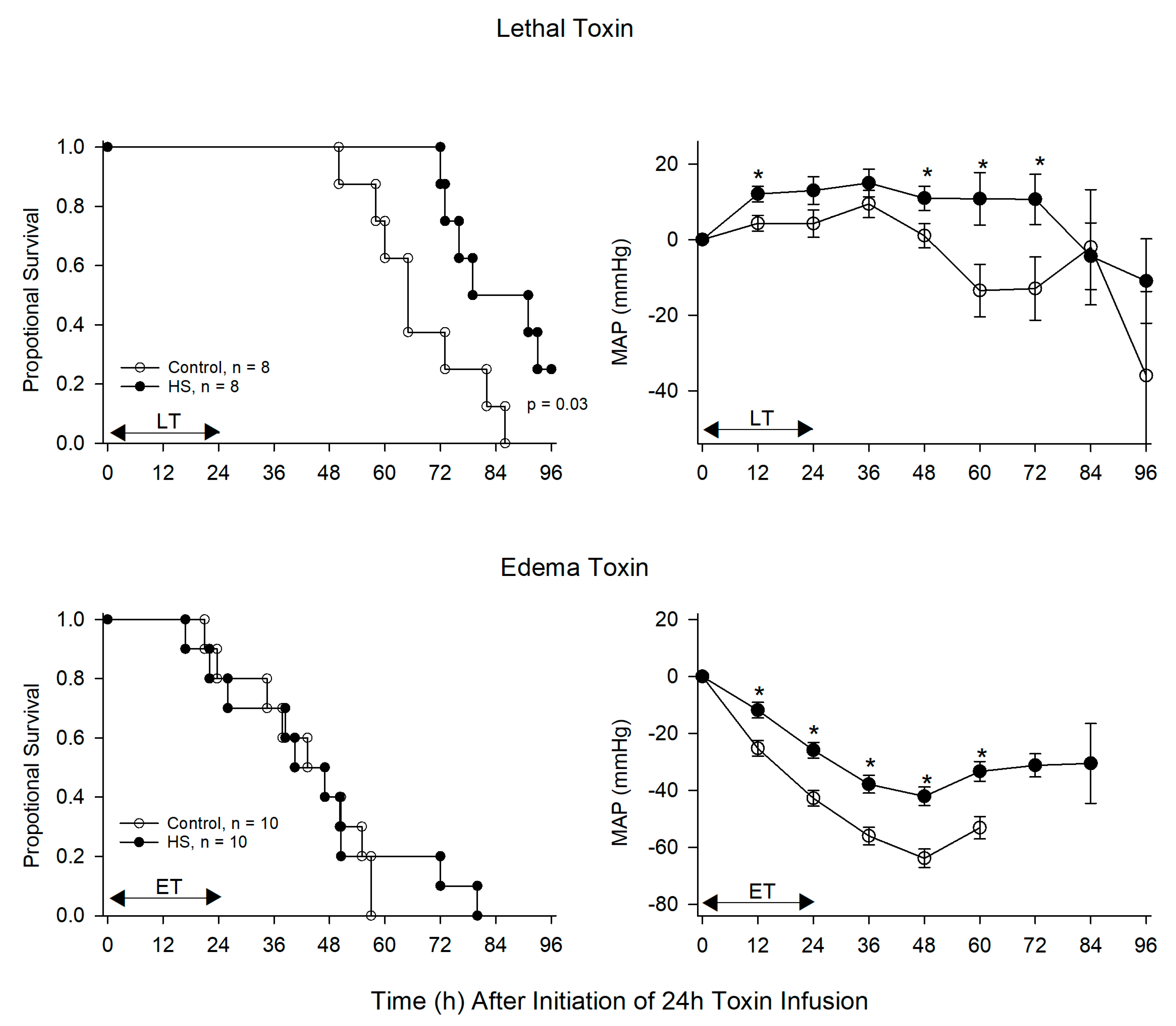
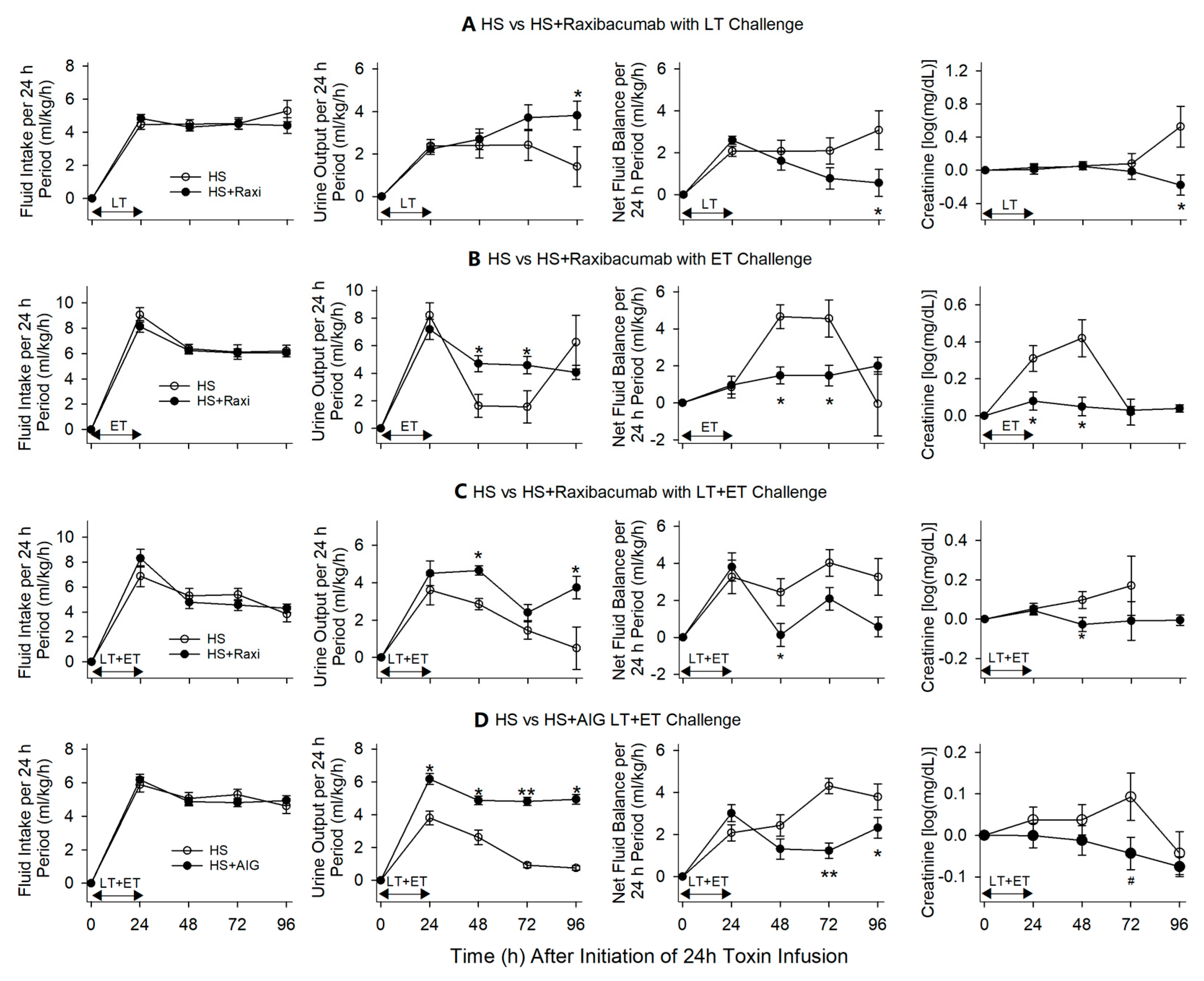
3. Effects of the Raxibacumab and AIGIV when Combined with Titrated Hemodynamic Support in a Canine Model of Anthrax Toxin-Associated Shock
4. Summary
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Jernigan, D.B.; Raghunathan, P.L.; Bell, B.P.; Brechner, R.; Bresnitz, E.A.; Butler, J.C.; Cetron, M.; Cohen, M.; Doyle, T.; Fischer, M.; et al. Investigation of bioterrorism-related anthrax, United States, 2001: Epidemiologic findings. Emerg. Infect. Dis. 2002, 8, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Nolen, L.D.; Sun, J.; Booth, M.; Donaldson, L.; Quinn, C.P.; Boyer, A.E.; Hendricks, K.; Shadomy, S.; Bothma, P.; et al. Analysis of Anthrax Immune Globulin Intravenous with Antimicrobial Treatment in Injection Drug Users, Scotland, 2009–2010. Emerg. Infect Dis. 2017, 23, 56–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, M.; Donaldson, L.; Cui, X.; Sun, J.; Cole, S.; Dailsey, S.; Hart, A.; Johns, N.; McConnell, P.; McLennan, T.; et al. Confirmed Bacillus anthracis infection among persons who inject drugs, Scotland, 2009–2010. Emerg. Infect. Dis. 2014, 20, 1452–1463. [Google Scholar] [CrossRef] [PubMed]
- Adalja, A.A.; Toner, E.; Inglesby, T.V. Clinical management of potential bioterrorism-related conditions. N Engl. J. Med. 2015, 372, 954–962. [Google Scholar] [CrossRef] [PubMed]
- Collier, R.J.; Young, J.A. Anthrax toxin. Annu. Rev. Cell Dev. Biol. 2003, 19, 45–70. [Google Scholar] [CrossRef] [PubMed]
- Pezard, C.; Berche, P.; Mock, M. Contribution of individual toxin components to virulence of Bacillus anthracis. Infect. Immun. 1991, 59, 3472–3477. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sweeney, D.A.; Hicks, C.W.; Cui, X.; Li, Y.; Eichacker, P.Q. Anthrax infection. Am. J. Respir Crit Care Med. 2011, 184, 1333–1341. [Google Scholar] [CrossRef]
- Moayeri, M.; Leppla, S.H.; Vrentas, C.; Pomerantsev, A.P.; Liu, S. Anthrax Pathogenesis. Annu Rev. Microbiol. 2015, 69, 185–208. [Google Scholar] [CrossRef]
- Leppla, S.H. Anthrax toxin edema factor: A bacterial adenylate cyclase that increases cyclic AMP concentrations of eukaryotic cells. Proc. Natl. Acad. Sci. USA 1982, 79, 3162–3166. [Google Scholar] [CrossRef] [Green Version]
- Shen, Y.; Zhukovskaya, N.L.; Zimmer, M.I.; Soelaiman, S.; Bergson, P.; Wang, C.R.; Gibbs, C.S.; Tang, W.J. Selective inhibition of anthrax edema factor by adefovir, a drug for chronic hepatitis B virus infection. Proc. Natl. Acad. Sci. USA 2004, 101, 3242–3247. [Google Scholar] [CrossRef] [Green Version]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Crit Care Med. 2017, 45, 486–552. [Google Scholar] [CrossRef] [PubMed]
- Natanson, C.; Danner, R.L.; Reilly, J.M.; Doerfler, M.L.; Hoffman, W.D.; Akin, G.L.; Hosseini, J.M.; Banks, S.M.; Elin, R.J.; MacVittie, T.J.; et al. Antibiotics versus cardiovascular support in a canine model of human septic shock. Am. J. Physiol. 1990, 259, H1440–H1447. [Google Scholar] [CrossRef]
- Huang, E.; Pillai, S.K.; Bower, W.A.; Hendricks, K.A.; Guarnizo, J.T.; Hoyle, J.D.; Gorman, S.E.; Boyer, A.E.; Quinn, C.P.; Meaney-Delman, D. Antitoxin Treatment of Inhalation Anthrax: A Systematic Review. Health Secur. 2015, 13, 365–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohanjanian, L.; Remy, K.E.; Li, Y.; Cui, X.; Eichacker, P.Q. An overview of investigational toxin-directed therapies for the adjunctive management of Bacillus anthracis infection and sepsis. Expert Opin. Investig. Drugs 2015, 24, 851–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, W.; Ohanjanian, L.; Sun, J.; Cui, X.; Suffredini, D.; Li, Y.; Welsh, J.; Eichacker, P.Q. A systematic review and meta-analysis of preclinical trials testing anti-toxin therapies for B. anthracis infection: A need for more robust study designs and results. PLoS ONE 2017, 12, e0182879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sweeney, D.A.; Cui, X.; Solomon, S.B.; Vitberg, D.A.; Migone, T.S.; Scher, D.; Danner, R.L.; Natanson, C.; Subramanian, G.M.; Eichacker, P.Q. Anthrax lethal and edema toxins produce different patterns of cardiovascular and renal dysfunction and synergistically decrease survival in canines. J. Infect. Dis. 2010, 202, 1885–1896. [Google Scholar] [CrossRef]
- Barochia, A.V.; Cui, X.; Sun, J.; Li, Y.; Solomon, S.B.; Migone, T.S.; Subramanian, G.M.; Bolmer, S.D.; Eichacker, P.Q. Protective antigen antibody augments hemodynamic support in anthrax lethal toxin shock in canines. J. Infect. Dis. 2012, 205, 818–829. [Google Scholar] [CrossRef] [Green Version]
- Suffredini, D.A.; Cui, X.; Jaswal, D.; Remy, K.E.; Li, Y.; Sun, J.; Solomon, S.B.; Fitz, Y.; Moayeri, M.; Leppla, S.; et al. Anthrax immune globulin improves hemodynamics and survival during B. anthracis toxin-induced shock in canines receiving titrated fluid and vasopressor support. Intensive Care Med. Exp. 2017, 5, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Migone, T.S.; Subramanian, G.M.; Zhong, J.; Healey, L.M.; Corey, A.; Devalaraja, M.; Lo, L.; Ullrich, S.; Zimmerman, J.; Chen, A.; et al. Raxibacumab for the treatment of inhalational anthrax. N. Engl. J. Med. 2009, 361, 135–144. [Google Scholar] [CrossRef] [Green Version]
- Migone, T.S.; Bolmer, S.; Zhong, J.; Corey, A.; Vasconcelos, D.; Buccellato, M.; Meister, G. Added benefit of raxibacumab to antibiotic treatment of inhalational anthrax. Antimicrob Agents Chemother. 2015, 59, 1145–1151. [Google Scholar] [CrossRef] [Green Version]
- US Dept. of HHS FDA. Raxibacumab Treatment of Inhalational Anthrax. November 2012. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2012/125349Orig1s000ODMemo.pdf (accessed on 16 November 2020).
- Kammanadiminti, S.; Patnaikuni, R.K.; Comer, J.; Meister, G.; Sinclair, C.; Kodihalli, S. Combination therapy with antibiotics and anthrax immune globulin intravenous (AIGIV) is potentially more effective than antibiotics alone in rabbit model of inhalational anthrax. PLoS ONE 2014, 9, e106393. [Google Scholar] [CrossRef] [PubMed]
- US Dept. of HHS FDA. ANTHRASIL (AIGIV) Injection Prescribing Information. March 2015. Available online: https://www.fda.gov/vaccines-blood-biologics/approved-blood-products/anthrasil (accessed on 16 November 2020).
- Biron, B.; Beck, K.; Dyer, D.; Mattix, M.; Twenhafel, N.; Nalca, A. Efficacy of ETI-204 monoclonal antibody as an adjunct therapy in a New Zealand white rabbit partial survival model for inhalational anthrax. Antimicrob. Agents Chemother. 2015, 59, 2206–2214. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, B.J.; Shadiack, A.M.; Carpenter, S.; Sanford, D.; Henning, L.N.; Gonzales, N.; O’Connor, E.; Casey, L.S.; Serbina, N.V. Obiltoxaximab Prevents Disseminated Bacillus anthracis Infection and Improves Survival during Pre- and Postexposure Prophylaxis in Animal Models of Inhalational Anthrax. Antimicrob. Agents Chemother. 2016, 60, 5796–5805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- US Dept. of HHS FDA. Anthim (Obiltoxaximab) Injection Prescribing Information. March 2016. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/125509lbl.pdf (accessed on 16 November 2020).
- Remy, K.E.; Cui, X.; Li, Y.; Sun, J.; Solomon, S.B.; Fitz, Y.; Barochia, A.V.; Al-Hamad, M.; Moayeri, M.; Leppla, S.H.; et al. Raxibacumab augments hemodynamic support and improves outcomes during shock with B. anthracis edema toxin alone or together with lethal toxin in canines. Intensive Care Med. Exp. 2015, 3, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reagan, W.J.; Scott-Moncrieff, C.; Christian, J.; Snyder, P.; Kelly, K.; Glickman, L. Effects of human intravenous immunoglobulin on canine monocytes and lymphocytes. Am. J. Vet. Res. 1998, 59, 1568–1574. [Google Scholar]
- Tabrizi, M.; Neupane, D.; Elie, S.E.; Shankaran, H.; Juan, V.; Zhang, S.; Hseih, S.; Fayadat-Dilman, L.; Zhang, D.; Song, Y.; et al. Pharmacokinetic Properties of Humanized IgG1 and IgG4 Antibodies in Preclinical Species: Translational Evaluation. AAPS J. 2019, 21, 39. [Google Scholar] [CrossRef]
- Li, Y.; Cui, X.; Su, J.; Haley, M.; Macarthur, H.; Sherer, K.; Moayeri, M.; Leppla, S.H.; Fitz, Y.; Eichacker, P.Q. Norepinephrine increases blood pressure but not survival with anthrax lethal toxin in rats. Crit Care Med. 2009, 37, 1348–1354. [Google Scholar] [CrossRef]
- Sherer, K.; Li, Y.; Cui, X.; Li, X.; Subramanian, M.; Laird, M.W.; Moayeri, M.; Leppla, S.H.; Fitz, Y.; Su, J.; et al. Fluid support worsens outcome and negates the benefit of protective antigen-directed monoclonal antibody in a lethal toxin-infused rat Bacillus anthracis shock model. Crit Care Med. 2007, 35, 1560–1567. [Google Scholar] [CrossRef]
- Coggeshall, K.M.; Lupu, F.; Ballard, J.; Metcalf, J.P.; James, J.A.; Farris, D.; Kurosawa, S. The sepsis model: An emerging hypothesis for the lethality of inhalation anthrax. J. Cell Mol. Med. 2013, 17, 914–920. [Google Scholar] [CrossRef]
- Remy, K.E.; Qiu, P.; Li, Y.; Cui, X.; Eichacker, P.Q.B. anthracis associated cardiovascular dysfunction and shock: The potential contribution of both non-toxin and toxin components. BMC Med. 2013, 11, 217. [Google Scholar] [CrossRef] [Green Version]
- Stearns-Kurosawa, D.J.; Lupu, F.; Taylor, F.B., Jr.; Kinasewitz, G.; Kurosawa, S. Sepsis and pathophysiology of anthrax in a nonhuman primate model. Am. J. Pathol. 2006, 169, 433–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popescu, N.I.; Silasi, R.; Keshari, R.S.; Girton, A.; Burgett, T.; Zeerleder, S.S.; Gailani, D.; Gruber, A.; Lupu, F.; Coggeshall, K.M. Peptidoglycan induces disseminated intravascular coagulation in baboons through activation of both coagulation pathways. Blood 2018, 132, 849–860. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, P.; Li, Y.; Shiloach, J.; Cui, X.; Sun, J.; Trinh, L.; Kubler-Kielb, J.; Vinogradov, E.; Mani, H.; Al-Hamad, M.; et al. Bacillus anthracis cell wall peptidoglycan but not lethal or edema toxins produces changes consistent with disseminated intravascular coagulation in a rat model. J. Infect. Dis. 2013, 208, 978–989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortes-Puch, I.; Hicks, C.W.; Sun, J.; Solomon, S.B.; Eichacker, P.Q.; Sweeney, D.A.; Nieman, L.K.; Whitley, E.M.; Behrend, E.N.; Natanson, C.; et al. Hypothalamic-pituitary-adrenal axis in lethal canine Staphylococcus aureus pneumonia. Am. J. Physiol. Endocrinol. Metab. 2014, 307, E994–E1008. [Google Scholar] [CrossRef] [Green Version]
- Hicks, C.W.; Sweeney, D.A.; Danner, R.L.; Eichacker, P.Q.; Suffredini, A.F.; Feng, J.; Sun, J.; Moriyama, B.; Wesley, R.; Behrend, E.N.; et al. Beneficial effects of stress-dose corticosteroid therapy in canines depend on the severity of staphylococcal pneumonia. Intensive Care Med. 2012, 38, 2063–2071. [Google Scholar] [CrossRef] [Green Version]
- Minneci, P.C.; Deans, K.J.; Hansen, B.; Parent, C.; Romines, C.; Gonzales, D.A.; Ying, S.X.; Munson, P.; Suffredini, A.F.; Feng, J.; et al. A canine model of septic shock: Balancing animal welfare and scientific relevance. Am. J. Physiol Heart Circ. Physiol. 2007, 293, H2487–H2500. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Exp # | Species | Sex | Inhalational Ames Strain Challenge Dose | Antibiotics Treatment | Anti-Toxin Treatment | Trigger | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Type | Route | Dose | Time (h) | Type | Route | Dose | Time (h) | ||||||
| Migone (2009) [19] | 1 | Rabbit | M/F | 200 × LD50 | Levo | Oral | 50 mg/kg | 0 | RAXI | IV | 40 mg/kg | NR | PA det |
| 2 | Cynos | M/F | 200 × LD50 | Cipro | Oral | 75 mg | 0 | RAXI | IV | 40 mg/kg | NR | PA det | |
| Migone (2015) [20] | 3 | Rabbit | M/F | 2.1 × 107 s | Levo | GI, IV | 50 mg/kg | 84 | RAXI | IV | 40 mg/kg | 84 | NT |
| Kammanadiminti (2014) [22] | 4 | Rabbit | NR | 2.1 × 107 s | Levo | Oral | 50 mg/kg | 30 | AIGIV | IV | 15 U/kg | 30 | NT |
| 5 | Rabbit | NR | 2.1 × 107 s | Levo | Oral | 50 mg/kg | 36 | AIGIV | IV | 15 U/kg | 36 | NT | |
| 6 | Rabbit | NR | 2.1 × 107 s | Levo | Oral | 50 mg/kg | 48 | AIGIV | IV | 15 U/kg | 48 | NT | |
| 7 | Rabbit | NR | 2.1 × 107 s | Levo | Oral | 50 mg/kg | 60 | AIGIV | IV | 15 U/kg | 60 | NT | |
| 8 | Rabbit | NR | 2.1 × 107 s | Levo | Oral | 50 mg/kg | 60 | AIGIV | IV | 15 U/kg | 60 | NT | |
| 9 | Rabbit | NR | 2.1 × 107 s | Levo | Oral | 50 mg/kg | 72 | AIGIV | IV | 15 U/kg | 72 | NT | |
| 10 | Rabbit | NR | 2.1 × 107 s | Levo | Oral | 50 mg/kg | 84 | AIGIV | IV | 15 U/kg | 84 | NT | |
| 11 | Rabbit | NR | 2.1 × 107 s | Levo | Oral | 50 mg/kg | 96 | AIGIV | IV | 15 U/kg | 96 | NT | |
| 12 | Rabbit | NR | 2.1 × 107 s | Levo | Oral | 50 mg/kg | 96 | AIGIV | IV | 15 U/kg | 96 | NT | |
| FDA AIG (2015) [23] | 13 | Cynos | M/F | 200 × LD50 | Cipro | Oral | 32 mg/kg 16 mg/kg | 64 | AIGIV | IV | 15 U/kg | 64 | NT |
| 14 | Cynos | M/F | 200 × LD50 | Cipro | Oral | 32 mg/kg 16 mg/kg | 64 | AIGIV | IV | 30 U/kg | 64 | NT | |
| Biron (2015) [24] | 15 | Rabbit | M/F | 150–250 × LD50 | Doxy | IV | 2.0 mg/kg | 30 | ETI | IV | 8 mg/kg | 30 * | PA det |
| Yamomato (2016) [25] | 16 | Rabbit | M/F | 200 × LD50 | Levo | Oral | 50 mg/kg | 9 | ETI | IV | 4 mg/kg | 9 | NT |
| 17 | Rabbit | M/F | 200 × LD50 | Levo | Oral | 50 mg/kg | 9 | ETI | IM | 8 mg/kg | 9 | NT | |
| FDA ETI (2015) [26] | 18 | Rabbit | NR | NR | Levo | NR | 50 mg/kg | 96 | ETI | IV | 8 mg/kg | 96 | NT |
| 19 | Rabbit | NR | NR | Levo | NR | 50 mg/kg | 72 | ETI | IV | 8 mg/kg | 72 | NT | |
| 20 | Rabbit | NR | NR | Levo | NR | 50 mg/kg | 30 | ETI | IV | 16 mg/kg | 30 | NT | |
| 21 | Rabbit | NR | NR | Levo | Oral | 6.5 mg/kg | 72 | ETI | IV | 16 mg/kg | 72 | NT | |
| 22 | Cynos | NR | NR | Cipro | Oral | 10 mg/kg | 48 | ETI | IV | 8 mg/kg | 48 ** | PA det | |
| 23 | Cynos | NR | NR | Cipro | Oral | 10 mg/kg | 48 | ETI | IV | 8 mg/kg | 48 ** | PA det | |
| Author (Year) | Experiment Number | Treatments | Data Source | Animal Number | |||
|---|---|---|---|---|---|---|---|
| Challenged ## | Randomized or Assigned | ||||||
| Control | Anti-Toxin | Control | Anti-Toxin | ||||
| Migone (2009) [19] | 1 | Levo + placebo * | Levo + Raxi | FDA-BD | 40 | 20 | 20 |
| 2 | Cipro + placebo * | Cipro + Raxi | FDA-BD | 28 | 14 | 14 | |
| Migone (2015) [20] | 3 | Levo + Raxi-buffer | Levo + Raxi | PR | 180 | 37 | 39 |
| Kammanadiminti (2014) [22] | 4 | Levo + IGIV | Levo + AIG | PR | 16 | 8 | 8 |
| 5 | Levo + IGIV | Levo + AIG | PR | 16 | 8 | 7 | |
| 6 | Levo + IGIV | Levo + AIG | PR | 16 | 8 | 8 | |
| 7 | Levo + IGIV | Levo + AIG | PR | 16 | 8 | 8 | |
| 8 | Levo + IGIV | Levo + AIG | PR | 20 | 10 | 8 | |
| 9 | Levo + IGIV | Levo + AIG | PR | 72 | 20 | 23 | |
| 10 | Levo + IGIV | Levo + AIG | PR | 19 | 9 | 10 | |
| 11 | Levo + IGIV | Levo + AIG | PR | 72 | 8 | 7 | |
| FDA AIG (2015) [23] | 12 | Levo + IGIV | Levo + AIG | FDA-BD | 336 | 33 | 31 |
| 13 | Cipro + IGIV | Cipro + AIG | FDA-BD | 20 | 12 # | 12 # | |
| 14 | Cipro + IGIV | Cipro + AIG | FDA-BD | 20 | 12 # | 14 # | |
| Biron (2015) [24] | 15 | Doxy + Saline | Doxy + ETI | PR | 20 | 10 | 10 |
| Yamomato (2016) [25] | 16 | Levo ** | Levo + ETI | PR | 21 | 12 | 9 |
| 17 | Levo ** | Levo + ETI | PR | 21 | 12 | 9 | |
| FDA ETI (2015) [26] | 18 | Levo ** | Levo + ETI | FDA-BD | 32 | 5 | 4 |
| 19 | Levo ** | Levo + ETI | FDA-BD | 32 | 9 | 11 | |
| 20 | Levo ** | Levo + ETI | FDA-BD | 40 | 20 | 20 | |
| 21 | Levo ** | Levo + ETI | FDA-BD | 103 | 38 | 34 | |
| 22 | Cipro ** | Cipro + ETI | FDA-BD | 32 | 13 | 13 | |
| 23 | Cipro ** | Cipro + ETI | FDA-BD | 32 | 13 | 14 | |
| Author (Year) | Exp # | Agent | Species | Random. | Blind. | Pro. Samp. Size | Pro. Obs. Sched. | Pro. Euth. Crit. |
|---|---|---|---|---|---|---|---|---|
| Migone (2009) [19] | 1 | RAXI | Rabbit | Yes | Yes | Yes | NR | NR |
| 2 | RAXI | Cynos | Yes | Yes | Yes | NR | NR | |
| Migone (2015) [20] | 3 | RAXI | Rabbit | Yes | Yes | Yes | NR | NR |
| Kammanadiminti (2014) [22] | 4 | AIG | Rabbit | Yes | No | Yes | Yes | Yes |
| 5 | AIG | Rabbit | Yes | No | Yes | Yes | Yes | |
| 6 | AIG | Rabbit | Yes | No | Yes | Yes | Yes | |
| 7 | AIG | Rabbit | Yes | No | Yes | Yes | Yes | |
| 8 | AIG | Rabbit | Yes | No | Yes | Yes | Yes | |
| 9 | AIG | Rabbit | Yes | No | Yes | Yes | Yes | |
| 10 | AIG | Rabbit | Yes | No | Yes | Yes | Yes | |
| 11 | AIG | Rabbit | Yes | No | Yes | Yes | Yes | |
| FDA AIG (2015) [23] | 12 | AIG | Rabbit | Yes | Yes | Yes | Yes | Yes |
| 13 | AIG | Cynos | Yes | No | Yes | Yes | Yes | |
| 14 | AIG | Cynos | Yes | No | Yes | Yes | Yes | |
| Biron (2015) [24] | 15 | ETI | Rabbit | No | No | Yes | Yes | Yes |
| Yamomato (2016) [25] | 16 | ETI | Rabbit | Yes | No | Yes | Yes | Yes |
| 17 | ETI | Rabbit | Yes | No | Yes | Yes | Yes | |
| FDA ETI (2015) [26] | 18 | ETI | Rabbit | Yes | No | Yes | Yes | Yes |
| 19 | ETI | Rabbit | Yes | No | Yes | Yes | Yes | |
| 20 | ETI | Rabbit | Yes | No | Yes | Yes | Yes | |
| 21 | ETI | Rabbit | Yes | No | Yes | Yes | Yes | |
| 22 | ETI | Cynos | Yes | No | Yes | Yes | Yes | |
| 23 | ETI | Cynos | Yes | No | Yes | Yes | Yes |
| Report | Study | Challenge | Treatment Comparisons | Timing of Anti-Toxin Treatments * | Purpose of Study |
|---|---|---|---|---|---|
| Sweeney (2010) [16] | 1 | LT, ET or Diluent | None | NA | Investigate the survival and cardiopulmonary effects of LT or ET alone versus a diluent challenge |
| 2 | LT, ET, LT + ET or Diluent | None | NA | Investigate the survival and cardiopulmonary effects of LT + ET together versus a diluent challenge | |
| Barochia (2012) [17] | 3 | LT | HS ** vs. no HS | NA | Investigate the survival effects of HS alone versus no HS support with LT |
| Raxi + HS vs. HS alone | 0, 9, or 12 h | Investigate the survival effects of Raxi versus HS with LT | |||
| Remy (2015) [27] | 4 | ET | HS vs. no HS | NA | Investigate the survival effects of HS alone versus no HS with ET |
| Raxi + HS vs. HS alone | 0, 6, or 12 h | Investigate the survival effects of Raxi with HS versus HS alone with ET | |||
| 5 | LT + ET | Raxi + HS vs. HS alone | 0 or 6 h | Investigate the survival effects of Raxi with HS versus HS alone with LT + ET | |
| Suffredini (2017) [18] | 6 | LT + ET | AIG-IV + HS vs. HS alone | 0, 6 or 9 h | Investigate the survival effects of AIG-IV with HS versus HS alone with LT + ET |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Couse, Z.; Cui, X.; Li, Y.; Moayeri, M.; Leppla, S.; Eichacker, P.Q. A Review of the Efficacy of FDA-Approved B. anthracis Anti-Toxin Agents When Combined with Antibiotic or Hemodynamic Support in Infection- or Toxin-Challenged Preclinical Models. Toxins 2021, 13, 53. https://doi.org/10.3390/toxins13010053
Couse Z, Cui X, Li Y, Moayeri M, Leppla S, Eichacker PQ. A Review of the Efficacy of FDA-Approved B. anthracis Anti-Toxin Agents When Combined with Antibiotic or Hemodynamic Support in Infection- or Toxin-Challenged Preclinical Models. Toxins. 2021; 13(1):53. https://doi.org/10.3390/toxins13010053
Chicago/Turabian StyleCouse, Zoe, Xizhong Cui, Yan Li, Mahtab Moayeri, Stephen Leppla, and Peter Q. Eichacker. 2021. "A Review of the Efficacy of FDA-Approved B. anthracis Anti-Toxin Agents When Combined with Antibiotic or Hemodynamic Support in Infection- or Toxin-Challenged Preclinical Models" Toxins 13, no. 1: 53. https://doi.org/10.3390/toxins13010053
APA StyleCouse, Z., Cui, X., Li, Y., Moayeri, M., Leppla, S., & Eichacker, P. Q. (2021). A Review of the Efficacy of FDA-Approved B. anthracis Anti-Toxin Agents When Combined with Antibiotic or Hemodynamic Support in Infection- or Toxin-Challenged Preclinical Models. Toxins, 13(1), 53. https://doi.org/10.3390/toxins13010053