Therapeutic Applications of Botulinum Neurotoxin for Autonomic Symptoms in Parkinson’s Disease: An Updated Review


Abstract
:1. Introduction

2. Results


{kind=link}
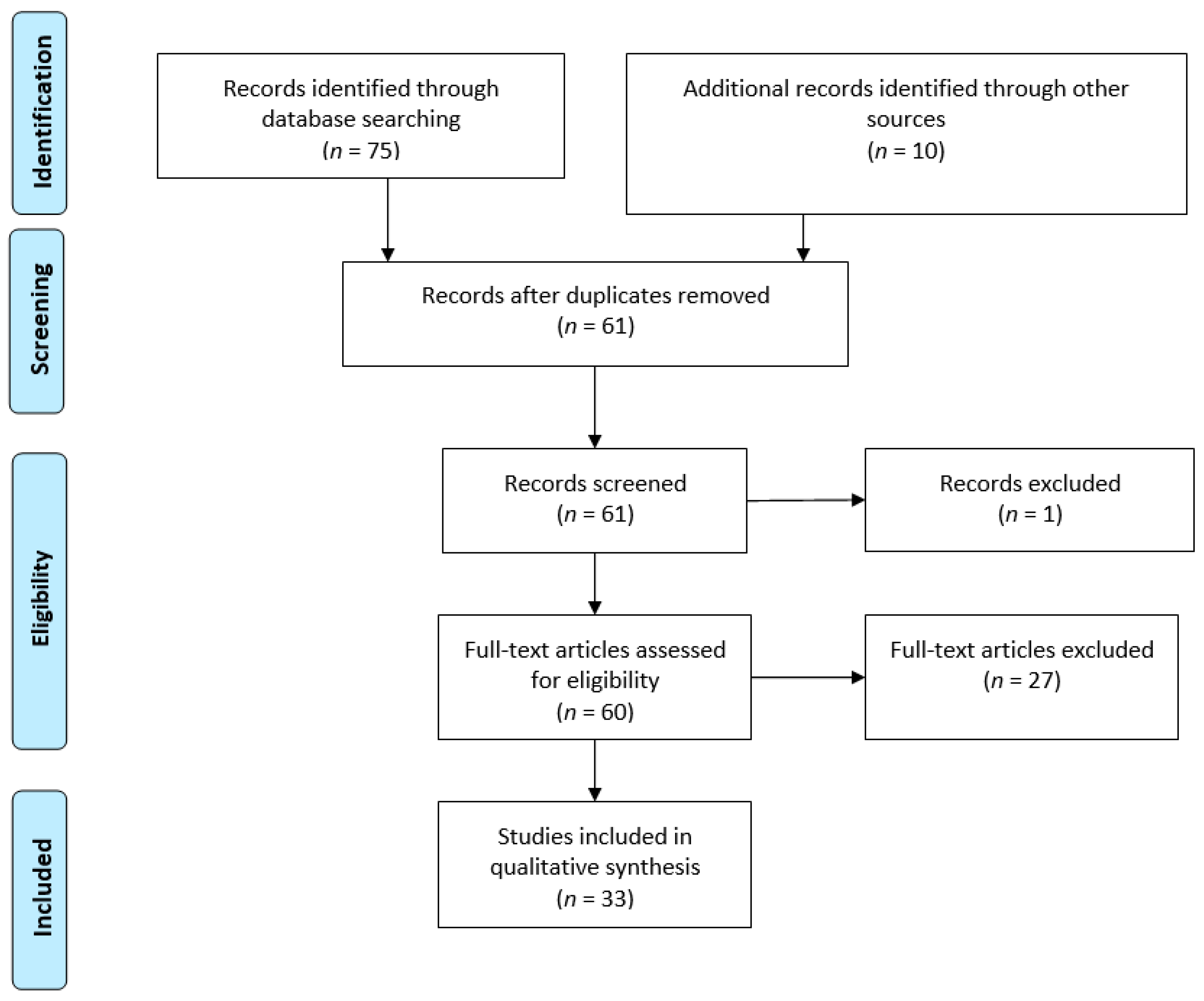{kind=link}
| Topic | Lead Author (Year) [Reference] | Type of Study | Toxin Type + Total Patients (If Applicable) | Result/Conclusion |
|---|---|---|---|---|
| Sialorrhea | Tiigimäe-Saar (2017) [30] | Retrospective cohort | abobotulinumtoxinA 38 (12 injected with BoNT via US guidance) | Significant decrease in salivary flow rate was observed in those treated with BoNT type A. No significant change was found in salivary composition at 1 month follow-up. |
| Hayes (2019) [31] | Review | A + B | Off-label BoNT injection into parotid or submandibular glands (with US guidance) can be an effective treatment for sialorrhea. | |
| Papesh (2019) [32] | Case report | onabotulinumtoxinA + rimabotulinumtoxinB 1 | Case report of parotitis and sialolithiasis following BoNT injection. | |
| Seppi (2019) [33] | Review | A + B | BoNT type B is efficacious and clinically useful for drooling based on one high-quality positive study. Generally, BoNT type A and type B are considered to pose an acceptable risk with specialized monitoring techniques. | |
| Kulshreshtha (2020) [34] | Review | A | BoNT is the best treatment for management of sialorrhea, but repeated injections are needed. | |
| Quarracino (2020) [35] | Expert opinion | A + B | Sialorrhea can be managed with BoNT injections and oral glycopyrrolate. | |
| Gastrointestinal Dysfunction | Triadafilopoulos (2017) [36] | Retrospective open cohort | not specified 14 | Endoscopic BoNT injection to the esophagus, pylorus or anal canal is safe, well-tolerated, and leads to symptomatic improvement of dysphagia, gastroparesis, and chronic anismus that lasts up to several months. |
| Ramprasad (2018) [37] | Review | A | BoNT type A can prove beneficial for patients who fail levodopa treatment and display significant upper esophageal sphincter dysfunction. | |
| Sharma (2018) [38] | Review | not specified | Chronic constipation is a common, nonmotor, and prodromal symptom in PD. Its underlying neuropathology may provide pathophysiological insight into PD. BoNT injection into the puborectalis may help dyssynergic defecation. | |
| Barbagelata (2019) [39] | Review | A | BoNT type A for dysphagia may be an effective and safe alternative to invasive procedures or may be useful to identify patients who might benefit from surgical myotomy. | |
| Mendoza-Velásquez (2019) [40] | Review | not specified | BoNT in the distal esophagus could improve dysphagia. | |
| Urinary Dysfunction | Brucker (2017) [41] | Review | onabotulinumtoxinA + abobotulinumtoxinA | BoNT can be used for intractable urinary incontinence in PD with a risk of impairing bladder emptying. |
| Madan (2017) [42] | Review | A | Intravesical BoNT has been shown to be effective in the management of urinary symptoms in PD patients, and there is evidence that it may improve detrusor sphincter dyssynergia. | |
| McDonald (2017) [43] | Review | A | Intravesical BoNT may be helpful for lower urinary tract symptoms in PD, but trials have been small and frequently lacked a suitable control group, making them vulnerable to placebo effect. Any patient undergoing intra-detrusor BoNT must be consented for possible urinary retention and need for an intermittent or indwelling catheter. | |
| Sakakibara (2018) [44] | Review | A | Intramural, multiple BoNT injection in the bladder seems to be a promising method to treat intractable detrusor overactivity in patients with PD. | |
| Mehnert (2019) [45] | Review | A | BoNT type A intra-detrusor injections are a safe treatment with few adverse events. BoNT type A intra-detrusor injections are recommended as second line treatment for neurogenic detrusor overactivity refractory to antimuscarinic treatment. | |
| Miller-Patterson (2020) [46] | Cross-sectional | not specified 308 | Men with PD are more likely than women to receive a medication, such as BoNT, for urinary symptom treatment, despite no difference in overall urinary symptom prevalence. | |
| Pain | Bruno (2017) [47] | Randomized controlled crossover trial | A 12 | BoNT for dystonic and musculoskeletal pain showed a mild, non-significant reduction in pain after 4 weeks compared to placebo. |
| Rana (2017) [48] | Review | not specified | BoNT has been shown to alleviate painful dystonias associated with PD, including blepharospasm, axial dystonia, camptocormia, and limb dystonia. | |
| Rieu (2018) [49] | Randomized controlled trial | incobotulinumtoxinA 45 | BoNT injections are effective for improving clinical state of parkinsonian patients with plantar flexion of toe dystonia. | |
| Buhidma (2020) [50] | Review | not specified | BoNT can be used for dystonic pain in PD. Treatment of pain in PD remains less than optimum. Rodent models may assist with better understanding the mechanism of PD-related pain. | |
| Buhmann (2020) [51] | Review | A | Off-label injection of BoNT into pain trigger points might be helpful. BoNT can also help with painful myotonus or spasms in the esophagus, pylorus, anal sphincter, or in painful detrusor hyperactivity of the bladder. | |
| Karnik (2020) [52] | Review | A | BoNT type A had a non-significant signal toward improving dystonic limb pain in PD. | |
| Tai (2020) [53] | Review | A | Pain is a heterogeneous symptom in PD. A randomized double-blind crossover study tested BoNT type A for limb pain in advanced PD. This treatment did not significantly reduce the pain score in the pain group; however, a subgroup analysis showed that it significantly improved dystonic pain. | |
| Multiple Topics | Jost (2017) [54] | Review | not specified | BoNT can be considered for use in focal hyperhidrosis. BoNT is also approved for the treatment of neurogenic and idiopathic detrusor hyperactivity and should be considered for therapy-resistant cases. |
| Shukla (2017) [27] | Review | A + B | BoNT can effectively ameliorate the symptoms of cervical dystonia, blepharospasm, sialorrhea, and hyperactive bladder and is increasingly being used for additional PD-related indications including limb dystonia, oromandibular dystonia, tremors, constipation, dysphagia, gastroparesis, and sweating dysfunction. | |
| Sławek (2017) [55] | Review | A + B | BoNT offers effective treatment for drooling and bladder dysfunctions and alternative treatment for constipation and pain related to parkinsonism. | |
| Safarpour (2018) [56] | Review | A + B | Literature supports a level A efficacy (established) for BoNT therapy in cervical dystonia and a level B efficacy (probably effective) for blepharospasm, hemifacial spasm, laryngeal dystonia (spasmodic dysphonia), task-specific dystonias, essential tremor, and PD rest tremor. | |
| Tater (2018) [57] | Review | A + B | BoNT is effective for apraxia of eyelid opening with blepharospasm in PD. BoNT is also effective for sialorrhea, axillary hyperhidrosis, detrusor overactivity, and pain in PD. | |
| Jocson (2019) [58] | Review | A + B | Uses of BoNT in idiopathic PD include sialorrhea, limb, dystonia, tremor, dyskinesias, freezing of gait, camptocormia, pisa syndrome, urinary dysfunction, constipation, dysphagia, eyelid opening apraxia, and blepharospasm. | |
| Chen (2020) [59] | Review | A + B | BoNT is effective for treatment of sialorrhea in PD. In addition, BoNT type A may improve gastroparesis and defecatory dysfunction in PD. BoNT type A has been demonstrated to be effective for the treatment of urinary symptoms in PD. | |
| Jankovic (2020) [7] | Review | not specified | BoNT is effective in controlling high-amplitude rest and postural hand tremor, which may be resistant to levodopa. BoNT may be also beneficial in the treatment of a variety of other non-levodopa responsive parkinsonian symptoms such as blepharospasm, apraxia of eyelid opening, anterocollis, camptocormia, bruxism, sialorrhea, seborrhea, hyperhidrosis, overactive bladder, and constipation. | |
| Savitt (2020) [60] | Review | not specified | Blepharospasm responds to BoNT injection of the eyelids. |
3. Discussion
3.1. Botulinum Neurotoxin for Sialorrhea
3.2. Botulinum Neurotoxin for Hyperhidrosis
3.3. Botulinum Neurotoxin for Gastrointestinal Dysfunction
3.4. Botulinum Neurotoxin for Urinary Dysfunction
3.5. Botulinum Neurotoxin for Pain
3.6. Botulinum Neurotoxin for Other Indications
4. Conclusions
5. Methods
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BoNT | botulinum neurotoxin |
| COMTIs | catechol-O-methyl transferase inhibitors |
| GI | gastrointestinal |
| MAOIs | monoamine oxidase inhibitors |
| PD | Parkinson’s disease |
| TeNT | tetanus toxin |
| US | ultrasound |
References
- Parkinson, J. An essay on the shaking palsy 1817. J. Neuropsychiatry Clin. Neurosci. 2002, 14, 223–236. [Google Scholar] [CrossRef] [PubMed]
- Mhyre, T.R.; Boyd, J.T.; Hamill, R.W.; Maguire-Zeiss, K.A. Parkinson’s disease. Subcell Biochem. 2012, 65, 389–455. [Google Scholar] [CrossRef] [Green Version]
- Gitler, A.D.; Dhillon, P.; Shorter, J. Neurodegenerative disease: Models, mechanisms, and a new hope. Dis. Models Mech. 2017, 10, 499–502. [Google Scholar] [CrossRef] [Green Version]
- Reeve, A.; Simcox, E.; Turnbull, D. Ageing and Parkinson’s disease: Why is advancing age the biggest risk factor? Ageing Res. Rev. 2014, 14, 19–30. [Google Scholar] [CrossRef] [PubMed]
- Marras, C.; Beck, J.C.; Bower, J.H.; Roberts, E.; Ritz, B.; Ross, G.; Tanner, C.M.; on behalf of the Parkinson’s Foundation P4 Group. Prevalence of Parkinson’s disease across North America. NPJ Parkinson’s Dis. 2018, 4, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Jankovic, J. Parkinson’s disease: Clinical features and diagnosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 368–376. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jankovic, J.; Tan, E.K. Parkinson’s disease: Etiopathogenesis and treatment. J. Neurol. Neurosurg. Psychiatry 2020, 91, 8. [Google Scholar] [CrossRef]
- Armstrong, M.J.; Okun, M.S. Diagnosis and treatment of Parkinson disease. JAMA 2020, 323, 548–560. [Google Scholar] [CrossRef]
- Pfeiffer, R.F. Non-motor symptoms in Parkinson’s disease. Parkinsonism Relat. Disord. 2016, 22, S119–S122. [Google Scholar] [CrossRef] [PubMed]
- Aerts, M.B.; Esselink, R.A.J.; Post, B.; van de Warrenburg, B.P.; Bloem, B.R. Improving the diagnostic accuracy in parkinsonism: A three-pronged approach. Pract. Neurol. 2012, 12, 77–87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munhoz, R.P.; Werneck, L.C.; Teive, H.A.G. The differential diagnoses of parkinsonism: Findings from a cohort of 1528 patients and a 10 years comparison in tertiary movement disorders clinics. Clin. Neurol. Neurosurg. 2010, 112, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Espay, A.J.; Schwarzschild, M.A.; Tanner, C.M.; Fernandez, H.H.; Simon, D.K.; Leverenz, J.B.; Lang, A.E. Biomarker-driven phenotyping in Parkinson’s disease: A translational missing link in disease-modifying clinical trials. Mov. Disord. 2017, 32, 319–324. [Google Scholar] [CrossRef]
- Trifonova, O.P.; Maslov, D.L.; Balashova, E.E.; Urazgildeeva, G.R.; Abaimov, D.A.; Fedotova, E.Y.; Lokhov, P.G. Parkinson’s disease: Available clinical and promising omics tests for diagnostics, disease risk assessment, and pharmacotherapy personalization. Diagnostics 2020, 10, 339. [Google Scholar] [CrossRef] [PubMed]
- Espay, A.J.; Vizcarra, J.A.; Marsili, L.; Lang, A.E.; Simon, D.K.; Merola, A.; Leverenz, J.B. Revisiting protein aggregation as pathogenic in sporadic Parkinson and Alzheimer diseases. Neurology 2019, 92, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Giguère, N.; Burke Nanni, S.; Trudeau, L.E. On cell loss and selective vulnerability of neuronal populations in Parkinson’s disease. Front. Neurol. 2018, 19, 455. [Google Scholar] [CrossRef] [PubMed]
- Annesley, S.J.; Lay, S.T.; De Piazza, S.W.; Sanislav, O.; Hammersley, E.; Allan, C.Y.; Fisher, P.R. Immortalized Parkinson’s disease lymphocytes have enhanced mitochondrial respiratory activity. Dis. Models Mech. 2016, 9, 1295–1305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaudhuri, K.R.; Sauerbier, A. Unravelling the nonmotor mysteries of Parkinson disease. Nat. Rev. Neurol. 2016, 12, 10–11. [Google Scholar] [CrossRef]
- Pezzoli, G.; Zini, M. Levodopa in Parkinson’s disease: From the past to the future. Expert Opin. Pharmacother. 2010, 11, 627–635. [Google Scholar] [CrossRef]
- Fabbri, M.; Coelho, M.; Guedes, L.C.; Chendo, I.; Sousa, C.; Rosa, M.M.; Ferreira, J.J. Response of non-motor symptoms to levodopa in late-stage Parkinson’s disease: Results of a levodopa challenge test. Parkinsonism Relat. Disord. 2017, 39, 37–43. [Google Scholar] [CrossRef]
- Rana, A.Q.; Ahmed, U.A.; Chaudry, Z.M.; Vasan, S. Parkinson’s disease: A review of non-motor symptoms. Expert Rev. Neurother. 2015, 15, 549–562. [Google Scholar] [CrossRef]
- Heusinkveld, J.E.; Hacker, M.L.; Turchan, M.; Davis, T.L.; Charles, D. Impact of tremor on patients with early stage Parkinson’s disease. Front. Neurol. 2018, 9, 628. [Google Scholar] [CrossRef] [Green Version]
- Emamzadeh, F.N.; Surguchov, A. Parkinson’s disease: Biomarkers, treatment, and risk factors. Front. Neurosci. 2018, 12, 612. [Google Scholar] [CrossRef] [PubMed]
- Dhaked, R.K.; Singh, M.K.; Singh, P.; Gupta, P. Botulinum toxin: Bioweapon & magic drug. Indian J. Med. Res. 2010, 132, 489–503. [Google Scholar]
- Jankovic, J. Botulinum toxin: State of the art. Mov. Disord. 2017, 32, 1131–1138. [Google Scholar] [CrossRef] [PubMed]
- Mills, R.; Bahroo, L.; Pagan, F. An update on the use of botulinum toxin therapy in Parkinson’s disease. Curr. Neurol. Neurosci. Rep. 2015, 15, 511. [Google Scholar] [CrossRef] [PubMed]
- Barr, J.R.; Moura, H.; Boyer, A.E.; Woolfitt, A.R.; Kalb, S.R.; Pavlopoulos, A. Botulinum neurotoxin detection and differentiation by mass spectrometry. Emerg. Infect. Dis. 2005, 11, 1578–1583. [Google Scholar] [CrossRef]
- Shukla, A.W.; Malaty, I.A. Botulinum toxin therapy for Parkinson’s disease. Semin Neurol. 2017, 37, 193–204. [Google Scholar] [CrossRef]
- Abrams, S.B.; Hallett, M. Clinical utility of different botulinum neurotoxin preparations. Toxicon 2013, 67, 81–86. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tiigimäe-Saar, J.; Tamme, T.; Taba, P. Saliva changes and the oral health in Parkinson’s disease. Mov. Disord. 2017, 32 (Suppl. 2), 35. [Google Scholar]
- Hayes, M.W.; Fung, V.S.C.; Kimber, T.E.; O’Sullivan, J.D. Updates and advances in the treatment of Parkinson disease. Med. J. Aust. 2019, 211, 277–283. [Google Scholar] [CrossRef]
- Papesh, K.; Nguyen, J. Parotitis as adverse event following BoNT injections for sialorrhea. Mov. Disord. 2019, 34 (Suppl. 2), S72. [Google Scholar]
- Seppi, K.; Ray Chaudhuri, K.; Coelho, M.; Fox, S.H.; Katzenschlager, R.; Perez Lloret, S.; Djamshidian-Tehrani, A. Update on treatments for nonmotor symptoms of Parkinson’s disease—An evidence-based medicine review. Mov. Disord. 2019, 34, 180–198. [Google Scholar] [CrossRef] [Green Version]
- Kulshreshtha, D.; Ganguly, J.; Jog, M. Managing autonomic dysfunction in Parkinson’s disease: A review of emerging drugs. Expert Opin. Emerg. Drugs 2020, 25, 37–47. [Google Scholar] [CrossRef]
- Quarracino, C.; Otero-Losada, M.; Capani, F.; Pérez-Lloret, S. State-of-the-art pharmacotherapy for autonomic dysfunction in Parkinson’s disease. Expert Opin. Pharmacother. 2020, 21, 445–457. [Google Scholar] [CrossRef] [PubMed]
- Triadafilopoulos, G.; Gandhy, R.; Barlow, C. Pilot cohort study of endoscopic botulinum neurotoxin injection in Parkinson’s disease. Parkinsonism Relat. Disord. 2017, 44, 33–37. [Google Scholar] [CrossRef]
- Ramprasad, C.; Douglas, J.Y.; Moshiree, B. Parkinson’s disease and current treatments for its gastrointestinal neurogastromotility effects. Curr. Treat Options Gastroenterol. 2018, 16, 489–510. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Kurek, J.; Morgan, J.C.; Wakade, C.; Rao, S.S.C. Constipation in Parkinson’s disease: A nuisance or nuanced answer to the pathophysiological puzzle? Curr. Gastroenterol. Rep. 2018, 20, 1. [Google Scholar] [CrossRef] [PubMed]
- Barbagelata, E.; Nicolini, A.; Tognetti, P. Swallowing dysfunctions in Parkinson’s disease patients: A novel challenge for the internist. Ital. J. Med. 2019, 13, 91–94. [Google Scholar] [CrossRef]
- Mendoza-Velásquez, J.J.; Flores-Vázquez, J.F.; Barrón-Velázquez, E.; Sosa-Ortiz, A.L.; Illigens, B.M.W.; Siepmann, T. Autonomic dysfunction in α-synucleinopathies. Front. Neurol. 2019, 10, 363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brucker, B.M.; Kalra, S. Parkinson’s disease and its effect on the lower urinary tract: Evaluation of complications and treatment strategies. Urol. Clin. N. Am. 2017, 44, 415–428. [Google Scholar] [CrossRef]
- Madan, A.; Ray, S.; Burdick, D.; Agarwal, P. Management of lower urinary tract symptoms in Parkinson’s disease in the neurology clinic. Int. J. Neurosci. 2017, 127, 1136–1149. [Google Scholar] [CrossRef]
- McDonald, C.; Winge, K.; Burn, D.J. Lower urinary tract symptoms in Parkinson’s disease: Prevalence, aetiology and management. Parkinsonism Relat. Disord. 2017, 35, 8–16. [Google Scholar] [CrossRef] [Green Version]
- Sakakibara, R.; Tateno, F.; Yamamoto, T.; Uchiyama, T.; Yamanishi, T. Urological dysfunction in synucleinopathies: Epidemiology, pathophysiology and management. Clin. Auton. Res. 2018, 28, 83–101. [Google Scholar] [CrossRef]
- Mehnert, U.; Chartier-Kastler, E.; de Wachter, S.; van Kerrebroeck, P.E.V.A.; van Koeveringe, G.A. The management of urine storage dysfunction in the neurological patient. SN Compr. Clin. Med. 2019, 3, 160–182. [Google Scholar] [CrossRef] [Green Version]
- Miller-Patterson, C.; Edwards, K.A.; Chahine, L.M. Sex disparities in autonomic symptom treatment in Parkinson’s disease. Mov. Disord. Clin. Pract. 2020, 7, 718–719. [Google Scholar] [CrossRef] [PubMed]
- Bruno, V.; Freitas, M.E.; Mancini, D.; Lui, J.P.; Miyasaki, J.; Fox, S.H. Botulinum toxin type A for pain in advanced Parkinson’s disease. Can. J. Neurol. Sci. 2018, 45, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rana, A.Q.; Qureshi, D.; Sabeh, W.; Mosabbir, A.; Rahman, E.; Sarfraz, Z.; Rana, R. Pharmacological therapies for pain in Parkinson’s disease—A review paper. Expert Rev. Neurother. 2017, 17, 1209–1219. [Google Scholar] [CrossRef]
- Rieu, I.; Degos, B.; Castelnovo, G.; Vial, C.; Durand, E.; Pereira, B.; Durif, F. Incobotulinum toxin A in Parkinson’s disease with foot dystonia: A double blind randomized trial. Parkinsonism Relat. Disord. 2018, 46, 9–15. [Google Scholar] [CrossRef]
- Buhidma, Y.; Rukavina, K.; Chaudhuri, K.R.; Duty, S. Potential of animal models for advancing the understanding and treatment of pain in Parkinson’s disease. NPJ Parkinson’s Dis. 2020, 6, 1. [Google Scholar] [CrossRef]
- Buhmann, C.; Kassubek, J.; Jost, W.H. Management of pain in Parkinson’s disease. J. Parkinson’s Dis. 2020, 10, S37–S48. [Google Scholar] [CrossRef] [PubMed]
- Karnik, V.; Farcy, N.; Zamorano, C.; Bruno, V. Current status of pain management in Parkinson’s disease. Can. J. Neurol. Sci. 2020, 47, 336–343. [Google Scholar] [CrossRef]
- Tai, Y.C.; Lin, C.H. An overview of pain in Parkinson’s disease. Clin. Parkinsonism Relat. Disord. 2020, 2, 1–8. [Google Scholar] [CrossRef]
- Jost, W.H. Autonomic dysfunction in Parkinson’s disease: Cardiovascular symptoms, thermoregulation, and urogenital symptoms. Int. Rev. Neurobiol. 2017, 134, 771–785. [Google Scholar] [PubMed]
- Sławek, J.; Madaliński, M. Botulinum toxin therapy for nonmotor aspects of Parkinson’s disease. Int. Rev. Neurobiol. 2017, 134, 1111–1142. [Google Scholar] [CrossRef]
- Safarpour, Y.; Jabbari, B. Botulinum toxin treatment of movement disorders. Curr. Treat. Options Neurol. 2018, 20, 4. [Google Scholar] [CrossRef]
- Tater, P.; Pandey, S. Botulinum toxin in movement disorders. Neurol. India 2018, 66, S79–S89. [Google Scholar] [CrossRef]
- Jocson, A.; Lew, M. Use of botulinum toxin in Parkinson’s disease. Parkinsonism Relat. Disord. 2019, 59, 57–64. [Google Scholar] [CrossRef]
- Chen, Z.; Li, G.; Liu, J. Autonomic dysfunction in Parkinson’s disease: Implications for pathophysiology, diagnosis, and treatment. Neurobiol. Dis. 2020, 134, 104700. [Google Scholar] [CrossRef]
- Savitt, J.; Aouchiche, R. Management of visual dysfunction in patients with Parkinson’s disease. J. Parkinson’s Dis. 2020, 10, S49–S56. [Google Scholar] [CrossRef]
- Papesh, K.; Nguyen, J. Atropine as alternate therapy for treatment of sialorrhea in Parkinson’s disease. Mov. Disord. 2019, 34 (Suppl. 2), S72–S73. [Google Scholar]
- Foresti, C.; Stabile, A. Botulinum toxin treatment of sialorrhea in children. Toxicon 2018, 156 (Suppl. 1), S34–S35. [Google Scholar] [CrossRef]
- Khan, W.U.; Campisi, P.; Nadarajah, S.; Shakur, Y.A.; Khan, N.; Semenuk, D.; Connolly, B. Botulinum toxin A for treatment of sialorrhea in children: An effective, minimally invasive approach. Arch. Otolaryngol. Head Neck Surg. 2011, 137, 339–344. [Google Scholar] [CrossRef] [Green Version]
- Van Wamelen, D.J.; Leta, V.; Podlewska, A.M.; Wan, Y.M.; Krbot, K.; Jaakkola, E.; Chaudhuri, K.R. Exploring hyperhidrosis and related thermoregulatory symptoms as a possible clinical identifier for the dysautonomic subtype of Parkinson’s disease. J. Neurol. 2019, 266, 1736–1742. [Google Scholar] [CrossRef] [Green Version]
- Nóbrega, A.C.; Rodrigues, B.; Torres, A.C.; Scarpel, R.D.A.; Neves, C.A.; Melo, A. Is drooling secondary to a swallowing disorder in patients with Parkinson’s disease? Parkinsonism Relat. Disord. 2008, 14, 243–245. [Google Scholar] [CrossRef]
- Braak, H.; de Vos, R.A.; Bohl, J.; Del Tredici, K. Gastric alpha-synuclein immunoreactive inclusions in Meissner’s and Auerbach’s plexuses in cases staged for Parkinson’s disease-related brain pathology. Neurosci. Lett. 2006, 396, 67–72. [Google Scholar] [CrossRef]
- Akbar, U.; Dham, B.; He, Y. Trends of aspiration pneumonia in Parkinson’s disease in the United States, 1979–2010. Parkinson Relat. Disord. 2015, 21, 1082–1086. [Google Scholar] [CrossRef]
- Fereshtehnejad, S.M.; Yao, C.; Pelletier, A.; Montplaisir, J.Y.; Gagnon, J.F.; Postuma, R.B. Evolution of prodromal Parkinson’s disease and dementia with Lewy bodies: A prospective study. Brain J. Neurol. 2019, 142, 2051–2067. [Google Scholar] [CrossRef] [PubMed]
- ClinicalTrials.gov [Internet]. Bethesda (MD): National Library of Medicine (US). Identifier NCT02660359. Dysport® Treatment of Urinary Incontinence in Adults Subjects With Neurogenic Detrusor Overactivity (NDO) Due to Spinal Cord Injury or Multiple Sclerosis—Study 2 (CONTENT2). 21 January 2016. Available online: https://clinicaltrials.gov/ct2/show/NCT02660359 (accessed on 1 February 2021).
- Valkovic, P.; Minar, M.; Singliarova, H.; Harsany, J.; Hanakova, M.; Martinkova, J.; Benetin, J. Pain in Parkinson’s disease: A cross-sectional study of its prevalence, types, and relationship to depression and quality of life. PLoS ONE 2015, 10, e0136541. [Google Scholar] [CrossRef]
- Beiske, A.G.; Loge, J.H.; Rønningen, A.; Svensson, E. Pain in Parkinson’s disease: Prevalence and characteristics. Pain 2009, 141, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Rana, A.Q.; Kabir, A.; Dogu, O.; Patel, A.; Khondker, S. Prevalence of blepharospasm and apraxia of eyelid opening in patients with parkinsonism, cervical dystonia and essential tremor. Eur. Neurol. 2012, 68, 318–321. [Google Scholar] [CrossRef] [PubMed]
- Hallett, M.; Evinger, C.; Jankovic, J.; Stacy, M. BEBRF International Workshop. Update on blepharospasm: Report from the BEBRF International Workshop. Neurology 2008, 71, 1275–1282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, K.E.; Rastall, D.; Eggenberger, E. Treatment of blepharospasm/hemifacial spasm. Curr. Treat. Options Neurol. 2017, 19, 41. [Google Scholar] [CrossRef] [PubMed]
| Toxin Property | OnabotulinumtoxinA | AbobotulinumtoxinA | RimabotulinumtoxinB | IncobotulinmtoxinA |
|---|---|---|---|---|
| Year introduced | 1989 | 1991 | 2000 | 2005 |
| Trade name | BOTOX® | Dysport® | Myobloc/NeuroBloc® | Xeomin® |
| Mechanism of action | Cleaves SNAP 25 | Cleaves SNAP 25 | Cleaves VAMP | Cleaves SNAP 25 |
| Molecular weight (kD) | 900 | 500–900 | 700 | 150 |
| Total protein (ng/vial) | ~5 | ~5 | ~50 | ~0.6 |
| Units/vial | 50, 100, or 200 | 300 or 500 | 2500, 5000, or 10,000 | 50 or 100 |
| Shelf life (months) | 36 | 24 | 24 | 36 |
| Formulation | Vacuum dried | Freeze dried | Sterile solution | Freeze dried |
| pH after reconstitution | 7.4 | 7.4 | 5.6 | 7.4 |
| FDA-approved uses (in adults unless indicated) | Cervical dystonia (16 years and up), blepharospasm (12 years and up), hyperactive bladder, upper and lower limb spasticity, strabismus (12 years and up), glabellar lines, axillary hyperhidrosis, and chronic migraine | Cervical dystonia, glabellar lines, upper limb spasticity, and lower limb spasticity (2 years and up) | Cervical dystonia and chronic sialorrhea | Cervical dystonia, chronic sialorrhea, blepharospasm, and upper limb spasticity (2 years and up) |
| Off-label uses | Sialorrhea, hemifacialspasm, focal limb dystonia, oromandibular dystonia, tremors, tics, and tardive dyskinesia | Sialorrhea, focal limb dystonia, oromandibular dystonia, and tremors | Focal limb dystonia and oromandibular dystonia | Focal limb dystonia and oromandibular dystonia |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitchell, S.D.; Sidiropoulos, C. Therapeutic Applications of Botulinum Neurotoxin for Autonomic Symptoms in Parkinson’s Disease: An Updated Review. Toxins 2021, 13, 226. https://doi.org/10.3390/toxins13030226
Mitchell SD, Sidiropoulos C. Therapeutic Applications of Botulinum Neurotoxin for Autonomic Symptoms in Parkinson’s Disease: An Updated Review. Toxins. 2021; 13(3):226. https://doi.org/10.3390/toxins13030226
Chicago/Turabian StyleMitchell, Steven D., and Christos Sidiropoulos. 2021. "Therapeutic Applications of Botulinum Neurotoxin for Autonomic Symptoms in Parkinson’s Disease: An Updated Review" Toxins 13, no. 3: 226. https://doi.org/10.3390/toxins13030226
APA StyleMitchell, S. D., & Sidiropoulos, C. (2021). Therapeutic Applications of Botulinum Neurotoxin for Autonomic Symptoms in Parkinson’s Disease: An Updated Review. Toxins, 13(3), 226. https://doi.org/10.3390/toxins13030226