Expanded Haemodialysis as a Current Strategy to Remove Uremic Toxins



Abstract
:1. Introduction
2. HDx Clinical Evidences
2.1. Uremic Toxin Removal Efficacy
2.1.1. HDx vs. HDF
2.1.2. HDx vs. Conventional HD
3. Safety
3.1. Albumin Removal
3.2. Microbial Contamination
3.3. Adverse Events
4. Quality of Life (QOL)
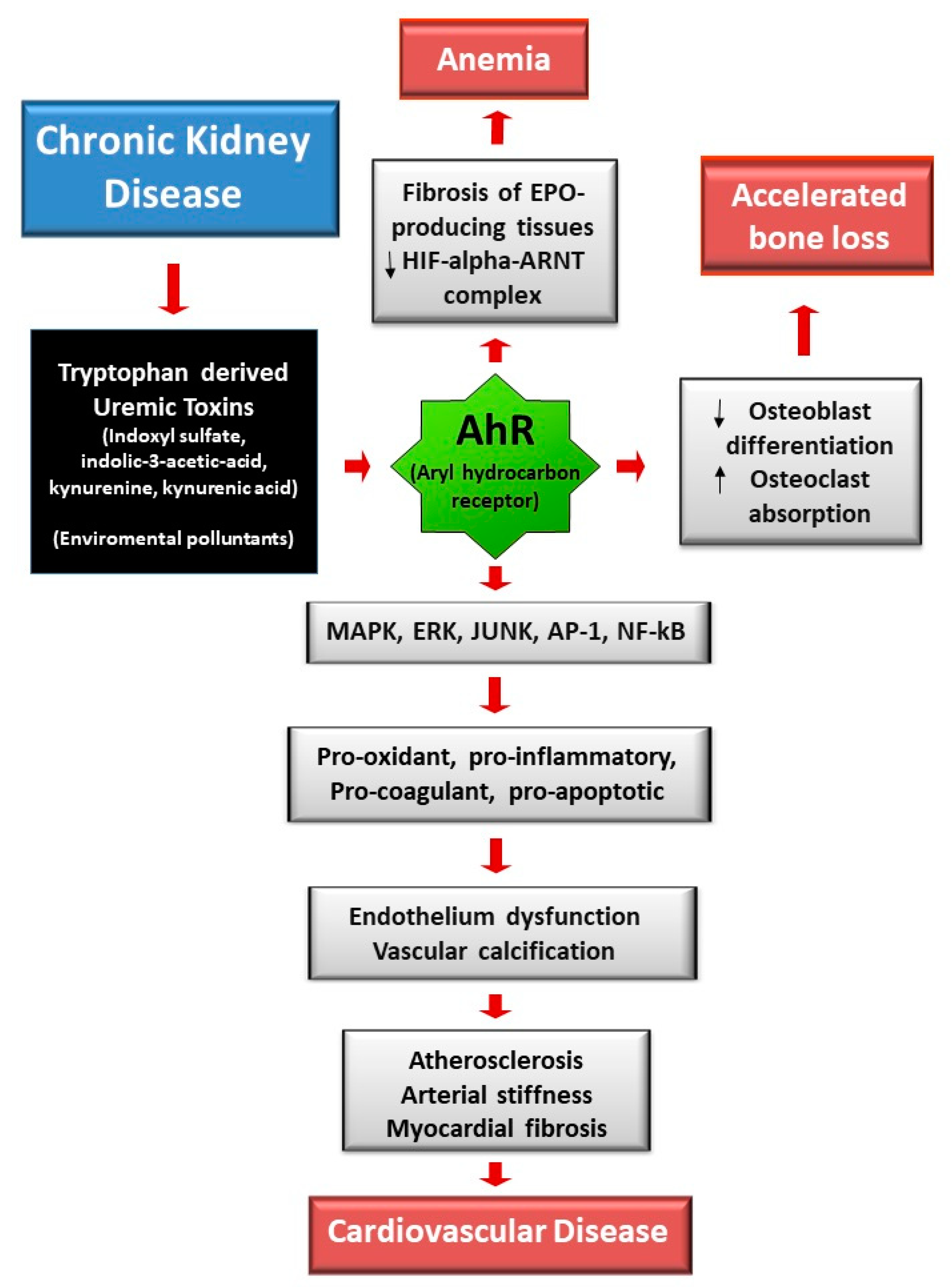
5. Potential Mechanisms and Pathogenetic Hypothesis
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cozzolino, M.; Mangano, M.; Stucchi, A.; Ciceri, P.; Conte, F.; Galassi, A. Cardiovascular disease in dialysis patients. Nephrol. Dial. Transpl. 2018, 33, iii28–iii34. [Google Scholar] [CrossRef] [PubMed]
- Viggiano, D.; Wagner, C.A.; Martino, G.; Nedergaard, M.; Zoccali, C.; Unwin, R.; Capasso, G. Mechanisms of cognitive dysfunction in CKD. Nat. Rev. Nephrol. 2020, 16, 452–469. [Google Scholar] [CrossRef]
- Cozzolino, M.; Magagnoli, L.; Ciceri, P.; Conte, F.; Galassi, A. Effects of a medium cut-off (Theranova®) dialyser on haemodialysis patients: A prospective, cross-over study. Clin. Kidney J. 2021, 14, 382–389. [Google Scholar] [CrossRef] [Green Version]
- Cozzolino, M.; Ronco, C. Medium Cut-Off Membranes: Incremental or Quantum Leap Innovation in Haemodialysis? Blood Purif. 2020, 22, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Belmouaz, M.; Diolez, J.; Bauwens, M.; Duthe, F.; Ecotiere, L.; Desport, E.; Bridoux, F. Comparison of hemodialysis with medium cut-off dialyzer and on-line hemodiafiltration on the removal of small and middle-sized molecules. Clin. Nephrol. 2017. [Google Scholar] [CrossRef] [PubMed]
- García-Prieto, A.M.; Vega, A.; Abad, S.; Macías, N.; Aragoncillo, I.; Hurtado, E.; Delgado, A.; Torres, E.; Barbieri, D.; Luño, J. Evaluation of the efficacy of a very high permeability dialyser and comparison with another high-flux dialyser in online haemodiafiltration. Clin. Kidney J. 2019, 13, 114–115. [Google Scholar] [CrossRef]
- Maduell, F.; Rodas, L.; Broseta, J.J.; Gomez, M.; Xipell, M.; Guillen, E.; Montagud-Marrahi, E.; Arias-Guillén, M.; Fontseré, N.; Vera, M.; et al. Medium Cut-Off Dialyzer versus Eight Hemodiafiltration Dialyzers: Comparison Using a Global Removal Score. Blood Purif. 2019, 48, 167–174. [Google Scholar] [CrossRef]
- Kirsch, A.H.; Lyko, R.; Nilsson, L.-G.; Beck, W.; Amdahl, M.; Lechner, P.; Schneider, A.; Wanner, C.; Rosenkranz, A.R.; Krieter, D.H. Performance of hemodialysis with novel medium cut-off dialyzers. Nephrol. Dial. Transpl. 2016, 32, 165–172. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.H.; Kim, S.-H.; Park, H.Y.; Jung, K.S.; Lee, M.H.; Jhee, J.H.; Lee, J.E.; Choi, H.Y.; Park, H.C.; Kim, T.Y. Removal of large middle molecules via haemodialysis with medium cut-off membranes at lower blood flow rates: An observational prospective study. BMC Nephrol. 2019, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zickler, D.; Schindler, R.; Willy, K.; Martus, P.; Pawlak, M.; Storr, M.; Hulko, M.; Boehler, T.; Glomb, M.A.; Liehr, K.; et al. Medium Cut-Off (MCO) Membranes Reduce Inflammation in Chronic Dialysis Patients—A Randomized Controlled Clinical Trial. PLoS ONE 2017, 12, e0169024. [Google Scholar] [CrossRef]
- Cho, N.-J.; Park, S.; Islam, I.; Song, H.-Y.; Lee, E.Y.; Gil, H.-W. Long-term effect of medium cut-off dialyzer on middle uremic toxins and cell-free hemoglobin. PLoS ONE 2019, 14, e0220448. [Google Scholar] [CrossRef] [Green Version]
- Lindgren, A.; Fjellstedt, E.; Christensson, A. Comparison of Hemodialysis Using a Medium Cutoff Dialyzer versus Hemodiafiltration: A Controlled Cross-Over Study. Int. J. Nephrol. Renov. Dis. 2020, 13, 273–280. [Google Scholar] [CrossRef]
- Lim, J.-H.; Park, Y.; Yook, J.-M.; Choi, S.-Y.; Jung, H.-Y.; Choi, J.-Y.; Park, S.-H.; Kim, C.-D.; Kim, Y.-L.; Cho, J.-H. Randomized controlled trial of medium cut-off versus high-flux dialyzers on quality of life outcomes in maintenance hemodialysis patients. Sci. Rep. 2020, 10, 7780. [Google Scholar] [CrossRef] [PubMed]
- Weiner, D.E.; Falzon, L.; Skoufos, L.; Bernardo, A.; Beck, W.; Xiao, M.; Tran, H. Efficacy and Safety of Expanded Hemodialysis with the Theranova 400 Dialyzer. Clin. J. Am. Soc. Nephrol. 2020, 15, 1310–1319. [Google Scholar] [CrossRef]
- Krishnasamy, R.; Hawley, C.M.; Jardine, M.J.; Roberts, M.A.; Cho, Y.; Wong, M.; Heath, A.; Nelson, C.L.; Sen, S.; Mount, P.F.; et al. A tRial Evaluating Mid Cut-Off Value Membrane Clearance of Albumin and Light Chains in HemoDialysis Patients: A Safety Device Study. Blood Purif. 2020, 49, 468–478. [Google Scholar] [CrossRef] [PubMed]
- Sevinc, M.; Hasbal, N.B.; Yilmaz, V.; Basturk, T.; Ahbap, E.; Sakaci, T.; Ozcafer, P.N.; Unsal, A. Comparison of Circulating Levels of Uremic Toxins in Hemodialysis Patients Treated with Medium Cut-Off Membranes and High-Flux Membranes: Theranova in Sisli Hamidiye Etfal (THE SHE) Randomized Control Study. Blood Purif. 2020, 49, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Reis, T.; Martino, F.; Dias, P.; De Freitas, G.R.R.; Filho, E.R.D.S.; De Azevedo, M.L.C.; Reis, F.; Cozzolino, M.; Rizo-Topete, L.; Ronco, C. Removal of middle molecules with medium cutoff dialyzer in patients on short frequent hemodialysis. Hemodial. Int. 2020. [Google Scholar] [CrossRef]
- Pérez-Alba, A.; Reque-Santiváñez, J.; Vázquez-Gómez, M.; Pons-Prades, R. Expanded home hemodialysis: Case reports. Int. Urol. Nephrol. 2020, 52, 977–980. [Google Scholar] [CrossRef]
- Rambabova, B.I.; Trajceska, L.; Biljali, S.; Balkanov, T.; Dejanov, P.; Spasovski, G. Efficacy of Medium Cut-Off Dialyzer and Comparison with Standard High-Flux Hemodialysis. Blood Purif. 2020, 1–7. [Google Scholar] [CrossRef]
- Belmouaz, M.; Bauwens, M.; Hauet, T.; Bossard, V.; Jamet, P.; Joly, F.; Chikhi, E.; Joffrion, S.; Gand, E.; Bridoux, F. Comparison of the removal of uraemic toxins with medium cut-off and high-flux dialysers: A randomized clinical trial. Nephrol. Dial. Transpl. 2019, 1, 328–335. [Google Scholar] [CrossRef]
- Yamamoto, S. Molecular mechanisms underlying uremic toxin-related systemic disorders in chronic kidney disease: Focused on β2-microglobulin-related amyloidosis and indoxyl sulfate-induced atherosclerosis—Oshima Award Address 2016. Clin. Exp. Nephrol. 2019, 23, 151–157. [Google Scholar] [CrossRef] [Green Version]
- Liabeuf, S.; Lenglet, A.; Desjardins, L.; Neirynck, N.; Glorieux, G.; Lemke, H.-D.; Vanholder, R.; Diouf, M.; Choukroun, G.; Massy, Z.A. Plasma beta-2 microglobulin is associated with cardiovascular disease in uremic patients. Kidney Int. 2012, 82, 1297–1303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mutluay, R.; Konca, C.; Erten, Y.; Paşaoğlu, H.; Değer, S.M.; Ağirgün, Ç.; Derici, Ü.; Arinsoy, T.; Sindel, Ş. Predictive markers of asymptomatic atherosclerosis in end-stage renal disease patients. Ren. Fail. 2010, 32, 448–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plotnikov, E.Y.; Chupyrkina, A.A.; Pevzner, I.B.; Isaev, N.K.; Zorov, D.B. Myoglobin causes oxidative stress, increase of NO production and dysfunction of kidney’s mitochondria. Biochim. Biophys. Acta (BBA) Mol. Basis Dis. 2009, 1792, 796–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parry, S.N.; Ellis, N.; Li, Z.; Maitz, P.; Witting, P.K. Myoglobin Induces Oxidative Stress and Decreases Endocytosis and Monolayer Permissiveness in Cultured Kidney Epithelial Cells without Affecting Viability. Kidney Blood Press. Res. 2008, 31, 16–28. [Google Scholar] [CrossRef]
- Chen, T.K.; Estrella, M.M.; Appel, L.J.; Coresh, J.; Luo, S.; Reiser, J.; Obeid, W.; Parikh, C.R.; Grams, M.E. Biomarkers of Immune Activation and Incident Kidney Failure with Replacement Therapy: Findings from the African American Study of Kidney Disease and Hypertension. Am. J. Kidney Dis. 2021, 1. [Google Scholar] [CrossRef]
- Jalal, D.; Sanford, B.; Renner, B.; Eyck, P.T.; Laskowski, J.; Cooper, J.; Sun, M.; Zakharia, Y.; Spitz, D.; Dokun, A.; et al. Detection of pro angiogenic and inflammatory biomarkers in patients with CKD. Sci. Rep. 2021, 11, 1–16. [Google Scholar] [CrossRef]
- Lim, Y.; Sidor, N.; Tonial, N.; Che, A.; Urquhart, B. Uremic Toxins in the Progression of Chronic Kidney Disease and Cardiovascular Disease: Mechanisms and Therapeutic Targets. Toxins 2021, 13, 142. [Google Scholar] [CrossRef]
- Haring, R.; Friedrich, N.; Völzke, H.; Vasan, R.S.; Felix, S.B.; Dörr, M.; Meyer zu Schwabedissen, H.E.; Nauck, M.; Wallaschofski, H. Positive association of serum prolactin concentrations with all-cause and cardiovascular mortality. Eur. Heart J. 2014, 35, 1215–1221. [Google Scholar] [CrossRef] [Green Version]
- Carrero, J.J.; Kyriazis, J.; Sonmez, A.; Tzanakis, I.; Qureshi, A.R.; Stenvinkel, P.; Saglam, M.; Stylianou, K.; Yaman, H.; Taslipinar, A.; et al. Prolactin levels, endothelial dysfunction, and the risk of cardiovascular events and mortality in patients with CKD. Clin. J. Am. Soc. Nephrol. 2012, 7, 207–215. [Google Scholar] [CrossRef] [Green Version]
- Fraser, S.D.; Fenton, A.; Harris, S.; Shardlow, A.; Liabeuf, S.; Massy, Z.A.; Burmeister, A.; Hutchison, C.A.; Landray, M.; Emberson, J.; et al. The Association of Serum Free Light Chains with Mortality and Progression to End-Stage Renal Disease in Chronic Kidney Disease: Systematic Review and Individual Patient Data Meta-analysis. Mayo Clin. Proc. 2017, 92, 1671–1681. [Google Scholar] [CrossRef] [Green Version]
- Faul, C.; Amaral, A.P.; Oskouei, B.; Hu, M.C.; Sloan, A.; Isakova, T.; Gutiérrez, O.M.; Aguillon-Prada, R.; Lincoln, J.; Hare, J.M.; et al. FGF23 induces left ventricular hypertrophy. J. Clin. Investig. 2011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, F.N.; Falkner, B.; Gidding, S.; Price, H.E.; Keith, S.W.; Langman, C.B. Fibroblast Growth Factor-23 in Obese, Normotensive Adolescents Is Associated with Adverse Cardiac Structure. J. Pediatr. 2014, 165, 738–743.e1. [Google Scholar] [CrossRef] [Green Version]
- Deppisch, R.M.; Beck, W.; Goehl, H.; Ritz, E. Complement components as uremic toxins and their potential role as mediators of microinflammation. Kidney Int. Suppl. 2001, 78, S271–S277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafi, T.; Parekh, R.S.; Jaar, B.G.; Plantinga, L.C.; Oberai, P.C.; Eckfeldt, J.H.; Levey, A.S.; Powe, N.R.; Coresh, J. Serum b-trace protein and risk of mortality in incident hemodialysis patients. Clin. J. Am. Soc. Nephrol. 2012, 7, 1435–1445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inoue, T.; Eguchi, Y.; Matsumoto, T.; Kijima, Y.; Kato, Y.; Ozaki, Y.; Waseda, K.; Oda, H.; Seiki, K.; Node, K.; et al. Lipocalin-type prostaglandin Dsynthase is a powerful biomarker for severity of stable coronary artery disease. Atherosclerosis 2008, 201, 385–391. [Google Scholar] [CrossRef]
- Eguchi, Y.; Eguchi, N.; Oda, H.; Seiki, K.; Kijima, Y.; Matsu-Ura, Y.; Urade, Y.; Hayaishi, O. Expression of lipocalin-type prostaglandin D synthase (beta-trace) in human heart and its accumulation in the coronary circulation of angina patients. Proc. Natl. Acad. Sci. USA 1997, 94, 14689–14694. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bullen, A.L.; Katz, R.; Jotwani, V.; Garimella, P.S.; Lee, A.K.; Estrella, M.M.; Shlipak, M.G.; Ix, J.H. Biomarkers of Kidney Tubule Health, CKD Progression, and Acute Kidney Injury in SPRINT (Systolic Blood Pressure Intervention Trial) Participants. Am. J. Kidney Dis. 2021, 12. [Google Scholar] [CrossRef]
- Robles, N.R.; Gomez, J.L.; Pino, G.G.; Valladares, J.; Gallego, R.H.; Cerezo, I. Alfa-1-microglobulina: Valor pronóstico en la enfermedad renal crónica. Med. Clínica 2020. [Google Scholar] [CrossRef]
- Bhatraju, P.K.; Zelnick, L.R.; Shlipak, M.; Katz, R.; Kestenbaum, B. Association of Soluble TNFR-1 Concentrations with Long-Term Decline in Kidney Function: The Multi-Ethnic Study of Atherosclerosis. J. Am. Soc. Nephrol. 2018, 29, 2713–2721. [Google Scholar] [CrossRef] [Green Version]
- Goicoechea, M.; de Vinuesa, S.G.; Gómez-Campderá, F.; Luño, J. Predictive cardiovascular risk factors in patients with chronic kidney disease (CKD). Kidney Int. 2005, 67, S35–S38. [Google Scholar] [CrossRef] [Green Version]
- Mallamaci, F.; Zoccali, C.; Parlongo, S.; Tripepi, G.; Benedetto, F.A.; Cutrupi, S.; Bonanno, G.; Fatuzzo, P.; Rapisarda, F.; Seminara, G.; et al. Diagnostic value of troponin T for alterations in left ventricular mass and function in dialysis patients. Kidney Int. 2002, 62, 1884–1890. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Puthumana, J.; Thiessen-Philbrook, H.; Xu, L.; Coca, S.G.; Garg, A.X.; Himmelfarb, J.; Bhatraju, P.K.; Ikizler, T.A.; Siew, E.D.; Ware, L.B.; et al. Biomarkers of inflammation and repair in kidney disease progression. J. Clin. Investig. 2021, 131. [Google Scholar] [CrossRef] [PubMed]
- Spiller, F.; Carlos, D.; Souto, F.O.; de Freitas, A.; Soares, F.S.; Vieira, S.M.; Paula, F.J.; Alves-Filho, J.C.; Cunha, F.Q. a1-Acid glycoprotein decreases neutrophil migration and increases susceptibility to sepsis in diabetic mice. Diabetes 2012, 61, 1584–1591. [Google Scholar] [CrossRef] [Green Version]
- Anderson, C.E.; Hamm, L.L.; Batuman, G.; Kumbala, D.R.; Chen, C.-S.; Kallu, S.G.; Siriki, R.; Gadde, S.; Kleinpeter, M.A.; Krane, N.K.; et al. The association of angiogenic factors and chronic kidney disease. BMC Nephrol. 2018, 19, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allawati, H.; Dallas, L.; Nair, S.; Palmer, J.; Thaikandy, S.; Hutchison, C. A Pharmacokinetic Study Comparing the Clearance of Vancomycin during Haemodialysis Using Medium Cut-Off Membrane (Theranova) and High-Flux Membranes (Revaclear). Toxins 2020, 12, 317. [Google Scholar] [CrossRef] [PubMed]
- Voigt, M.; Gebert, M.; Haug, U.; Hulko, M.; Storr, M.; Boschetti-De-Fierro, A.; Beck, W.; Krause, B. Retention of beneficial molecules and coagulation factors during haemodialysis and haemodiafiltration. Sci. Rep. 2019, 9, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Lim, J.-H.; Jeon, Y.; Yook, J.-M.; Choi, S.-Y.; Jung, H.-Y.; Choi, J.-Y.; Park, S.-H.; Kim, C.-D.; Kim, Y.-L.; Cho, J.-H. Medium cut-off dialyzer improves erythropoiesis stimulating agent resistance in a hepcidin-independent manner in maintenance hemodialysis patients: Results from a randomized controlled trial. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Yeter, H.H.; Korucu, B.; Akcay, O.F.; Derici, K.; Derici, U.; Arinsoy, T. Effects of medium cut-off dialysis membranes on inflammation and oxidative stress in patients on maintenance hemodialysis. Int. Urol. Nephrol. 2020, 52, 1779–1789. [Google Scholar] [CrossRef]
- Ciceri, P.; Tettamanti, G.; Galassi, A.; Magagnoli, L.; Fabresse, N.; Alvarez, J.-C.; Massy, Z.A.; Messa, P.; Cozzolino, M. Pro-calcifying analysis of uraemic serum from patients treated with medium cut-off membrane in a prospective, cross-over study. Clin. Kidney J. 2020, 1–10. [Google Scholar] [CrossRef]
- Gama-Axelsson, T.; Heimbürger, O.; Stenvinkel, P.; Bárány, P.; Lindholm, B.; Qureshi, A.R. Serum Albumin as Predictor of Nutritional Status in Patients with ESRD. Clin. J. Am. Soc. Nephrol. 2012, 7, 1446–1453. [Google Scholar] [CrossRef]
- Bunch, A.; Sanchez, R.; Nilsson, L.; Bernardo, A.A.; Vesga, J.I.; Ardila, F.; Guerrero, I.M.; Sanabria, R.M.; Rivera, A.S.; The Colombian Registry of Expanded Hemodialysis investigators. Medium cut-off dialyzers in a large population of hemodialysis patients in Colombia: COREXH registry. Ther. Apher. Dial. 2021, 25, 33–43. [Google Scholar] [CrossRef] [PubMed]
- Schepers, E.; Glorieux, G.; Eloot, S.; Hulko, M.; Boschetti-De-Fierro, A.; Beck, W.; Krause, B.; Van Biesen, W. Assessment of the association between increasing membrane pore size and endotoxin permeability using a novel experimental dialysis simulation set-up. BMC Nephrol. 2018, 19, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hulko, M.; Dietrich, V.; Koch, I.; Gekeler, A.; Gebert, M.; Beck, W.; Krause, B. Pyrogen retention: Comparison of the novel medium cut-off (MCO) membrane with other dialyser membranes. Sci. Rep. 2019, 9, 6791. [Google Scholar] [CrossRef] [PubMed]
- Alarcon, J.C.; Bunch, A.; Ardila, F.; Zuñiga, E.; Vesga, J.I.; Rivera, A.; Sánchez, R.; Sanabria, R.M.; On behalf of the Colombian Registry of Expanded Hemodialysis Investigators. Impact of Medium Cut-Off Dialyzers on Patient-Reported Outcomes: COREXH Registry. Blood Purif. 2021, 50, 110–118. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Kopple, J.D.; Block, G.; Humphreys, M.H. Association among SF36 quality of life measures and nutrition, hospitalization, and mortality in hemodialysis. J. Am. Soc. Nephrol. 2001, 12, 2797–2806. [Google Scholar] [CrossRef]
- Trojanowicz, B.; Ulrich, C.; Fiedler, R.; Martus, P.; Storr, M.; Boehler, T.; Werner, K.; Hulko, M.; Zickler, D.; Willy, K.; et al. Modulation of leucocytic angiotensin-converting enzymes expression in patients maintained on high-permeable haemodialysis. Nephrol. Dial. Transpl. 2017, 33, 34–43. [Google Scholar] [CrossRef]
- Ciceri, P.; Galassi, A.; Alfieri, C.; Messa, P.; Cozzolino, M. Uremic Patients with Increased Vascular Calcification Score Have Serum with High Calcific Potential: Role of Vascular Smooth Muscle Cell Osteoblastic Differentiation and Apoptosis. Blood Purif. 2019, 48, 142–149. [Google Scholar] [CrossRef]
- Zimmermann, J.; Herrlinger, S.; Pruy, A.; Metzger, T.; Wanner, C. Inflammation enhances cardiovascular risk and mortality in hemodialysis patients. Kidney Int. 1999, 55, 648–658. [Google Scholar] [CrossRef] [Green Version]
- Willy, K.; Hulko, M.; Storr, M.; Speidel, R.; Gauss, J.; Schindler, R.; Zickler, D. In Vitro Dialysis of Cytokine-Rich Plasma with High and Medium Cut-Off Membranes Reduces Its Procalcific Activity. Artif. Organs 2017, 41, 803–809. [Google Scholar] [CrossRef]
- Willy, K.; Girndt, M.; Voelkl, J.; Fiedler, R.; Martus, P.; Storr, M.; Schindler, R.; Zickler, D. Expanded Haemodialysis Therapy of Chronic Haemodialysis Patients Prevents Calcification and Apoptosis of Vascular Smooth Muscle Cells in vitro. Blood Purif. 2017, 45, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Ciceri, P.; Elli, F.; Braidotti, P.; Falleni, M.; Tosi, D.; Bulfamante, G.; Block, G.A.; Cozzolino, M. Iron citrate reduces high phosphate-induced vascular calcification by inhibiting apoptosis. Atherosclerosis 2016, 254, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Ciceri, P.; Falleni, M.; Tosi, D.; Martinelli, C.; Cannizzo, S.; Marchetti, G.; Monforte, A.D.; Bulfamante, G.; A Block, G.; Messa, P.; et al. Therapeutic Effect of Iron Citrate in Blocking Calcium Deposition in High Pi-Calcified VSMC: Role of Autophagy and Apoptosis. Int. J. Mol. Sci. 2019, 20, 5925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallée, M.; Dou, L.; Cerini, C.; Poitevin, S.; Brunet, P.; Burtey, S. The Aryl Hydrocarbon Receptor-Activating Effect of Uremic Toxins from Tryptophan Metabolism: A New Concept to Understand Cardiovascular Complications of Chronic Kidney Disease. Toxins 2014, 6, 934–949. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Year | 1st Author Publication | N Patients | Dialysis Treatment | Time | Study Design | MM Significantly Removed by MCO Pre- and Post-Dialysis | MM Significantly Removed by MCO End Study | |
|---|---|---|---|---|---|---|---|---|
| HDx vs. HDF | 2017 | Kirsch [8] | 39 | HDF+HF HD+HF HD+MCO | One midweek dialysis | Myoglobin, beta-2 microglobulin, kappa and lambdaFLC, CFD, alpha1-microglobulin, YKL40 * | - | |
| 2018 | Belmouaz [5] | 10 | HDF+HF HD+MCO | 12 months | Switch from OL-HDF to HD MCO | - | No difference | |
| 2018 | Garcia-Prieto [6] | 18 | HDF+HF HD+HF HD+MCO | 3 weeks | Midweek dialysis, 3 consecutive weeks | Myoglobin, beta-2 microglobulin, prolactin, alpha1 acid glycoprotein **. | - | |
| 2019 | Kim [9] | 6 | HDF+HF HD+HF HD+MCO | 3 weeks | Midweek dialysis, 3 consecutive weeks | Myoglobin, lambda FLC * | - | |
| 2019 | Maduell [7] | 22 | HD+MCO+ HDF+8 different dialyzers | 9 weeks | 9 dialysis sessions once a week | No difference | - | |
| HDx vs. HD | 2017 | Zickler [10] | 48 | HD, MCO vs. HF | 12 weeks | 12 weeks (4+8) | - | kappa and lambda FLC, sTNFR1 |
| 2019 | Cho [11] | 57 | HD, MCO vs. HF | 12 months | 12 months | beta-2 microglobulin, kappa and lambda FLC, CFH | No difference | |
| 2020 | Lindgren [12] | 16 | HDF+HF HD+MCO | 4 weeks | 1 single dialysis section OL-HDF-2w washout-MCO | No difference | - | |
| 2020 | Lim [13] | 49 | HD, MCO vs. HF | 12 weeks | 12 weeks | No difference | kappa and lambda FLC | |
| 2020 | Weiner [14] | 172 | HD, MCO vs. HF | 24 weeks | 24 weeks | - | beta-2 microglobulin, CFD, kappa and lambda FLC, TNFalpha | |
| 2020 | Krishnasamy [15] | 89 | HD, MCO vs. HF | 32 w | 4 weeks HF+24 week MCO +4 weeks HF | - | kappa and lambda FLC | |
| 2020 | Sevinc [16] | 52 | HD, MCO vs. HF | 6 months | 3 months+3 months pre-post dialysis | Myoglobin, beta-2 microglobulin, kappa and lambda FLC (RR) | beta-2 microglobulin, kappa and lambda FLC, VEGF | |
| 2020 | Reis [17] | 15 | HD, MCO vs. HF | 2 m | 5 sessions/week 2 h 30 min each (short frequent HD) | - | Prolactin | |
| 2020 | Perez-Alba [18] | 7 | HD, MCO | 12 months | Home hemodialysis | - | beta-2 microglobulin | |
| 2020 | Rambabova [19] | 4 | HD, MCO vs. HF | 12 weeks | Pre-post dialysis | Myoglobin, beta-2 microglobulin, kappa and lambda FLC | - | |
| 2020 | Belmouaz [20] | 40 | HD, MCO vs. HF | 6 m | 3 months+3 months pre-post dialysis | beta-2 microglobulin, kappa and lambda FLC | Myoglobin, beta-2 microglobulin, prolactin, FGF23, homocysteine, kappa and lambda FLC (RR) |
| Middle Molecule. | MW (KDa) | Possible Role in Uremia | Studies Evaluating the Removal | |
|---|---|---|---|---|
| SMM | beta2 microglobulin | 11 | Dialysis related amyloidosis, inflammation, immune-dysfunction, mortality [21,22] | [6,7,8,11,12,14,16,18,19,20] |
| myoglobin | 16.7 | Oxidative stress, mitochondrial dysfunction, organ damage [23,24,25] | [6,7,8,9,12,16,19] | |
| TNFalpha | 17.3 | Left ventricular hypertrophy, anorexia, protein muscle breakdown [26,27,28] | [14] | |
| prolactin | 22 | Cardiovascular events, amplification of inflammatory cytokine response [29,30] | [6,7,17,20] | |
| kappa FLC | 22.5 | Inflammation, infection, mortality [31] | [8,10,11,13,14,15,16,19,20] | |
| FGF-23 | 22.5 | Cardiovascular events [32,33] | [20] | |
| CFD | 24 | Over-activity of complement system [34] | [8,14] | |
| beta trace | 25 | Atherosclerosis, cardiovascular mortality [35,36,37] | [12] | |
| LMM | alpha1 microglobulin | 26 | Inhibition leukocyte migration, chemiotaxis, IL-2 secretion [38,39] | [7,8] |
| sTNFR1 | 34 | Cardiovascular events [26,40] | [10] | |
| troponin T | 35 | Cardiovascular events [41,42] | [12] | |
| YKL40 | 40 | Local tissue inflammation and fibrosis [38,43] | [8] | |
| alpha1 acid glycoprotein | 41 | Inhibition leukocyte migration, secondary immunodeficiency [44] | [6,7] | |
| VEGF | 42 | Cardiomyopathy, left ventricular dysfunction [45] | [16] | |
| lambda FLC | 45 | Inflammation, infection, mortality [31] | [8,9,10,11,13,14,15,16,19,20] |
| Year | 1st Author Publication | N pz | Dialysis Treatment | Time | Study Design | Albumin Significant Reduction by MCO | Albumin Values (Baseline vs. End of MCO Period) | |
|---|---|---|---|---|---|---|---|---|
| HDx vs. HDF | 2017 | Kirsch [8] | 39 | HD+HF HDF+HF HD+MCO | One midweek dialysis | tendency * | 2.9–3.2 g filter AA 4.8–4.9 g filterBB 7.3 gr filter CC ** | |
| 2018 | Belmouaz [5] | 10 | HD, MCO | 12 months | Switch from OL-HDF to HD MCO | No | ||
| 2018 | Garcia-Prieto [6] | 18 | HDF+HF HD+HF HD+MCO | 3 weeks | Midweek dialysis, 3 consecutive weeks | No | 0.03 ± 0.01 g/session | |
| 2019 | Kim [9] | 6 | HD+HF HDF+HF HD+MCO | 3 weeks | Midweek dialysis, 3 consecutive weeks | No | 3.77 ± 0.3 to 3.58 ± 0.32 g/dL pre-post dialysis session | |
| 2019 | Maduell [7] | 22 | HD+MCO HDF with 8 different dialyzers | 9 weeks | 9 dialysis sessions once a week | No | 10.3 ± 6.5 RR% pre-post dialysis session | |
| HDx vs. HD | 2017 | Zickler [10] | 48 | HD, MCO vs. HF | 12 weeks | 12 weeks (4 + 8 extension) | Yes | 37.0 ± 3.6 to 35.3 ± 3.7 g/L |
| 2019 | Cozzolino [3] | 20 | HD, MCO vs. HF | 6 months | 3 months+3 months | Yes | −0.45 g/dL | |
| 2019 | Cho [11] | 57 | HD, MCO vs. HF | 12 months | 12 months | No | 3.96 ± 0.31 to 3.94 ± 0.37 g/dL | |
| 2020 | Lindgren [12] | 16 | HDF+HF HD+MCO | 4 weeks | 1 single dialysis section OL-HDF-2w wo-MCO | No | −2.02 ± 3.9 RR% pre-post dialysis session | |
| 2020 | Lim [13] | 49 | HD, MCO vs. HF | 12 weeks | 12 weeks | No | 4.11 ± 0.38 vs. 3.98 ± 0.27 g/dl | |
| 2020 | Weiner [14] | 172 | HD, MCO vs. HF | 24 week | 24 week | No | 4.0 ± 0.3 vs. 4.0 ± 0.3 g/dl | |
| 2020 | Krishnasamy [15] | 89 | HD, MCO vs. HF | 32 weeks | 4 weeks HF + 24 weeks MCO + 4 weeks HF | No | 35.8 ± 3.9 vs. 35.1 ± 4.0 g/L | |
| 2020 | Sevinc [16] | 52 | HD, MCO vs. HF | 6 months | 3 months+3 months pre-post dialysis | Yes | 3.88 to 3.62 g/L | |
| 2020 | Reis [17] | 15 | HD, MCO vs. HF | 2 months | 5 sessions/week 2 h 30 min each | Yes | 39.9 ± 3.7 vs. 38.3 ± 3.3 g/L | |
| 2020 | Perez-Alba [18] | 7 | HD, MCO | 12 months | Home haemodialysis | No | ||
| 2020 | Rambabova [19] | 4 | HD, MCO vs. HF | 12 weeks | Pre-post dialysis | No | 40.50 ± 4.79 vs. 42.25 ± 4.50 g/L | |
| 2020 | Belmouaz [20] | 40 | HD, MCO vs. HF | 6 months | 3 months+3 months pre-post dialysis | Yes | 38.2 ± 4.1 vs. 36.9 ± 4.3 g/L | |
| 2020 | Yeter [24] | 42 | HD, MCO; HF; LF | 6 months | 6 months | No | 4.00 ± 0.25 vs. 3.84 ± 0.26 g/dl | |
| 2020 | Bunch [52] | 638 | HD, MCO | 12 months | 12 months | Yes | −1.8% cumulative change |
| Year | 1st Author Publication | N pz | Dialysis Treatment | Time | Study Design | Parameter Tested | Parameters Significantly Improved by MCO |
|---|---|---|---|---|---|---|---|
| 2020 | Lim [13] | 49 | HD, MCO vs. HF | 12 weeks | 12 weeks | KDQoL-SF36, pruritus | Physical functioning, physical role, morning pruritus distribution, frequencing of scracing during sleep. |
| 2020 | Weiner [14] | 172 | HD, MCO vs. HF | 24 weeks | 24 weeks | KDQoL-SF36, EQ-5D-5L | No difference |
| 2020 | Krishnasamy [15] | 89 | HD, MCO vs. HF | 32 weeks | 4 weeks HF + 24 weeks MCO + 4 weeks HF | 6 monthsWT, MIS, RLS, QOL | No difference |
| 2020 | Reis [17] | 15 | HD, MCO vs. HF | 2 months | 5 sessions/week 2 h 30 min each (short frequent HD) | KDQoL-SF36 | KDQoL-SF36 |
| 2020 | Alarcon [54] | 638 | HD, MCO vs. HF | 12 months | 12 months | KDQoL-SF36, DSI, RLS | RLS 3 KDQoL-SF36 domains: -symptoms -effects of kidney disease -burden of kidney disease |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciceri, P.; Cozzolino, M. Expanded Haemodialysis as a Current Strategy to Remove Uremic Toxins. Toxins 2021, 13, 380. https://doi.org/10.3390/toxins13060380
Ciceri P, Cozzolino M. Expanded Haemodialysis as a Current Strategy to Remove Uremic Toxins. Toxins. 2021; 13(6):380. https://doi.org/10.3390/toxins13060380
Chicago/Turabian StyleCiceri, Paola, and Mario Cozzolino. 2021. "Expanded Haemodialysis as a Current Strategy to Remove Uremic Toxins" Toxins 13, no. 6: 380. https://doi.org/10.3390/toxins13060380
APA StyleCiceri, P., & Cozzolino, M. (2021). Expanded Haemodialysis as a Current Strategy to Remove Uremic Toxins. Toxins, 13(6), 380. https://doi.org/10.3390/toxins13060380