Intramuscular Neural Arborization of the Latissimus Dorsi Muscle: Application of Botulinum Neurotoxin Injection in Flap Reconstruction



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
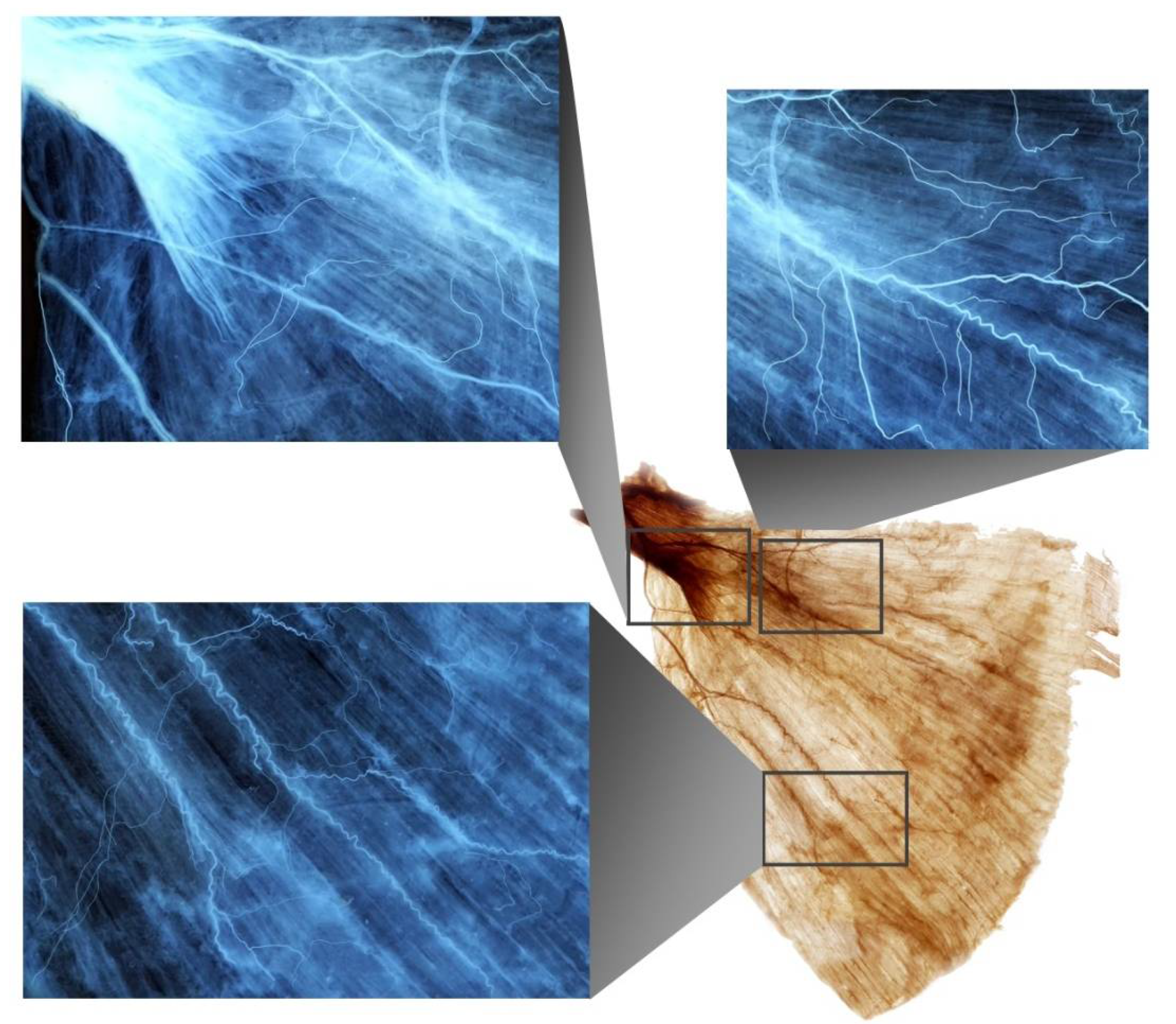
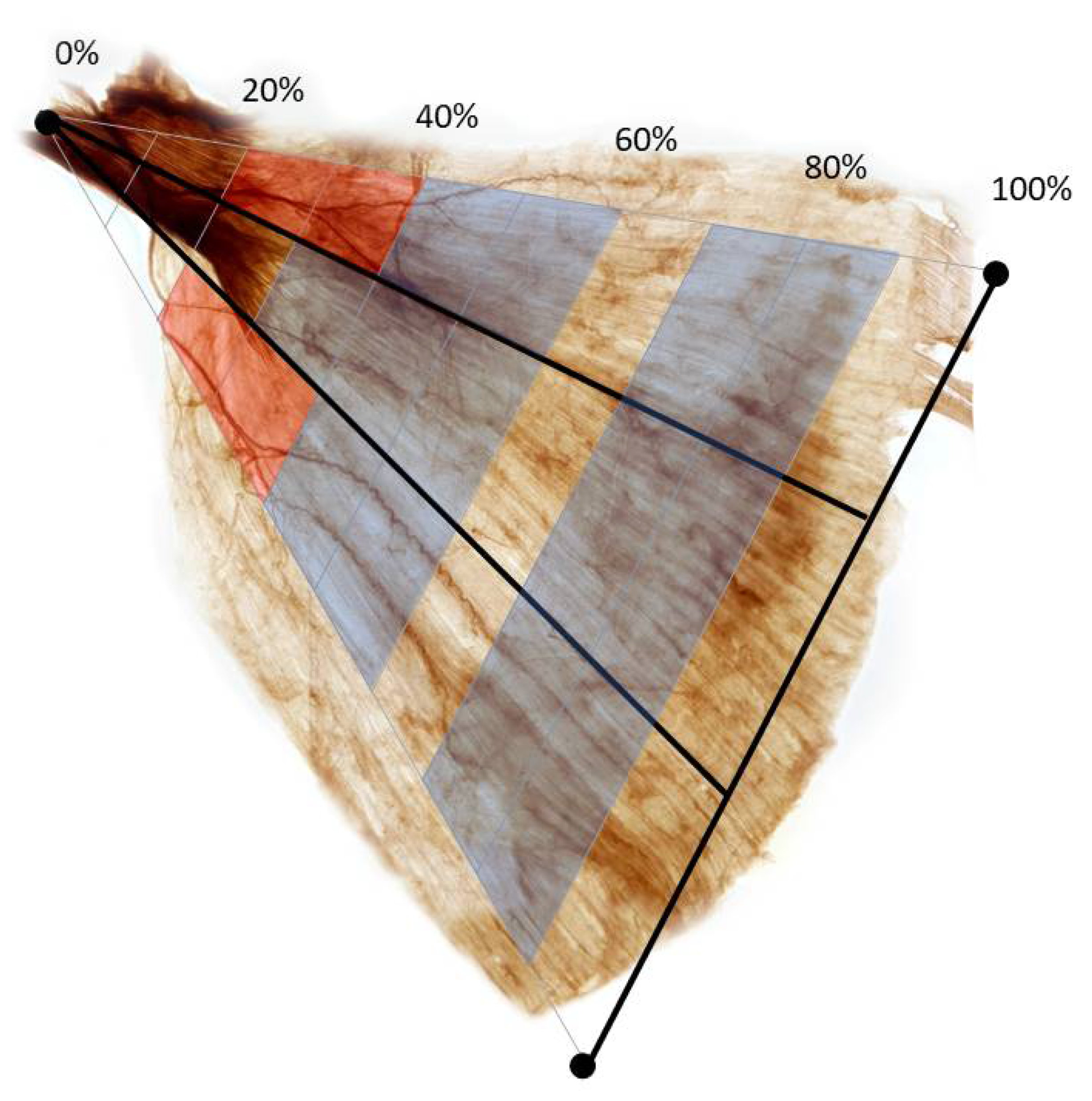
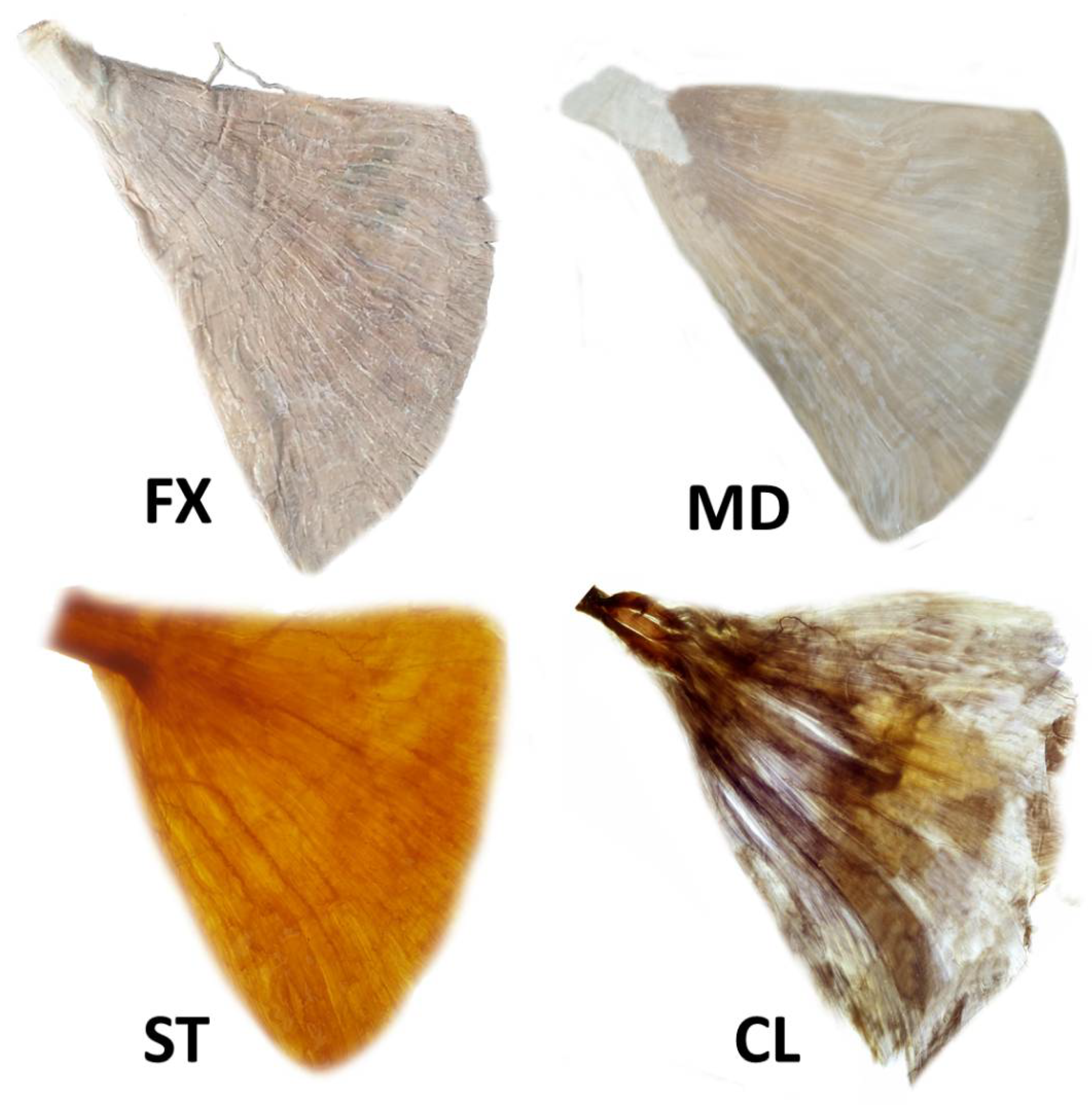
2.1. Intramuscular Arborization Patterns of the LD Muscle
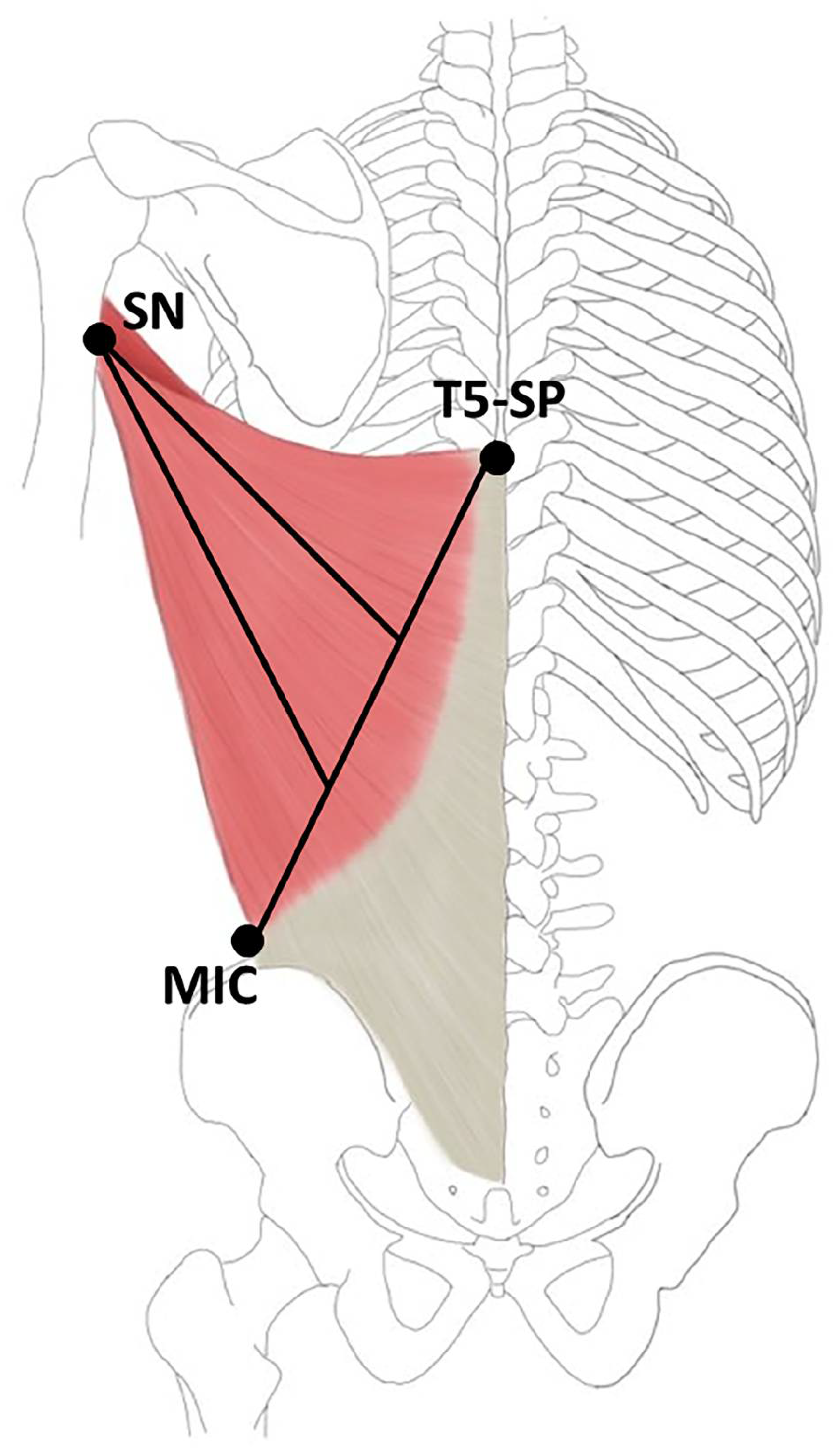
2.2. Nerve Entry Point of the LD Muscle
3. Discussion
4. Materials and Methods
Modified Sihler Staining
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, A.; Champaneria, M.C.; Maxwell, G.P. The efficacy of botulinum toxin A in post-mastectomy breast reconstruction: A pilot study. Aesthet. Surg. J. 2015, 35, 402–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rainsbury, R.M. Breast-sparing reconstruction with latissimus dorsi miniflaps. Eur. J. Surg. Oncol. 2002, 28, 891–895. [Google Scholar] [CrossRef] [PubMed]
- Paillocher, N.; Florczak, A.S.; Richard, M.; Classe, J.M.; Oger, A.S.; Raro, P.; Wernert, R.; Lorimier, G. Evaluation of mastectomy with immediate autologous latissimus dorsi breast reconstruction following neoadjuvant chemotherapy and radiation therapy: A single institution study of 111 cases of invasive breast carcinoma. Eur. J. Surg. Oncol. 2016, 42, 949–955. [Google Scholar] [CrossRef] [PubMed]
- Navin, C.; Agrawal, A.; Kolar, K.M. The use of latissimus dorsi miniflap for reconstruction following breast-conserving surgery: Experience of a small breast unit in a district hospital. World J. Surg. 2007, 31, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Munhoz, A.M.; Aldrighi, C.; Montag, E.; Arruda, E.G.; Aldrighi, J.M.; Filassi, J.R.; Ferreira, M.C. Periareolar skin-sparing mastectomy and latissimus dorsi flap with biodimensional expander implant reconstruction: Surgical planning, outcome, and complications. Plast. Reconstr. Surg. 2007, 119, 1637–1649; discussion 1650–1652. [Google Scholar] [CrossRef]
- Figus, A.; Mazzocchi, M.; Dessy, L.A.; Curinga, G.; Scuderi, N. Treatment of muscular contraction deformities with botulinum toxin type A after latissimus dorsi flap and sub-pectoral implant breast reconstruction. J. Plast. Reconstr. Aesthet. Surg. 2009, 62, 869–875. [Google Scholar] [CrossRef]
- Denewer, A.; Farouk, O. Can nipple-sparing mastectomy and immediate breast reconstruction with modified extended latissimus dorsi muscular flap improve the cosmetic and functional outcome among patients with breast carcinoma? World J. Surg. 2007, 31, 1169–1177. [Google Scholar] [CrossRef]
- Sternberg, E.G.; Perdikis, G.; McLaughlin, S.A.; Terkonda, S.P.; Waldorf, J.C. Latissimus dorsi flap remains an excellent choice for breast reconstruction. Ann. Plast. Surg. 2006, 56, 31–35. [Google Scholar] [CrossRef]
- Patel, N.G.; Ramakrishnan, V. Microsurgical Tissue Transfer in Breast Reconstruction. Clin. Plast. Surg. 2017, 44, 345–359. [Google Scholar] [CrossRef]
- Kroll, S.S.; Sharma, S.; Koutz, C.; Langstein, H.N.; Evans, G.R.D.; Robb, G.L.; Chang, D.W.; Reece, G.P. Postoperative morphine requirements of free TRAM and DIEP flaps. Plast. Reconstr. Surg. 2001, 107, 338–341. [Google Scholar] [CrossRef] [PubMed]
- Shah, J.P.; Haribhakti, V.; Loree, T.R.; Sutaria, P. Complications of the pectoralis major myocutaneous flap in head and neck reconstruction. Am. J. Surg. 1990, 160, 352–355. [Google Scholar] [CrossRef]
- Merve, A.; Mitra, I.; Swindell, R.; Homer, J.J. Shoulder morbidity after pectoralis major flap reconstruction for head and neck cancer. Head Neck 2009, 31, 1470–1476. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.; Sarkar, S.; Kavarana, N.; Bhathena, H.; Mehta, A. Complications of the pectoralis major myocutaneous flap in the oral cavity: A prospective evaluation of 220 cases. Plast. Reconstr. Surg. 1996, 98, 31–37. [Google Scholar] [CrossRef]
- Trignano, E.; Dessy, L.A.; Fallico, N.; Rampazzo, A.; Bassiri, B.; Mazzocchi, M.; Scuderi, N.; Chen, H.C. Treatment of pectoralis major flap myospasms with botulinum toxin type A in head and neck reconstruction. J. Plast. Reconstr. Aesthet. Surg. 2012, 65, e23–e28. [Google Scholar] [CrossRef]
- Senior, M.A.; Fourie, L.R. Botox and the management of pectoral spasm after subpectoral implant insertion. Plast. Reconstr. Surg. 2000, 106, 224–225. [Google Scholar] [CrossRef]
- Cattin, T.; Govender, S. Botulinum toxin for tethering of breast implant. Plast. Reconstr. Surg. 2005, 116, 686–688. [Google Scholar] [CrossRef]
- Losken, A.; Nicholas, C.S.; Pinell, X.A.; Carlson, G.W. Outcomes evaluation following bilateral breast reconstruction using latissimus dorsi myocutaneous flaps. Ann. Plast. Surg. 2010, 65, 17–22. [Google Scholar] [CrossRef]
- Temiz, G.; Yesiloglu, N.; Sirinoglu, H.; Akpinar, A.C.; Sarici, M.; Filinte, D.; Filinte, G.T.; Bozkurt, M. Increasing the survival of transverse rectus abdominis musculocutaneous flaps with a Botulinum toxin-A injection: A comparison of surgical and chemical flap delay methods. J. Plast. Reconstr. Aesthet. Surg. 2016, 69, 944–951. [Google Scholar] [CrossRef]
- Kim, Y.S.; Roh, T.S.; Lee, W.J.; Yoo, W.M.; Tark, K.C. The effect of botulinum toxin A on skin flap survival in rats. Wound Repair Regen. 2009, 17, 411–417. [Google Scholar] [CrossRef]
- Fathi, M.; Fathi, H.; Mazloumi, M.; Khalilzadeh, O.; Amanpour, S.; Meysamie, A.; Mashali, L.; Kardar, M.H. Preventive effect of botulinum toxin A in microanastomotic thrombosis: A rabbit model. J. Plast. Reconstr. Aesthet. Surg. 2010, 63, e720–e724. [Google Scholar] [CrossRef] [PubMed]
- Clemens, M.W.; Higgins, J.P.; Wilgis, E.F. Prevention of anastomotic thrombosis by botulinum toxin a in an animal model. Plast. Reconstr. Surg. 2009, 123, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Camargo, C.H.; Teive, H.A.; Zonta, M.; Silva, G.C.; Oliveira, M.R.; Roriz, M.M.; Brandi, I.V.; Becker, N.; Scola, R.H.; Werneck, L.C. Botulinum toxin type A in the treatment of lower-limb spasticity in children with cerebral palsy. Arq. Neuropsiquiatr. 2009, 67, 62–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ade-Hall, R.A.; Moore, A.P. Botulinum toxin type A in the treatment of lower limb spasticity in cerebral palsy. Cochrane Database Syst. Rev. 2000, 2, CD001408. [Google Scholar] [CrossRef]
- Westhoff, B.; Seller, K.; Wild, A.; Jaeger, M.; Krauspe, R. Ultrasound-guided botulinum toxin injection technique for the iliopsoas muscle. Dev. Med. Child Neurol. 2003, 45, 829–832. [Google Scholar] [CrossRef]
- Childers, M.K.; Brashear, A.; Jozefczyk, P.; Reding, M.; Alexander, D.; Good, D.; Walcott, J.M.; Jenkins, S.W.; Turkel, C.; Molloy, P.T. Dose-dependent response to intramuscular botulinum toxin type A for upper-limb spasticity in patients after a stroke. Arch. Phys. Med. Rehabil. 2004, 85, 1063–1069. [Google Scholar] [CrossRef]
- Childers, M.K. Targeting the neuromuscular junction in skeletal muscles. Am. J. Phys. Med. Rehabil. 2004, 83, S38–S44. [Google Scholar] [CrossRef]
- Ramirez-Castaneda, J.; Jankovic, J.; Comella, C.; Dashtipour, K.; Fernandez, H.H.; Mari, Z. Diffusion, spread, and migration of botulinum toxin. Mov. Disord. 2013, 28, 1775–1783. [Google Scholar] [CrossRef]
- Gracies, J.M.; Lugassy, M.; Weisz, D.J.; Vecchio, M.; Flanagan, S.; Simpson, D.M. Botulinum toxin dilution and endplate targeting in spasticity: A double-blind controlled study. Arch. Phys. Med. Rehabil. 2009, 90, 9–16.e2. [Google Scholar] [CrossRef]
- Van Campenhout, A.; Verhaegen, A.; Pans, S.; Molenaers, G. Botulinum toxin type A injections in the psoas muscle of children with cerebral palsy: Muscle atrophy after motor end plate-targeted injections. Res. Dev. Disabil. 2013, 34, 1052–1058. [Google Scholar] [CrossRef]
- Kinnett, D. Botulinum toxin A injections in children: Technique and dosing issues. Am. J. Phys. Med. Rehabil. 2004, 83, S59–S64. [Google Scholar] [CrossRef] [PubMed]
- Hsu, T.S.; Dover, J.S.; Arndt, K.A. Effect of volume and concentration on the diffusion of botulinum exotoxin A. Arch. Dermatol. 2004, 140, 1351–1354. [Google Scholar] [CrossRef] [PubMed]
- Lepage, D.; Parratte, B.; Tatu, L.; Vuiller, F.; Monnier, G. Extra- and intramuscular nerve supply of the muscles of the anterior antebrachial compartment: Applications for selective neurotomy and for botulinum toxin injection. Surg. Radiol. Anat. 2005, 27, 420–430. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, M.; Leodori, G.; Fernandes, R.M.; Bhidayasiri, R.; Marti, M.J.; Colosimo, C.; Ferreira, J.J. Neutralizing Antibody and Botulinum Toxin Therapy: A Systematic Review and Meta-analysis. Neurotox. Res. 2016, 29, 105–117. [Google Scholar] [CrossRef]
- Rha, D.W.; Yi, K.H.; Park, E.S.; Park, C.; Kim, H.J. Intramuscular nerve distribution of the hamstring muscles: Application to treating spasticity. Clin. Anat. 2016, 29, 746–751. [Google Scholar] [CrossRef]
- Yi, K.H.; Choi, Y.J.; Cong, L.; Lee, K.L.; Hu, K.S.; Kim, H.J. Effective botulinum toxin injection guide for treatment of cervical dystonia. Clin. Anat. 2020, 33, 192–198. [Google Scholar] [CrossRef]
- Yi, K.H.; Cong, L.; Bae, J.H.; Park, E.S.; Rha, D.W.; Kim, H.J. Neuromuscular structure of the tibialis anterior muscle for functional electrical stimulation. Surg. Radiol. Anat. 2017, 39, 77–83. [Google Scholar] [CrossRef]
- Yi, K.H.; Rha, D.W.; Lee, S.C.; Cong, L.; Lee, H.J.; Lee, Y.W.; Kim, H.J.; Hu, K.S. Intramuscular nerve distribution pattern of ankle invertor muscles in human cadaver using sihler stain. Muscle Nerve 2016, 53, 742–747. [Google Scholar] [CrossRef]
- Yi, K.H.; Lee, H.J.; Choi, Y.J.; Lee, J.H.; Hu, K.S.; Kim, H.J. Intramuscular Neural Distribution of Rhomboid Muscles: Evaluation for Botulinum Toxin Injection Using Modified Sihler’s Method. Toxins 2020, 12, 289. [Google Scholar] [CrossRef]
- Yi, K.H.; Lee, H.J.; Lee, J.H.; Seo, K.K.; Kim, H.J. Application of Botulinum Neurotoxin Injections in TRAM Flap for Breast Reconstruction: Intramuscular Neural Arborization of the Rectus Abdominis Muscle. Toxins 2021, 13, 269. [Google Scholar] [CrossRef]
- Yi, K.H.; Lee, H.J.; Seo, K.K.; Kim, H.J. Botulinum neurotoxin injection guidelines regarding flap surgeries in breast reconstruction. J. Plast. Reconstr. Aesthet. Surg. 2022, 75, 503–505. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.H.; Lee, J.H.; Lee, D.K.; Hu, H.W.; Seo, K.K.; Kim, H.J. Anatomical locations of the motor endplates of sartorius muscle for botulinum toxin injections in treatment of muscle spasticity. Surg. Radiol. Anat. 2021, 43, 2025–2030. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.H.; Lee, K.L.; Lee, J.H.; Hu, H.W.; Lee, K.; Seo, K.K.; Kim, H.J. Guidelines for botulinum neurotoxin injections in piriformis syndrome. Clin. Anat. 2021, 34, 1028–1034. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.H.; Lee, H.J.; Lee, J.H.; Lee, K.L.; Kim, H.J. Effective botulinum neurotoxin injection in treating iliopsoas spasticity. Clin. Anat. 2021, 34, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.H.; Lee, H.J.; Choi, Y.J.; Lee, K.; Lee, J.H.; Kim, H.J. Anatomical guide for botulinum neurotoxin injection: Application to cosmetic shoulder contouring, pain syndromes, and cervical dystonia. Clin. Anat. 2021, 34, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Van Campenhout, A.; Hubens, G.; Fagard, K.; Molenaers, G. Localization of motor nerve branches of the human psoas muscle. Muscle Nerve 2010, 42, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Oddy, M.J.; Brown, C.; Mistry, R.; Eastwood, D.M. Botulinum toxin injection site localization for the tibialis posterior muscle. J. Pediatr. Orthop. B 2006, 15, 414–417. [Google Scholar] [CrossRef] [PubMed]
- Hao, L.; Clarke, C.P. Persistent twitching of the latissimus dorsi muscle after a posterolateral thoracotomy. ANZ J. Surg. 2002, 72, 680–681. [Google Scholar] [CrossRef]
- Yu, D.Z.; Liu, A.T.; Dang, R.S.; Zhang, C.S.; Zhang, J.L.; Chen, G.; Yi, J.; Han, T.; Jiang, H. Intramuscular innervations of muscle flaps that are commonly used in clinical settings. Surg. Radiol. Anat. 2010, 32, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.W.; Youssef, A.; Cha, S.; Reece, G.P. Autologous breast reconstruction with the extended latissimus dorsi flap. Plast. Reconstr. Surg. 2002, 110, 751–759; discussion 760–761. [Google Scholar] [CrossRef]
- Munhoz, A.M.; Montag, E.; Fels, K.W.; Arruda, E.G.; Sturtz, G.P.; Aldrighi, C.; Gemperli, R.; Ferreira, M.C. Outcome analysis of breast-conservation surgery and immediate latissimus dorsi flap reconstruction in patients with T1 to T2 breast cancer. Plast. Reconstr. Surg. 2005, 116, 741–752. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Chang, T.W. Extended latissimus dorsi musculocutaneous flap for breast reconstruction: Experience in Oriental patients. Br. J. Plast. Surg. 1999, 52, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, M.S.; Wren, D.R.; Filshie, J. Neuromyotonia in a muscle flap producing a convulsing breast: Successful treatment with botulinum toxin. Mov. Disord. 1998, 13, 188–190. [Google Scholar] [CrossRef] [PubMed]
- Gur, E.; Hanna, W.; Andrighetti, L.; Semple, J.L. Light and electron microscopic evaluation of the pectoralis major muscle following tissue expansion for breast reconstruction. Plast. Reconstr. Surg. 1998, 102, 1046–1051. [Google Scholar] [CrossRef]
- Schweizer, D.F.; Schweizer, R.; Zhang, S.; Kamat, P.; Contaldo, C.; Rieben, R.; Eberli, D.; Giovanoli, P.; Erni, D.; Plock, J.A. Botulinum toxin A and B raise blood flow and increase survival of critically ischemic skin flaps. J. Surg. Res. 2013, 184, 1205–1213. [Google Scholar] [CrossRef]
- Park, T.H.; Lee, S.H.; Park, Y.J.; Lee, Y.S.; Rah, D.K.; Kim, S.Y. Presurgical Botulinum Toxin A Treatment Increases Angiogenesis by Hypoxia-Inducible Factor-1alpha/Vascular Endothelial Growth Factor and Subsequent Superiorly Based Transverse Rectus Abdominis Myocutaneous Flap Survival in a Rat Model. Ann. Plast. Surg. 2016, 76, 723–728. [Google Scholar] [CrossRef]
- Hara, T.; Momosaki, R.; Niimi, M.; Yamada, N.; Hara, H.; Abo, M. Botulinum Toxin Therapy Combined with Rehabilitation for Stroke: A Systematic Review of Effect on Motor Function. Toxins 2019, 11, 707. [Google Scholar] [CrossRef] [Green Version]
- Melling, J.; Hambleton, P.; Shone, C.C. Clostridium botulinum toxins: Nature and preparation for clinical use. Eye 1988, 2, 16–23. [Google Scholar] [CrossRef] [Green Version]
- Shaari, C.M.; George, E.; Wu, B.L.; Biller, H.F.; Sanders, I. Quantifying the spread of botulinum toxin through muscle fascia. Laryngoscope 1991, 101, 960–964. [Google Scholar] [CrossRef]
- Liem, R.S.; Douwe van Willigen, J. In toto staining and preservation of peripheral nervous tissue. Stain Technol. 1988, 63, 113–120. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yi, K.-H.; Lee, H.-J.; Seo, K.K.; Kim, H.-J. Intramuscular Neural Arborization of the Latissimus Dorsi Muscle: Application of Botulinum Neurotoxin Injection in Flap Reconstruction. Toxins 2022, 14, 107. https://doi.org/10.3390/toxins14020107
Yi K-H, Lee H-J, Seo KK, Kim H-J. Intramuscular Neural Arborization of the Latissimus Dorsi Muscle: Application of Botulinum Neurotoxin Injection in Flap Reconstruction. Toxins. 2022; 14(2):107. https://doi.org/10.3390/toxins14020107
Chicago/Turabian StyleYi, Kyu-Ho, Hyung-Jin Lee, Kyle K. Seo, and Hee-Jin Kim. 2022. "Intramuscular Neural Arborization of the Latissimus Dorsi Muscle: Application of Botulinum Neurotoxin Injection in Flap Reconstruction" Toxins 14, no. 2: 107. https://doi.org/10.3390/toxins14020107
APA StyleYi, K. -H., Lee, H. -J., Seo, K. K., & Kim, H. -J. (2022). Intramuscular Neural Arborization of the Latissimus Dorsi Muscle: Application of Botulinum Neurotoxin Injection in Flap Reconstruction. Toxins, 14(2), 107. https://doi.org/10.3390/toxins14020107