Assessing the Impacts of Preanalytical Field Sampling Challenges on the Reliability of Serum Aflatoxin B1-Lysine Measurements by Use of LC-MS/MS

Abstract
:1. Introduction
2. Results
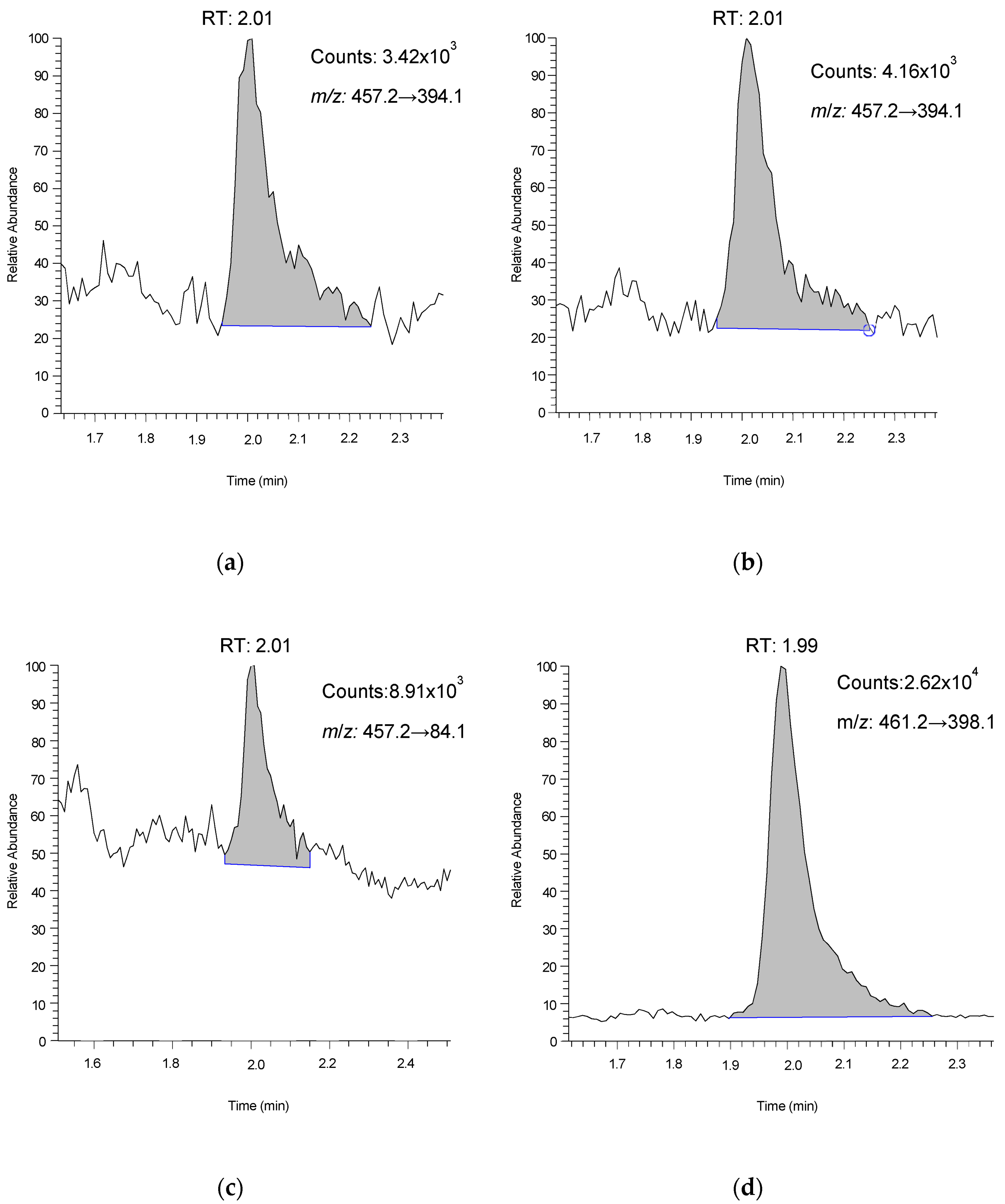
2.1. Method Development
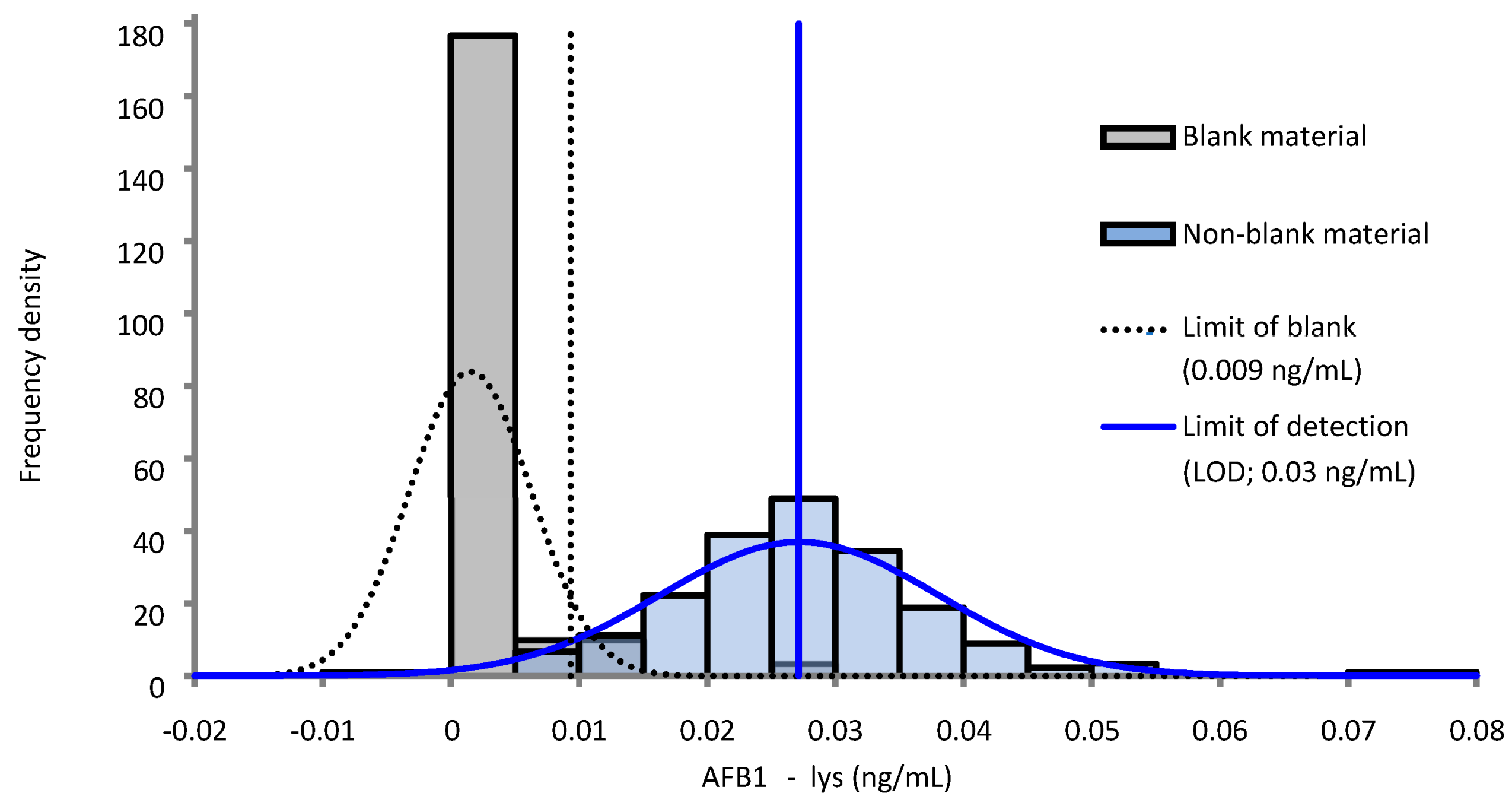
2.2. Imprecision, Accuracy, and Sensitivity
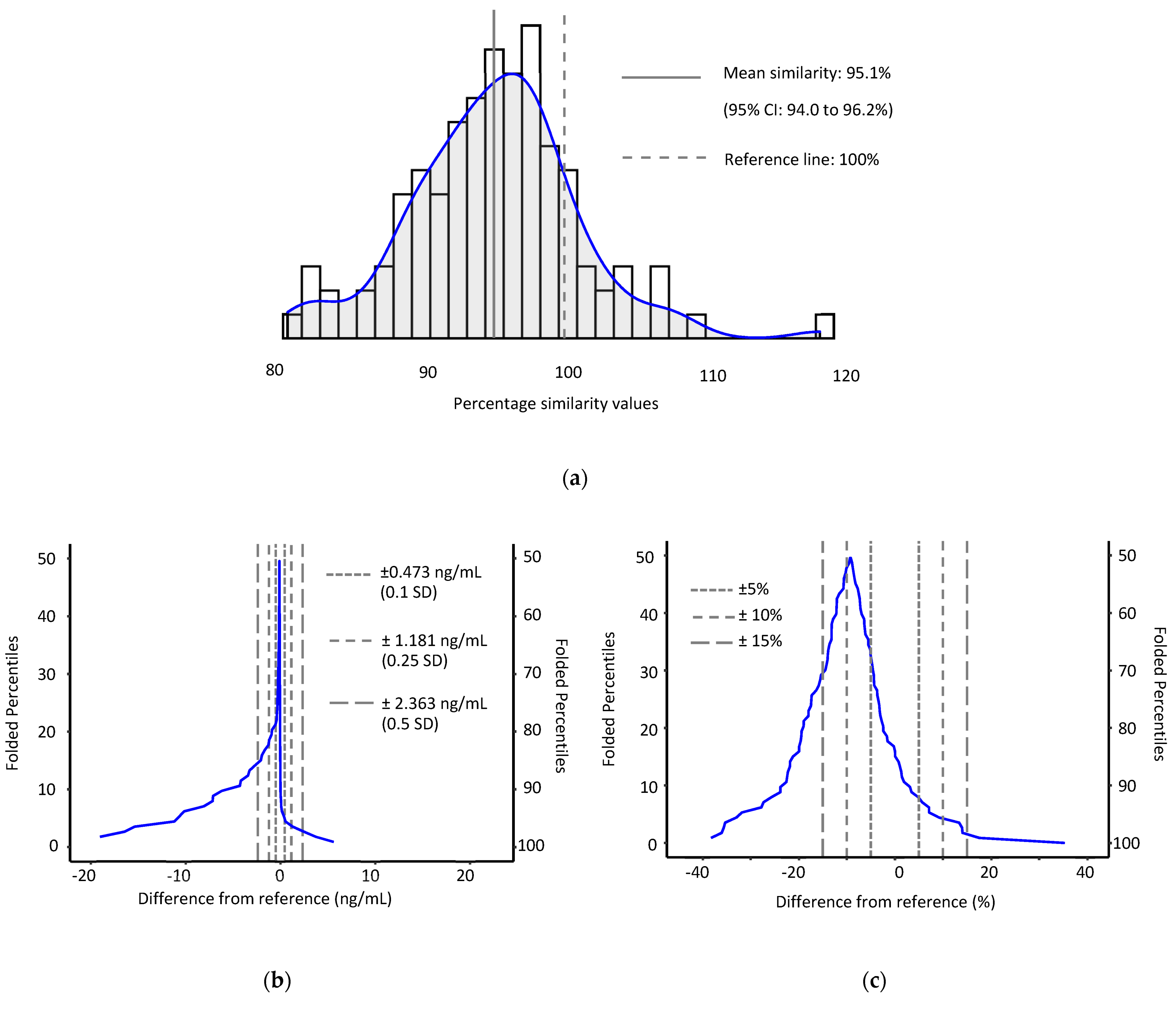
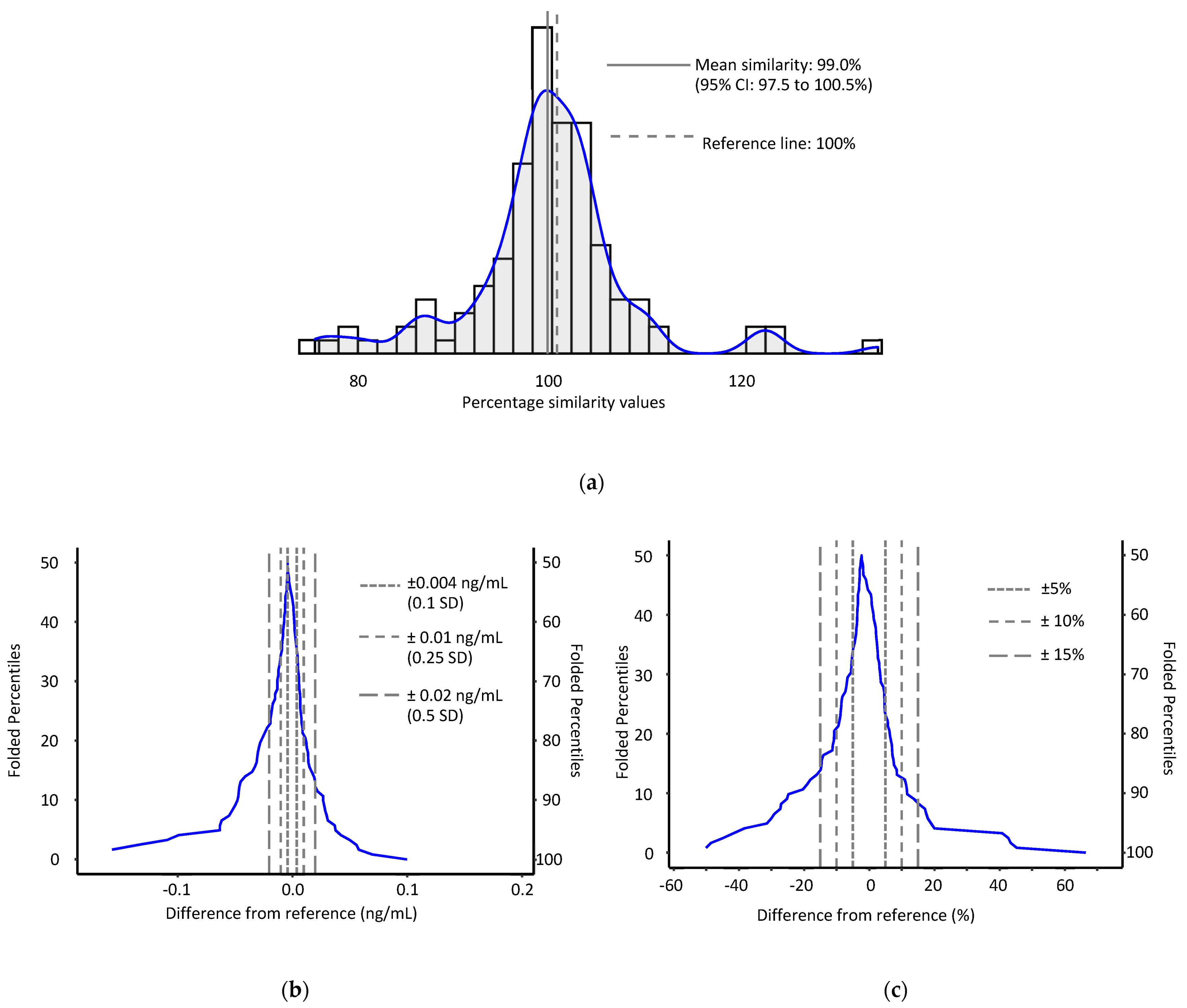
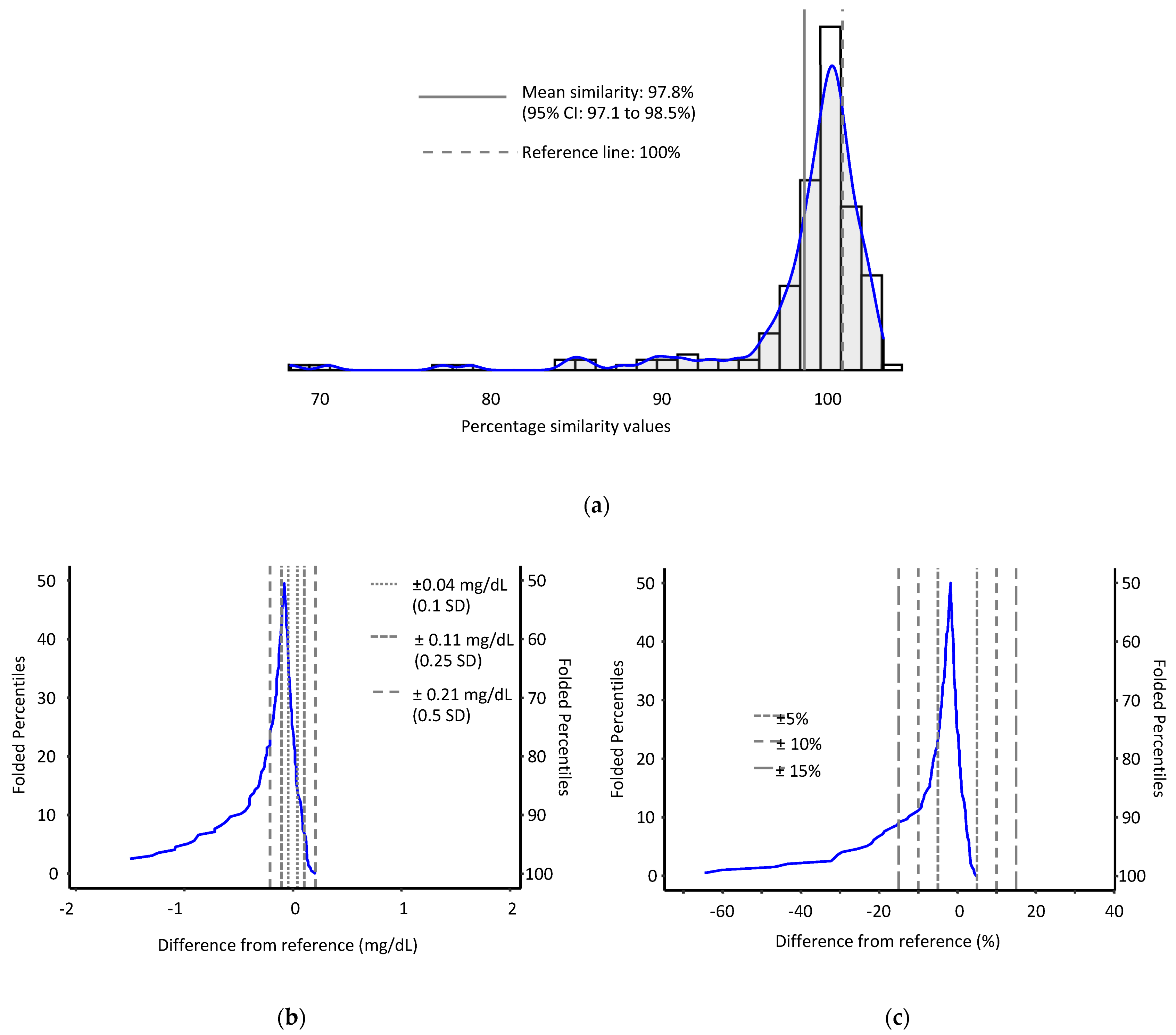
2.3. Method Comparison
2.4. Effect of Prolonged Exposure to Elevated Temperature on AFB1-lys
2.5. Effect of Hemolysis on AFB1-lys
2.6. Effect of Substituting Heparinized Plasma for Serum
3. Discussion
3.1. LC-MS/MS Method Performance
3.2. Preanalytical Factors
4. Materials and Methods
4.1. Preanalytical Factors
4.2. Sample Preparation
4.3. LC-MS/MS Analysis
4.4. Statistical and Other Methods
4.5. Method Validation and Analytical Performance
4.6. Preanalytical Factors Experiments
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Wild, C.P.; Gong, Y.Y. Mycotoxins and human disease: A largely ignored global health issue. Carcinogenesis 2010, 31, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, J.; Trabjerg, E.; Grevys, A.; Azevedo, C.; Brennan, S.O.; Stensland, M.; Wilson, J.; Sand, K.M.K.; Bern, M.; Dalhus, B. An intact C-terminal end of albumin is required for its long half-life in humans. Commun. Biol. 2020, 3, 181. [Google Scholar] [CrossRef] [PubMed]
- Wild, C.P.; Jiang, Y.-Z.; Sabbioni, G.; Chapot, B.; Montesano, R. Evaluation of methods for quantitation of aflatoxin-albumin adducts and their application to human exposure assessment. Cancer Res. 1990, 50, 245–251. [Google Scholar] [PubMed]
- Wild, C.P.; Hudson, G.J.; Sabbioni, G.; Chapot, B.; Hall, A.J.; Wogan, G.N.; Whittle, H.; Montesano, R.; Groopman, J.D. Dietary intake of aflatoxins and the level of albumin-bound aflatoxin in peripheral blood in The Gambia, West Africa. Cancer Epidemiol. Biomark. Prev. 1992, 1, 229–234. [Google Scholar]
- Xue, K.S.; Cai, W.; Tang, L.; Wang, J.-S. Aflatoxin B1-lysine adduct in dried blood spot samples of animals and humans. Food Chem. Toxicol. 2016, 98, 210–219. [Google Scholar] [CrossRef]
- McCoy, L.F.; Scholl, P.F.; Schleicher, R.L.; Groopman, J.D.; Powers, C.D.; Pfeiffer, C.M. Analysis of aflatoxin B1-lysine adduct in serum using isotope-dilution liquid chromatography/tandem mass spectrometry. Rapid Commun. Mass Spectrom. 2005, 19, 2203–2210. [Google Scholar] [CrossRef]
- McCoy, L.F.; Scholl, P.F.; Sutcliffe, A.E.; Kieszak, S.M.; Powers, C.D.; Rogers, H.S.; Gong, Y.Y.; Groopman, J.D.; Wild, C.P.; Schleicher, R.L. Human aflatoxin albumin adducts quantitatively compared by ELISA, HPLC with fluorescence detection, and HPLC with isotope dilution mass spectrometry. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1653–1657. [Google Scholar] [CrossRef]
- Simundic, A.M.; Lippi, G. Preanalytical phase–a continuous challenge for laboratory professionals. Biochem. Med. 2012, 22, 145–149. [Google Scholar] [CrossRef]
- Yard, E.E.; Daniel, J.H.; Lewis, L.S.; Rybak, M.E.; Paliakov, E.M.; Kim, A.A.; Montgomery, J.M.; Bunnell, R.; Abudo, M.U.; Akhwale, W.; et al. Human aflatoxin exposure in Kenya, 2007: A cross-sectional study. Food Addit. Contam. Part A 2013, 30, 1322–1331. [Google Scholar] [CrossRef]
- Zitomer, N.C.; Awuor, A.O.; Widdowson, M.A.; Daniel, J.H.; Sternberg, M.R.; Rybak, M.E.; Mbidde, E.K. Human aflatoxin exposure in Uganda: Estimates from a subset of the 2011 Uganda AIDS indicator survey (UAIS). Food Addit. Contam. Part A 2021, 38, 136–147. [Google Scholar] [CrossRef]
- Pierson-Perry, J.F.; Vaks, J.E.; Vore, T.E.K.; Durham, A.P.; Fischer, C.; Gutenbrunner, C.; Hillyard, D.; Kondratovich, M.V.; Ladwig, P.; Middleberg, R.A. Evaluation of Detection Capability for Clinical Laboratory Measurement Procedures; Approved Guideline (EP17-A2); Clinical Laboratory Standards Institute: Wayne, PA, USA, 2012. [Google Scholar]
- Azziz-Baumgartner, E.; Lindblade, K.; Gieseker, K.; Rogers, H.S.; Kieszak, S.; Njapau, H.; Schleicher, R.; McCoy, L.F.; Misore, A.; DeCock, K.; et al. Case-control study of an acute aflatoxicosis outbreak, Kenya, 2004. Environ. Health Perspect. 2005, 113, 1779–1783. [Google Scholar] [CrossRef]
- Liu, C.; Van der Fels-Klerx, H.J. Quantitative Modeling of Climate Change Impacts on Mycotoxins in Cereals: A Review. Toxins 2021, 13, 276. [Google Scholar] [CrossRef]
- Cotty, P.J.; Jamie-Garcia, R. Influences of climate on aflatoxin producing fungi and aflatoxin contamination. Int. J. Food Microbiol. 2007, 119, 109–115. [Google Scholar] [CrossRef]
- Belinskaia, D.A.; Voronina, P.A.; Batalova, A.A.; Goncharov, N.V. Serum Albumin. Encyclopedia 2021, 1, 65–75. [Google Scholar] [CrossRef]
- Peters, T., Jr. All about Albumin: Biochemistry, Genetics, and Medical Applications; Academic Press: Cambridge, MA, USA, 1995; pp. 14–17. [Google Scholar]
- Berg, B.; Estborn, B.; Tryding, N. Stability of serum and blood constituents during mail transport. Scand. J. Clin. Lab. Investig. 1981, 41, 425–430. [Google Scholar] [CrossRef]
- Pawlik-Sobecka, L.; Sołkiewicz, K.; Kokot, I.; Kiraga, A.; Płaczkowska, S.; Schlichtinger, A.M.; Kratz, E.M. The Influence of Serum Sample Storage Conditions on Selected Laboratory Parameters Related to Oxidative Stress: A Preliminary Study. Diagnostics 2020, 10, 51. [Google Scholar] [CrossRef]
- Renaud, J.B.; Walsh, J.P.; Sumarah, M.W. Simplified Synthesis and Stability Assessment of Aflatoxin B1-Lysine and Aflatoxin G1-Lysine. Toxins 2022, 14, 56. [Google Scholar] [CrossRef]
- Scholl, P.F.; Groopman, J.D. Long-term Stability of Human Aflatoxin B1 Albumin Adducts Assessed by Isotope Dilution Mass Spectrometry and High-Performance Liquid Chromatography–Fluorescence. Cancer Epidemiol. Biomark. Prev. 2008, 17, 1436–1439. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M.; Di Somma, S.; Cervellin, G. Hemolyzed specimens: A major challenge for emergency departments and clinical laboratories. Crit. Rev. Clin. Lab. Sci. 2011, 48, 143–153. [Google Scholar] [CrossRef]
- Yin, P.; Peter, A.; Franken, H.; Zhao, X.; Neukamm, S.S.; Rosenbaum, L.; Lucio, M.; Zell, A.; Häring, H.U.; Xu, G.; et al. Preanalytical Aspects and Sample Quality Assessment in Metabolomics Studies of Human Blood. Clin. Chem. 2013, 59, 833–845. [Google Scholar] [CrossRef]
- Salvagno, G.L.; Danese, E.; Lippi, G. Preanalytical variables for liquid chromatography-mass spectrometry (LC-MS) analysis of human blood specimens. Clin. Biochem. 2017, 50, 582–586. [Google Scholar] [CrossRef] [PubMed]
- Giuseppe, L.; Salvagno, G.L.; Montagnana, M.; Brocco, G.; Guidi, G.C. Influence of hemolysis on routine clinical chemistry testing. Clin. Chem. Lab. Med. 2006, 44, 311–316. [Google Scholar] [CrossRef]
- Smith, J.W.; Ng, D.K.; Alvarez, C.S.; Egner, P.A.; Burke, S.M.; Chen, J.G.; Kensler, T.W.; Koshiol, J.; Rivera-Andrade, A.; Kroker-Lobos, M.F.; et al. Assessing the Validity of Normalizing Aflatoxin B1-Lysine Albumin Adduct Biomarker Measurements to Total Serum Albumin Concentration across Multiple Human Population Studies. Toxins 2022, 14, 162. [Google Scholar] [CrossRef] [PubMed]
- Bonvicini, P.; Ceriotti, G.; Plebani, M.; Volpe, G. Heparin interferes with albumin determination by dye-binding methods. Clin. Chem. 1979, 25, 1459–1460. [Google Scholar] [CrossRef] [PubMed]
- Meng, Q.H.; Krahn, J. Lithium heparinised blood-collection tubes give falsely low albumin results with an automated bromcresol green method in haemodialysis patients. Clin. Chem. Lab. Med. 2008, 46, 396–400. [Google Scholar] [CrossRef] [PubMed]
- Doumas, B.T.; Watson, W.A.; Biggs, H.G. Albumin standards and the measurement of serum albumin with bromocresol green. Clin. Chim. Acta 1971, 31, 87–96. [Google Scholar] [CrossRef]
- Caudill, S.P.; Schleicher, R.L.; Pirkle, J.L. Multi-rule quality control for the age-related eye disease study. Stat. Med. 2008, 27, 4094–4106. [Google Scholar] [CrossRef] [PubMed]
- Scott, L.E.; Galpin, J.S.; Glencross, D.K. Multiple method comparison: Statistical model using percentage similarity. Cytom. B Clin. Cytom. 2003, 54, 46–53. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| QC Pool | Mean AFB1-lys, ng/mL | Imprecision, % CV * | ||
|---|---|---|---|---|
| Within-Run | Between-Run | Total | ||
| P1 | 0.103 | 8.1 | 11.6 | 14.2 |
| P2 | 0.178 | 3.5 | 2.9 | 4.6 |
| P3 | 0.524 | 2.0 | 1.9 | 2.8 |
| P4 | 0.864 | 2.1 | 2.4 | 3.1 |
| Variable | QC Pool | F-Test P-Value for Overall Effect | Estimated Average Difference in Serum AFB1-lys Concentration (95% CI), ng/mL |
|---|---|---|---|
| Temperature * | LOD | 0.02311 | 0.009 (0.0017–0.0163) |
| P2 | <0.0001 | 0.0137 (0.0086–0.0187) | |
| P3 | <0.0001 | 0.0334 (0.0205–0.0463) | |
| P4 | 0.0605 | 0.0223 (−0.001–0.0457) | |
| F-test P-value for linear trend | |||
| Time * | LOD | 0.8387 | 0.5179 |
| P2 | 0.3829 | 0.0908 | |
| P3 | 0.1452 | 0.6149 | |
| P4 | 0.3309 | 0.6047 |
| Variable | Outcome, Units | QC Pool | F-Test P-Value for Overall Effect |
|---|---|---|---|
| Hemoglobin * | IS area, counts | P3 | <0.0001 |
| P4 | <0.0001 | ||
| AFB1-lys, ng/mL | P3 | 0.5514 | |
| P4 | 0.9202 |
| QC Pool | Hemoglobin, mg/mL | Mean Change in Internal Standard Peak Area from Control, % (95% CI) | P-Value | Bonferroni-Adjusted P-Value * |
|---|---|---|---|---|
| P3 | 0.25 | −15.1 (−20.1 to −10.2) | <0.0001 | <0.0001 |
| 0.5 | −18.4 (−23.3 to −13.4) | <0.0001 | <0.0001 | |
| 1.0 | −16.9 (−21.9 to −12) | <0.0001 | <0.0001 | |
| 2.0 | −22.1 (−27.1 to −17.1) | <0.0001 | <0.0001 | |
| 3.0 | −22.9 (−27.8 to −17.9) | <0.0001 | <0.0001 | |
| P4 | 0.25 | −18.9 (−25.8 to −12) | <0.0001 | 0.0003 |
| 0.5 | −10.5 (−17.3 to −3.6) | 0.0063 | 0.0313 | |
| 1.0 | −25.0 (−31.9 to −18.1) | <0.0001 | <0.0001 | |
| 2.0 | −16.2 (−23.1 to −9.3) | 0.0003 | 0.0012 | |
| 3.0 | −24.9 (−31.8 to −18) | <0.0001 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zitomer, N.C.; Rybak, M.E.; Sternberg, M.R. Assessing the Impacts of Preanalytical Field Sampling Challenges on the Reliability of Serum Aflatoxin B1-Lysine Measurements by Use of LC-MS/MS. Toxins 2022, 14, 612. https://doi.org/10.3390/toxins14090612
Zitomer NC, Rybak ME, Sternberg MR. Assessing the Impacts of Preanalytical Field Sampling Challenges on the Reliability of Serum Aflatoxin B1-Lysine Measurements by Use of LC-MS/MS. Toxins. 2022; 14(9):612. https://doi.org/10.3390/toxins14090612
Chicago/Turabian StyleZitomer, Nicholas C., Michael E. Rybak, and Maya R. Sternberg. 2022. "Assessing the Impacts of Preanalytical Field Sampling Challenges on the Reliability of Serum Aflatoxin B1-Lysine Measurements by Use of LC-MS/MS" Toxins 14, no. 9: 612. https://doi.org/10.3390/toxins14090612
APA StyleZitomer, N. C., Rybak, M. E., & Sternberg, M. R. (2022). Assessing the Impacts of Preanalytical Field Sampling Challenges on the Reliability of Serum Aflatoxin B1-Lysine Measurements by Use of LC-MS/MS. Toxins, 14(9), 612. https://doi.org/10.3390/toxins14090612