Prediction Model for Identifying Computational Phenotypes of Children with Cerebral Palsy Needing Neurotoxin Treatments

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Results
- Neuromuscular scoliosis: p = 0.0013, Odds ratio (OR) = 2.7;
- Equines foot: p < 0.001, OR = 4.1;
- Type of etiology: prenatal > peri/postnatal causes, p = 0.05, OR = 0.53.
- Upper limbs ability, p < 0.001, OR = 3;
- Trunk muscle tone disorders, p = 0.02, OR = 1.9;
- The presence of spasticity, p = 0.01, OR = 2;
- Dystonia, p = 0.004, OR = 5.3;
- Hip dysplasia, p = 0.005, OR = 4.
3. Discussion
3.1. Tolerance and Precautions
3.2. Limitations
4. Materials and Methods
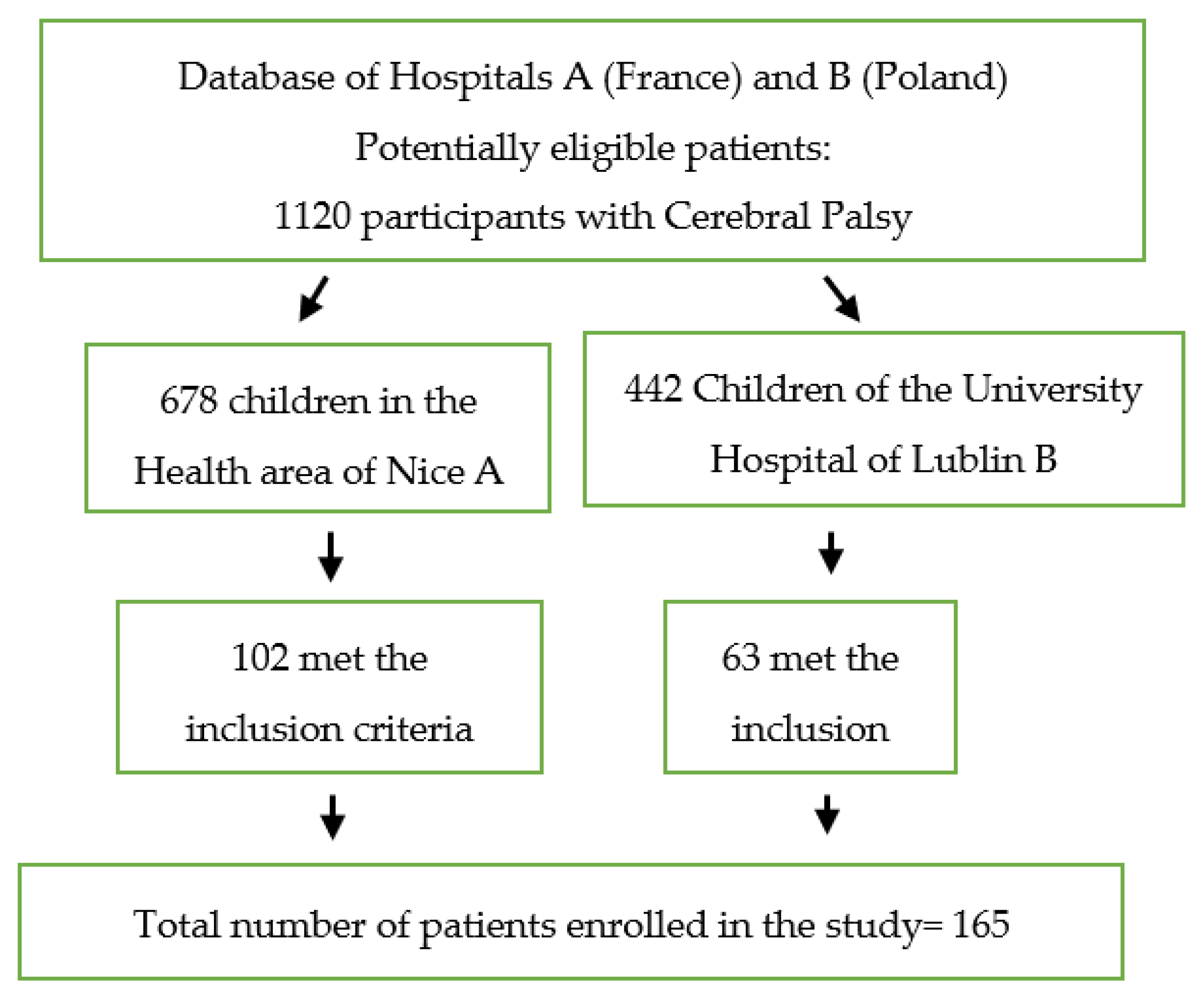
4.1. Study Design
4.2. Botulin Toxin Clinical Use
4.3. The Doses
- For Botox, 300 units per session and 20 Allergan units/kg;
- For Dysport, 1000 units per session and 30 Speywood units/kg (professional agreement).
- For Botox, 500 Allergan units;
- For Dysport, 1500 Speywood units.
- For Botox, 3 to 8 units/kg without exceeding 300 units per session;
- For Dysport, 10 units/kg in unilateral injections and 20 units/kg in bilateral injections without exceeding 1000 units per session.
4.4. Measurements
- antenatal: cerebral malformation, genetic, prematurity, infection, vascular;
- perinatal: anoxic, infectious ischemic;
- postnatal: postnatal anoxic/ischemic injury epilepsy, cranial trauma, infectious.
- o
- Neurotoxins treatments (NT);
- o
- Presence of Neuromuscular scoliosis (NS);
- o
- Trunk muscle tone disorder (TT);
- o
- Spasticity (SP);
- o
- Dystonia (D);
- o
- Epilepsy (E);
- o
- Hip Dysplasia (HD);
- o
- Equines foot (EF);
- o
- Gastrostomy feeding (GA);
- o
- Sex (SE);
- o
- Etiology (ET);
- o
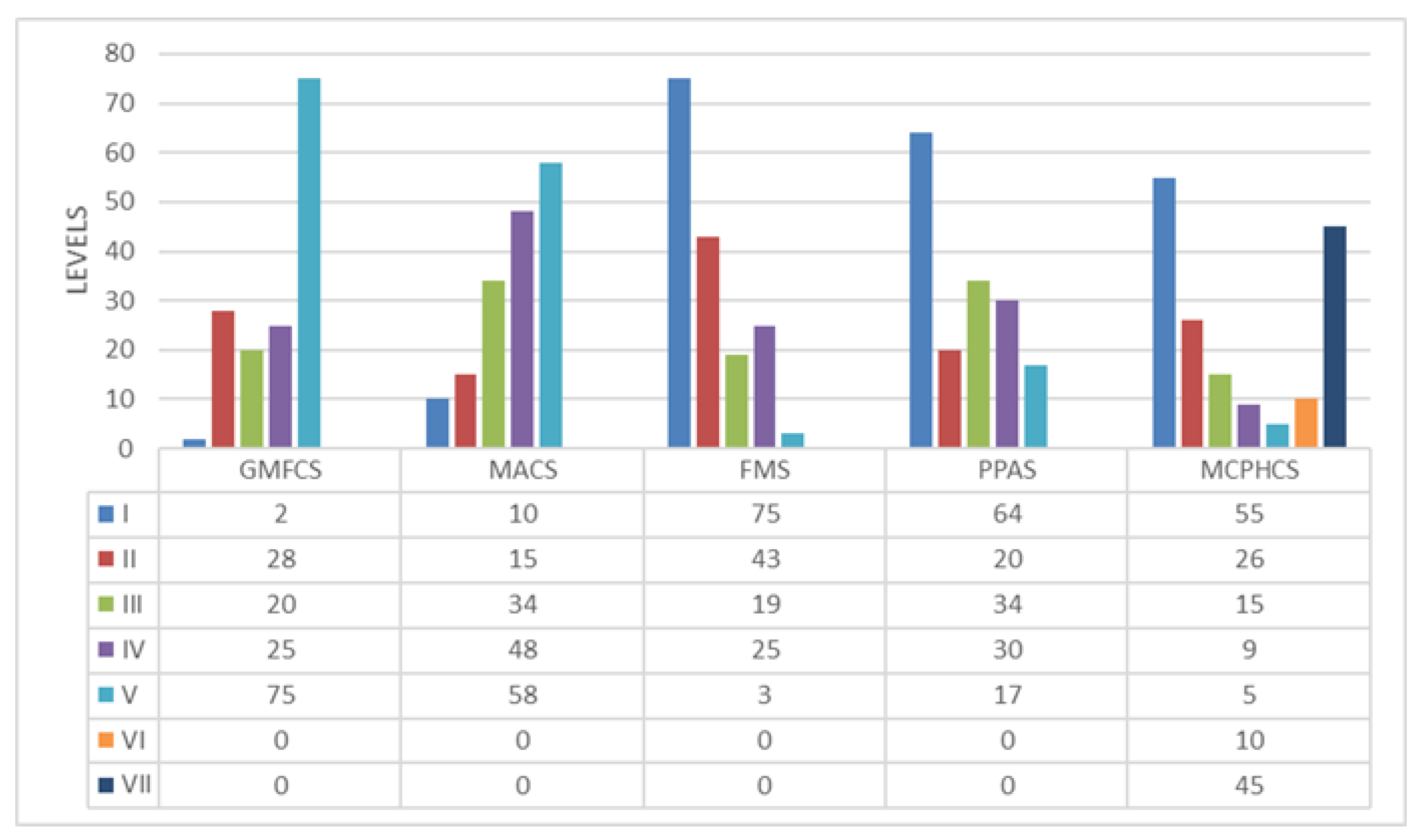
- GMFCS;
- o
- MACS.
4.5. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bertoncelli, C.M.; Solla, F.; Loughenbury, P.R.; Tsirikos, A.I.; Bertoncelli, D.; Rampal, V. Risk factors for developing scoliosis in cerebral palsy: A cross sectional descriptive study. J. Child Neurol. 2017, 32, 657–662. [Google Scholar] [CrossRef]
- Multani, I.; Manji, J.; Hastings-Ison, T.; Khot, A.; Graham, K. Botulinum Toxin in the Management of Children with Cerebral Palsy. Pediatr. Drugs 2019, 21, 261–281. [Google Scholar] [CrossRef] [Green Version]
- Lasko, T.A.; Denny, J.; Levy, M.A. Computational Phenotype Discovery Using Unsupervised Feature Learning over Noisy, Sparse, and Irregular Clinical Data. PLoS ONE 2013, 8, e66341. [Google Scholar] [CrossRef]
- Seymour, T.; Frantsvog, D.A.; Graeber, T. Electronic Health Records (EHR). Am. J. Health Sci. 2012, 3, 201–210. [Google Scholar] [CrossRef] [Green Version]
- Denny, J.C.; Spickard, A.; Johnson, K.B.; Peterson, N.B.; Peterson, J.F.; Miller, R.A. Evaluation of a Method to Identify and Categorize Section Headers in Clinical Documents. J. Am. Med. Inform. Assoc. 2009, 16, 806–815. [Google Scholar] [CrossRef] [Green Version]
- Dean, B.B.; Lam, J.; Natoli, J.L.; Butler, Q.; Aguilar, D.; Nordyke, R.J. Use of electronic medical records for health outcomes research: A literature review. Med. Care Res. Rev. 2009, 66, 611–638. [Google Scholar] [CrossRef]
- Kho, A.N.; Pacheco, J.A.; Peissig, P.L.; Rasmussen, L.; Newton, K.M.; Weston, N.; Crane, P.K.; Pathak, J.; Chute, C.G.; Bielinski, S.J.; et al. Electronic Medical Records for Genetic Research: Results of the eMERGE Consortium. Sci. Transl. Med. 2011, 3, 79re1. [Google Scholar] [CrossRef] [Green Version]
- Kohane, I.S. Using electronic health records to drive discovery in disease genomics. Nat. Rev. Genet. 2011, 12, 417–428. [Google Scholar] [CrossRef]
- Bertoncelli, C.M.; Altamura, P.; Bagui, S.; Vieira, E.R.; Costantini, S.; Monticone, M.; Solla, F.; Bertoncelli, D. Predicting osteoarthritis in adults using statistical data mining and machine learning. Ther. Adv. Musculoskelet. Dis. 2022, 14, 1759720X221104935. [Google Scholar] [CrossRef]
- Bertoncelli, C.M.; Altamura, P.; Bertoncelli, D.; Rampal, V.; Vieira, E.R.; Solla, F. PredictMed: A Machine Learning Model for Identifying Risk Factors of Neuromuscular Hip Dysplasia: A Multicenter Descriptive Study. Neuropediatrics 2020, 52, 343–350. [Google Scholar] [CrossRef]
- Bertoncelli, C.M.; Solla, F. Machine learning for monitoring and evaluating physical activity in cerebral palsy. Dev. Med. Child Neurol. 2020, 62, 1010. [Google Scholar] [CrossRef]
- Hastie, T.; Tibshirani, R.; Friedman, J. Boosting and additive trees. In The Elements of Statistical Learning, 2nd ed.; Springer: New York, NY, USA, 2009. [Google Scholar]
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD statement. BMJ 2015, 350, g7594. [Google Scholar] [CrossRef] [Green Version]
- Pereira, F.; Mitchell, T.; Botvinick, M. Machine learning classifiers and fMRI: A tutorialoverview. Neuroimage 2009, 45, S199–S209. [Google Scholar] [CrossRef] [Green Version]
- Bertoncelli, C.M.; Bertoncelli, D.; Elbaum, L.; Latalski, M.; Altamura, P.; Musoff, C.; Rampal, V.; Solla, F. Validation of a Clinical Prediction Model for the Development of Neuromuscular Scoliosis: A Multinational Study. Pediatr. Neurol. 2018, 79, 14–20. [Google Scholar] [CrossRef]
- Bertoncelli, C.M.; Altamura, P.; Vieira, V.R.; Bertoncelli, D.; Solla, F. Predicting hip dysplasia in teenagers with cerebral palsy in order to optimize prevention and rehabilitation. A longitudinal descriptive study. Dev. Neurorehabilit. 2020, 24, 166–172. [Google Scholar] [CrossRef]
- Bertoncelli, C.M.; Altamura, P.; Vieira, E.; Bertoncelli, D.; Latalski, M.; Berthet, S.; Solla, F. Predictive Model for Gastrostomy Placement in Adolescents with Developmental Disabilities and Cerebral Palsy. Nutr. Clin. Pr. 2020, 35, 149–156. [Google Scholar] [CrossRef] [Green Version]
- Bertoncelli, C.M.; Altamura, P.; Vieira, E.R.; Bertoncelli, D.; Thummler, S.; Solla, F. Identifying factors associated with intellectual disabilities in teenagers with cerebral palsy using a predictive learning model. J. Child. Neurol. 2019, 34, 221–229. [Google Scholar] [CrossRef]
- Bertoncelli, C.M.; Altamura, P.; Vieira, E.R.; Bertoncelli, D.; Solla, F. Using Artificial Intelligence to Identify Factors Associated with Autism Spectrum Disorder in Adolescents with Cerebral Palsy. Neuropediatrics 2019, 50, 178–187. [Google Scholar] [CrossRef]
- Bertoncelli, C.M.; Altamura, P.; Vieira, E.R.; Iyengar, S.S.; Solla, F.; Bertoncelli, D. PredictMed: A logistic regression-based model to predict health conditions in cerebral palsy. Health Inform. J. 2020, 26, 2105–2118. [Google Scholar] [CrossRef] [Green Version]
- Moons, K.G.; Altman, D.G.; Reitsma, J.B.; Collins, G.S. New guideline for the reporting of studies developing, validating, or updating a multivariable clinical prediction model: The TRIPOD statement. Adv. Anat. Pathol. 2015, 22, 303–305. [Google Scholar] [CrossRef]
- Moons, K.G.M.; Kengne, A.P.; Grobbee, D.E.; Royston, P.; Vergouwe, Y.; Altman, D.G.; Woodward, M. Risk prediction models: II. External validation, model updating, and impact assessment. Heart 2012, 98, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Altman, D.G.; Vergouwe, Y.; Royston, P.; Moons, K.G. Prognosis and prognostic research: Validating a prognostic model. BMJ 2009, 338, b605. [Google Scholar] [CrossRef] [PubMed]
- Hareb, F.; Rampal, V.; Bertoncelli, C.M.; Rosello, O.; Solla, F. Botulinum toxin in children with cerebral palsy: An update. Neuropediatrics 2020, 51, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Mirska, A.; Kułak, W.; Okurowska-Zawada, B.; Dmitruk, E. Effectiveness of multiple botulinum toxin sessions and the duration of effects in spasticity therapy in children with cerebral palsy. Childs Nerv Syst. 2019, 35, 141–147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barlaan Lukban, M.; Rosales, R.L.; Dressler, D. Effectiveness of botulinum toxin A for upper and lower limb spasticity in children with cerebral palsy: A summary of evidence. J. Neural Transm. 2009, 116, 319–331. [Google Scholar] [CrossRef]
- Bohn, E.; Goren, K.; Switzer, L.; Falck-Ytter, Y.; Fehlings, D. Pharmacological and neurosurgical interventions for individuals with cerebral palsy and dystonia: A systematic review update and meta-analysis. Dev. Med. Child Neurol. 2021, 63, 1038–1050. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Chung, C.H.; Matthews, D.J.; Chu, H.Y.; Chen, L.C.; Yang, S.S.; Chien, W.C. Long-term effect of botulinum toxin A on the hip and spine in cerebral palsy: A national retrospective cohort study in Taiwan. PLoS ONE 2021, 16, e0255143. [Google Scholar] [CrossRef]
- Young Choi, J.; Kim, S.K.; Park, E.S. The Effect of Botulinum Toxin Injections on Gross Motor Function for Lower Limb Spasticity in Children with Cerebral Palsy. Toxins 2019, 11, 651. [Google Scholar] [CrossRef] [Green Version]
- Aydil, S.; Akpinar, F.M.; Akpinar, E.; Beng, K.; Yagmurlu, M.F. Effectiveness of Multilevel Botulinum Toxin a Injection with Integrated Treatment Program on Spasticity Reduction in Non-Ambulatory Young Children with Cerebral Palsy. Med. Princ. Pract. 2019, 28, 309–314. [Google Scholar] [CrossRef] [Green Version]
- Mall, V.; Heinen, F.; Linder, M.; Philipsen, A.; Korinthenberg, R. Treatment of cerebral palsy with botulinum toxin A: Functional benefit and reduction of disability. Three case reports. Pediatr. Rehabil. 1997, 1, 235–237. [Google Scholar] [CrossRef]
- Corry, I.S.; Cosgrove, A.P.; Duffy, C.M.; McNeill, S.; Taylor, T.C.; Graham, H.K. Botulinum toxin A compared with stretching casts in the treatment of spastic equinus: A randomised prospective trial. J. Pediatr. Orthop. 1998, 18, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Chaléat-Valayer, E.; Parratte, B.; Colin, C.; Denis, A.; Oudin, S.; Bérard, C.; Bernard, J.C.; Bourg, V. A French observational study of botulinum toxin use in the management of children with cerebral palsy: BOTULOSCOPE. Eur. J. Paediatr. Neurol. 2011, 15, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Lee, S.; Jang, J.; Lim, J.; Ryu, J.S. Effect of Botulinum Toxin Injection on the Progression of Hip Dislocation in Patients with Spastic Cerebral Palsy: A Pilot Study. Toxins 2021, 13, 872. [Google Scholar] [CrossRef]
- Biering-Soerensen, B.; Stevenson, V.; Bensmail, D.; Grabljevec, K. European expert consensus on improving patient selection for the management of disabling spasticity with intrathecal baclofen and/or botulinum toxin type A. J. Rehabil. Med. 2022, 54, jrm00241. [Google Scholar] [CrossRef] [PubMed]
- Berg, A.T. Defining intractable epilepsy. Adv. Neurol. 2006, 97, 5–10. [Google Scholar] [PubMed]
- Sinha, S.; Siddiqui, K.A. Definition of intractable epilepsy. Neurosciences 2011, 16, 3–9. [Google Scholar]
- Berg, A.T. Identification of pharmacoresistant epilepsy. Neurol. Clin. 2009, 27, 1003–1013. [Google Scholar] [CrossRef] [Green Version]
- Terjesen, T. The natural history of hip development in cerebral palsy. Dev. Med. Child Neurol. 2012, 54, 951–957. [Google Scholar] [CrossRef]
- Lins, L.A.; Watkins, C.J.; Shore, B.J. Natural History of Spastic Hip Disease. Disease J. Pediatr. Orthop. 2019, 39 (Suppl. 1), S33–S37. [Google Scholar] [CrossRef]
- Solla, F.; Tran, A.; Bertoncelli, D.; Musoff, C.; Bertoncelli, C. Why a p-value is not enough. Clin. Spine Surg. 2018, 31, 385–388. [Google Scholar] [CrossRef]
- Sullivan, K.; Andrew, D.; Minn Minn, S. OpenEpi: A web-based epidemiologic and statistical calculator for public health. Public Health Rep. 2009, 124, 458–471. [Google Scholar] [CrossRef] [PubMed]
- Wen, Z.; Zeng, N.; Wang, N. Sensitivity, specificity, accuracy, associated confidence interval and ROC analysis with practical SAS® implementations. In Proceedings of the NESUG Proceedings: Health Care and Life Sciences, Baltimore, Maryland, 14–17 November 2010; pp. 1–9. [Google Scholar]
- Robert, J.T. An Introduction to Error Analysis: The Study of Uncertainties in Physical Measurements; University Science Books: Sausalito, CA, USA, 1999; pp. 128–129. ISBN 0-935702-75-X. [Google Scholar]
- Mickey, R.M.; Greenland, S. The impact of confounder selection criteria on effect estimation. Am. J. Epidemiol. 1993, 129, 125–137. [Google Scholar] [CrossRef] [PubMed]
- Maldonado, G.; Greenland, S. Simulation study of confounder-selection strategies. Am. J. Epidemiol. 1993, 138, 923–936. [Google Scholar] [CrossRef] [PubMed]
- Vapnik, V. The Nature of Statistical Learning Theory; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2013. [Google Scholar]



{kind=link}
{kind=link}
| Patients Profile | Pediatric Hospital A | Children Hospital B | Multicenter A + B | ||||
|---|---|---|---|---|---|---|---|
| Neurotoxin Treatments | Neurotoxin Treatments | Total (%) | |||||
| Yes (%) | No (%) | Total (%) | Yes (%) | No (%) | Total (%) | ||
| Patients n. (%) | 17 (17) | 85 (83) | 102 (100) | 49 (77) | 14 (23) | 63 (100) | 165 (100) |
| Male | 35 (58) | 25 (42) | 60 (100) | 22 (70) | 9 (30) | 31 (100) | 91 (55) |
| Female | 23 (55) | 19 (45) | 42 (100) | 18 (58) | 14 (42) | 32 (100) | 74 (45) |
| Average age (mean, SD) | 16.4 (1.8) | 16.8 (1.8) | 16.6 (1.8) | 15.8 (1.8) | 16.0 (1.8) | 15.9 (1.8) | 16.2 (1.8) |
| Spasticity, n. (%) | 16 (21) | 59 (79) | 75 (100) | 34 (48) | 20 (52) | 54 (100) | 129 (78) |
| Hemiplegia | 2 (22) | 7 (78) | 9 (100) | 3 (75) | 1 (25) | 4 (100) | 13 (8) |
| Diplegia | 1 (6) | 15 (94) | 16 (100) | 20 (86) | 3 (14) | 23 (100) | 39 (24) |
| Tri/quadriplegia | 13 (26) | 37 (74) | 50 (100) | 11 (41) | 16 (59) | 27 (100) | 77 (68) |
| Dystonia n. (%) | 10 (71) | 4 (29) | 14 (100) | 8 (66) | 4 (36) | 12 (100) | 26 (16) |
| Well-controlled Epilepsy, n. (%) | 10 (20) | 40 (80) | 50 (100) | 23 (79) | 6 (21) | 29 (100) | 79 (48) |
| Intractable Epilepsy | 4 (18) | 18 (82) | 22 (100) | 10 (77) | 3 (23) | 13 (100) | 35 (20) |
| No Epilepsy | 3 (10) | 27 (90) | 30 (100) | 16 (76) | 5 (24) | 21 (100) | 51 (31) |
| Severe Scoliosis (%) | 23 (59) | 16 (41) | 39 (100) | 16 (53) | 14 (47) | 30 (100) | 69 (41) |
| Equines Foot (%) | 31 (75) | 10 (25) | 41 (100) | 21 (75) | 7 (25) | 28 (100) | 69 (41) |
| Hip Dysplasia (%) | 18 (56) | 14 (44) | 32 (100) | 13 (59) | 9 (41) | 22 (100) | 54 (38) |
| Truncal tone disorder (%) | 11 (21) | 42 (79) | 53 (100) | 29 (74) | 10 (26) | 39 (100) | 92 (56) |
| Ante-natal Causes | 10 (16) | 54 (84) | 64 (100) | 21 (84) | 4 (16) | 25 (100) | 89 (54) |
| Perinatal Causes | 4 (14) | 25 (86) | 29 (100) | 24 (72) | 9 (28) | 33 (100) | 62 (37) |
| Postnatal Causes | 3 (34) | 6 (66) | 9 (100) | 4 (80) | 1 (20) | 5 (100) | 14 (9) |
| Independent Variables | Multicenter Pediatric Hospital A + Children Hospital B | Hospitals | |||||||
|---|---|---|---|---|---|---|---|---|---|
| A | B | ||||||||
| Neurotoxin Treatments | Odds Ratio | 95% CIs | Z Statistic | p Value | p Value | p Value | |||
| Yes | No | ||||||||
| Neuromuscular Scoliosis (NS) | Yes | 39 | 30 | 2.86 | 1.50–5.43 | 3.20 | 0.0013 | 0.007 | 0.006 |
| No | 30 | 66 | |||||||
| Equines Foot (EF) | Yes | 45 | 30 | 4.12 | 2.13–7.95 | 4.22 | <0.0001 | <0.0001 | <0.0001 |
| No | 24 | 66 | |||||||
| Etiology (ET) PreNatal > Peri/PostNatal causes | Yes | 31 | 58 | 0.53 | 0.28–0.99 | 1.96 | 0.05 | 0.05 | 0.05 |
| No | 38 | 38 | |||||||
| Logistic Regressions | |||||
|---|---|---|---|---|---|
| Independent Variables | Odds Ratio | Standard Error | Z Ratio | Prob(>|Z|) p Value | |
| Logarithm | Linear | ||||
| Intercept | 1.563 | 4.77 | 0.879 | 1.777 | 0.075 |
| Scoliosis (NS) | 0.146 | 0.863 | 0.476 | −0.308 | 0.757 |
| Truncal Tone Disorder (TT) | 0.626 | 1.870 | 0.277 | 2.258 | 0.023 |
| Etiology | 0.077 | 1.080 | 0.316 | 0.246 | 0.805 |
| Spasticity (SP) | 0.677 | 1.967 | 0.285 | 2.374 | 0.017 |
| Dystonia (D) | 1.670 | 5.312 | 0.583 | 2.864 | 0.004 |
| Epilepsy (E) | 0.227 | 1.254 | 0.349 | 0.649 | 0.515 |
| Gender (SE) | 0.512 | 1.668 | 0.421 | 1.215 | 0.224 |
| GMFCS score | 0.299 | 0.741 | 0.312 | −0.957 | 0.338 |
| MACS score | 1.085 | 2.959 | 0.250 | −4.334 | <0.001 |
| Hip Dysplasia (HD) | 1.392 | 4.022 | 0.500 | 2.7822 | 0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bertoncelli, C.M.; Latalski, M.; Bertoncelli, D.; Bagui, S.; Bagui, S.C.; Gautier, D.; Solla, F. Prediction Model for Identifying Computational Phenotypes of Children with Cerebral Palsy Needing Neurotoxin Treatments. Toxins 2023, 15, 20. https://doi.org/10.3390/toxins15010020
Bertoncelli CM, Latalski M, Bertoncelli D, Bagui S, Bagui SC, Gautier D, Solla F. Prediction Model for Identifying Computational Phenotypes of Children with Cerebral Palsy Needing Neurotoxin Treatments. Toxins. 2023; 15(1):20. https://doi.org/10.3390/toxins15010020
Chicago/Turabian StyleBertoncelli, Carlo M., Michal Latalski, Domenico Bertoncelli, Sikha Bagui, Subhash C. Bagui, Dechelle Gautier, and Federico Solla. 2023. "Prediction Model for Identifying Computational Phenotypes of Children with Cerebral Palsy Needing Neurotoxin Treatments" Toxins 15, no. 1: 20. https://doi.org/10.3390/toxins15010020
APA StyleBertoncelli, C. M., Latalski, M., Bertoncelli, D., Bagui, S., Bagui, S. C., Gautier, D., & Solla, F. (2023). Prediction Model for Identifying Computational Phenotypes of Children with Cerebral Palsy Needing Neurotoxin Treatments. Toxins, 15(1), 20. https://doi.org/10.3390/toxins15010020