
Increased Circulating Levels of Vitamin D Binding Protein in MS Patients

Abstract
:1. Introduction
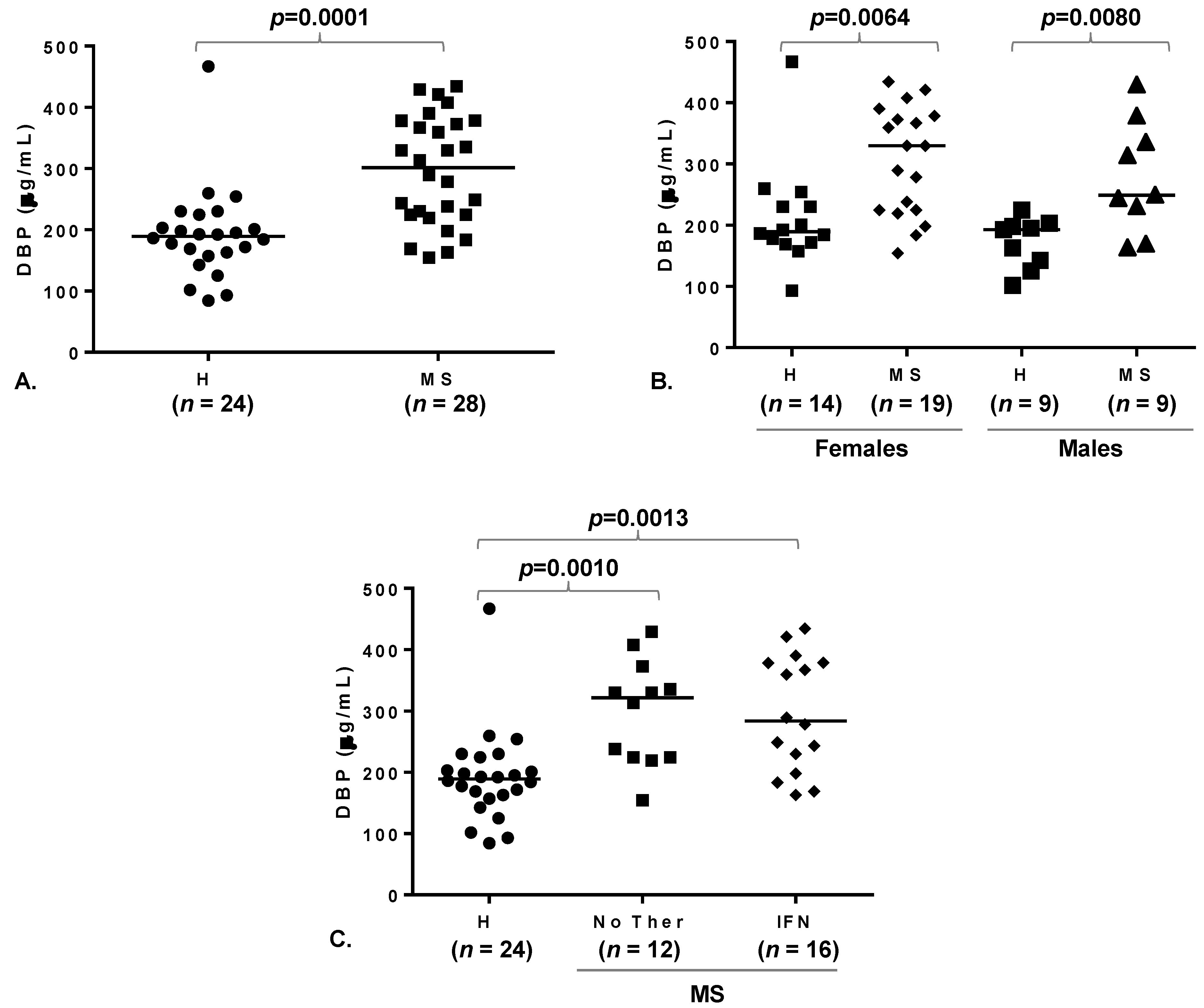
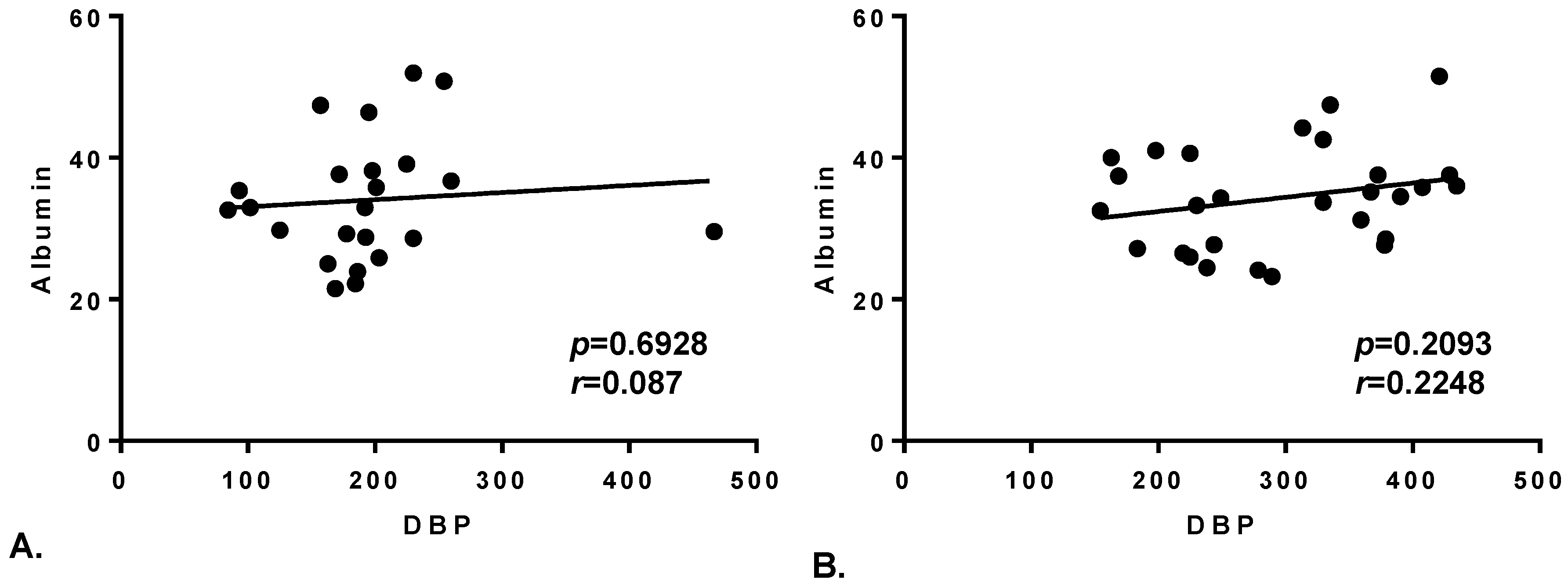
2. Results


3. Discussion
4. Materials and Methods
4.1. Subjects

{kind=link}
{kind=link}
| No of subjects | 28 |
| Age (years; mean ± SD) | 36 ± 8 |
| Females/males (n) | 19:9 |
| EDSS 1 (mean ± SD) | 0.98 ± 1.93 |
| Disease duration (years; mean ± SD) | 5.3 ± 3.8 |
| No of subjects on IFN therapy 2 | 16 |
4.2. Biochemical Analysis
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Ramagopalan, S.V.; Dobson, R.; Meier, U.C.; Giovannoni, G. Multiple sclerosis: Risk factors, prodromes, and potential causal pathways. Lancet Neurol. 2010, 9, 727–739. [Google Scholar] [CrossRef] [PubMed]
- Simon, K.C.; Munger, K.L.; Ascherio, A. Vitamin D and multiple sclerosis: Epidemiology, immunology, and genetics. Curr. Opin. Neurol. 2012, 25, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Smolders, J.; Menheere, P.; Kessels, A.; Damoiseaux, J.; Hupperts, R. Association of vitamin D metabolite levels with relapse rate and disability in multiple sclerosis. Mult. Scler. 2008, 14, 1220–1224. [Google Scholar] [CrossRef] [PubMed]
- Soilu-Hanninen, M.; Laaksonen, M.; Laitinen, I.; Eralinna, J.P.; Lilius, E.M.; Mononen, I. A longitudinal study of serum 25-hydroxyvitamin D and intact parathyroid hormone levels indicate the importance of vitamin D and calcium homeostasis regulation in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Loken-Amsrud, K.I.; Holmoy, T.; Bakke, S.J.; Beiske, A.G.; Bjerve, K.S.; Bjornara, B.T.; Hovdal, H.; Lilleas, F.; Midgard, R.; Pedersen, T.; et al. Vitamin D and disease activity in multiple sclerosis before and during interferon-beta treatment. Neurology 2012, 79, 267–273. [Google Scholar] [CrossRef]
- Runia, T.F.; Hop, W.C.; de Rijke, Y.B.; Buljevac, D.; Hintzen, R.Q. Lower serum vitamin D levels are associated with a higher relapse risk in multiple sclerosis. Neurology 2012, 79, 261–266. [Google Scholar] [CrossRef] [PubMed]
- Stewart, N.; Simpson, S., Jr.; van der Mei, I.; Ponsonby, A.L.; Blizzard, L.; Dwyer, T.; Pittas, F.; Eyles, D.; Ko, P.; Taylor, B.V. Interferon-Beta and serum 25-hydroxyvitamin D interact to modulate relapse risk in MS. Neurology 2012, 79, 254–260. [Google Scholar] [CrossRef] [PubMed]
- Ascherio, A.; Munger, K.L.; White, R.; Kochert, K.; Simon, K.C.; Polman, C.H.; Freedman, M.S.; Hartung, H.P.; Miller, D.H.; Montalban, X.; et al. Vitamin D as an early predictor of multiple sclerosis activity and progression. JAMA Neurol. 2014, 71, 306–314. [Google Scholar] [CrossRef]
- Meier, U.; Gressner, O.; Lammert, F.; Gressner, A.M. Gc-globulin: Roles in response to injury. Clin. Chem. 2006, 52, 1247–1253. [Google Scholar] [CrossRef] [PubMed]
- Nagasawa, H.; Uto, Y.; Sasaki, H.; Okamura, N.; Murakami, A.; Kubo, S.; Kirk, K.L.; Hori, H. Gc PROTEIN (vitamin D-binding protein): Gc genotyping and GcMAF precursor activity. Anticancer Res. 2005, 25, 3689–3695. [Google Scholar] [PubMed]
- Mendel, C.M. The free hormone hypothesis: A physiologically based mathematical model. Endocr. Rev. 1989, 10, 232–274. [Google Scholar] [CrossRef] [PubMed]
- Willnow, T.E.; Nykjaer, A. Pathways for kidney-specific uptake of the steroid hormone 25-hydroxyvitamin D3. Curr. Opin. Lipidol. 2002, 13, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Smolders, J.; Moen, S.M.; Damoiseaux, J.; Huitinga, I.; Holmoy, T. Vitamin D in the healthy and inflamed central nervous system: Access and function. J. Neurol. Sci. 2011, 311, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Jeffery, L.E.; Wood, A.M.; Qureshi, O.S.; Hou, T.Z.; Gardner, D.; Briggs, Z.; Kaur, S.; Raza, K.; Sansom, D.M. Availability of 25-hydroxyvitamin D(3) to APCs controls the balance between regulatory and inflammatory T Cell responses. J. Immunol. 2012, 189, 5155–5164. [Google Scholar] [CrossRef] [PubMed]
- Chun, R.F.; Lauridsen, A.L.; Suon, L.; Zella, L.A.; Pike, J.W.; Modlin, R.L.; Martineau, A.R.; Wilkinson, R.J.; Adams, J.; Hewison, M. Vitamin D-binding protein directs monocyte responses to 25-hydroxy- and 1,25-dihydroxyvitamin D. J. Clin. Endocrinol. Metab. 2010, 95, 3368–3376. [Google Scholar] [CrossRef] [PubMed]
- Kongsbak, M.; von Essen, M.; Levring, T.; Schjerling, P.; Woetmann, A.; Odum, N.; Bonefeld, C.; Geisler, C. Vitamin D-binding protein controls T cell responses to vitamin D. BMC Immunol. 2014, 15, 35. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D.D.; Siiteri, P.K.; Ryzen, E.; Haddad, J.G. Serum protein binding of 1,25-dihydroxyvitamin D: A reevaluation by direct measurement of free metabolite levels. J. Clin. Endocrinol. Metab. 1985, 61, 969–975. [Google Scholar] [CrossRef] [PubMed]
- Chun, R.F.; Peercy, B.E.; Orwoll, E.S.; Nielson, C.M.; Adams, J.S.; Hewison, M. Vitamin D and DBP: The free hormone hypothesis revisited. J. Steroid Biochem. Mol. Biol. 2014, 144 Pt A, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Carter, G.D.; Phinney, K.W. Assessing vitamin D status: Time for a rethink? Clin. Chem. 2014, 60, 809–811. [Google Scholar] [CrossRef] [PubMed]
- Rithidech, K.N.; Honikel, L.; Milazzo, M.; Madigan, D.; Troxell, R.; Krupp, L.B. Protein expression profiles in pediatric multiple sclerosis: Potential biomarkers. Mult. Scler. 2009, 15, 455–464. [Google Scholar] [CrossRef] [PubMed]
- Kulakowska, A.; Ciccarelli, N.J.; Wen, Q.; Mroczko, B.; Drozdowski, W.; Szmitkowski, M.; Janmey, P.A.; Bucki, R. Hypogelsolinemia, a disorder of the extracellular actin scavenger system, in patients with multiple sclerosis. BMC Neurol. 2010, 10, 107. [Google Scholar] [CrossRef] [PubMed]
- Smolders, J.; Peelen, E.; Thewissen, M.; Menheere, P.; Damoiseaux, J.; Hupperts, R. Circulating vitamin D binding protein levels are not associated with relapses or with vitamin D status in multiple sclerosis. Mult. Scler. 2014, 20, 433–437. [Google Scholar] [CrossRef] [PubMed]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the Mcdonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef]
- Powe, C.E.; Evans, M.K.; Wenger, J.; Zonderman, A.B.; Berg, A.H.; Nalls, M.; Tamez, H.; Zhang, D.; Bhan, I.; Karumanchi, S.A.; et al. Vitamin D-binding protein and vitamin D status of black Americans and white Americans. N. Engl. J. Med. 2013, 369, 1991–2000. [Google Scholar] [CrossRef]
- Harvey, N.C.; Holroyd, C.; Ntani, G.; Javaid, K.; Cooper, P.; Moon, R.; Cole, Z.; Tinati, T.; Godfrey, K.; Dennison, E.; et al. Vitamin D supplementation in pregnancy: A systematic review. Health Technol. Assess. 2014, 18, 1–190. [Google Scholar] [CrossRef]
- Munger, K.L.; Ascherio, A. Prevention and treatment of MS: Studying the effects of vitamin D. Mult. Scler. 2011, 17, 1405–1411. [Google Scholar] [CrossRef] [PubMed]
- James, E.; Dobson, R.; Kuhle, J.; Baker, D.; Giovannoni, G.; Ramagopalan, S.V. The effect of vitamin D-related interventions on multiple sclerosis relapses: A meta-analysis. Mult. Scler. 2013, 19, 1571–1579. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Qin, Z.; Zhu, Y.; Li, Y.; Qin, Y.; Jing, Y.; Liu, S. Vitamin D-binding protein in cerebrospinal fluid is associated with multiple sclerosis progression. Mol. Neurobiol. 2013, 47, 946–956. [Google Scholar] [CrossRef] [PubMed]
- Correale, J.; Ysrraelit, M.C.; Gaitan, M.I. Gender differences in 1,25 dihydroxyvitamin D3 immunomodulatory effects in multiple sclerosis patients and healthy subjects. J. Immunol. 2010, 185, 4948–4958. [Google Scholar] [CrossRef] [PubMed]
- Aarskog, D.; Aksnes, L.; Markestad, T.; Rodland, O. Effect of estrogen on vitamin D metabolism in tall girls. J. Clin. Endocrinol. Metab. 1983, 57, 1155–1158. [Google Scholar] [CrossRef] [PubMed]
- Dick, I.M.; Prince, R.L.; Kelly, J.J.; Ho, K.K. Oestrogen effects on calcitriol levels in post-menopausal women: A comparison of oral versus transdermal administration. Clin. Endocrinol. (Oxf.) 1995, 43, 219–224. [Google Scholar] [CrossRef]
- Harris, S.S.; Dawson-Hughes, B. The association of oral contraceptive use with plasma 25-hydroxyvitamin D levels. J. Am. Coll. Nutr. 1998, 17, 282–284. [Google Scholar] [CrossRef] [PubMed]
- Disanto, G.; Ramagopalan, S.V.; Para, A.E.; Handunnetthi, L. The emerging role of vitamin D binding protein in multiple sclerosis. J. Neurol. 2011, 258, 353–358. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rinaldi, A.O.; Sanseverino, I.; Purificato, C.; Cortese, A.; Mechelli, R.; Francisci, S.; Salvetti, M.; Millefiorini, E.; Gessani, S.; Gauzzi, M.C. Increased Circulating Levels of Vitamin D Binding Protein in MS Patients. Toxins 2015, 7, 129-137. https://doi.org/10.3390/toxins7010129
Rinaldi AO, Sanseverino I, Purificato C, Cortese A, Mechelli R, Francisci S, Salvetti M, Millefiorini E, Gessani S, Gauzzi MC. Increased Circulating Levels of Vitamin D Binding Protein in MS Patients. Toxins. 2015; 7(1):129-137. https://doi.org/10.3390/toxins7010129
Chicago/Turabian StyleRinaldi, Arturo Ottavio, Isabella Sanseverino, Cristina Purificato, Antonio Cortese, Rosella Mechelli, Silvia Francisci, Marco Salvetti, Enrico Millefiorini, Sandra Gessani, and Maria Cristina Gauzzi. 2015. "Increased Circulating Levels of Vitamin D Binding Protein in MS Patients" Toxins 7, no. 1: 129-137. https://doi.org/10.3390/toxins7010129
APA StyleRinaldi, A. O., Sanseverino, I., Purificato, C., Cortese, A., Mechelli, R., Francisci, S., Salvetti, M., Millefiorini, E., Gessani, S., & Gauzzi, M. C. (2015). Increased Circulating Levels of Vitamin D Binding Protein in MS Patients. Toxins, 7(1), 129-137. https://doi.org/10.3390/toxins7010129