
Treatments for Latrodectism—A Systematic Review on Their Clinical Effectiveness


Abstract
:1. Introduction
2. Clinical Characteristics of Latrodectism
3. Earlier Treatments for Latrodectism
4. Antivenoms and Their Mechanism of Action
4.1. Black Widow Spider Antivenoms
4.2. Red-Back Spider Antivenom
5. Clinical Studies of Antivenom Effectiveness
5.1. Non-Randomised Clinical Trials
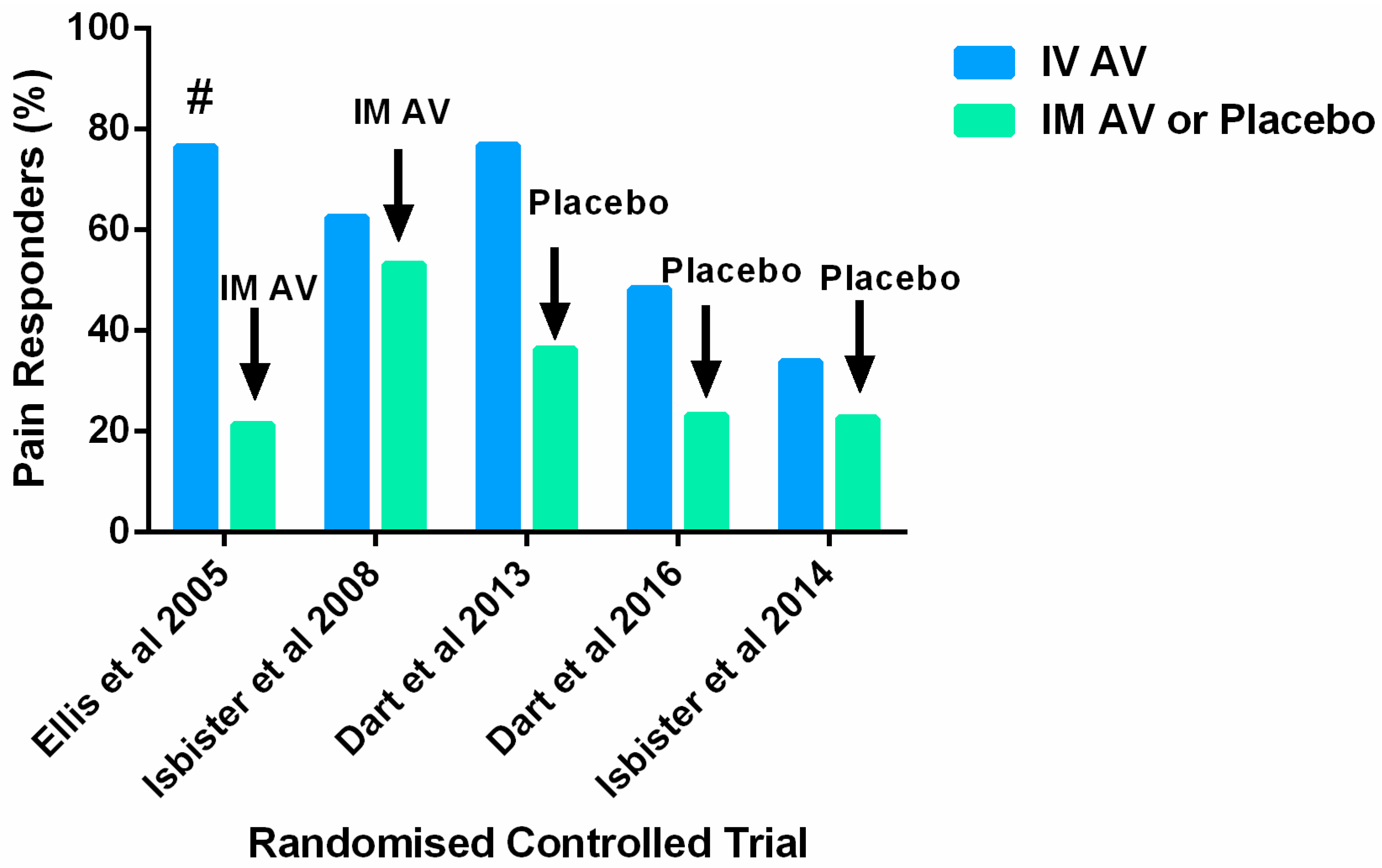
5.2. Randomised Clinical Trials of Antivenom for Latrodectism
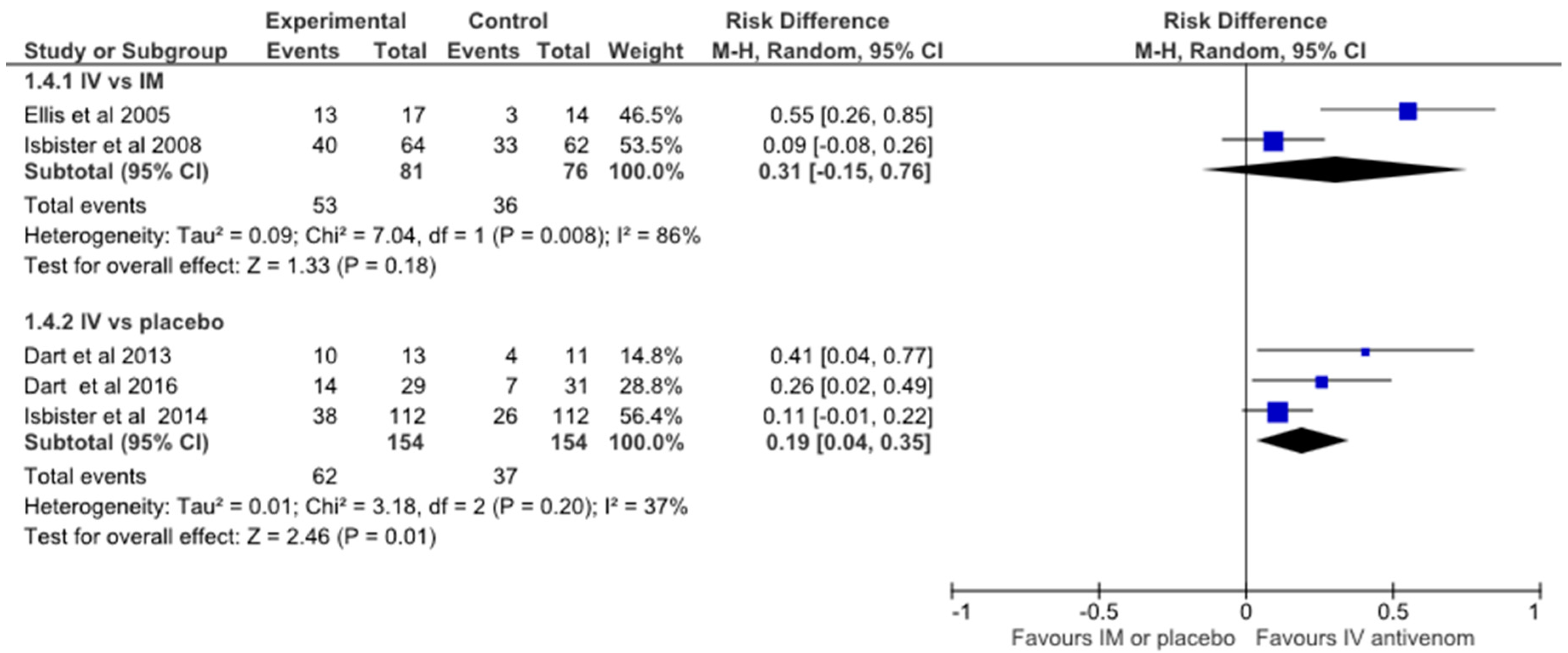
5.3. Meta-Analysis of Randomised Controlled Trials of Antivenom for Latrodectism
6. Discussion
7. Materials and Methods
Acknowledgments
Conflicts of Interest
References
- Clark, R.F.; Wethern-Kestner, S.; Vance, M.V.; Gerkin, R. Clinical presentation and treatment of black widow spider envenomation: A review of 163 cases. Ann. Emerg. Med. 1992, 21, 782–787. [Google Scholar] [CrossRef]
- Saucier, J.R. Arachnid envenomation. Emerg. Med. Clin. N. Am. 2004, 22, 405–422. [Google Scholar] [CrossRef] [PubMed]
- Thorp, R.W.; Woodson, W.D. The Black Widow Spider: (Formerly: Black Widow; America’s Most Poisonous Spider); University of North Carolina Press: Raleigh, NC, USA, 1945. [Google Scholar]
- Isbister, G.K.; Brown, S.G.; Miller, M.; Tankel, A.; Macdonald, E.; Stokes, B.; Ellis, R.; Nagree, Y.; Wilkes, G.J.; James, R.; et al. A randomised controlled trial of intramuscular vs. intravenous antivenom for latrodectism—The RAVE study. QJM 2008, 101, 557–565. [Google Scholar] [PubMed]
- Isbister, G.K.; Fan, H.W. Spider bite. Lancet 2011, 378, 2039–2047. [Google Scholar] [CrossRef]
- Nicholson, G.M.; Graudins, A. Spiders of medical importance in the Asia-Pacific: Atracotoxin, latrotoxin and related spider neurotoxins. Clin. Exp. Pharmacol. Physiol. 2002, 29, 785–794. [Google Scholar] [CrossRef] [PubMed]
- Monte, A.A.; Bucher-Bartelson, B.; Heard, K.J. A US Perspective of Symptomatic Latrodectus spp. Envenomation and Treatment: A national poison data system review. Ann. Pharmacother. 2011, 45, 1491–1498. [Google Scholar] [PubMed]
- Hlubek, M.D.; Stuenkel, E.L.; Krasnoperov, V.G.; Petrenko, A.G.; Holz, R.W. Calcium-Independent Receptor for a-Latrotoxin and Neurexin 1a Facilitate Toxin-Induced Channel Formation: Evidence That Channel Formation Results from Tethering of Toxin to Membrane. Mol. Pharmacol. 2000, 57, 519–528. [Google Scholar] [PubMed]
- Lelianova, V.G.; Davletov, B.A.; Sterling, A.; Rahman, M.A.; Grishin, E.V.; Totty, N.F.; Ushkaryov, Y.A. α-Latrotoxin Receptor, Latrophilin, Is a Novel Member of the Secretin Family of G Protein-coupled Receptors. J. Biol. Chem. 1997, 272, 21504–21508. [Google Scholar] [CrossRef] [PubMed]
- Khvotchev, M.; Südhof, T.C. α-latrotoxin triggers transmitter release via direct insertion into the presynaptic plasma membrane. EMBO J. 2000, 19, 3250–3262. [Google Scholar] [CrossRef] [PubMed]
- Isbister, G.K.; Gray, M.R. Latrodectism: A prospective cohort study of bites by formally identified redback spiders. Med. J. Aust. 2003, 179, 88–91. [Google Scholar] [PubMed]
- Maretić, Z. Latrodectism: Variations in clinical manifestations provoked by Latrodectus species of spiders. Toxicon 1983, 21, 457–466. [Google Scholar] [CrossRef]
- Ballantyne, J.C.; Carr, D.B.; deFerranti, S.; Suarez, T.; Lau, J.; Chalmers, T.C.; Angelillo, I.F.; Mosteller, F. The Comparative Effects of Postoperative Analgesic Therapies on Pulmonary Outcome: Cumulative Meta-Analyses of Randomized, Controlled Trials. Anesth. Analg. 1998, 86, 598–612. [Google Scholar] [CrossRef] [PubMed]
- Monte, A.A. Black widow spider (Latrodectus mactans) antivenom in clinical practice. Cur. Pharm. Biotechnol. 2012, 13, 1935–1939. [Google Scholar] [CrossRef]
- Clark, R.F. The Safety and Efficacy of Antivenin Latrodectus mactans. J. Toxicol. Clin. Toxicol. 2001, 39, 125–127. [Google Scholar] [CrossRef] [PubMed]
- Key, G.F. A comparison of calcium gluconate and methocarbamol (Robaxin) in the treatment of latrodectism (black widow spider envenomation). Am. J. Trop. Med. Hyg. 1981, 30, 273–277. [Google Scholar] [PubMed]
- Ryan, P.J. Preliminary report: Experience with the use of dantrolene sodium in the treatment of bites by the black widow spider Latrodectus hesperus. J. Toxicol. Clin. Toxicol. 1984, 21, 487–489. [Google Scholar] [CrossRef]
- Timms, P.K.; Gibbons, R.B. Latrodectism—Effects of the black widow spider bite. West. J. Med. 1986, 144, 315–317. [Google Scholar] [PubMed]
- Binder, L.S. Acute arthropod envenomation. Incidence, clinical features and management. Med. Toxicol. Adv. Drug Exp. 1989, 4, 163–173. [Google Scholar] [CrossRef]
- O’Malley, G.F.; Dart, R.C.; Kuffner, E.F. Successful treatment of latrodectism with antivenin after 90 h. N. Engl. J. Med. 1999, 340, 657. [Google Scholar] [CrossRef] [PubMed]
- Graudins, A. Medical Toxicology; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2004. [Google Scholar]
- Hahn, L.; Lewin, N. Goldfrank’s Toxicologic Emergencies; Flomenbaum, N.E., Goldfrank, L.R., Hoffmanm, R.S., Howland, M.A., Lewin, N.A., LS, N., Eds.; McGraw-Hill: New York, NY, USA, 2006. [Google Scholar]
- Gutierrez, J.M.; Leon, G.; Lomonte, B. Pharmacokinetic-pharmacodynamic relationships of immunoglobulin therapy for envenomation. Clin. Pharmacokinet. 2003, 42, 721–741. [Google Scholar] [CrossRef] [PubMed]
- Rivière, G.; Choumet, V.; Audebert, F.; Sabouraud, A.; Debray, M.; Scherrmann, J.-M.; Bon, C. Effect of antivenom on venom pharmacokinetics in experimentally envenomed rabbits: Toward an optimization of antivenom therapy. J. Pharmacol. Exp. Ther. 1997, 281, 1–8. [Google Scholar]
- Isbister, G.K.; Graudins, A.; White, J.; Warrell, D. Antivenom Treatment in Arachnidism. J. Toxicol. Clin. Toxicol. 2003, 41, 291–300. [Google Scholar] [CrossRef] [PubMed]
- Isbister, G.K. Antivenom efficacy or effectiveness: the Australian experience. Toxicology 2010, 268, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Ellis, R.M.; Sprivulis, P.C.; Jelinek, G.A.; Banham, N.D.; Wood, S.V.; Wilkes, G.J.; Siegmund, A.; Roberts, B.L. A double-blind, randomized trial of intravenous versus intramuscular antivenom for red-back spider envenoming. Emerg. Med. Australas. 2005, 17, 152–156. [Google Scholar] [CrossRef] [PubMed]
- Stanford, C.; Bush, S.; Clark, R.; Arnold, T.; Haynes, J.; Holstege, C.; Bogdan, G.; Garcia, W.; Smith, J.; Dart, R. A new F(ab)2 antivenom for widow spider envenomation (Latrodectism). In Clinical Toxicology; Informa Healthcare: New York, NY, USA, 2007. [Google Scholar]
- Isbister, G.K. Safety of i.v. administration of redback spider antivenom. Intern. Med. J. 2007, 37, 820–822. [Google Scholar] [PubMed]
- Graudins, A.; Padula, M.; Broady, K.; Nicholson, G.M. Red-back spider (Latrodectus hasselti) antivenom prevents the toxicity of widow spider venoms. Ann. Emerg. Med. 2001, 37, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Daly, F.F.S.; Daly, F.; Hill, R.E.; Bogdan, G.M.; Dart, R.C. Neutralization of Latrodectus mactans and L. hesperus Venom by Redback Spider (L. hasseltii) Antivenom. J. Toxicol. Clin. Toxicol. 2001, 39, 119–123. [Google Scholar] [CrossRef] [PubMed]
- Jelinek, G.A. Widow spider envenomation (latrodectism): A worldwide problem. Wilderness Environ. Med. 1997, 8, 226–231. [Google Scholar] [CrossRef]
- Hoyte, C.O.; Cushing, T.A.; Heard, K.J. Anaphylaxis to black widow spider antivenom. Am. J. Emerg. Med. 2012, 30, 836.e1-2. [Google Scholar] [CrossRef] [PubMed]
- Murphy, C.M.; Hong, J.J.; Beuhler, M.C. Anaphylaxis with Latrodectus Antivenin Resulting in Cardiac Arrest. J. Med. Toxicol. 2011, 7, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Wiener, S. Red back spider bite in Australia: An analysis of 167 cases. Med. J. Aust. 1961, 48, 44–49. [Google Scholar] [PubMed]
- Keegan, H.L. Effectiveness of Latrodectus tredecimguttatus antivenin in protecting laboratory mice against effects of intraperitoneal injections of Latrodectus mactans venom. Am. J. Trop. Med. Hyg. 1955, 4, 762–764. [Google Scholar] [PubMed]
- Sutherland, S.K.; Trinca, J.C. Survey of 2144 cases of red-back spider bites: Australia and New Zealand, 1963–1976. Med. J. Aust. 1978, 2, 620–623. [Google Scholar] [PubMed]
- Jelinek, G.A.; Banham, N.D.; Dunjey, S.J. Red-back spider-bites at Fremantle Hospital, 1982–1987. Med. J. Aust. 1989, 150, 693–695. [Google Scholar] [PubMed]
- Mead, H.J.; Jelinek, G.A. Red-back spider bites to Perth children, 1979-1988. J. Paediatr. Child Health 1993, 29, 305–308. [Google Scholar] [CrossRef] [PubMed]
- Anderson, P. Spider bites and scorpion stings. In Conn’s Current Therapy; Rakel, R., Ed.; W.B. Saunders: Philadelphia, PA, USA, 1988; pp. 1000–1002. [Google Scholar]
- Kunkel, D. Arthropod envenomations. Emerg. Med. Clin. N. Am. 1984, 2, 579–586. [Google Scholar]
- Rees, R.S.; Campbell, D. Spider bites. In Management of Wilderness and Environmental Emergencies; Auerbach, P., Geehr, E., Eds.; CV Mosby Company: St. Louis, MO, USA, 1989; pp. 548–549. [Google Scholar]
- Sutherland, S. Treatment of arachnid poisoning in Australia. Aust. Fam. Physician 1996, 5, 305–312. [Google Scholar]
- Mollison, L.; Liew, D.; McDermott, R.; Hatch, F. Red-back spider envenomation in the red centre of Australia. Med. J. Aust. 1994, 161, 704–705. [Google Scholar]
- Dzelalija, B.; Medic, A. Latrodectus bites in Northern Dalmatia, Croatia: Clinical, laboratory, epidemiological, and therapeutical aspects. Croatian Med. J. 2003, 44, 135–138. [Google Scholar]
- Trethewy, C.E.; Bolisetty, S.; Wheaton, G. Red-back spider envenomation in children in Central Australia. Emerg. Med. (Fremantle, W.A.) 2003, 15, 170–175. [Google Scholar] [CrossRef]
- Byrne, G.C.; Pemberton, P.J. Red-back spider (Latrodectus mactans hasselti) envenomation in a neonate. Med. J. Aust. 1983, 2, 665–666. [Google Scholar] [PubMed]
- Nordt, S.P.; Lee, A.; Sasaki, K.; Clark, R.; Cantrell, F.L. Retrospective review of black widow antivenom use. Clin. Toxicol. 2010, 48, 627. [Google Scholar]
- Basanou, E.; Kalostou, A.; Sofidiotou, V.; Fountas, K.; Kalantzopoulos, D.; Papathanassiou, V.; Neou, P. Treatment of black widow spider (Latrodectus mactans) envenomation: A review of 53 cases. Clin. Toxicol. 2015, 53, 281. [Google Scholar]
- Fatovich, D.M.; Dunjey, S.J.; Constantine, C.J.; Hirsch, R.L. Successful treatment of red-back spider bite using a Bier’s block technique. Med. J. Aust. 1999, 170, 342–343. [Google Scholar] [PubMed]
- Isbister, G.K.; O’Leary, M.; Miller, M.; Brown, S.G.A.; Ramasamy, S.; James, R.; Schneider, J.S. A comparison of serum antivenom concentrations after intravenous and intramuscular administration of redback (widow) spider antivenom. Br. J. Clin. Pharmacol. 2008, 65, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Dart, R.; Heard, K.; Bush, S.; Arnold, T.; Sutter, M.; Campagne, D.; Holstege, C.; Seifert, S.; Quan, D.; Borron, S.W. A Phase III Clinical Trial of Analatro (R)[Antivenin Latrodectus (Black Widow) Equine Immune F(ab’)2] in Patients with Systemic Latrodectism. In Clinical Toxicology; Taylor & Francis Ltd.: Abingdon, UK, 2016. [Google Scholar]
- Dart, R.C.; Bogdan, G.; Heard, K.; Bucher, B.B.; Garcia-Ubbelohde, W.; Bush, S.; Arnold, T.; Clark, R.C.; Hendey, G.W.; Holstege, C.; et al. A randomized, double-blind, placebo-controlled trial of a highly purified equine F(ab)2 antibody black widow spider antivenom. Ann. Emerg. Med. 2013, 61, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Isbister, G.K.; Page, C.B.; Buckley, N.A.; Fatovich, D.M.; Pascu, O.; MacDonald, S.P.; Calver, L.A.; Brown, S.G. Randomized controlled trial of intravenous antivenom versus placebo for latrodectism: The second Redback Antivenom Evaluation (RAVE-II) study. Ann. Emerg. Med. 2014, 64, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Loten, C.; Stokes, B.; Worsley, D.; Seymour, J.E.; Jiang, S.; Isbister, G.K. A randomised controlled trial of hot water (45 °C) immersion versus ice packs for pain relief in bluebottle stings. Med. J. Aust. 2006, 184, 329–333. [Google Scholar] [PubMed]
- Berthier, F.; Potel, G.; Leconte, P.; Touze, M.-D.; Baron, D. Comparative study of methods of measuring acute pain intensity in an ED. Am. J. Emerg. Med. 1998, 16, 132–136. [Google Scholar] [CrossRef]
- Bijur, P.E.; Latimer, C.T.; Gallagher, E.J. Validation of a verbally administered numerical rating scale of acute pain for use in the emergency department. Acad. Emerg. Med. 2003, 10, 390–392. [Google Scholar] [CrossRef] [PubMed]
- Ferreira-Valente, M.A.; Pais-Ribeiro, J.L.; Jensen, M.P. Validity of four pain intensity rating scales. Pain 2011, 152, 2399–2404. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study Author/s | Type of Study | N | Study Arms | Efficacy Outcome | Design Problems | Study Conclusion/s |
|---|---|---|---|---|---|---|
| Key, 1981 [16] | Prospective observational study, with cross over to the alternative treatment with treatment failure | 13/10 | calcium gluconate vs. methocarbamol | Not specified | Small study | Calcium gluconate should remain the treatment of first choice for latrodectism as it had a better outcome than methocarbamol |
| Ryan, 1984 [17] | Retrospective, case series | 6/2 | IV and oral dantrolene sodium vs oral dantrolene sodium | Not specified | Small uncontrolled study | Medication side effects noted as mild. Further studies on optimal dose and efficacy compared to other treatments necessary |
| Timms & Gibbons, 1986 [18] | Retrospective, case series | 11 | 9 pts received IV calcium gluconate with diazepam or methocarbamol, 1 received methocarbamol, meperidine hydrochloride and nasogastric suction and 1 received calcium gluconate and methylprednisolone sodium succinate. Two of the 11 patients also received L. mactans antivenom 2.5 mg IV. 7/11 pts required narcotic analgesics for pain. | Recovery Time | Small, uncontrolled non-comparative study | Latrodectism is responsive to calcium gluconate with muscle relaxant. AV is effective but rarely necessary and may result in serum sickness |
| Study Author/s | Type of Study | N | Treatment | Efficacy Outcome | Design Problems | Study Conclusion/s |
|---|---|---|---|---|---|---|
| Sutherland & Trinca, 1978 [37] | Retrospective case series | 2073/44 (IM/IV) | RBSAV IM/IV | Not specified | Reporting bias e. Data from questionnaires included with AV therefore no data on RBS bites that did not require AV, missing data. Multiple outcomes. | Difficult to elucidate—Signs and symptoms of envenomation and general perception of ‘good’ outcome after antivenom but no quantitation of outcome data presented. |
| Jelinek et al., 1989, [38] | Retrospective case series | 150 | RBSAV by IM if systemic symptoms present, n = 32. | Not specified | ED presentations only—May have selected more serious cases. | 11/32 pts given AV by IM needed more than 1 ampoule. Authors suggest this is because WA red-back spider is more venomous. |
| Clark, 1992, [1] | Retrospective case series | 163 | IV opioids and benzodiazepines +58 patients received L mactans AV by IV | Pain relief ≥30 min after treatment administered. | Retrospective review of case notes—There was an attempt to standardise with operational definitions for data entry; strict inclusion/exclusion criteria; small group of toxicologists looking after patients. Retrospective telephone follow up for delayed AV reactions could only be done in 9 patients. | Calcium gluconate was found to be ineffective while L mactans AV significantly shortened the duration of symptoms in severe envenomations. |
| Mead & Jelinek, 1993, [39] | Retrospective Paediatric case series | 241 | 21% of children received RBSAV | Not specified | Poorly defined criteria for systemic envenomation—May result in under-reporting. | Definite bite by RBS defined; syndrome in children primarily similar to adults. Use of AV comparable to previous studies in older age groups; however, no child received more than one ampoule. Results suggested that contrary to current opinion at the time [40,41,42,43] children may not be at an increased risk of morbidity from latrodectism. |
| Mollison et al., 1994, [44] | Retrospective ICU case series | 32 | 26 patients received RBSAV | Partial, features of red-back spider envenomation in Australian Aborigines determined by collecting data on standard forms | Only severe cases (ICU)-reported, no data kept on patients seen in ED. | Annual incidence of severe RBS bite calculated. Unlike earlier series this study had a predominance of female patients. |
| Dzelalirja & Medic, 2003, [45] | Retrospective case series & lab analysis | 32 | 21 patients received European WSAV | Pain intensity and duration after antivenom | Inadequate power for AV vs no AV comparison | Latrodectism in Northern Dalmatia presents with severe clinical symptoms. AV is advisable in the treatment of all afflicted patients. |
| Trethewy et al., 2003, [46] | Retrospective Paediatric case series | 54 | 45 patients received IM RBSAV | Not specified | Qualitative not quantitative assessment of symptoms-patient notes reviewed retrospectively. Clinical signs/symptoms difficult to define in children. For example, only 50% patients had a bite site identified. | No statistically significant difference between age groups for local or systemic envenomation even though the older children were twice the weight of younger group. This was in contrast to previous studies suggesting envenomation is different in children [37,47]. 46 children classified as systemic envenomation and 38 of these received RBSAV. |
| Isbister & Gray, 2003, [11] | Prospective case series on calls to NSW, QLD & WA Poison Information Centres and presentations to two Hospital ED (Sydney & Darwin). | 68 with definite RBS bite | 6 patients received IM RBSAV | Reported proportion of 6 patients with no pain at 24 h. | Study lacked power to compare IM AV and no treatment. | The severity of envenomation should be defined by the severity of pain and systemic features, AND also to the duration of these effects. Only 1/6 of patients receiving AV were pain-free at 24 h, an unacceptable treatment effect. IM RBSAV was no better than no treatment when all patients were followed up over a week. |
| Nordt et al., 2010, [48] ^ | Retrospective case series | 96 | All patients received L. mactans AV | Not specified | Published abstract only therefore limited methodology explained. | Symptomatic treatment for black widow spider envenomation includes opioid pain control and muscle relaxants. Definitive treatment includes AV to neutralize venom. Noted that adequate pain control is often difficult to achieve. Although derived from horse serum, hypersensitivity reactions appear to be mild and rare but further prospective studies are required to confirm. |
| Monte et al., 2011, [7] | Retrospective case series on Latrodectus spp. exposures & treatment reported to US National Poison Data System over 8 years. | 9872 | Patients received benzodiazepines, calcium, IV fluids or dilution/wash of bite site. 374 (3.8%) patients received L. mactans AV. | Not specified | Only cases reported to US poison centers reviewed. Dataset contained no information on dosing or timing of treatments. Unable to differentiate adverse drug reactions for the different treatments as most patients received multiple therapies and the dataset does not attribute ADRs to the specific treatment given. | Few patients received AV although it was associated with shorter symptom duration (<24 h) in moderate and major severity groups. There was no evidence of shorter symptom duration in patients who received benzodiazepines or calcium. Adverse drug reactions were more common in patients receiving benzos and AV. |
| Basanou et al., 2015, [49] ^ | Retrospective case series of Poisons Centre consults | 53 | Mod to severe cases (23/53) treated with IV benzos, n = 6, IV opioids n = 5 or combination of both n = 12. IV L. mactans AV in 5 patients with severe systemic effects. | Not specified possibly “symptomatic control” | Published abstract only therefore limited methodology explained. | Opioid analgesics combined with muscle relaxants, such as benzodiazepines, are generally effective at symptomatic control. In selected severe cases antivenom is the most efficacious therapy available. |
| Study Author/s | Number in Each Arm | Blinded | Allocation Concealed | AV Dose/Brand | Primary Outcome/s | Conclusion/s |
|---|---|---|---|---|---|---|
| Ellis et al., 2005 [27] | 15/18 (IM AV/IV AV) | Yes | Yes (1 from each arm was unblinded and removed from the analysis) | 500 units RBS Antivenom (CSL Ltd., Melbourne, Australia) | Partially defined 2: number of AV ampoules used and pain scores up to 2 h. | Both IM and IV RBSAV were deemed effective as after 1 h-pain VAS fell, with a better outcome at 24 h for the IV route. There were some major and acknowledged study limitations including too small sample size, and an insensitive primary outcome (N of AV ampoules) Thus the study was underpowered and inconclusively negative. |
| Isbister et al., 2008 [4] | 62/64 (IM AV/IV AV) | Yes | Yes | 1 or 2 vials of RBS Antivenom (equine Fab’2 500 U/vial, CSL Ltd., Australia) | Pain at 2 h after treatment administered. | No real difference in IV and IM routes. Further, RBSAV may provide no benefit over placebo. |
| Dart et al., 2013 [53] | 13/11 (AV/placebo) | Yes | Yes | 3 vials of Antivenom Latrodectus (Black Widow) Equine Immune F(ab)2 (Analatro®, Instituto Bioclon S.A. de C.V., Mexico). | VAS pain intensity at 150 min after treatment administered. | No difference between BWAV and placebo pain VAS * |
| Isbister et al., 2014 [54] | 112/112 (AV/placebo) | Yes | Yes | 2 vials of RBS Antivenom (equine Fab’2 500 U/vial, CSL Ltd., Australia) | Yes, pain at 2 h after treatment administered. | No difference between RBSAV and placebo pain VNRS ** |
| Dart et al., 2016 [52] ^ | AV/placebo | Yes ^ | Yes ^ | 1 to 2 doses of F(ab’)2 Antivenom (Analatro®) | Treatment failure-pain at 48 h after treatment administered. | F(ab’)2 AV was effective at reducing moderate to severe pain caused by latrodectism, however a 1-sided hypothesis test was used. No serious safety concerns were identified ^ |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ryan, N.M.; Buckley, N.A.; Graudins, A. Treatments for Latrodectism—A Systematic Review on Their Clinical Effectiveness. Toxins 2017, 9, 148. https://doi.org/10.3390/toxins9040148
Ryan NM, Buckley NA, Graudins A. Treatments for Latrodectism—A Systematic Review on Their Clinical Effectiveness. Toxins. 2017; 9(4):148. https://doi.org/10.3390/toxins9040148
Chicago/Turabian StyleRyan, Nicole M., Nicholas A. Buckley, and Andis Graudins. 2017. "Treatments for Latrodectism—A Systematic Review on Their Clinical Effectiveness" Toxins 9, no. 4: 148. https://doi.org/10.3390/toxins9040148
APA StyleRyan, N. M., Buckley, N. A., & Graudins, A. (2017). Treatments for Latrodectism—A Systematic Review on Their Clinical Effectiveness. Toxins, 9(4), 148. https://doi.org/10.3390/toxins9040148