
A Review on Manufacturing and Post-Processing Technology of Vascular Stents

Abstract
:1. Introduction
2. Clinical Trials
3. Stent Materials
3.1. Traditional Materials
3.2. Biodegradable Materials
4. Stent Manufacturing Techniques
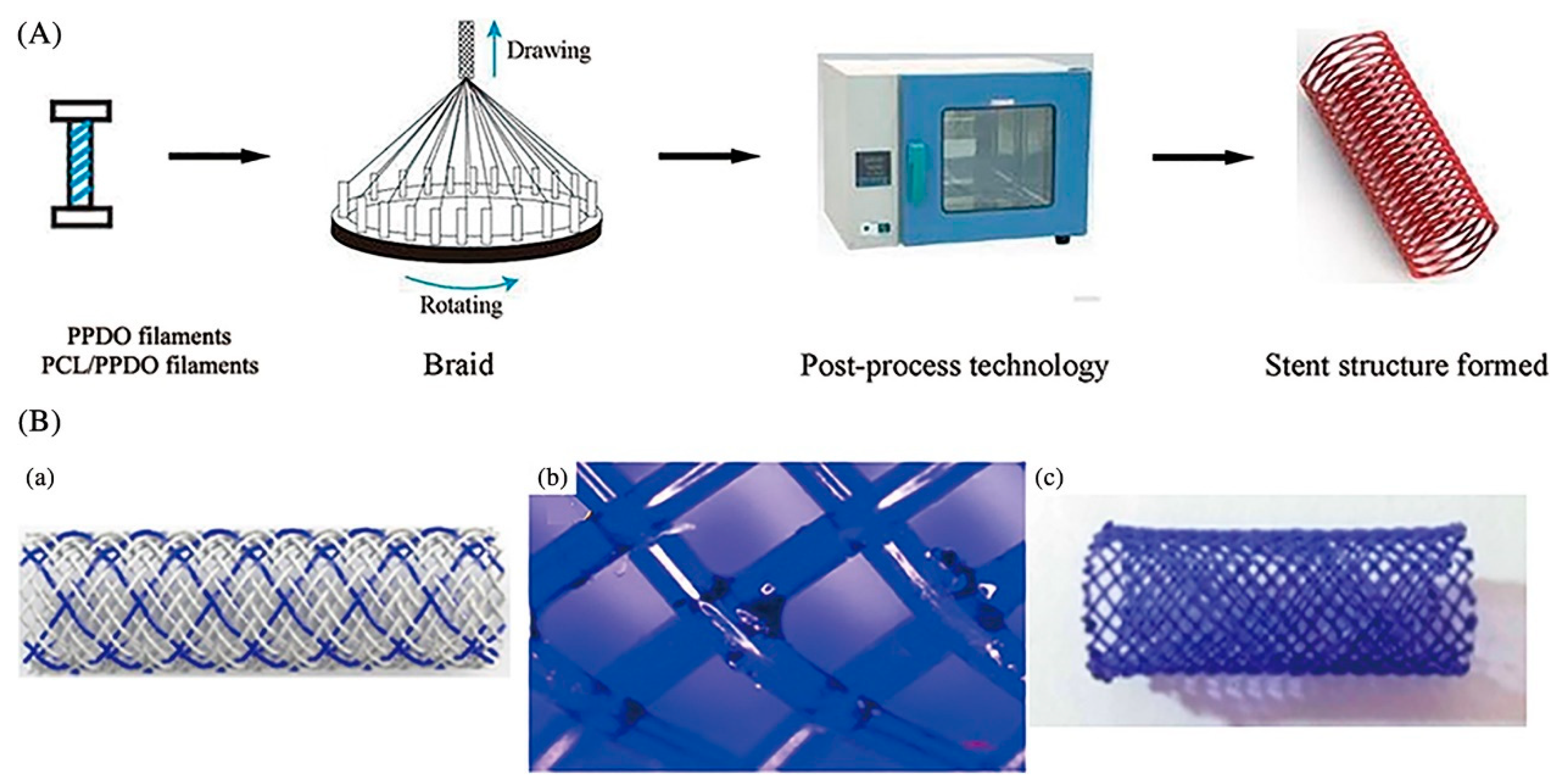
4.1. Braiding Technique
4.2. Micro-Injection Molding
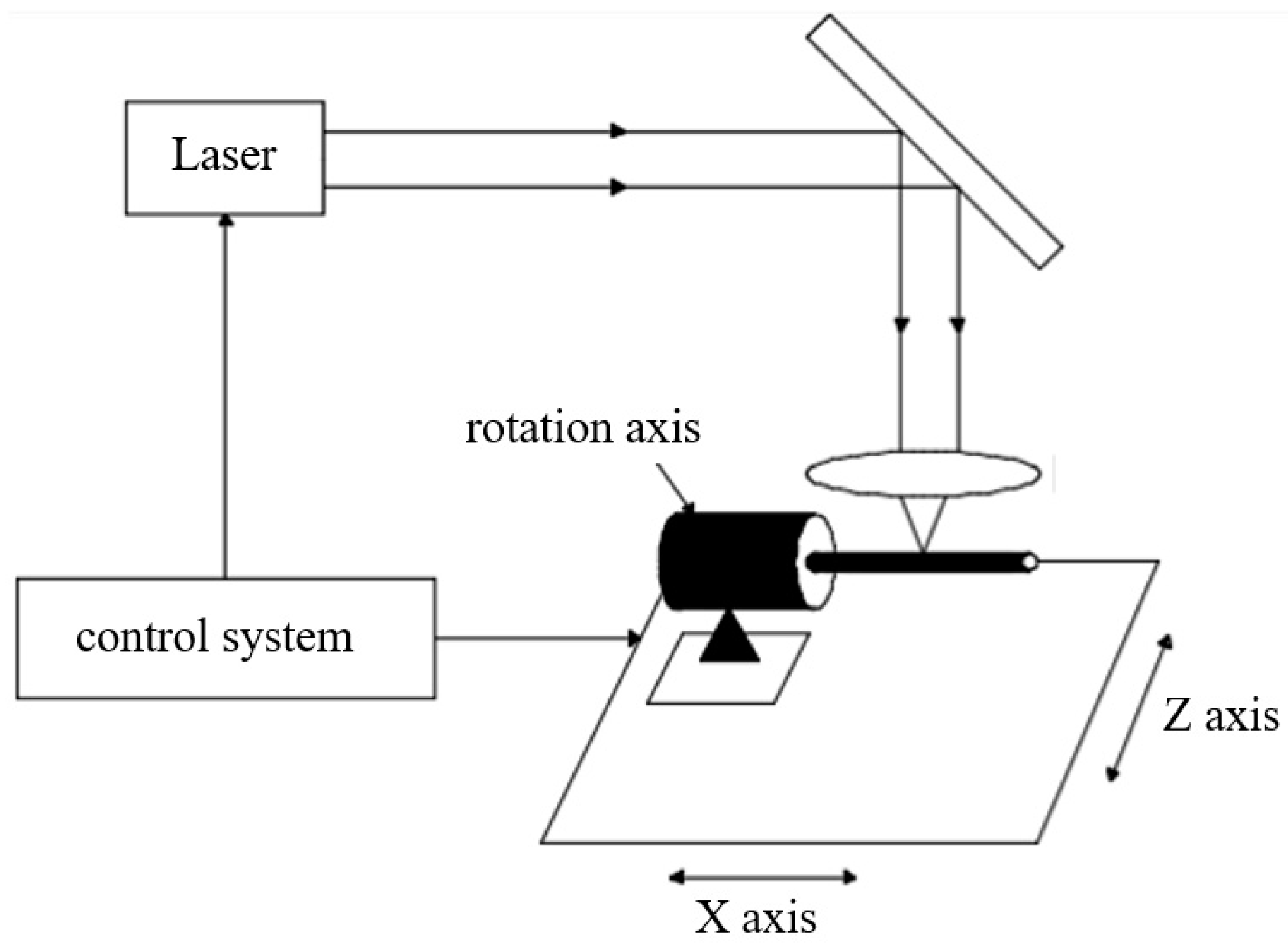
4.3. Laser Cutting
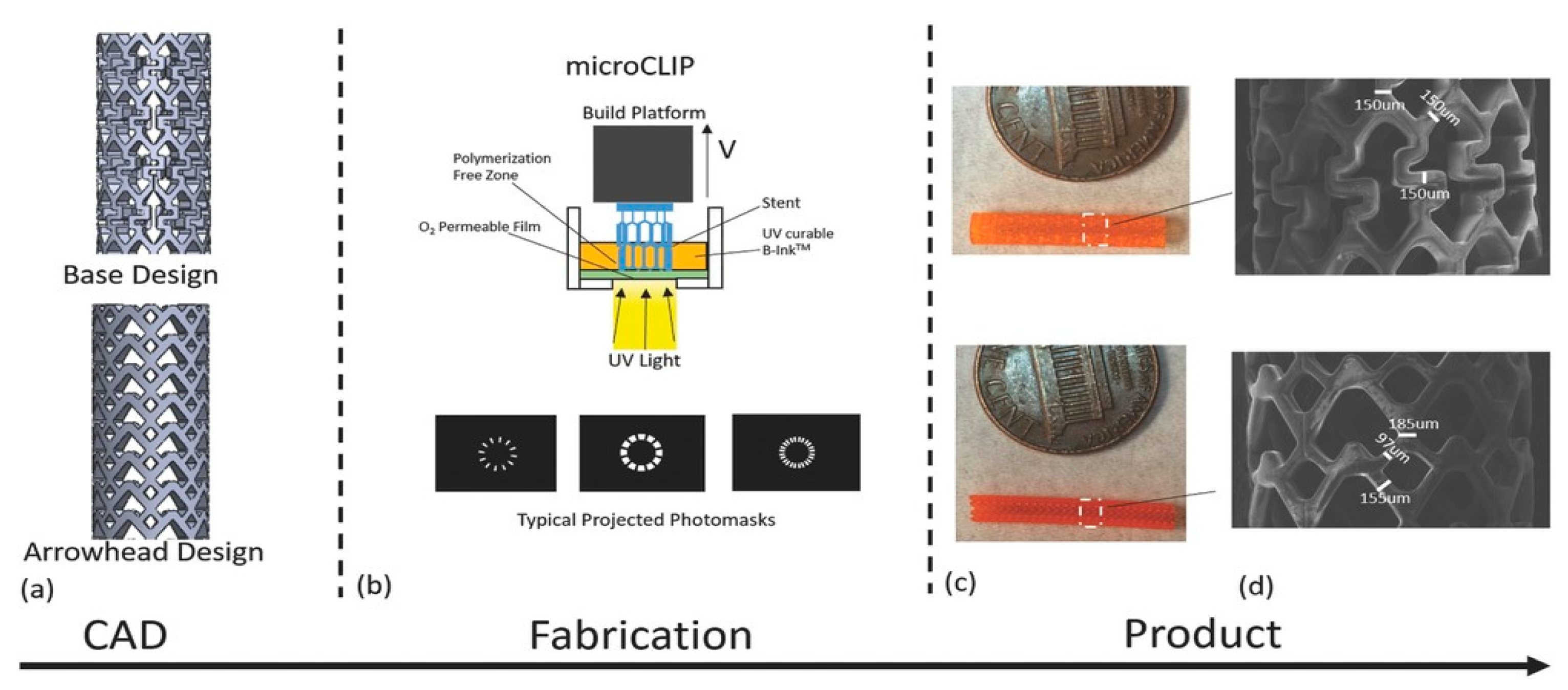
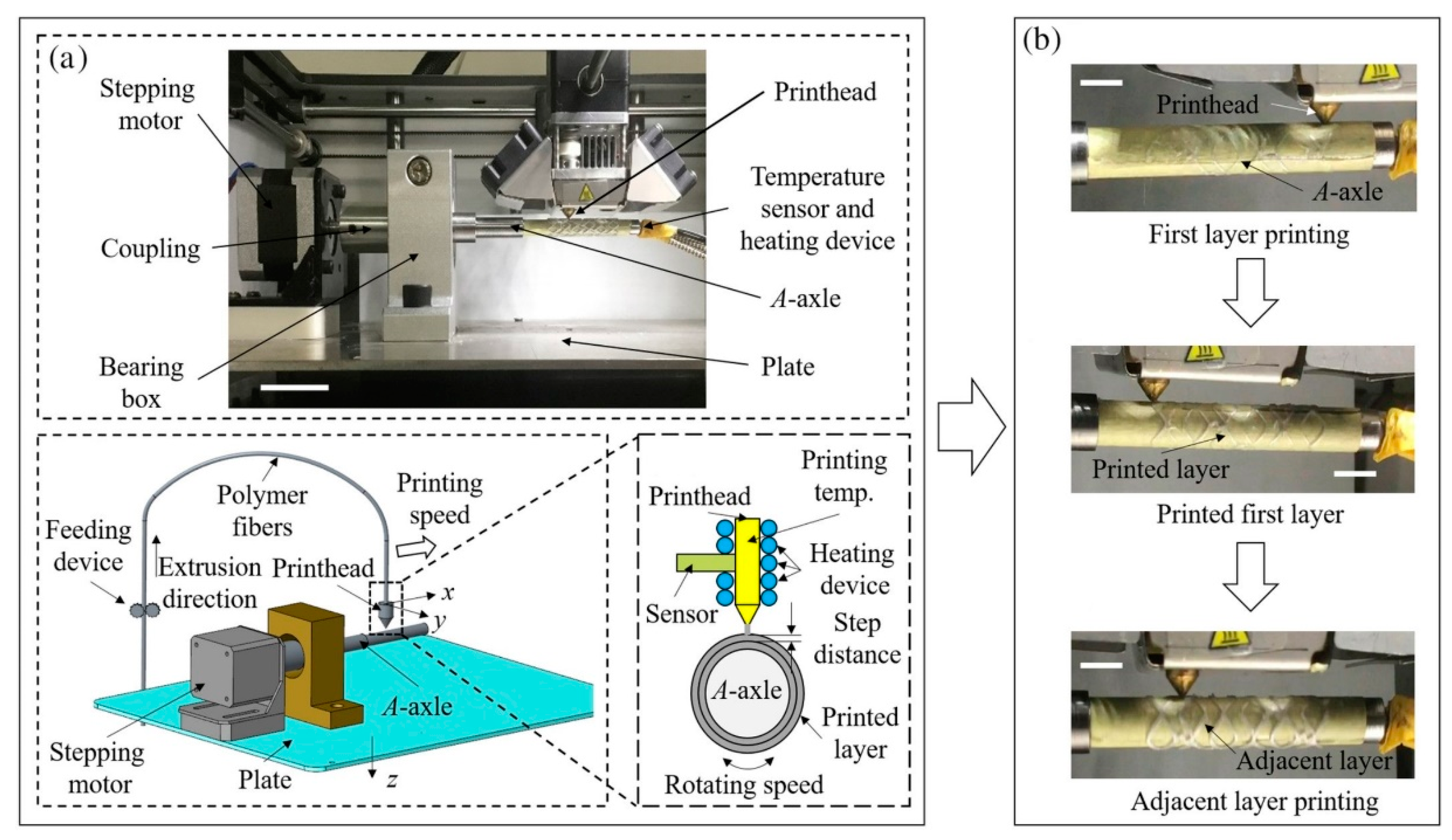
4.4. 3D Printing
4.5. Other Manufacturing Techniques
5. Post-Processing Techniques
5.1. Drug Coating
5.2. Surface Modification
5.3. Microstructures
5.4. Other Post-Processing Techniques
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- WHO. World Health Statistics 2020: Monitoring Health for the SDGs, Sustainable Development Goals; World Health Organization: Geneva, Switzerland, 2020.
- Sal, H.; Kara, B.; Krali, M.K. Focus on Coronary Atherosclerosis. In Atherosclerosis-Yesterday, Today and Tomorrow; Gianturco, L., Ed.; IntechOpen: Rijeka, Croatia, 2018; p. 7. [Google Scholar]
- Landau, C.; Lange, R.A.; Hillis, L.D. Percutaneous Transluminal Coronary Angioplasty. N. Engl. J. Med. 1994, 330, 981–993. [Google Scholar] [CrossRef]
- Block, P.C. Percutaneous transluminal coronary angioplasty. Am. J. Roentgenol. 1980, 135, 955–959. [Google Scholar] [CrossRef]
- Koo, Y.; Tiasha, T.; Shanov, V.N.; Yun, Y. Expandable Mg-based Helical Stent Assessment using Static, Dynamic, and Porcine Ex Vivo Models. Sci. Rep. 2017, 7, 1173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dotter, C.T.; Judkins, M.P. Percutaneous Transluminal Treatment of Arteriosclerotic Obstruction. Radiology 1965, 84, 631–643. [Google Scholar] [CrossRef] [PubMed]
- Dotter, C.T. Transluminally-placed Coilspring Endarterial Tube Grafts. Investig. Radiol. 1969, 4, 329–332. [Google Scholar] [CrossRef] [PubMed]
- Grüntzig, A. Transluminal dilatation of coronary-artery stenosis. Lancet 1978, 311, 263. [Google Scholar] [CrossRef]
- Palmaz, J.C.; Sibbitt, R.R.; Reuter, S.R.; Tio, F.O.; Rice, W.J. Expandable intraluminal graft: A preliminary study. Work in progress. Radiology 1985, 156, 73–77. [Google Scholar] [PubMed]
- Sigwart, U.; Puel, J.; Mirkovitch, V.; Joffre, F.; Kappenberger, L. Intravascular Stents to Prevent Occlusion and Re-Stenosis after Transluminal Angioplasty. N. Engl. J. Med. 1987, 316, 701–706. [Google Scholar] [CrossRef]
- Günther, R.W.; Vorwerk, D.; Bohndorf, K.; Klose, K.C.; Kistler, D.; Mann, H.; Sieberth, H.G.; El-Din, A. Venous stenoses in dialysis shunts: Treatment with self-expanding metallic stents. Radiology 1989, 170, 401–405. [Google Scholar] [CrossRef]
- Kim, M.; Taulbee, D.; Tremmel, M.; Meng, H. Comparison of Two Stents in Modifying Cerebral Aneurysm Hemodynamics. Ann. Biomed. Eng. 2008, 36, 726–741. [Google Scholar] [CrossRef] [PubMed]
- Palmerini, T.; Biondi-Zoccai, G.; Riva, D.D.; Stettler, C.; Sangiorgi, D.; D’Ascenzo, F.; Kimura, P.T.; Briguotri, C.; Sabatè, M.; Kim, H.S.; et al. Stent thrombosis with drug-eluting and bare-metal stents: Evidence from a comprehensive network meta-analysis. Lancet 2012, 379, 1393–1402. [Google Scholar] [CrossRef]
- Kirtane, A.J.; Gupta, A.; Iyengar, S.; Moses, J.W.; Leon, M.B.; Applegate, R.; Brodie, B.; Hannan, E.; Harjai, K.; Jen-sen, L.O.; et al. Safety and efficacy of drug eluting and bare metal stents: Comprehensive meta-analysis of randomized trials and observational studies. Circulation 2009, 119, 3198–3206. [Google Scholar] [CrossRef] [Green Version]
- Douglas, J.S. Role of adjunct pharmacologic therapy in the era of drug-eluting stents. Atheroscler. Suppl. 2005, 6, 47–52. [Google Scholar] [CrossRef]
- Karjalainen, P.P.; Nammas, W.; Airaksinen, J.K. Optimal stent design: Past, present and future. Interv. Cardiol. 2014, 6, 29–44. [Google Scholar] [CrossRef]
- Serruys, P.W.; Onuma, Y.; Garg, S.; Vranckx, P.; Bruyne, B.D.; Morice, M.C.; Colombo, A.; Macaya, C.; Richardt, G.; Fajadet, J. 5-year clinical outcomes of the ARTS II (Arterial Revascularization Therapies Study II) of the siroli-mus-eluting stent in the treatment of patients with multivessel de novo coronary artery lesions. J. Am. Coll. Cardiol. 2010, 55, 1093–1101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, B. Development of imported drug eluting stent. Chin. J. Cardiovasc. Med. 2009, 14, 263–265. [Google Scholar]
- Virmani, R. Localized hypersensitivity and late coronary thrombosis secondary to a sirolimuseluting stent: Should we be cautious. Circulation 2004, 110, 701–705. [Google Scholar] [CrossRef] [Green Version]
- Bourantas, C.V.; Onuma, Y.; Farooq, V.; Zhang, Y.; Serruys, P.W. Bioresorbable scaffolds: Current knowledge, potentialities and limitations experienced during their first clinical applications. Int. J. Cardiol. 2013, 167, 11–21. [Google Scholar] [CrossRef]
- Samochowiec, L.; Wójcicki, J.; Gregorczyk, K.; Szmatloch, E. Current status of bioresorbable scaffolds in the treatment of coronary artery disease. J. Am. Coll. Cardiol. 2014, 64, 2541–2551. [Google Scholar]
- Abizaid, A.; Schofer, J.; Maeng, M.; Witzenbichler, B.; Botelho, R.; Ormiston, J.A.; Costa, R.A.; Costa, J.D.; Chamié, D.; Abizaid, A.; et al. TCT- 610 Prospective, Multi-Center Evaluation of the DESolve Novolimus-Eluting Bioresorbable Coronary Scaffold: Imaging Outcomes and 2-Year Clinical Results. J. Am. Coll. Cardiol. 2014, 64, B178. [Google Scholar] [CrossRef] [Green Version]
- Ormiston, J.A.; Serruys, P.W.; Evelyn, R.; Dariusz, D.; Leif, T.; Webster, M.W.I.; Yoshinobu, O.; Garcia-Garcia, H.M.; Robert, M.G.; Susan, V. A bioabsorbable everolimuseluting coronary stent system for patients with single denovo coronary artery lesions (ABSORB): A prospective open-label trial. Lancet 2008, 371, 899–907. [Google Scholar] [CrossRef]
- Lin, W.; Qin, L.; Qi, H.; Zhang, D.; Zhang, G.; Gao, R.; Qiu, H.; Xia, Y.; Cao, P.; Wang, X.; et al. Long-term in vivo corrosion behavior, biocompatibility and bioresorption mechanism of a bioresorbable nitrided iron scaffold. Acta Biomater. 2017, 54, 454–468. [Google Scholar] [CrossRef]
- Ormiston, J.A.; Dixon, S.R.; Webster, M.W.I.; Ruygrok, P.N.; Stewart, J.T.; Minchington, I.; West, T. Stent longitudinal flexibility: A comparison of 13 stent designs before and after balloon expansion. Catheter. Cardiovasc. Interv. 2000, 50, 120–124. [Google Scholar] [CrossRef]
- Wei, L.; Chen, Q.; Li, Z.-Y. Study on the impact of straight stents on arteries with different curvatures. J. Mech. Med. Biol. 2016, 16, 1650093. [Google Scholar] [CrossRef]
- Azaouzi, M.; Makradi, A.; Belouettar, S. Numerical investigations of the structural behavior of a balloon expandable stent design using finite element method. Comput. Mater. Sci. 2013, 72, 54–61. [Google Scholar] [CrossRef]
- Wei, Y.B.; Wang, M.J.; Zhao, D.Y.; Li, H.X. In vitroexperimental study on the mechanical properties of biodegradable polymer stents. J. Biomed. Eng. 2019, 36, 604–612. [Google Scholar]
- Wei, Y.B.; Zhao, D.Y.; Wang, M.J.; Li, H.X. Design and Mechanics Analysis of Biodegradable Polymer Vascular Stents with High Radial Supporting Property. Chin. J. Mech. Eng. 2020, 31, 1098–1107. [Google Scholar]
- Douglas, G.R.; Phani, A.S.; Gagnon, J. Analyses and design of expansion mechanisms of balloon expandable vascular stents. J. Biomech. 2014, 47, 1438–1446. [Google Scholar] [CrossRef] [PubMed]
- Dolla, W.J.S.; Fricke, B.A.; Becker, B.R. Structural and Drug Diffusion Models of Conventional and Auxetic Drug-Eluting Stents. J. Med. Devices 2006, 1, 47–55. [Google Scholar] [CrossRef]
- Tan, T.W.; Douglas, G.R.; Bond, T.; Phani, A.S. Compliance and Longitudinal Strain of Cardiovascular Stents: Influence of Cell Geometry. J. Med. Devices 2011, 5, 041002. [Google Scholar] [CrossRef]
- Liu, R.; Xu, S.; Luo, X.; Liu, Z. Theoretical and Numerical Analysis of Mechanical Behaviors of a Metamaterial-Based Shape Memory Polymer Stent. Polymers 2020, 12, 1784. [Google Scholar] [CrossRef]
- Ruan, X.L.; Li, J.J.; Song, X.K.; Zhou, H.J.; Yuan, W.; Wu, W.W.; Xia, R. Mechanical Design of Antichiral-Reentrant Hybrid Intravascular Stent. Int. J. Appl. Mech. 2019, 10, 1850105. [Google Scholar] [CrossRef]
- Han, Y.; Lu, W. Optimizing the deformation behavior of stent with nonuniform Poisson's ratio distribution for curved artery. J. Mech. Behav. Biomed. Mater. 2018, 88, 442–452. [Google Scholar] [CrossRef] [PubMed]
- Auricchio, F.; Conti, M.; De Beule, M.; De Santis, G.; Verhegghe, B. Carotid artery stenting simulation: From patient-specific images to finite element analysis. Med. Eng. Phys. 2011, 33, 281–289. [Google Scholar] [CrossRef]
- Morlacchi, S.; Colleoni, S.G.; Cardenes, R.; Chiastra, C.; Diez, J.L.; Larrabide, I.; Migliavacca, F. Patient-specific simulations of stenting procedures in coronary bifurcations: Two clinical cases. Med. Eng. Phys. 2013, 35, 1272–1281. [Google Scholar] [CrossRef]
- Ragkousis, G.E.; Curzen, N.; Bressloff, N.W. Simulation of longitudinal stent deformation in a patient-specific coronary artery. Med. Eng. Phys. 2014, 36, 467–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueng, K.-C.; Wen, S.-P.; Lou, C.-W.; Lin, J.-H. Stainless steel/nitinol braid coronary stents: Braiding structure stability and cut section treatment evaluation. J. Ind. Text. 2014, 45, 965–977. [Google Scholar] [CrossRef]
- Sun, J.; Sun, K.; Bai, K.; Chen, S.; Wang, F.; Zhao, F.; Hong, N.; Hu, H. A Novel Braided Biodegradable Stent for Use in Congenital Heart Disease: Short-term Results in Porcine Iliac Artery. J. Biomed. Mater. Res. 2019, 107, 1667–1677. [Google Scholar] [CrossRef]
- Huang, B.; Castro, D.; Gale, D.C.; Hossainy, S.F.A. Fabricating Polymer Stents with Injection Molding. U.S. Patent US20080001330A1, 28 June 2006. [Google Scholar]
- Li, H.; Liu, K.; Zhao, D.; Wang, M.; Li, Q.; Hou, J. Multi-Objective Optimizations for Microinjection Molding Process Parameters of Biodegradable Polymer Stent. Materials 2018, 11, 2322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, S.-J.; Chiang, F.-J.; Hsiao, C.-Y.; Kau, Y.-C.; Liu, K.-S. Fabrication of Balloon-Expandable Self-Lock Drug-Eluting Polycaprolactone Stents Using Micro-Injection Molding and Spray Coating Techniques. Ann. Biomed. Eng. 2010, 38, 3185–3194. [Google Scholar] [CrossRef]
- Momma, C.; Knop, U. Laser Cutting of Slotted Tube Coronary Stents—State of the Art and Future Developments. Prog. Biomed. Res. 1999, 4, 39–44. [Google Scholar]
- Li, C.; Nikumb, S.; Wong, F. An optimal process of femtosecond laser cutting of NiTi shape memory alloy for fabrication of miniature devices. Opt. Lasers Eng. 2005, 44, 1078–1087. [Google Scholar] [CrossRef]
- Raval, A.; Choubey, A.; Engineer, C.; Kothwala, D. Development and Assessment of 316LVM Cardiovascular Stents. Mater. Sci. Eng. A 2004, 386, 331–343. [Google Scholar] [CrossRef]
- Chen, C.-S.; Lin, S.-Y.; Chou, N.-K.; Chen, Y.-S.; Ma, S.-F. Optimization of Laser Processing in the Fabrication of Stents. Mater. Trans. 2012, 53, 2023–2027. [Google Scholar] [CrossRef] [Green Version]
- Kathuria, Y. Laser microprocessing of metallic stent for medical therapy. J. Mater. Process. Technol. 2005, 170, 545–550. [Google Scholar] [CrossRef]
- García-López, E.; Medrano-Tellez, A.G.; Ibarra-Medina, J.R.; Siller, H.R.; Rodriguez, C.A. Experimental Study of Back Wall Dross and Surface Roughness in Fiber Laser Microcutting of 316L Miniature Tubes. Micromachines 2017, 9, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baer, G.M.; Small, W.; Wilson, T.S.; Benett, W.J.; Matthews, D.L.; Hartman, J.; Maitland, D.J. Fabrication and in Vitro Deployment of a Laser-Activated Shape Memory Polymer Vascular Stent. BioMed. Eng. Online 2007, 6, 43. [Google Scholar] [CrossRef] [Green Version]
- Stępak, B.; Antończak, A.; Bartkowiak-Jowsa, M.; Filipiak, J.; Pezowicz, C.; Abramski, K. Fabrication of a polymer-based biodegradable stent using a CO2 laser. Arch. Civ. Mech. Eng. 2014, 14, 317–326. [Google Scholar] [CrossRef]
- Demir, A.G.; Previtali, B.; Colombo, D.; Ge, Q.; Vedani, M.; Petrini, L.; Wu, W.; Biffi, C.A. Fiber Laser Micromachining of Magnesium Alloy Tubes for Biocompatible and Biodegradable Cardiovascular Stents. In Proceedings of the Fiber Lasers IX: Technology, Systems, and Applications, San Francisco, CA, USA, 15 February 2012; p. 823730. [Google Scholar]
- Liu, L.; Li, D.B.; Tong, Y.F.; Zhu, Y.F. Fiber laser micromachining of thin NiTi tubes for shape memory vascular stents. Appl. Phys. A 2016, 122, 638. [Google Scholar] [CrossRef]
- Guerra, A.; de Ciurana, J. Fibre laser cutting of polymer tubes for stents manufacturing. Procedia Manuf. 2017, 13, 190–196. [Google Scholar] [CrossRef]
- Meng, H.; Liao, J.; Zhou, Y.; Zhang, Q. Laser micro-processing of cardiovascular stent with fiber laser cutting system. Opt. Laser Technol. 2009, 41, 300–302. [Google Scholar] [CrossRef]
- Muhammad, N.; Whitehead, D.; Boor, A.; Oppenlander, W.; Liu, Z.; Li, L. Picosecond laser micromachining of nitinol and platinum–iridium alloy for coronary stent applications. Appl. Phys. A 2011, 106, 607–617. [Google Scholar] [CrossRef]
- Flege, C.; Vogt, F.; Höges, S.; Jauer, L.; Borinski, M.; Schulte, V.A.; Hoffmann, R.; Poprawe, R.; Meiners, W.; Jobmann, M.; et al. Development and characterization of a coronary polylactic acid stent prototype generated by selective laser melting. J. Mater. Sci. Mater. Electron. 2012, 24, 241–255. [Google Scholar] [CrossRef] [PubMed]
- Finazzi, V.; Demir, A.G.; Biffi, C.A.; Migliavacca, F.; Petrini, L.; Previtali, B. Design and Functional Testing of a Novel Balloon-Expandable Cardiovascular Stent in CoCr Alloy Produced by Selective Laser Melting. J. Manuf. Processes 2020, 55, 161–173. [Google Scholar] [CrossRef]
- Van Lith, R.; Baker, E.; Ware, H.; Yang, J.; Farsheed, A.C.; Sun, C.; Ameer, G. 3D-Printing Strong High-Resolution Antioxidant Bioresorbable Vascular Stents. Adv. Mater. Technol. 2016, 1, 1600138. [Google Scholar] [CrossRef]
- Ware, H.O.T.; Farsheed, A.C.; Akar, B.; Duan, C.; Chen, X.; Ameer, G.; Sun, C. High-Speed on-Demand 3D Printed Bioresorbable Vascular Scaffolds. Mater. Today Chem. 2018, 7, 25–34. [Google Scholar] [CrossRef]
- Guerra, A.J.; Cano, P.; Rabionet, M.; Puig, T.; Ciurana, J. 3D-Printed PCL/PLA Composite Stents: Towards a New Solution to Cardiovascular Problems. Materials 2018, 11, 1679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.; Zhang, L.; Liu, Y.; Liu, L.; Leng, J. 4D printing of personalized shape memory polymer vascular stents with negative Poisson’s ratio structure: A preliminary study. Sci. China Technol. Sci. 2020, 63, 578–588. [Google Scholar] [CrossRef]
- Jia, H.; Gu, S.-Y.; Chang, K. 3D printed self-expandable vascular stents from biodegradable shape memory polymer. Adv. Polym. Technol. 2018, 37, 3222–3228. [Google Scholar] [CrossRef]
- Zhao, D.; Zhou, R.; Sun, J.; Li, H.; Jin, Y. Experimental study of polymeric stent fabrication using homemade 3D printing system. Polym. Eng. Sci. 2019, 59, 1122–1131. [Google Scholar] [CrossRef]
- Levy, Y.; Khan, W.; Farah, S.; Domb, A.J. Surface Crystallization of Rapamycin on Stents Using a Temperature Induced Process. Langmuir 2012, 28, 6207–6210. [Google Scholar] [CrossRef]
- Khan, W.; Farah, S.; Nyska, A.; Domb, A.J. Carrier Free Rapamycin Loaded Drug Eluting Stent: In Vitro and in Vivo Evaluation. J. Control. Release 2013, 168, 70–76. [Google Scholar] [CrossRef]
- Shanshan, C.; Lili, T.; Yingxue, T.; Bingchun, Z.; Ke, Y. Study of drug-eluting coating on metal coronary stent. Mater. Sci. Eng. C 2013, 33, 1476–1480. [Google Scholar] [CrossRef] [PubMed]
- Raval, A.; Parikh, J.; Engineer, C. Mechanism and in Vitro Release Kinetic Study of Sirolimus from a Biodegradable Polymeric Matrix Coated Cardiovascular Stent. Ind. Eng. Chem. Res. 2011, 50, 9539–9549. [Google Scholar] [CrossRef]
- Petersen, S.; Hussner, J.; Reske, T.; Grabow, N.; Senz, V.; Begunk, R.; Arbeiter, D.; Kroemer, H.K.; Schmitz, K.-P.; zu Schwabedissen, H.E.M.; et al. In vitro study of dual drug-eluting stents with locally focused sirolimus and atorvastatin release. J. Mater. Sci. Mater. Med. 2013, 24, 2589–2600. [Google Scholar] [CrossRef] [PubMed]
- van der Giessen, W.J.; Sorop, O.; Serruys, P.W.; Peters-Krabbendam, I.; van Beusekom, H.M. Lowering the Dose of Sirolimus, Released From a Nonpolymeric Hydroxyapatite Coated Coronary Stent, Reduces Signs of Delayed Healing. JACC Cardiovasc. Interv. 2009, 2, 284–290. [Google Scholar] [CrossRef] [Green Version]
- Meng, S.; Liu, Z.; Shen, L.; Guo, Z.; Chou, L.L.; Zhong, W.; Du, Q.; Ge, J. The effect of a layer-by-layer chitosan–heparin coating on the endothelialization and coagulation properties of a coronary stent system. Biomaterials 2009, 30, 2276–2283. [Google Scholar] [CrossRef] [PubMed]
- Qiu, T.; Jiang, W.; Yan, P.; Jiao, L.; Wang, X. Development of 3D-Printed Sulfated Chitosan Modified Bioresorbable Stents for Coronary Artery Disease. Front. Bioeng. Biotechnol. 2020, 8, 462. [Google Scholar] [CrossRef] [PubMed]
- Hossfeld, S.; Nolte, A.; Hartmann, H.; Recke, M.; Schaller, M.; Walker, T.; Kjems, J.; Schlosshauer, B.; Stoll, D.; Wendel, H.-P.; et al. Bioactive coronary stent coating based on layer-by-layer technology for siRNA release. Acta Biomater. 2013, 9, 6741–6752. [Google Scholar] [CrossRef]
- Kim, T.G.; Lee, H.; Jang, Y.; Park, T.G. Controlled Release of Paclitaxel from Heparinized Metal Stent Fabricated by Layer-by-Layer Assembly of Polylysine and Hyaluronic Acid-g-Poly(Lactic-Co-Glycolic Acid) Micelles Encapsulating Paclitaxel. Biomacromolecules 2009, 10, 1532–1539. [Google Scholar] [CrossRef] [PubMed]
- Palmaz, J.C.; Benson, A.; Sprague, E.A. Influence of surface topography on endothelialization of intravascular metallic material. J. Vasc. Interv. Radiol. 1999, 10, 439. [Google Scholar] [CrossRef]
- Wang, J.; Li, Y.; Gao, L.; Wang, S.; Mao, A.; Liu, B. Preparation of the micro/nano structures of the biomimetic coating stent for loading MiRNA126 by four-beam laser interference. Optik 2017, 128, 247–252. [Google Scholar] [CrossRef]
- Aguilar, C.A.; Lu, Y.; Mao, S.; Chen, S. Direct micro-patterning of biodegradable polymers using ultraviolet and femtosecond lasers. Biomaterials 2005, 26, 7642–7649. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Jiang, L.; Hu, J.; Liu, H.; Wang, S.; Zuo, P.; Ji, P.; Qu, L.; Cui, T. Multifunctional 3D Micro-Nanostructures Fabricated through Temporally Shaped Femtosecond Laser Processing for Preventing Thrombosis and Bacterial Infection. ACS Appl. Mater. Interfaces 2020, 12, 17155–17166. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Yang, Z.; Bi, C.W.C.; Yang, M.; Xu, S.L.; Lu, X.; Huang, N.; Huang, P.; Leng, Y. Directing Vascular Cell Selectivity and Hemocompatibility on Patterned Platforms Featuring Variable Topographic Geometry and Size. ACS Appl. Mater. Interfaces 2014, 6, 12062–12070. [Google Scholar] [CrossRef]
- Palmerini, T.; Benedetto, U.; Biondi-Zoccai, G.; Della Riva, D.; Bacchi-Reggiani, L.; Smits, P.C.; Vlachojannis, G.J.; Jensen, L.O.; Christiansen, E.H.; Berencsi, K.; et al. Long-Term Safety of Drug-Eluting and Bare-Metal Stents. J. Am. Coll. Cardiol. 2015, 65, 2496–2507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sousa, J.E.; Costa, M.A.; Abizaid, A.; Abizaid, A.S.; Feres, F.; Pinto, I.M.F.; Seixas, A.C.; Staico, R.; Mattos, L.A.; Sousa, A.G.M.R.; et al. Lack of Neointimal Proliferation After Implantation of Sirolimus-Coated Stents in Human Coronary Arteries. Circulation 2001, 103, 192–195. [Google Scholar] [CrossRef] [Green Version]
- Brugaletta, S. Absorb Bioresorbable Vascular Scaffold Versus Everolimus-Eluting Metallic Stent in ST-Segment Elevation Myocardial Infarction: 1-Year Results of a Propensity Score Matching Comparison. JACC Cardiovasc. Interv. 2015, 8, 9. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, P.S.; Ramos, R.G. Images in clinical medicine. Coronary-stent fracture. N. Engl. J. Med. 2002, 347, 581. [Google Scholar] [CrossRef]
- Scheinert, D.; Scheinert, S.; Sax, J.; Piorkowski, C.; Bräunlich, S.; Ulrich, M.; Biamino, G.; Schmidt, A. Prevalence and Clinical Impact of Stent Fractures after Femoropopliteal Stenting. J. Am. Coll. Cardiol. 2005, 45, 312–315. [Google Scholar] [CrossRef] [Green Version]
- Shaikh, F.; Maddikunta, R.; Djelmami-Hani, M.; Solis, J.; Allaqaband, S.; Bajwa, T. Stent Fracture, an Incidental Finding or a Significant Marker of Clinical in-Stent Restenosis? Cathet. Cardiovasc. Intervent. 2008, 71, 614–618. [Google Scholar] [CrossRef] [PubMed]
- Doi, H.; Maehara, A.; Mintz, G.S.; Tsujita, K.; Kubo, T.; Castellanos, C.; Liu, J.; Yang, J.; Oviedo, C.; Aoki, J.; et al. Classification and Potential Mechanisms of Intravascular Ultrasound Patterns of Stent Fracture. Am. J. Cardiol. 2009, 103, 818–823. [Google Scholar] [CrossRef]
- Dotter, C.T.; Buschmann, R.W.; McKinney, M.K.; Rosch, J. Transluminal expandable nitinol coil stent grafting: Preliminary report. Radiology 1983, 147, 259–260. [Google Scholar] [CrossRef]
- Cragg, A.; Lund, G.; Rysavy, J.; Castaneda, F.; Castaneda-Zuniga, W.; Amplatz, K. Nonsurgical placement of arterial endoprostheses: A new technique using nitinol wire. Radiology 1983, 147, 261–263. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Zhao, N.; Zhu, D. Biphasic Responses of Human Vascular Smooth Muscle Cells to Magnesium Ion: SMC Responses to Mg. J. Biomed. Mater. Res. 2016, 104, 347–356. [Google Scholar] [CrossRef]
- Kirkland, N.T.; Lespagnol, J.; Birbilis, N.; Staiger, M.P. A Survey of Bio-Corrosion Rates of Magnesium Alloys. Corros. Sci. 2010, 52, 287–291. [Google Scholar] [CrossRef]
- Böse, D.; Eggebrecht, H.; Haude, M.; Schmermund, A.; Erbel, R. First Absorbable Metal Stent Implantation in Human Coronary Arteries. Amer. Heart Hosp. J. 2006, 4, 128–130. [Google Scholar] [CrossRef]
- Erbel, R.; Mario, C.D.; Bartunek, J.; Bonnier, J.; de Bruyne, B.; Eberli, F.R.; Erne, P.; Haude, M.; Heublein, B.; Horrigan, M.; et al. Temporary Scaffolding of Coronary Arteries with Bioabsorbable Magnesium Stents: A Prospective, Non-Randomised Multicentre Trial. Lancet 2007, 369, 7. [Google Scholar] [CrossRef]
- Cao, N.Q.; Pham, D.N.; Kai, N.; Dinh, H.V.; Hiromoto, S.; Kobayashi, E. In Vitro Corrosion Properties of Mg Matrix In Situ Composites Fabricated by Spark Plasma Sintering. Metals 2017, 7, 358. [Google Scholar] [CrossRef] [Green Version]
- Patil, A.J.; Jackson, O.; Fulton, L.B.; Hong, D.; Desai, P.A.; Kelleher, S.A.; Chou, D.-T.; Tan, S.; Kumta, P.N.; Beniash, E. Anticorrosive Self-Assembled Hybrid Alkylsilane Coatings for Resorbable Magnesium Metal Devices. ACS Biomater. Sci. Eng. 2017, 3, 518–529. [Google Scholar] [CrossRef]
- Vallee, B.L.; Falchuk, K.H. The biochemical basis of zinc physiology. Physiol. Rev. 1993, 73, 79–118. [Google Scholar] [CrossRef]
- Bowen, P.K.; Drelich, J.; Goldman, J. Zinc Exhibits Ideal Physiological Corrosion Behavior for Bioabsorbable Stents. Adv. Mater. 2013, 25, 2577–2582. [Google Scholar] [CrossRef]
- Guillory, R.J.; Bowen, P.K.; Hopkins, S.P.; Shearier, E.R.; Earley, E.J.; Gillette, A.A.; Aghion, E.; Bocks, M.L.; Drelich, J.W.; Goldman, J. Corrosion Characteristics Dictate the Long-Term Inflammatory Profile of Degradable Zinc Arterial Implants. ACS Biomater. Sci. Eng. 2016, 2, 2355–2364. [Google Scholar] [CrossRef] [PubMed]
- Drelich, A.J.; Zhao, S.; Guillory, R.J.; Drelich, J.W.; Goldman, J. Long-term surveillance of zinc implant in murine artery: Surprisingly steady biocorrosion rate. Acta Biomater. 2017, 58, 539–549. [Google Scholar] [CrossRef] [PubMed]
- Drelich, A.J.; Bowen, P.K.; LaLonde, L.; Goldman, J.; Drelich, J.W. Importance of oxide film in endovascular biodegradable zinc stents. Surf. Innov. 2016, 4, 133–140. [Google Scholar] [CrossRef]
- Jarzębska, A.; Bieda, M.; Kawałko, J.; Rogal, Ł.; Koprowski, P.; Sztwiertnia, K.; Pachla, W.; Kulczyk, M. A New Approach to Plastic Deformation of Biodegradable Zinc Alloy with Magnesium and Its Effect on Microstructure and Mechanical Properties. Mater. Lett. 2018, 211, 58–61. [Google Scholar] [CrossRef]
- Tamai, H.; Igaki, K.; Kyo, E.; Kosuga, K.; Kawashima, A.; Matsui, S.; Komori, H.; Tsuji, T.; Motohara, S.; Uehata, H. Initial and 6-Month Results of Biodegradable Poly- l -Lactic Acid Coronary Stents in Humans. Circulation 2000, 102, 399–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grabow, N.; Schlun, M.; Sternberg, K.; Hakansson, N.; Kramer, S.; Schmitz, K.-P. Mechanical Properties of Laser Cut Poly(L-Lactide) Micro-Specimens: Implications for Stent Design, Manufacture, and Sterilization. J. Biomech. Eng. 2005, 127, 25–31. [Google Scholar] [CrossRef]
- Hu, T.; Yang, J.; Cui, K.; Rao, Q.; Yin, T.; Tan, L.; Zhang, Y.; Li, Z.; Wang, G. Controlled Slow-Release Drug-Eluting Stents for the Prevention of Coronary Restenosis: Recent Progress and Future Prospects. ACS Appl. Mater. Interfaces 2015, 7, 11695–11712. [Google Scholar] [CrossRef]
- Kwon, D.; Kim, J.; Kim, D.; Kang, H.; Lee, B.; Lee, K.; Kim, M. Biodegradable stent. J. Biomed. Sci. Eng. 2012, 5, 208–216. [Google Scholar] [CrossRef] [Green Version]
- Yang, C.; Yin, X.H.; Cheng, G.M. Microinjection molding of microsystem components: New aspects in improving performance. J. Micromech. Microeng. 2013, 23, 093001. [Google Scholar] [CrossRef]
- Heckele, M.; Schomburg, W.K. Review on micro molding of thermoplastic polymers. J. Micromech. Microeng. 2003, 14, R1–R14. [Google Scholar] [CrossRef]
- Holzer, C.; Gobrecht, J.; Schift, H.; Solak, H. Replication of Micro- and Nanostructures on Polymer Surfaces. Macromol. Symp. 2010, 296, 316–323. [Google Scholar] [CrossRef]
- Lee, W.L.; Wang, D.; Wu, J.; Ge, Q.; Low, H.Y. Injection Molding of Superhydrophobic Submicrometer Surface Topography on Macroscopically Curved Objects: Experimental and Simulation Studies. ACS Appl. Polym. Mater. 2019, 1, 1547–1558. [Google Scholar] [CrossRef]
- Stormonth-Darling, J.M.; Pedersen, R.H.; How, C.; Gadegaard, N. Injection Moulding of Ultra High Aspect Ratio Nanostructures Using Coated Polymer Tooling. J. Micromech. Microeng. 2014, 24, 075019. [Google Scholar] [CrossRef]
- Takahata, K.; Gianchandani, Y. A Planar Approach for Manufacturing Cardiac Stents: Design, Fabrication, and Mechanical Evaluation. J. Microelectromech. Syst. 2004, 13, 933–939. [Google Scholar] [CrossRef]
- Kuribayashi, K.; Tsuchiya, K.; You, Z.; Tomus, D.; Umemoto, M.; Ito, T.; Sasaki, M. Self-deployable origami stent grafts as a biomedical application of Ni-rich TiNi shape memory alloy foil. Mater. Sci. Eng. A 2006, 419, 131–137. [Google Scholar] [CrossRef]
- De Miranda, R.L.; Zamponi, C.; Quandt, E. Fabrication of TiNi thin film stents. Smart Mater. Struct. 2009, 18, 104010. [Google Scholar] [CrossRef]
- Rumpf, H.; Wipperfürth, V.; Zamponi, C.; Quandt, E. Near Net-Shape Fabrication of Superelastic NiTi Devices by Sputtering and Photoetching. Mater. Trans. 2006, 47, 523–526. [Google Scholar] [CrossRef] [Green Version]
- Grube, E.; Schofer, J.; Hauptmann, K.E.; Nickenig, G.; Curzen, N.; Allocco, D.J.; Dawkins, K.D. A Novel Paclitaxel-Eluting Stent with an Ultrathin Abluminal Biodegradable Polymer: 9-Month Outcomes with the JACTAX HD Stent. JACC Cardiovasc. Interv. 2010, 3, 431–438. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.; Liu, Y.; Chen, Y.; Liu, S.; Maitz, M.F.; Wang, X.; Zhang, K.; Wang, J.; Wang, Y.; Chen, J.; et al. Immobilization of Heparin/Poly-l-Lysine Nanoparticles on Dopamine-Coated Surface to Create a Heparin Density Gradient for Selective Direction of Platelet and Vascular Cells Behavior. Acta Biomater. 2014, 10, 1940–1954. [Google Scholar] [CrossRef]
- He, Y.; Zhou, T.; Dong, X.; Zhu, Z.; Yu, Q.; Liu, P.; Zhao, W.; Wang, X.; Hu, Y.; Yan, J. Diffraction manipulation of visible light with submicron structures for structural coloration fabrication. Opt. Express 2021, 29, 9294–9311. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; He, Y.; Wang, T.; Zhu, Z.; Xu, R.; Yu, Q.; Zhao, B.; Zhao, W.; Liu, P.; Wang, X. A review of the techniques for the mold manufacturing of micro/nanostructures for precision glass molding. Int. J. Extreme Manuf. 2021, 3, 042002. [Google Scholar] [CrossRef]
- Plant, S.; Grant, D.; Leach, L. Behaviour of human endothelial cells on surface modified NiTi alloy. Biomaterials 2005, 26, 5359–5367. [Google Scholar] [CrossRef] [PubMed]
- Hryniewicz, T.; Rokicki, R.; Rokosz, K. Co–Cr Alloy Corrosion Behaviour after Electropolishing and “Magnetoelectropolishing” Treatments. Mater. Lett. 2008, 62, 3073–3076. [Google Scholar] [CrossRef]
- Demir, A.G.; Previtali, B. Additive manufacturing of cardiovascular CoCr stents by selective laser melting. Mater. Des. 2017, 119, 338–350. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Methods | Advantages | Disadvantages |
|---|---|---|
| Braiding technique [39,40] | Easy to process | Limited to simple structure Poor radial stiffness |
| Micro-injection molding [41,42,43] | High production efficiency Good surface quality High consistency | Difficult to processing |
| Laser cutting [44,45,46,47,48,49,50,51,52,53,54,55,56] | Good quality High processing accuracy | Heat-affected zone |
| 3D printing [57,58,59,60,61,62,63,64] | Personalized customization High material utilization | Poor accuracy |
| μEDM Micro-photochemical etching Magnetron sputtering [110,111,112,113] | Burr/dross-free | Limited to specific materials |
| Micro-precision milling | High production efficiency High processing accuracy | Burrs |
| Drug | Structural Formula | Mode of Action | Products |
|---|---|---|---|
| Sirolimus |  | Anti-proliferative, immunosuppressive | Cordis Corporation, Hialeah, FL, USA Abbott Vascular, Temecula, CA, USA Biotronik, Berlin, Germany MicroPort, Shanghai, China |
| Everolimus |  | Immunosuppressive | Cordis Corporation, Hialeah, FL, USA Abbott Vascular, Temecula, CA, USA Biotronik, Berlin, Germany MicroPort, Shanghai, China |
| Paclitaxel |  | Anti-proliferative agent | Boston Scientific, Marlborough, MA, USA Conor Medsystems, Menlo Park, CA, USA Cook Medical, Bloomington, IN, USA Biotronik, Berlin, Germany Sahajanand Medical, Surat India |
| Tacrolimus |  | Anti-proliferative, immunosuppressive | Kaneka Corporation, Osaka, Japan Sorin Biomedica, Saluggia, Italy |
| Zotarolimus |  | Anti-proliferative, immunosuppressive | Medtronic CardioVascular, Minneapolis, MN, USA |
| Umirolimus |  | Immunosuppressive | Biosensors Inc., Schenectady, NY, USA Terumo Corporation, Tokyo, Japan Biosensors Europe SA, Morges, Switzerland |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, W.; Zhao, W.; Zhou, T.; Wang, L.; Qiu, T. A Review on Manufacturing and Post-Processing Technology of Vascular Stents. Micromachines 2022, 13, 140. https://doi.org/10.3390/mi13010140
Jiang W, Zhao W, Zhou T, Wang L, Qiu T. A Review on Manufacturing and Post-Processing Technology of Vascular Stents. Micromachines. 2022; 13(1):140. https://doi.org/10.3390/mi13010140
Chicago/Turabian StyleJiang, Wei, Wenxiang Zhao, Tianfeng Zhou, Liang Wang, and Tianyang Qiu. 2022. "A Review on Manufacturing and Post-Processing Technology of Vascular Stents" Micromachines 13, no. 1: 140. https://doi.org/10.3390/mi13010140
APA StyleJiang, W., Zhao, W., Zhou, T., Wang, L., & Qiu, T. (2022). A Review on Manufacturing and Post-Processing Technology of Vascular Stents. Micromachines, 13(1), 140. https://doi.org/10.3390/mi13010140