
Extraction and Evaluation of Discriminative Indexes of the Wearing Condition for High-Precision Blood Pressure Pulse Wave Measurement

Abstract
:1. Introduction
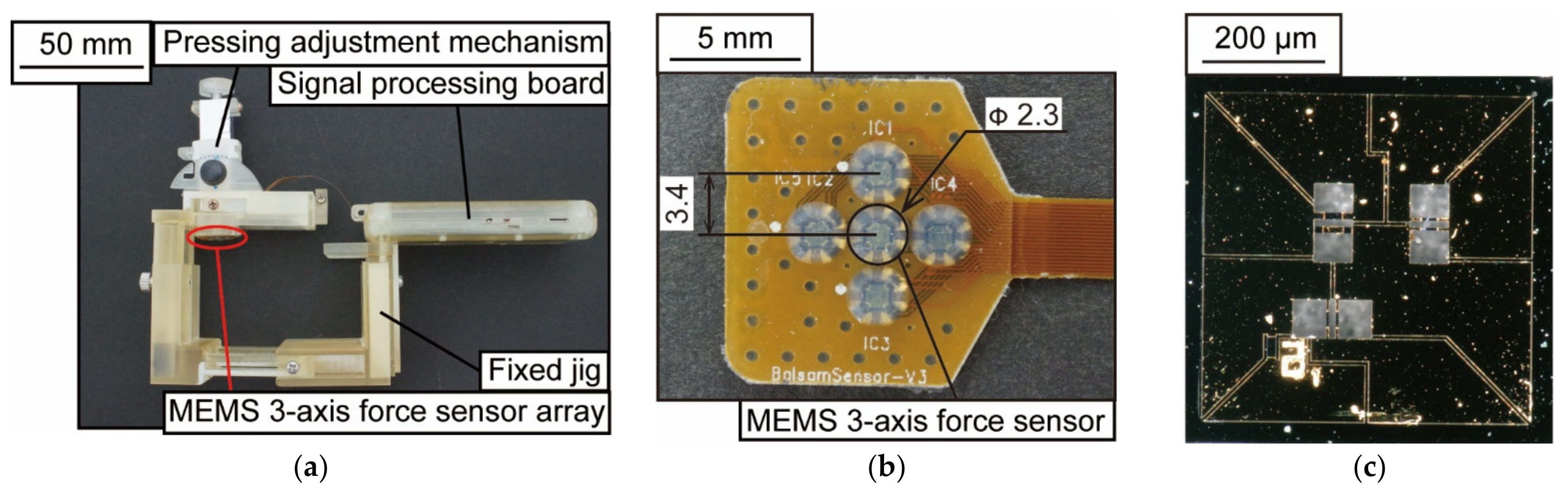
2. Principle and Device
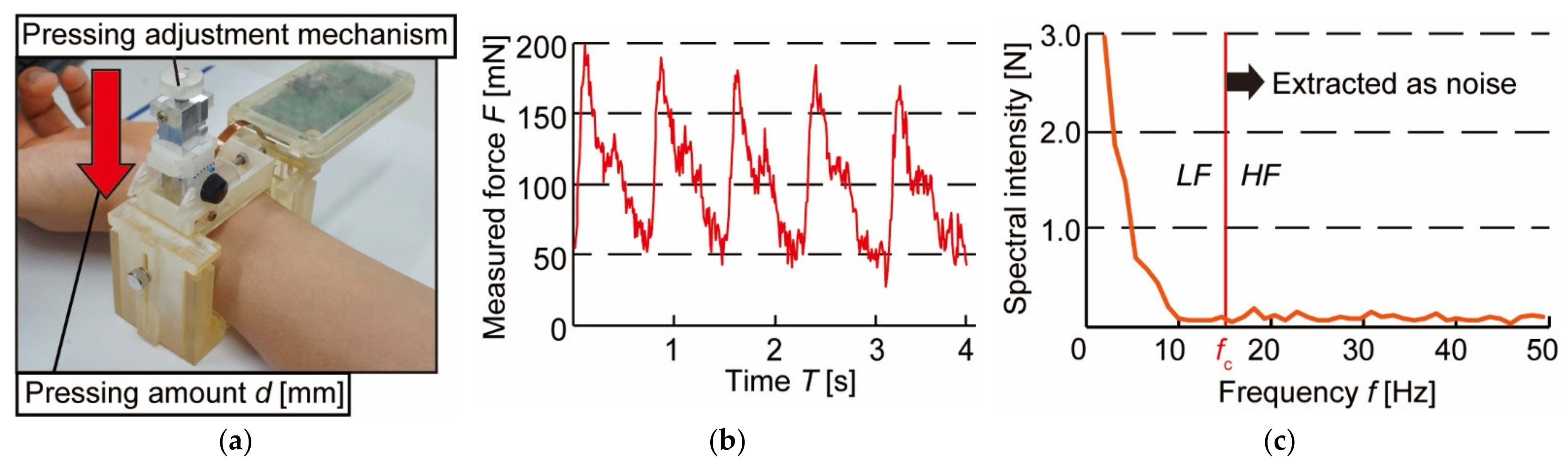
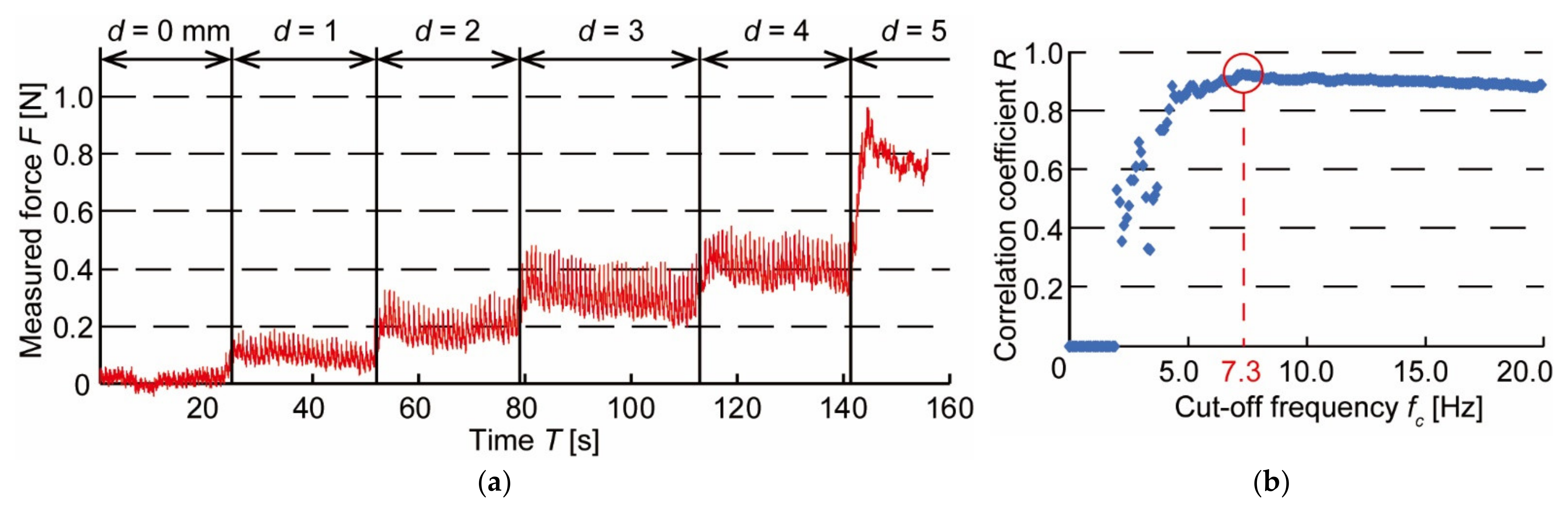
3. Experiments and Results
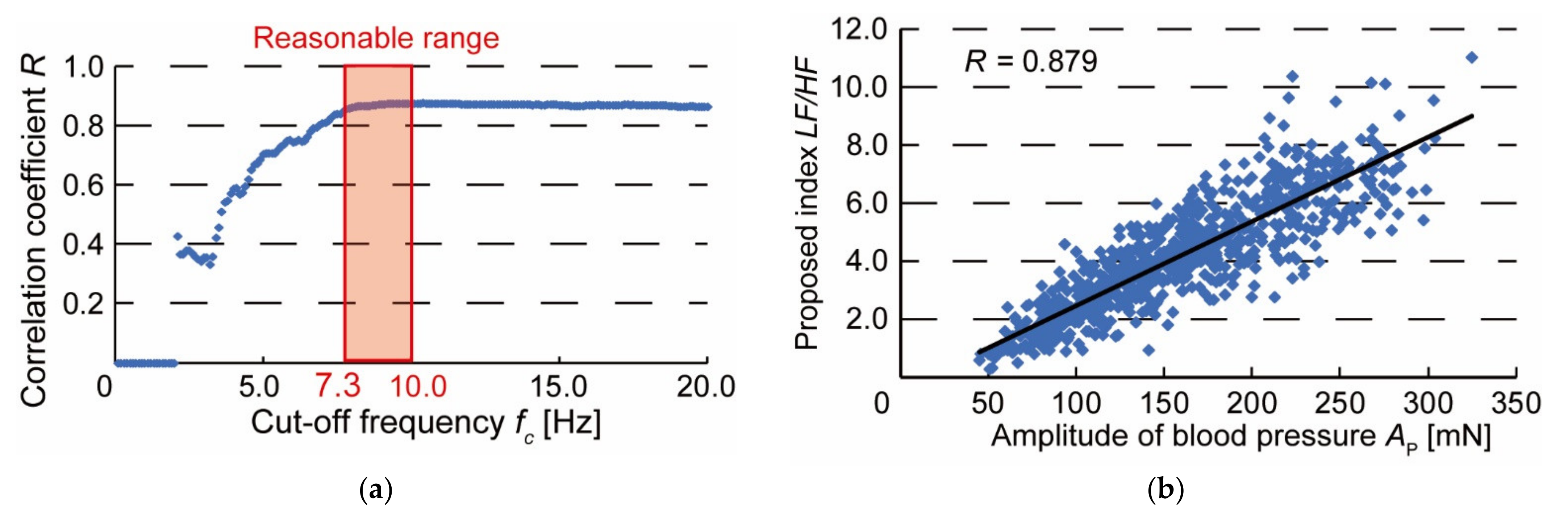
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Psaty, B.M.; Furberg, C.D.; Kuller, L.H.; Cushman, M.; Savage, P.J.; Levine, D.; O’Leary, D.H.; Bryan, R.N.; Anderson, M.; Lumley, T. Association Between Blood Pressure Level and the Risk of Myocardial Infarction, Stroke, and Total Mortality. Arch. Intern. Med. 2001, 161, 1183–1192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castillo, J.; Leira, R.; Garcia, M.M.; Serena, J.; Blanco, M. Blood pressure decrease during the acute phase of ischemic stroke is associated with brain injury and poor stroke outcome. Stroke 2004, 35, 520–527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, P.S. Oscillometric measurement of blood pressure a simplified explanation. A technical note on behalf of the British and Irish hypertension society. J. Hum. Hypertens. 2019, 33, 349–351. [Google Scholar] [CrossRef] [PubMed]
- Noda, A.; Okada, T.; Hayashi, H.; Yasuma, F.; Yokota, M. 24-hour ambulatory blood pressure variability in obstructive sleep apnea syndrome. Chest 1993, 103, 1343–1347. [Google Scholar] [CrossRef] [PubMed]
- Mansoor, G.A.; White, W.B. Olecranon bursitis associated with 24-hour ambulatory blood pressure monitoring. Am. J. Hypertens. 1994, 7, 855–856. [Google Scholar] [CrossRef] [PubMed]
- Dohi, T.; Waki, K. Blood pressure pulse wave measurement using a wristband type device with 3-axis force sensor. Int. Symp. Micro-Nano Sci. Technol. 2016, 2016, SuA1-B-8. [Google Scholar]
- Dohi, T.; Urata, H.; Fukahori, S.; Hori, M.; Nakai, A.; Nakamura, H. A Continuous and Wearable Blood Pressure Measurement Device with MEMS 3-Axis Force Sensor Array. In Proceedings of the Transducers 2019 International Conference on Solid-State Sensors, Actuators and Microsystems, Berlin, Germany, 23–27 June 2019; pp. 2182–2184. [Google Scholar]
- Sato, M.; Dohi, T. Blood pressure pulse wave device with 5-axis adjusting mechanism. Robomech 2016, 2P1-02b5. (In Japanese) [Google Scholar] [CrossRef]
- Dueck, R.; Goedje, O.; Clopton, P. Noninvasive continuous beat-to-beat radial artery pressure via TL-200 applanation tonometry. J. Clin. Monit. Comput. 2012, 26, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Kato, Y.; Hamaguchi, T. Sensor technology to realize continuous blood pressure monitoring. Omron Tech. 2018, 50, 26–34. [Google Scholar]
- Canning, J.; Helbert, K.; Iashin, G.; Matthews, J.; Yang, J.; Delano, M.K.; Sodini, C.G.; Zhang, Q. Noninvasive and continuous blood pressure measurement via superficial temporal artery tonometry. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Orlando, FL, USA, 16–20 August 2016; pp. 3382–3385. [Google Scholar]
- Shimura, K.; Hori, M.; Dohi, T.; Takao, H. The Calibration Method for Blood Pressure Pulse Wave Measurement Based on Arterial Tonometry Method. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Honolulu, HI, USA, 18–21 July 2018; pp. 3642–3645. [Google Scholar]
- Osawa, Y.; Hata, S.; Hori, M.; Dohi, T. Comparison of Features by Simultaneous Measurement of Blood Pressure Pulse Wave and Electrocardiogram. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Montreal, QC, Canada, 20–24 July 2020; pp. 4664–4667. [Google Scholar]
- Osawa, Y.; Hata, S.; Hori, M.; Dohi, T. Analysis of Blood Pressure Pulse Wave and Electrocardiogram Waveforms Measured by a Wearable Device with MEMS Sensors. Sens. Mater. 2021, 33, 1063–1072. [Google Scholar] [CrossRef]
- Kemmotsu, O.; Ueda, M.; Otuka, H.; Yamamura, T.; Okamura, A.; Ishikawa, T.; Winter, D.C.; Eckerle, J.S. Blood pressure measurement by arterial tonometry in controlled hypotension. Anesth. Analg. 1991, 73, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Nakai, A.; Thanh-Vinh, N.; Matsumoto, K.; Shimoyama, I. A triaxial tactile sensor without crosstalk using pairs of piezoresistive beams with sidewall doping. Sens. Actuators 2013, 199, 43–48. [Google Scholar] [CrossRef]
- McKenzie, I. Heart rate and blood pressure variability in subjects exposed to simulated increases in gravity. Exp. Physiol. 1993, 78, 825–834. [Google Scholar] [CrossRef] [PubMed]
- Holdsworth, D.W.; Norley, C.J.D.; Frayne, R.; Steinman, D.A.; Rutt, B.K. Characterization of common carotid artery blood-flow waveforms in normal human subjects. Physiol. Meas. 1999, 20, 219–240. [Google Scholar] [CrossRef] [PubMed]
- Safar, M.E.; Asmar, R.; Benetos, A.; Blacher, J.; Boutouyrie, P.; Lacolley, P.; Laurent, S.; London, G.; Panni, B.; Protogerou, A. Interaction between hypertension and arterial stiffness an expert reappraisal. Hypertension 2018, 72, 796–805. [Google Scholar] [CrossRef] [PubMed]
- Masuda, Y.; Hirai, A.; Ozawa, S.; Fukushima, K. The preejection waves in the arterial pulse waves. Cardiovasc. Sound Bull. 1974, 4, 273–280. (In Japanese) [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Amplitude of Blood Pressure Pulse Wave AP [mN] | Discriminant Index LF/HF | |
|---|---|---|
| Average | 208 | 5.74 |
| Standard deviation | 43.7 | 1.05 |
| Coefficient of variation | 0.210 | 0.183 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osawa, Y.; Dohi, T. Extraction and Evaluation of Discriminative Indexes of the Wearing Condition for High-Precision Blood Pressure Pulse Wave Measurement. Micromachines 2022, 13, 679. https://doi.org/10.3390/mi13050679
Osawa Y, Dohi T. Extraction and Evaluation of Discriminative Indexes of the Wearing Condition for High-Precision Blood Pressure Pulse Wave Measurement. Micromachines. 2022; 13(5):679. https://doi.org/10.3390/mi13050679
Chicago/Turabian StyleOsawa, Yosuke, and Tetsuji Dohi. 2022. "Extraction and Evaluation of Discriminative Indexes of the Wearing Condition for High-Precision Blood Pressure Pulse Wave Measurement" Micromachines 13, no. 5: 679. https://doi.org/10.3390/mi13050679
APA StyleOsawa, Y., & Dohi, T. (2022). Extraction and Evaluation of Discriminative Indexes of the Wearing Condition for High-Precision Blood Pressure Pulse Wave Measurement. Micromachines, 13(5), 679. https://doi.org/10.3390/mi13050679