
Predictability of Astigmatism Correction by Arcuate Incisions with a Femtosecond Laser Using the Gaussian Approximation Calculation


 ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
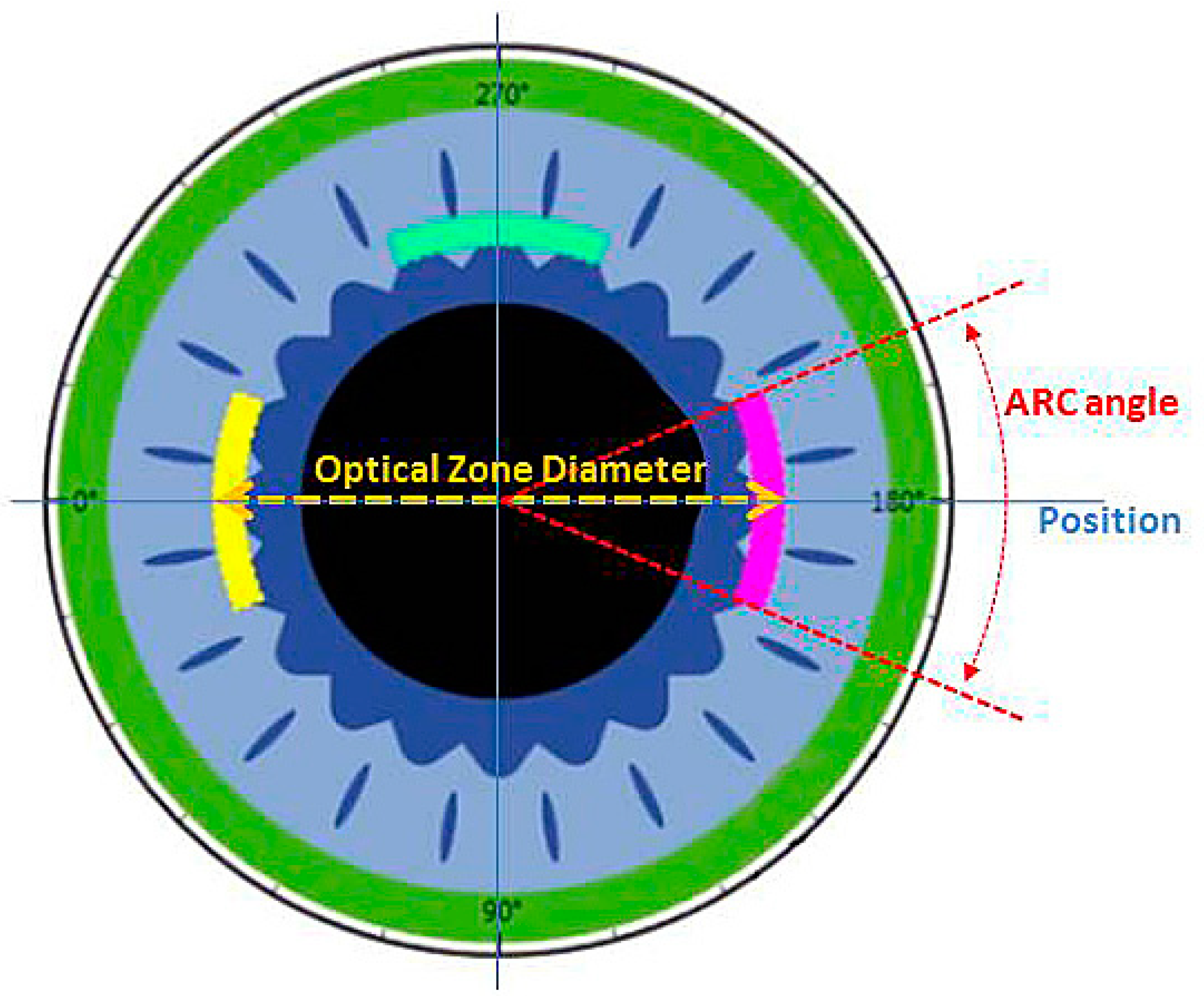
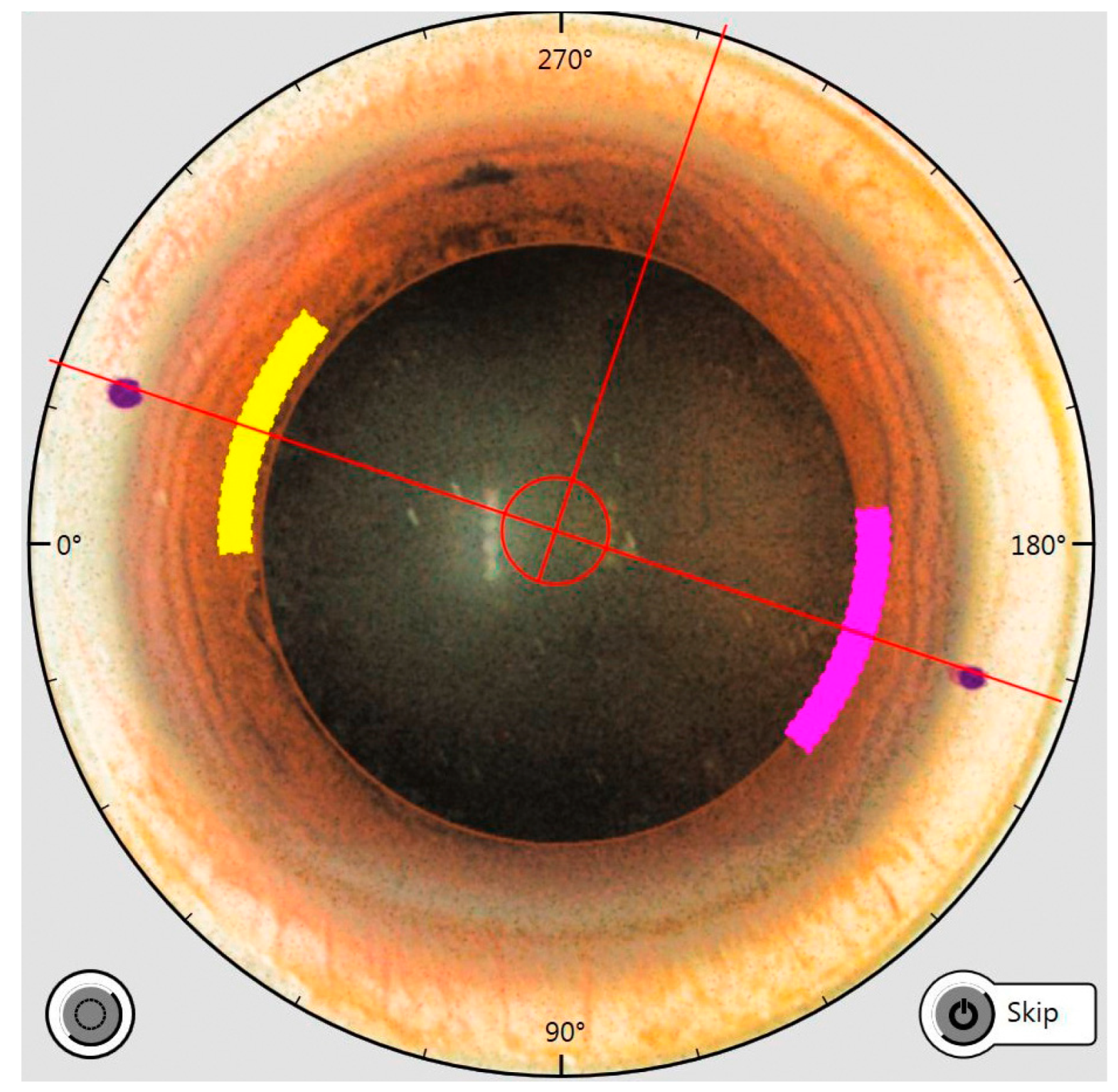
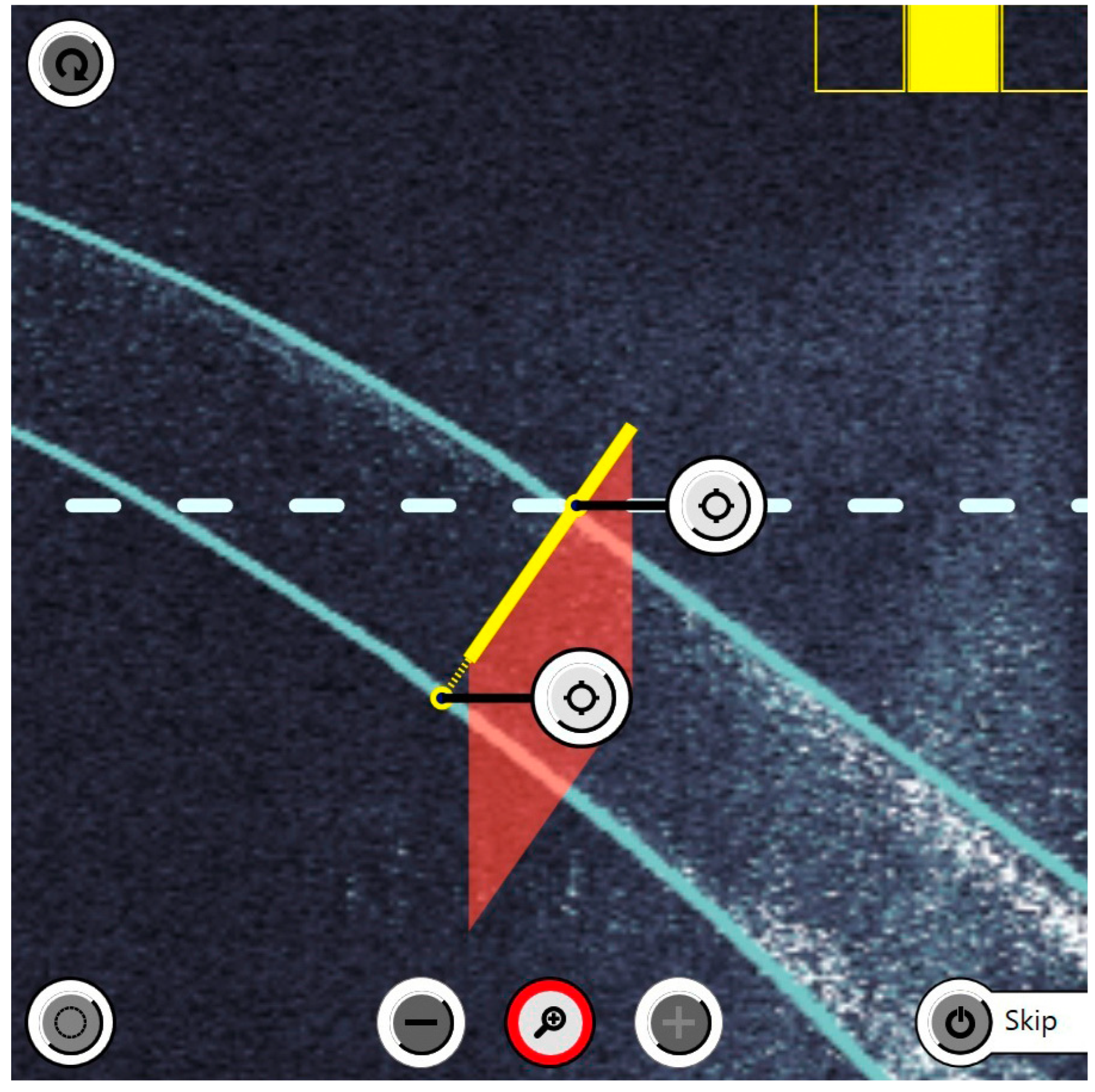
2.1. Surgery Technique with Femtosecond Laser of the Arcuate Incisions
2.2. Calculation and Application of the Treatment Parameters of the Arcuate Incisions
3. Results
3.1. Demographics
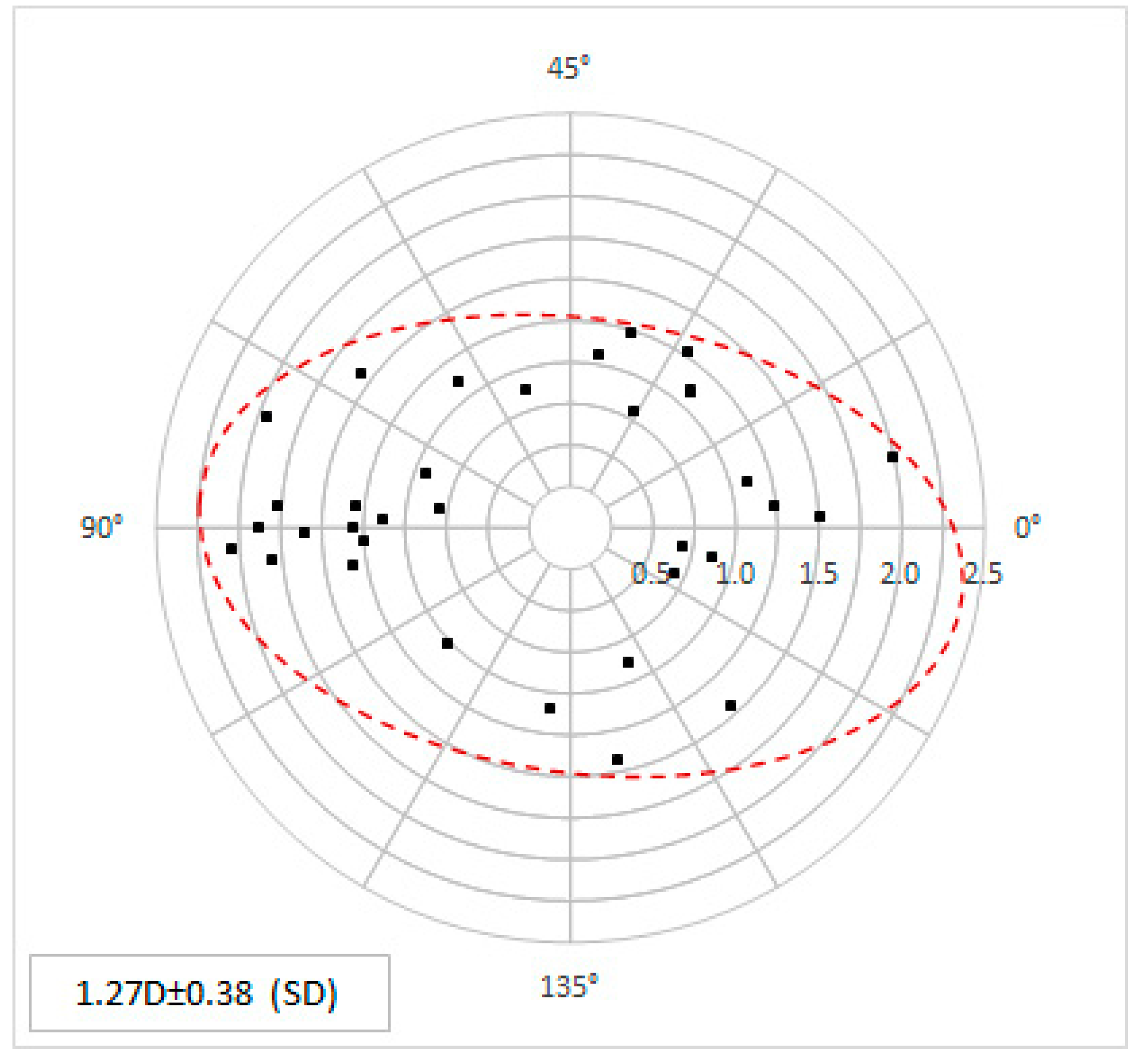
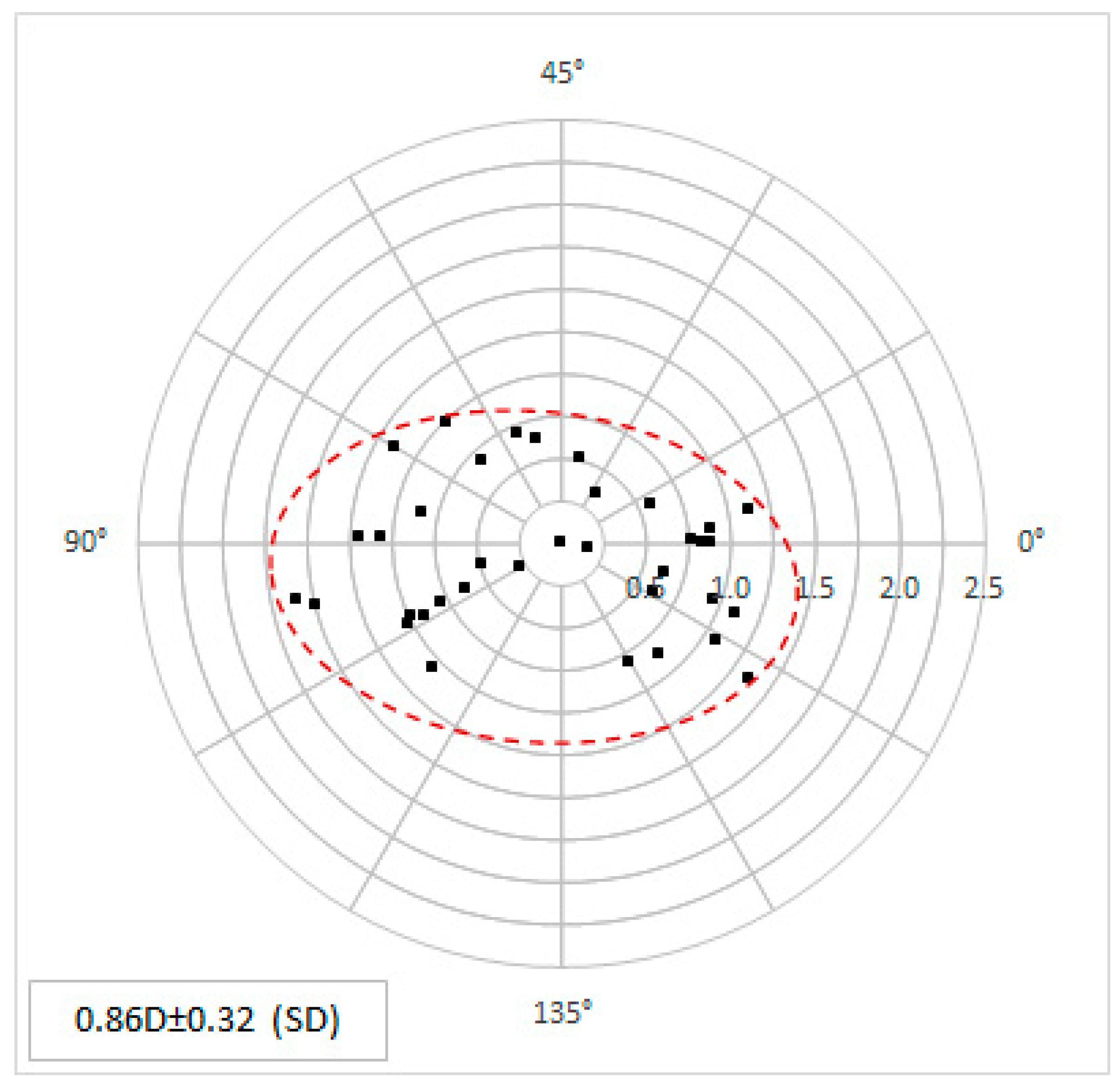
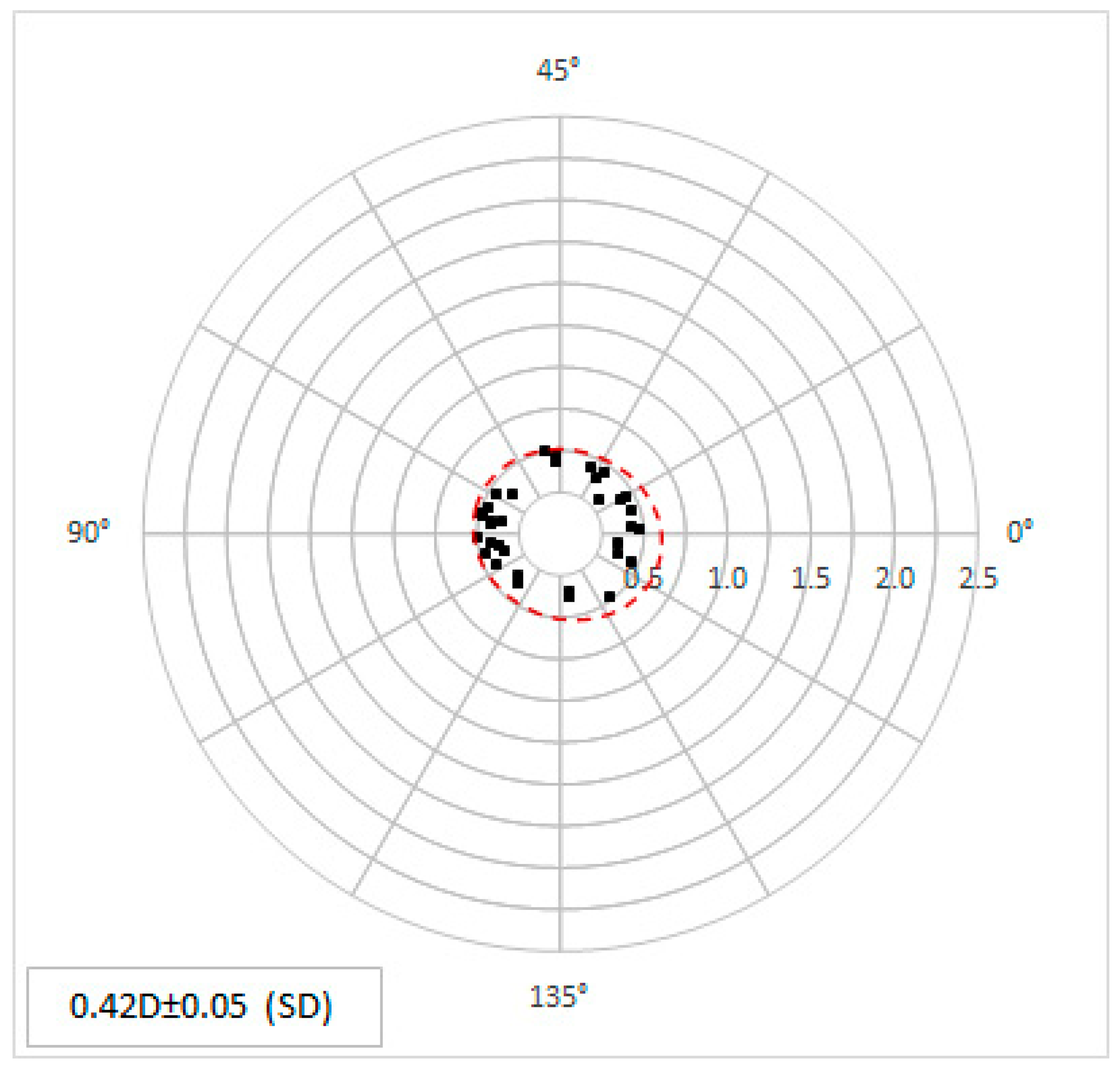
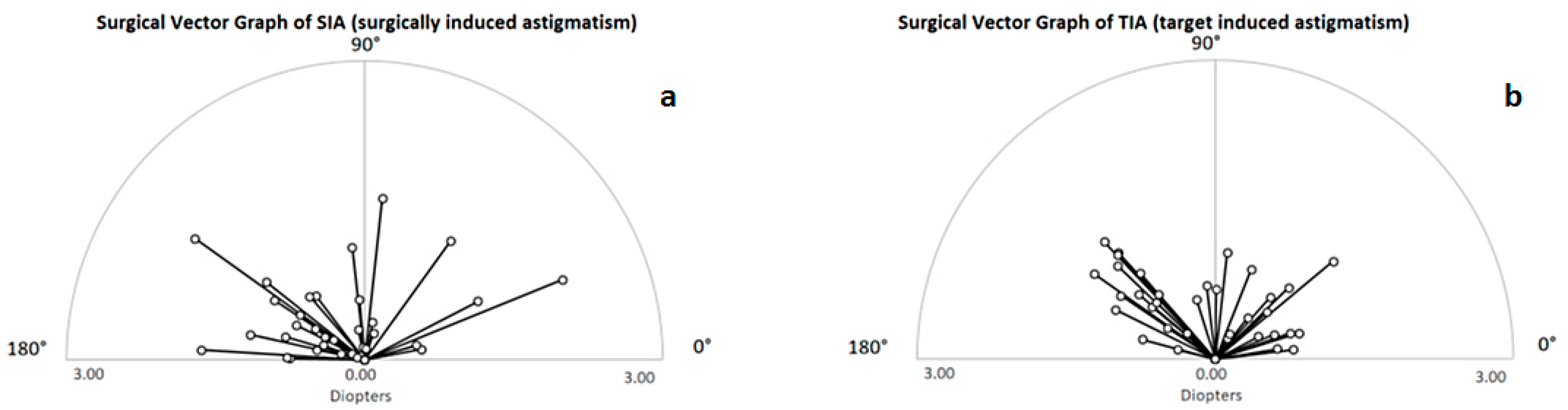
3.2. Clinical Outcomes of Astigmatism Correction
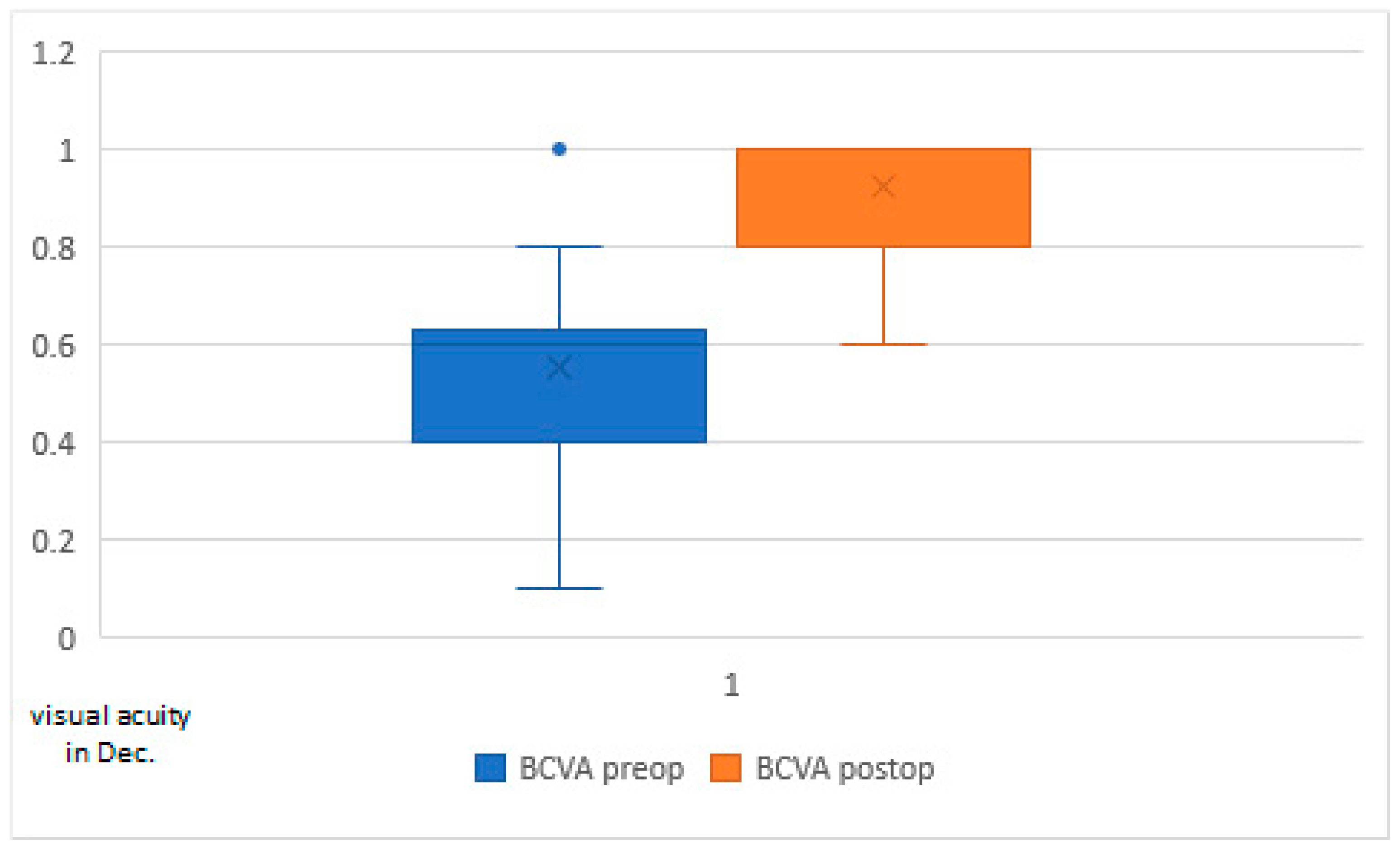
3.3. Visual Acuity and Target Refraction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
References
- Pascolini, D.; Mariotti, S.P. Global estimates of visual impairment: 2010. Br. J. Ophthalmol. 2012, 96, 614–618. [Google Scholar] [CrossRef] [PubMed]
- Hashemi, H.; Fotouhi, A.; Yekta, A.; Pakzad, R.; Ostadimoghaddam, H.; Khabazkhoob, M. Global and regional estimates of prevalence of refractive errors: Systematic review and meta-analysis. J. Curr. Ophthalmol. 2017, 30, 3–22. [Google Scholar] [CrossRef] [PubMed]
- De Bernardo, M.; Zeppa, L.; Cennamo, M.; Iaccarino, S.; Rosa, N. Prevalence of Corneal Astigmatism before Cataract Surgery in Caucasian Patients. Eur. J. Ophthalmol. 2014, 24, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Ferrer-Blasco, T.; Montés-Micó, R.; Peixoto-De-Matos, S.C.; González-Méijome, J.M.; Cerviño, A. Prevalence of corneal astigmatism before cataract surgery. J. Cataract. Refract. Surg. 2009, 35, 70–75. [Google Scholar] [CrossRef]
- Bae, J.; Kim, S.J.; Choi, Y. Pseudophakic Residual Astigmatism. Korean J. Ophthalmol. 2005, 18, 116–120. [Google Scholar] [CrossRef]
- Behndig, A.; Montan, P.; Stenevi, U.; Kugelberg, M.; Zetterström, C.; Lundström, M. Aiming for emmetropia after cataract surgery: Swedish National Cataract Register study. J. Cataract Refract. Surg. 2012, 38, 1181–1186. [Google Scholar] [CrossRef]
- Wang, L.-L.; Wang, W.; Han, X.-T.; He, M.-G. Influence of severity and types of astigmatism on visual acuity in school-aged children in southern China. Int. J. Ophthalmol. 2018, 11, 1377–1383. [Google Scholar] [CrossRef]
- Watanabe, K.; Negishi, K.; Kawai, M.; Torii, H.; Kaido, M.; Tsubota, K. Effect of Experimentally Induced Astigmatism on Functional, Conventional, and Low-Contrast Visual Acuity. J. Refract. Surg. 2013, 29, 19–25. [Google Scholar] [CrossRef]
- Kaczmarek, A.; Brockmann, C.; Laube, T. Non-Penetrating Femtosecond Laser Intrastromal Astigmatic Keratotomy Performed during Laser-Assisted Cataract Surgery: Results on Keratometric Astigmatism. Open J. Ophthalmol. 2017, 7, 262–272. [Google Scholar] [CrossRef]
- Visco, D.M.; Bedi, R.; Packer, M. Femtosecond laser–assisted arcuate keratotomy at the time of cataract surgery for the management of preexisting astigmatism. J. Cataract Refract. Surg. 2019, 45, 1762–1769. [Google Scholar] [CrossRef]
- Vickers, L.A.; Gupta, P.K. Femtosecond laser-assisted keratotomy. Curr. Opin. Ophthalmol. 2016, 27, 277–284. [Google Scholar] [CrossRef]
- Rückl, T.; Dexl, A.K.; Bachernegg, A.; Reischl, V.; Riha, W.; Ruckhofer, J.; Binder, P.S.; Grabner, G. Femtosecond laser–assisted intrastromal arcuate keratotomy to reduce corneal astigmatism. J. Cataract. Refract. Surg. 2013, 39, 528–538. [Google Scholar] [CrossRef]
- Chan, T.C.Y.; Ng, A.L.K.; Cheng, G.P.M.; Wang, Z.; Woo, V.C.P.; Jhanji, V. Corneal Astigmatism and Aberrations After Combined Femtosecond-Assisted Phacoemulsification and Arcuate Keratotomy: Two-Year Results. Am. J. Ophthalmol. 2016, 170, 83–90. [Google Scholar] [CrossRef]
- Chan, T.C.Y.; Ng, A.L.K.; Wang, Z.; Chang, J.S.M.; Cheng, G.P.M. Five-Year Changes in Corneal Astigmatism After Combined Femto-second-Assisted Phacoemulsification and Arcuate Keratotomy. Am. J. Ophthalmol. 2020, 217, 232–239. [Google Scholar] [CrossRef]
- Pepose, J.D.; Feigenbaum, S.K.; Qazi, M.A.; Sanderson, J.P.; Roberts, C.J. Changes in corneal biome-chanics and intraocular pressure following LASIK using static, dynamic and Noncontact Tonometry. Am. J. Ophthalmol. 2006, 143, 39–47. [Google Scholar] [CrossRef]
- Studer, H.P.; Roberts, C.J. Optimization of Surgical Treatments in the Cornea. Cataract. Refract. Surgery Today Europe 2015, March. Available online: https://crstodayeurope.com/articles/2015-mar/optimization-of-surgical-treatments-in-the-cornea/ (accessed on 10 March 2023).
- Baharozian, C.J.; Song, C.; Hatch, K.M.; Talamo, J.H. A novel nomogram for the treatment of Astigmatism with femtosecond-laser arcuate incisions at the time of cataract surgery. Clin. Ophthalmol. 2017, 11, 1841–1848. [Google Scholar] [CrossRef]
- Slade, S.G. Femtosecond laser arcuate incision astigmatism correction in cataract surgery. In Proceedings of the Cornea Day/ASCRS Symposium on Cataract, IOL and Refractive Surgery, San Diego, CA, USA, 25 March 2011. [Google Scholar]
- Wendelstein, J.A.; Hoffmann, P.C.; Mariacher, S.; Wingert, T.; Hirnschall, N.; Findl, O.; Bolz, M. Precision and refractive predictability of a new nomogram for femtosecond laser-assisted corneal arcuate incisions. Acta Ophthalmol. 2021, 99, e1297–e1306. [Google Scholar] [CrossRef]
- Aghamohammadzadeh, H.; Newton, R.H.; Meek, K.M. X-ray scattering used to map the preferred collagen orientation in the human cornea and limbus. Structure 2004, 12, 249–256. [Google Scholar] [CrossRef]
- Winkler, M.; Chai, D.; Kriling, S.; Nien, C.J.; Brown, D.J.; Jester, B.; Juhasz, T.; Jester, J. Nonlinear Optical Macroscopic Assessment of 3-D Corneal Collagen Organization and Axial Biomechanics. Investig. Opthalmology Vis. Sci. 2011, 52, 8818–8827. [Google Scholar] [CrossRef]
- Petsche, S.J.; Chernyak, D.; Martiz, J.; Levenston, M.; Pinsky, P.M. Depth-Dependent Transverse Shear Properties of the Human Corneal Stroma. Investig. Opthalmology Vis. Sci. 2012, 53, 873–880. [Google Scholar] [CrossRef]
- Petsche, S.J.; Pinsky, P.M. The role of 3-D collagen organization in stromal elasticity: A model based on X-ray diffraction data and second harmonic-generated images. Biomech. Model. Mechanobiol. 2013, 12, 1101–1113. [Google Scholar] [CrossRef] [PubMed]
- Elsheikh, A.; Wang, D.; Brown, M.; Rama, P.; Campanelli, M.; Pye, D. Assessment of Corneal Biomechanical Properties and Their Variation with Age. Curr. Eye Res. 2007, 32, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Elsheikh, A.; Brown, M.; Alhasso, D.; Rama, P.; Campanelli, M.; Garway-Heath, D. Experimental assessment of corneal anisot-ropy. J. Refract. Surg. 2008, 24, 178–187. [Google Scholar] [PubMed]
- Last, J.A.; Thomasy, S.M.; Croasdale, C.R.; Russell, P.; Murphy, C.J. Compliance profile of the human cornea as measured by atomic force microscopy. Micron 2012, 43, 1293–1298. [Google Scholar] [CrossRef]
- Koenig, S.B.; Hamano, T.; Yamaguchi, T.; Kimura, T.; McDonald, M.B.; Kaufman, H.E. Refractive keratoplasty with hydrogel implants in primates. Ophthalmic Surg. 1984, 15, 225–229. [Google Scholar]
- McCarey, B.E.; von Rij, G.; Waring, G.O., III. Keratophakia with hydrogel implants (ARVO Abstract). Investig. Ophthalmol. Vis. Sci. 1983, 24, 147. [Google Scholar]
- Whitford, C.; Studer, H.; Boote, C.; Meek, K.M.; Elsheikh, A. Biomechanical model of the human cornea: Considering shear stiffness and regional variation of collagen anisotropy and density. J. Mech. Behav. Biomed. Mater. 2015, 42, 76–87. [Google Scholar] [CrossRef]
- Studer, H.P.; Riedwyl, H.; Amstutz, C.A.; Hanson, J.V.; Büchler, P. Patient-specific finite-element simulation of the human cornea: A clinical validation study on cataract surgery. J. Biomech. 2013, 46, 751–758. [Google Scholar] [CrossRef]
- Studer, H.P.; Pradhan, K.R.; Reinstein, D.Z.; Businaro, E.; Archer, T.J.; Gobbe, M.; Roberts, C.J. Biomechanical Modeling of Femto-second Laser Keyhole Endokeratophakia Surgery. J. Refract. Surg. 2015, 31, 480–486. [Google Scholar] [CrossRef]
- Businaro, E.; Studer, H.; Pajic, B.; Büchler, P. Gaussian process prediction of the stress-free configuration of pre-deformed soft tissues: Application to the human cornea. Med. Eng. Phys. 2016, 38, 339–345. [Google Scholar] [CrossRef]
- Roberts, H.W.; Wagh, V.K.; Sullivan, D.L.; Archer, T.J.; O’brart, D.P. Refractive outcomes after limbal relaxing incisions or femtosecond laser arcuate keratotomy to manage corneal astigmatism at the time of cataract surgery. J. Cataract. Refract. Surg. 2018, 44, 955–963. [Google Scholar] [CrossRef]
- Day, A.C.; Lau, N.M.; Stevens, J.D. Nonpenetrating femtosecond laser intrastromal astigmatic keratotomy in eyes having cataract surgery. J. Cataract. Refract. Surg. 2016, 42, 102–109. [Google Scholar] [CrossRef]
- Hiep, N.X.; Khanh, P.T.M.; Quyet, D.; Van Thai, T.; Nga, V.T.; Dinh, T.C.; Bac, N.D. Correcting Corneal Astigmatism with Corneal Arcuate Incisions during Femtosecond Laser Assisted Cataract Surgery. Open Access Maced. J. Med. Sci. 2019, 7, 4260–4265. [Google Scholar] [CrossRef] [PubMed]
- Lindstrom, R.L. The Surgical Correction of Astigmatism: A Clinician’s Perspective. J. Refract. Surg. 1990, 6, 441–454. [Google Scholar] [CrossRef]
- Truffer, O.; Abler, D.; Pajic, B.; Grabner, G.; Kraker, H.; Büchler, P. Optimization of surgical parameters based on patient-specific models: Application to arcuate keratotomy. J. Cataract. Refract. Surg. 2019, 45, 1084–1091. [Google Scholar] [CrossRef]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanmillan, I.L.; Thumann, G.; Kropp, M.; Cvejic, Z.; Pajic, B. Predictability of Astigmatism Correction by Arcuate Incisions with a Femtosecond Laser Using the Gaussian Approximation Calculation. Micromachines 2023, 14, 1009. https://doi.org/10.3390/mi14051009
Sanmillan IL, Thumann G, Kropp M, Cvejic Z, Pajic B. Predictability of Astigmatism Correction by Arcuate Incisions with a Femtosecond Laser Using the Gaussian Approximation Calculation. Micromachines. 2023; 14(5):1009. https://doi.org/10.3390/mi14051009
Chicago/Turabian StyleSanmillan, Isabel Llopis, Gabriele Thumann, Martina Kropp, Zeljka Cvejic, and Bojan Pajic. 2023. "Predictability of Astigmatism Correction by Arcuate Incisions with a Femtosecond Laser Using the Gaussian Approximation Calculation" Micromachines 14, no. 5: 1009. https://doi.org/10.3390/mi14051009
APA StyleSanmillan, I. L., Thumann, G., Kropp, M., Cvejic, Z., & Pajic, B. (2023). Predictability of Astigmatism Correction by Arcuate Incisions with a Femtosecond Laser Using the Gaussian Approximation Calculation. Micromachines, 14(5), 1009. https://doi.org/10.3390/mi14051009