Intensity Modulated Radiotherapy (IMRT) + Carbon Ion Boost for Adenoid Cystic Carcinoma of the Minor Salivary Glands in the Oral Cavity

 , ,
, ,
Abstract
:1. Introduction
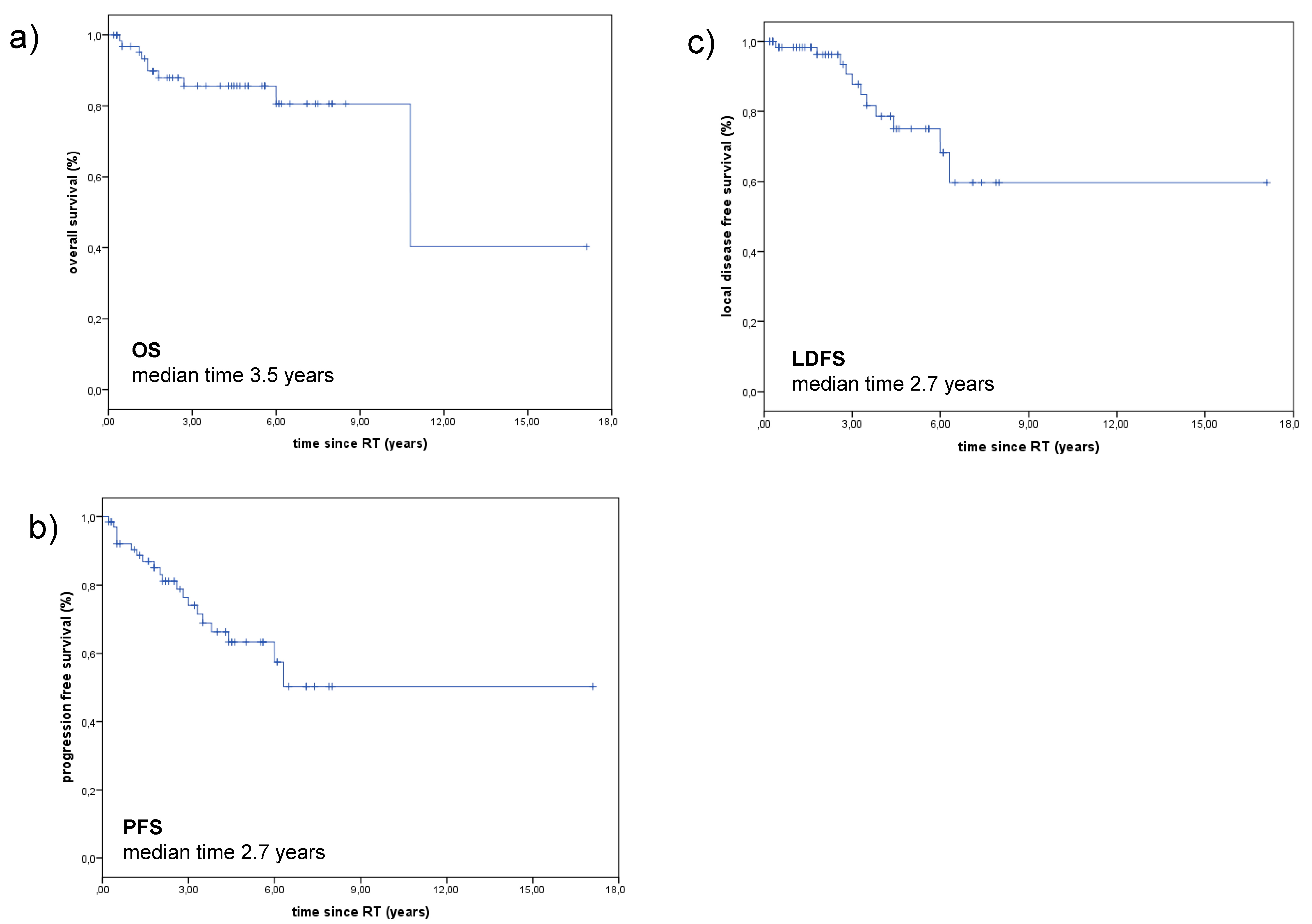
2. Results
2.1. Treatment Outcome
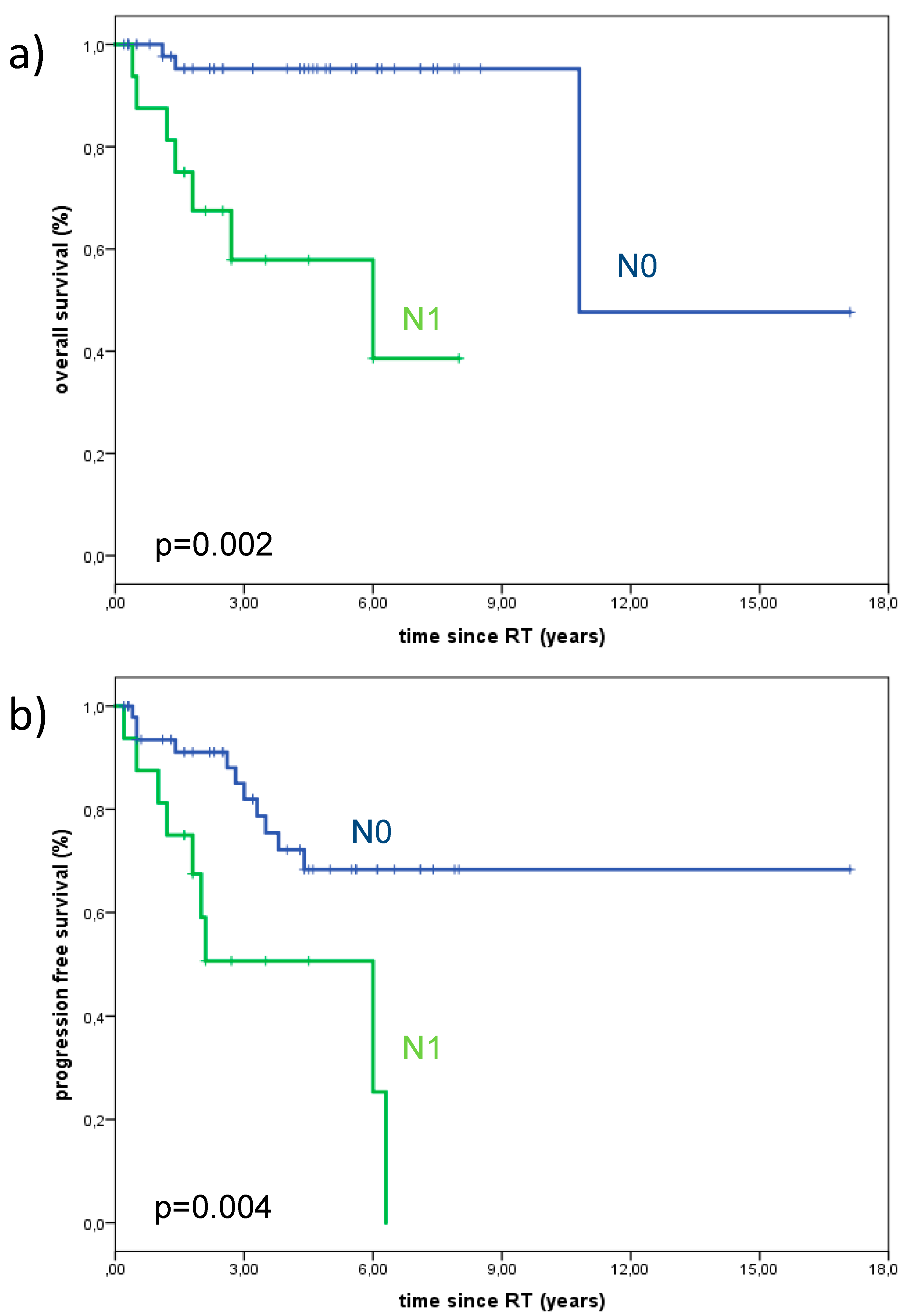
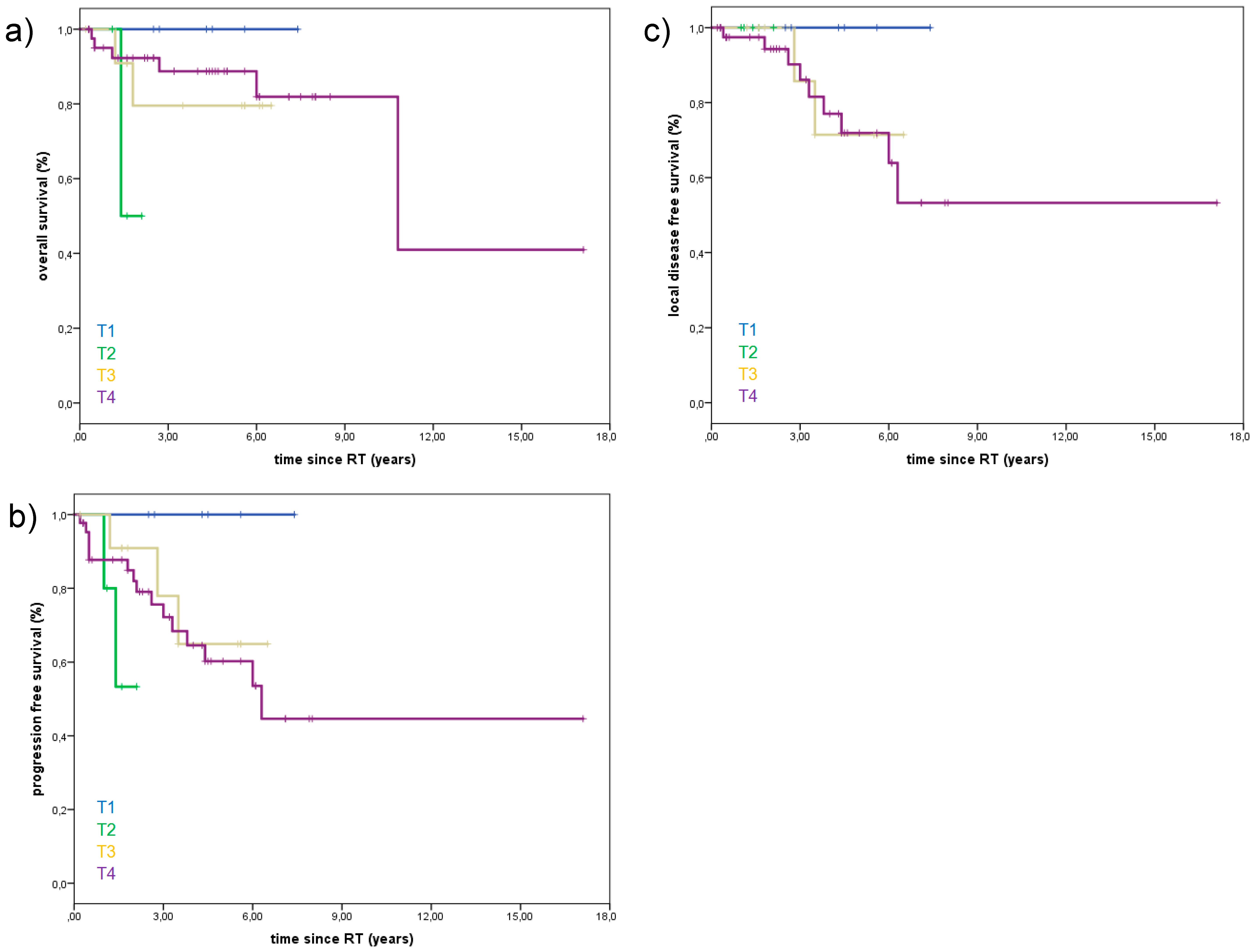
2.2. Prognostic Factors
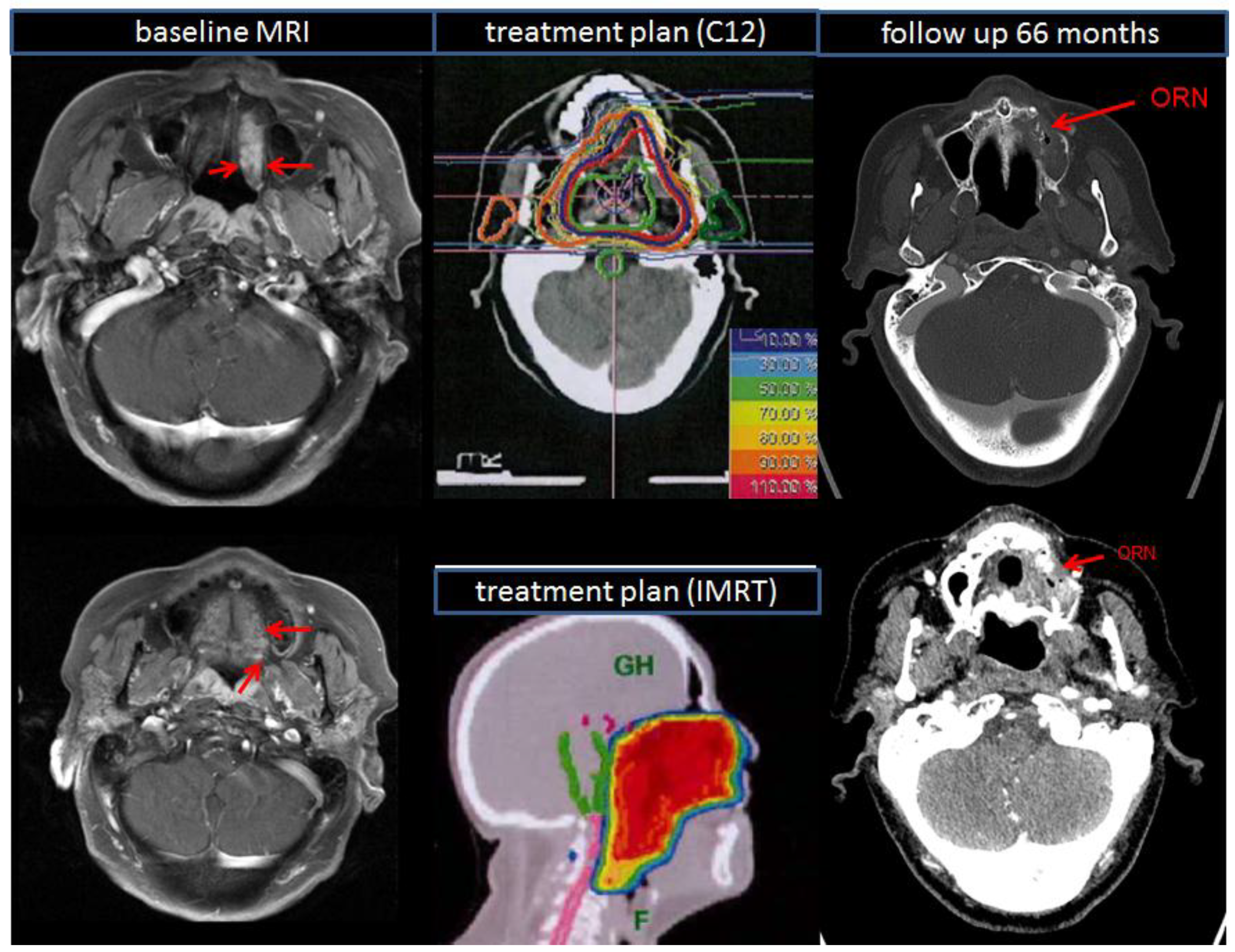
2.3. Treatment Toxicity
3. Discussion
4. Materials and Methods
4.1. Demographic and Patient Characteristics
4.2. Pre-Treatment Imaging
4.3. Treatment Modalities — Combined RT (IMRT+C12)
4.4. Follow-Up
4.5. Overall Survival (OS)
4.6. Progression-Free Survival (PFS)
4.7. Local Disease-Free Survival (LDFS)
4.8. Treatment Toxicity
4.9. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bradley, P.J. Adenoid cystic carcinoma of the head and neck: A review. Curr. Opin. Otolaryngol. Head Neck Surg. 2004, 12, 127–132. [Google Scholar] [CrossRef] [PubMed]
- Bjorndal, K.; Krogdahl, A.; Therkildsen, M.H.; Charabi, B.; Kristensen, C.A.; Andersen, E.; Schytte, S.; Primdahl, H.; Johansen, J.; Pedersen, H.B.; et al. Salivary adenoid cystic carcinoma in Denmark 1990–2005: Outcome and independent prognostic factors including the benefit of radiotherapy. Results of the Danish Head and Neck Cancer Group (DAHANCA). Oral Oncol. 2015, 51, 1138–1142. [Google Scholar] [CrossRef] [PubMed]
- DeAngelis, A.F.; Tsui, A.; Wiesenfeld, D.; Chandu, A. Outcomes of patients with adenoid cystic carcinoma of the minor salivary glands. Int. J. Oral Maxillofac. Surg. 2011, 40, 710–714. [Google Scholar] [CrossRef] [PubMed]
- Hyam, D.M.; Veness, M.J.; Morgan, G.J. Minor salivary gland carcinoma involving the oral cavity or oropharynx. Aust. Dent. J. 2004, 49, 16–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nascimento, A.G.; Amaral, A.L.; Prado, L.A.; Kligerman, J.; Silveira, T.R. Adenoid cystic carcinoma of salivary glands. A study of 61 cases with clinicopathologic correlation. Cancer 1986, 57, 312–319. [Google Scholar] [CrossRef] [Green Version]
- Kokemueller, H.; Eckardt, A.; Brachvogel, P.; Hausamen, J.E. Adenoid cystic carcinoma of the head and neck--a 20 years experience. Int. J. Oral Maxillofac. Surg. 2004, 33, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.J.; Pambuccian, S.E.; Ondrey, F.G.; Adams, G.L.; Gaffney, P.M. Genes associated with early development, apoptosis and cell cycle regulation define a gene expression profile of adenoid cystic carcinoma. Oral Oncol. 2006, 42, 994–1004. [Google Scholar] [CrossRef] [PubMed]
- Speight, P.M.; Barrett, A.W. Salivary gland tumours. Oral Dis. 2002, 8, 229–240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Triantafillidou, K.; Dimitrakopoulos, J.; Iordanidis, F.; Koufogiannis, D. Management of adenoid cystic carcinoma of minor salivary glands. J. Oral Maxillofac. Surg. 2006, 64, 1114–1120. [Google Scholar] [CrossRef]
- Coca-Pelaz, A.; Rodrigo, J.P.; Bradley, P.J.; Vander Poorten, V.; Triantafyllou, A.; Hunt, J.L.; Strojan, P.; Rinaldo, A.; Haigentz, M., Jr.; Takes, R.P.; et al. Adenoid cystic carcinoma of the head and neck--An update. Oral Oncol. 2015, 51, 652–661. [Google Scholar] [CrossRef]
- Coca-Pelaz, A.; Rodrigo, J.P.; Triantafyllou, A.; Hunt, J.L.; Rinaldo, A.; Strojan, P.; Haigentz, M., Jr.; Mendenhall, W.M.; Takes, R.P.; Vander Poorten, V.; et al. Salivary mucoepidermoid carcinoma revisited. Eur. Arch. Oto-Rhino-Laryngol. 2015, 272, 799–819. [Google Scholar] [CrossRef]
- Mucke, T.; Tannapfel, A.; Kesting, M.R.; Wagenpfeil, S.; Robitzky, L.K.; Wolff, K.D.; Holzle, F. Adenoid cystic carcinomas of minor salivary glands. Auris Nasus Larynx 2010, 37, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Schulz-Ertner, D.; Nikoghosyan, A.; Didinger, B.; Munter, M.; Jakel, O.; Karger, C.P.; Debus, J. Therapy strategies for locally advanced adenoid cystic carcinomas using modern radiation therapy techniques. Cancer 2005, 104, 338–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Debus, J.; Engenhart-Cabillic, R.; Kraft, G.; Wannenmacher, M. The role of high-LET radiotherapy compared to conformal photon radiotherapy in adenoid cystic carcinoma. Strahlenther. Onkol. 1999, 175, 63–65. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.D.; Poulakis, M.; Nikoghosyan, A.V.; Welzel, T.; Uhl, M.; Federspil, P.A.; Freier, K.; Krauss, J.; Hoss, A.; Haberer, T.; et al. High-LET radiotherapy for adenoid cystic carcinoma of the head and neck: 15 years’ experience with raster-scanned carbon ion therapy. Radiother. Oncol. 2016, 118, 272–280. [Google Scholar] [CrossRef]
- Chang, C.F.; Hsieh, M.Y.; Chen, M.K.; Chou, M.C. Adenoid cystic carcinoma of head and neck: A retrospective clinical analysis of a single institution. Auris Nasus Larynx 2018, 45, 831–837. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.M.; Bucci, M.K.; Weinberg, V.; Garcia, J.; Quivey, J.M.; Schechter, N.R.; Phillips, T.L.; Fu, K.K.; Eisele, D.W. Adenoid cystic carcinoma of the head and neck treated by surgery with or without postoperative radiation therapy: Prognostic features of recurrence. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Ellington, C.L.; Goodman, M.; Kono, S.A.; Grist, W.; Wadsworth, T.; Chen, A.Y.; Owonikoko, T.; Ramalingam, S.; Shin, D.M.; Khuri, F.R.; et al. Adenoid cystic carcinoma of the head and neck: Incidence and survival trends based on 1973-2007 Surveillance, Epidemiology, and End Results data. Cancer 2012, 118, 4444–4451. [Google Scholar] [CrossRef]
- He, S.; Li, P.; Zhong, Q.; Hou, L.; Yu, Z.; Huang, Z.; Chen, X.; Fang, J.; Chen, X. Clinicopathologic and prognostic factors in adenoid cystic carcinoma of head and neck minor salivary glands: A clinical analysis of 130 cases. Am. J. Otolaryngol. 2017, 38, 157–162. [Google Scholar] [CrossRef]
- Mendenhall, W.M.; Morris, C.G.; Amdur, R.J.; Werning, J.W.; Hinerman, R.W.; Villaret, D.B. Radiotherapy alone or combined with surgery for adenoid cystic carcinoma of the head and neck. Head Neck 2004, 26, 154–162. [Google Scholar] [CrossRef] [Green Version]
- Mendenhall, W.M.; Morris, C.G.; Amdur, R.J.; Werning, J.W.; Villaret, D.B. Radiotherapy alone or combined with surgery for salivary gland carcinoma. Cancer 2005, 103, 2544–2550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Da Cruz Perez, D.E.; de Abreu Alves, F.; Nobuko Nishimoto, I.; de Almeida, O.P.; Kowalski, L.P. Prognostic factors in head and neck adenoid cystic carcinoma. Oral Oncol. 2006, 42, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Mizoe, J.E.; Hasegawa, A.; Jingu, K.; Takagi, R.; Bessyo, H.; Morikawa, T.; Tonoki, M.; Tsuji, H.; Kamada, T.; Tsujii, H.; et al. Results of carbon ion radiotherapy for head and neck cancer. Radiother. Oncol. 2012, 103, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Spiro, R.H. Distant metastasis in adenoid cystic carcinoma of salivary origin. Am. J. Surg. 1997, 174, 495–498. [Google Scholar] [CrossRef]
- Huber, P.E.; Debus, J.; Latz, D.; Zierhut, D.; Bischof, M.; Wannenmacher, M.; Engenhart-Cabillic, R. Radiotherapy for advanced adenoid cystic carcinoma: Neutrons, photons or mixed beam? Radiother. Oncol. 2001, 59, 161–167. [Google Scholar] [CrossRef]
- Shah, J.P.; Gil, Z. Current concepts in management of oral cancer--surgery. Oral Oncol. 2009, 45, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Asikainen, P.J.; Kullaa, A.M.; Koistinen, A.; Schulten, E.; Ten Bruggenkate, C.M. A phd completed. The effect of radiotherapy on oral mucosa cell morphology. Ned. Tijdschr. Tandheelkd. 2018, 125, 169–171. [Google Scholar] [CrossRef] [PubMed]
- Cheriex, K.C.; Nijhuis, T.H.; Mureau, M.A. Osteoradionecrosis of the jaws: A review of conservative and surgical treatment options. J. Reconstr. Microsurg. 2013, 29, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Chronopoulos, A.; Zarra, T.; Ehrenfeld, M.; Otto, S. Osteoradionecrosis of the jaws: Definition, epidemiology, staging and clinical and radiological findings. A concise review. Int. Dent. J. 2018, 68, 22–30. [Google Scholar] [CrossRef]
- Dai, T.; Tian, Z.; Wang, Z.; Qiu, W.; Zhang, Z.; He, Y. Surgical management of osteoradionecrosis of the jaws. J. Craniofac. Surg. 2015, 26, e175–e179. [Google Scholar] [CrossRef]
- Rice, N.; Polyzois, I.; Ekanayake, K.; Omer, O.; Stassen, L.F. The management of osteoradionecrosis of the jaws--a review. Surgeon 2015, 13, 101–109. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors/Year | Number of Patients | Median Follow Up (Months) | RT Modality | Treatment Intention | T4-Stage | LC | OS | Conclusion for Using C12 |
|---|---|---|---|---|---|---|---|---|
| Jensen et al. 2015 [12] | 53 | 42 | Combined (IMRT+C12) | R1, R2, definitive | 57% | 3-years: 81.9% | 3-years: 78.4% | less toxicity in combined group |
| Jensen et al. 2015 [12] | 58 | 74 | Combined (IMRT+C12) | definitive, R2 | 90% | 5-years: 59.6% | 10-years: 44.2% | LC, OS, PFS better in combined group |
| Jensen et al. 2015 [12] | 37 | 63 | photons alone | definitive, R2 | 94% | 5-years: 39.9% | 10-years: 19.6% | LC, OS, PFS better in combined group |
| Jensen et al. 2016 [12] | 309 | 34 | Combined (IMRT+C12) | R1, R2, definitive | 60% | 3-years: 83.7% | 3-years: 88.9% | good LC in combined group |
| Early Treatment Toxicity | No of Patients | Late Treatment Toxicity | No of Patients | |||
|---|---|---|---|---|---|---|
| CTC grade | n | % | CTC grade | n | % | |
| Mukositis | ||||||
| 1 | 8 | 11.9 | 1 | 7 | 10.4 | |
| 2 | 21 | 31.3 | 2 | 2 | 4.5 | |
| 3 | 35 | 52.2 | ||||
| Dermatitis | ||||||
| 1 | 38 | 56.7 | 1 | 11 | 16.4 | |
| 2 | 22 | 32.9 | ||||
| 3 | 5 | 7.5 | ||||
| Dysphagia | ||||||
| 1 | 13 | 19.4 | 1 | 13 | 19.4 | |
| 2 | 39 | 58.2 | ||||
| 3 | 8 | 11.9 | ||||
| Xerostomia | ||||||
| 1 | 43 | 64.2 | 1 | 33 | 49.3 | |
| 2 | 8 | 11.9 | 2 | 7 | 10.4 | |
| Epitheliolysis | ||||||
| 3 | 11 | 16.4 | ||||
| Osteoradionecrosis | ||||||
| 3 | 2 | 3.0 | ||||
| Hearing impairment | ||||||
| 13 | 19.4 | 8 | 11.9 | |||
| Loss of taste | ||||||
| 50 | 74.6 | |||||
| Trismus | ||||||
| 16 | 23.9 | 20 | 29.9 | |||
| Edema | ||||||
| 2 | 3.0 | 1 | 1.5 | |||
| Fatigue | ||||||
| 59 | 88.1 | |||||
| Hair loss | ||||||
| 3 | 4.5 | |||||
| Characteristics | No of Patients (%) |
|---|---|
| gender | |
| male | 27 (40.3%) |
| female | 40 (59.7%) |
| T-stage | |
| 1 | 6 (9.0%) |
| 2 | 5 (7.5%) |
| 3 | 12 (17.9%) |
| 4 | 43 (64.2%) |
| N-stage | |
| 0 | 51 (76.1%) |
| + | 16 (23.9%) |
| Resection margin | |
| 0 | 10 (14.9%) |
| 1 | 52 (77.6%) |
| 2 | 5 (7.5%) |
| Locations in oral cavity | |
| buccal | 8 (11.9%) |
| palate (soft/hard) | 35 (52.2%) |
| tongue | 5 (7.5%) |
| maxilla | 19 (28.4%) |
| Characteristics | No of Patients |
|---|---|
| irradiation | |
| photons + carbon ions | 67 |
| median IMRT dose | Gy (range) |
| 50 (48–56) | |
| median C12 dose | |
| 24 (18–24) | |
| median dose of cervical lymphatic drainage | |
| 50 (48–56) | |
| cumulative dose (IMRT + C12) | |
| 74 (68–74) | |
| median CTV volume (ccm) | |
| IMRT | 346 ccm (range: 21–921 ccm) |
| C12 | 134 ccm (range: 21–411 ccm) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lang, K.; Baur, M.; Akbaba, S.; Held, T.; Kargus, S.; Bougatf, N.; Bernhardt, D.; Freier, K.; Plinkert, P.K.; Rieken, S.; et al. Intensity Modulated Radiotherapy (IMRT) + Carbon Ion Boost for Adenoid Cystic Carcinoma of the Minor Salivary Glands in the Oral Cavity. Cancers 2018, 10, 488. https://doi.org/10.3390/cancers10120488
Lang K, Baur M, Akbaba S, Held T, Kargus S, Bougatf N, Bernhardt D, Freier K, Plinkert PK, Rieken S, et al. Intensity Modulated Radiotherapy (IMRT) + Carbon Ion Boost for Adenoid Cystic Carcinoma of the Minor Salivary Glands in the Oral Cavity. Cancers. 2018; 10(12):488. https://doi.org/10.3390/cancers10120488
Chicago/Turabian StyleLang, Kristin, Melissa Baur, Sati Akbaba, Thomas Held, Steffen Kargus, Nina Bougatf, Denise Bernhardt, Kolja Freier, Peter K. Plinkert, Stefan Rieken, and et al. 2018. "Intensity Modulated Radiotherapy (IMRT) + Carbon Ion Boost for Adenoid Cystic Carcinoma of the Minor Salivary Glands in the Oral Cavity" Cancers 10, no. 12: 488. https://doi.org/10.3390/cancers10120488
APA StyleLang, K., Baur, M., Akbaba, S., Held, T., Kargus, S., Bougatf, N., Bernhardt, D., Freier, K., Plinkert, P. K., Rieken, S., Debus, J., & Adeberg, S. (2018). Intensity Modulated Radiotherapy (IMRT) + Carbon Ion Boost for Adenoid Cystic Carcinoma of the Minor Salivary Glands in the Oral Cavity. Cancers, 10(12), 488. https://doi.org/10.3390/cancers10120488